
Abstract
Keywords
Coordinated care for chronic disease management
Noncommunicable diseases (NCDs), primarily affect older age groups, encompassing cardiovascular diseases, cancers, chronic respiratory diseases, and diabetes. These conditions account for 74% of global deaths, 1 posing significant challenges for patients, healthcare providers, and systems worldwide. Managing NCDs requires complex models of care, involving collaboration among traditionally fragmented professionals and institutions. This complexity intensifies for individuals with multimorbidity. Existing healthcare systems, primarily designed for acute care, inadequately address the evolving needs of chronic patients, 2 producing fragmentation and inefficiency. Bridging professional, provider, and institutions divides through integrated care service delivery is crucial for improving patient-centred outcomes, and enhancing healthcare systems, addressing the pressing necessity for more coordinated care approaches. 3 Various strategies aim to enhance service coordination for chronic disease management. Research highlights its short and long-term advantages, like cost savings from complications avoided, patient’s enhanced quality of life, better patient experience and workplace productivity gains.4–9 Studies comparing integrated and patient-centered care through collaboration demonstrate quality improvement over usual care.10,11 Specifically, interprofessional collaboration stands as a key standard ensuring safe, high-quality healthcare services across all professionals. 12 Interprofessional collaboration in healthcare is typically described as an active and ongoing partnership between professionals from various backgrounds and distinctive professional cultures, who may represent different organizations or sectors, working together to provide services that benefit healthcare users. 13 In chronic disease management, the motivation for interprofessional teamwork stems from complex patient needs that require the input of a range of different professionals’ perspectives or expertise.
A proactive multidisciplinary approach offers potential life and resource-saving benefits. 14 Established components like multidisciplinary and interprofessional teams, self-management, patient education interventions, and care coordination strategies are integral to effective chronic disease management models. 15 Also, payment mechanisms like pay-for-coordination, pay-for-performance, and bundled payments have varying success in improving coordination for chronic patients. 16 Models fostering joint care often integrate care pathways and other clinical governance tools, defining evidence-based care standards and linking outcomes to interventions. However, solely relying on evidence-based standards is not enough to foster collaboration among professionals for chronic patient care. To reduce fragmentation and enhance care consistency, broader organizational changes emphasizing accountability, shared responsibility for healthcare quality, and continuous performance improvements are crucial.17,18 The idea is that clinical, professional, organizational, system together with functional (e.g. financing and accountability) and normative (e.g., attitudes, behavior) aspects should be tackled together to support integrated care. 19
This paper aims to provide initial evidence about some dimensions supporting care integration, specifically when considering the interprofessional collaboration occurring between primary care physicians and specialists in the context of chronic disease management. Evidence is collected through a survey targeting Primary Care Physicians (PCPs) and hospital specialists managing chronic patients in a specific regional context characterized by the implementation of the Chronic Care Model (CCM). This study is part of the CoNtAcT Project, 20 a project financed by Tuscany Region (Italy) with the aim of exploring, studying and validating new governance mechanisms that promote integration between clinical professionals, improving care to chronic patients while ensuring cost-efficient care. The project encompasses various activities including the development of a questionnaire to understand the current state of interprofessional collaboration (the subject of this paper), the identification through data analysis of multiprofessional care networks for the management of selected chronic populations, the development of a multidimensional performance measurement system for benchmarking, target setting and supporting to system budgeting. The context analyzed features the primary care physician as the gatekeeper and coordinator of care, a role common both in tax-funded health systems and in social health insurance systems. 21
Chronic care in Tuscany region (Italy)
The Italian health system follows a Beveridge-like system which provides universal coverage largely free of charge at the point of delivery. 22 Tuscany is an administrative region in the center of Italy with about 3.7 million inhabitants (6.2 % of the Italian population). There are 1.4 million chronically ill persons (444.8 per 1000 inhabitants compared to 409.6 per 1000 in Italy 23 ). More than half are women and about 6 out of 10 are over 65 years of age. 24 The regional health system in Tuscany (TRHS) is a non-competitive system covering prevention, primary care as well as hospital services almost exclusively by public providers. It comprises three Local Health Authorities (LHAs) with 39 district general hospitals directly managed by the LHAs, four teaching hospitals, one research hospital, and 26 health districts, which oversee the organization and delivery of services for local health networks. Each LHAs have large catchment areas (about 900,000 resident) and provide preventive medicine and public health services, primary care, and inpatient and outpatient care, while the teaching hospitals focus on acute care and professional training.
About 2300 PCPs provide family medicine services 25 and act as gatekeepers to higher levels of care. The primary care system is the first point of contact for many Tuscan patients and often coordinates services with other parts of the health care system, including care provided by specialist physicians. PCPs are funded on a capitation basis and their activity is coordinated with the services provided by the health district. PCPs work in mono-specialist networks called Territorial Functional Aggregations (Aggregazioni Funzionali e Territoriali - AFTs) which are expected to apply clinical governance principles to continuously improve the quality of services and safeguard high standards of care for the population. 116 AFT are currently active, with an average size of 30,000 inhabitants and about 20 PCPs each.
Tuscany’s healthcare system has a history of caring for chronic patients, initially introducing the Chronic Care Model (CCM) in 2008, focusing on integrated services and patient involvement in managing their chronic conditions. 26 This model aims at intercepting care needs before the onset of the disease, it is based on self-management and peer-support systems. This evolved into the Expanded Chronic Care Model (ECCM), merging clinical and public health aspects, emphasizing prevention and health promotion. 27 Governance tools within ECCM support consistent care delivery across multidisciplinary team of professionals (generally PCP and hospital specialist), defining diagnostic and therapeutic pathways for chronic diseases. 24 However, ECCM implementation slowed due to the COVID-19 pandemic, prompting the ongoing reorganization of Tuscany’s healthcare system under regional resolution 1508/2022. This reorganization aims to revive and strengthen the healthcare system, adapting to evolving challenges, particularly in chronic patient care.
Overall design and survey development
Survey development
A survey was developed to assess the state of the art in terms of interprofessional collaboration among PCP and specialists managing patients with NCDs in Tuscany. The survey consists of 58 items on perceptions of professionals regarding clinical, professional, and organizational collaborative practices, including available managerial and accountability tools. In the long-term, the systematic use of the survey could serve as a monitoring tool for enhanced chronic patient management. Indeed, often the attention is towards introduction of structural and process changes with the expectations that formal changes will be internalized by professionals and managers and system performance will improve. But few systems measure possible progress in the level of collaboration between professionals or organizations 28 and assess how the collaboration has an impact on health outcomes. 29
The survey's development involved a literature search of concepts and measures about health service integration and interprofessional collaboration in the broader healthcare context, coupled with discussions with healthcare experts (healthcare managers and professionals) for question clarity and comprehensiveness.
Scan of concepts and measures of integrated health care and interdisciplinary collaboration
Different perspectives or taxonomies for the concept of integration of care exist. One of the first example of operationalizing integration of care is included in the work of Lukas et al 28 which captures aspects of system operation as building blocks of an integrated system. The authors recognize clinical and functional integration as the main driver to develop a survey about health service integration, thus looking at clinical coordination, availability of clinical guidelines/standard of care, service and staff cooperation, goal alignment and shared vision, leadership, and quality improvement approach. A more comprehensive model is proposed by Valentijn 19 which recognize functional and clinical integration but also, professional, organizational, and normative integration as key enablers for achieving integrated care service models. Organizational integration refers to align units, services departments, or organizations through coordinated actions of shared planning and regulation to provide joined-up, personalized care. While professional integration, defined at the meso-level, involves partnerships between professionals, multidisciplinary guidelines and protocols, interprofessional education and governance mechanisms, all elements supporting interprofessional collaboration. Basically, interprofessional work requires specific professionals to be able to work together to achieve a common product or shared goal, in the face of highly connected and interdependent tasks.30,31
For the development of the survey, the paper focuses on the notion of professional integration and interdisciplinary collaboration 13 as the targeted participants are professionals thus, they can provide more valuable indications on this key dimension for achieving integrated care rather than thinking about macro-level dimensions.
The review by D’amour et al. highlihts the complexity of collaboration, a multifaceted concept encompassing concepts like sharing, partnership, interdependency, and power, emphasizing its dynamic nature and the various skills involved. 32 It notes that collaboration manifests in different degrees and is subject to constant change. Moreover, the review underscores a lack of differentiation between determinants, processes, and outcomes of collaboration, and suggests that merely team assembly does not ensure collaboration. More recently, Schot et al. provide an interesting insight about the development of interprofessional collaboration which is not just the job of managers and policy makers, it also requires active contributions of professional, especially considering the bridging role, negotiating overlaps and creating spaces. 33 Drawing from interprofessional collaboration literature, the survey include items related to interprofessional practice/teamwork29,32,34 emphasizing professionals working collectively towards enhanced patient care. The literature search focused on instruments available to help organizations evaluate the strength and weaknesses of their delivery of care for chronic patients and item were purposefully selected from QUALICOPC EU Project, 35 Bonomi et al. 36 Dobrow et al., 37 Block et al., 38 and Nuño-Solinís et al. 39 Specifically, the Qualicop questionnaire, 35 which was created to investigate the organizational modalities of the PCP practices was used to introduce items related to clinical leadership, clinical coordination, and communication between health professionals working in different setting and with different working arrangements. The work by Nuño-Solinís et al. 39 informed the item generation regarding mutual knowledge and possible incentives reflecting physician-system integration (e,g., physician remuneration) and functional integration for managing chronic care, such as back-office support with shared information systems or soft elements pertaining to cross-team meeting. A further dimension of information systems and the use of electronic medical record data was also extrapolated from Dobrow et al. 37 On incentives to physicians also the work by Bonomi et al. 36 was helpful in retrieving questions about the organization of the health care delivery system looking at the linkages between the health system and community resources. Items related to clinical integration were supported by the work of Dobrow et al. 37 which identified disease management programs, including the use of clinical protocols, pathways and guidelines as the most challenging and important component of an organized delivery system. For the structuring of the dimensions related to co-ordination and co-operation was extrapolated from Bonomi et al. 36 to delivery system design from Block et al. 38
Finally, in structuring the survey the local reference context was also considered, the care pathways and clinical guidelines provided by the regional health plan were taken as a reference in the part regarding regulations and guidelines.
Key-informants’ feedback and survey-item generation
After close reading the literature and policy indications and mechanisms analysis introduced at regional level for CCM, we synthesized key dimensions of professional care integration, developing a preliminary survey. Shared with project partners—specialists, PCPs, and healthcare managers—the draft sought their insights on relevance, completeness, and item formulation. Discussions and feedbacks help refining the pilot version.
The finalized survey comprises 58 items: 53 closed-ended and 5 open-ended queries. 65% of items are common between PCPs and specialists while the remaining are refereed only to one of the two targeted respondents. Categorized into five sections, the survey comprises the following aspects: (i) “Context” which probes formal/informal PCP-specialist links and consultation frequency for chronic patient care. (ii) “Regulation and Guidelines” which evaluates shared guidelines’ presence, adequacy, and use for coherent inter-professional care. (iii) “Clinical Coordination and Cooperation between Services” which explores organizational and service integration across the chronic care pathway, encompassing shared planning, continuous care, and multidisciplinary or cross-functional team presence. (iv) “Innovation and Information Systems” which examines functional integration facets like shared back-office functions via electronic patient records and other shared information systems. (v) “Experience and Future Perspectives” which investigates perceptions of regional collaboration mechanisms’ efficacy and future strategies to bolster integration. Additionally, initial survey questions capture respondent demographics (gender, age, seniority in the profession and rate of assisted chronic patient).
Methods
Sampling survey pre-testing and data handling
Respondents, comprising 496 professionals (430 specialists and 66 PCPs) from diverse clinical disciplines and hospitals within three LHAs in Tuscany, were contacted via email following a non- probabilistic sampling strategy. Invitations included CoNtAcT Project’s purpose, data management, and assured questionnaire anonymity. The LimeSurvey platform hosted the online survey launched in March 2021, allowing 45 days for completion, with reminders sent. Ethical approval was not necessary as the questionnaire ensured complete respondent anonymity, eliminating harm or identification risks. The sample largely involved specialists from disciplines handling chronic patient cohorts in the CoNtAcT Project, including cardiology, endocrinology, internal medicine, geriatrics, pneumology, and nephrology.
Data analysis
Taking into consideration the context and characteristics of the respondents, descriptive analysis was performed for each survey item to describe the sample’s perception of the organization of the chronic patients care and the level of integration and coordination between the different professionals and care settings.
To evaluate the reliability of the survey, the random split-half sample (split-half validation) technique was adopted. 40 The sample of respondents was in fact randomly divided into two parts and the responses obtained were compared through the Chi Squared test at a 5% significance level. The tests led to not rejecting the null hypothesis of equality between the two groups in responses for 94% of the analyzed items (p < 0.05). Survey results were summarized using frequency tables and graphs to describe the main features of the study.
Results
A total of 247 fully completed questionnaires out of 496 were obtained (50% overall response rate, 50% PCPs’ response rate, 57% specialists’ response rate). Out of the sample of 247 respondents, 33 (13%) were PCPs and the remainder (214) were hospital specialists. The respondents, of whom 37% are female and with an average age of 52 years (SD 10), on average, have been in service at their facility for 16 years (SD 11) (15 years (SD 10) for specialists and 23 years (SD 13) for PCPs. Among the survey respondents, the specialty with the highest response rate is Endocrinology (24.21%), followed by General Practice (13.1%), Nephrology (9.13%), Cardiology (8.73%) and Pulmonology (8.33%). The respondents primarily belong to one of the three LHAs (ranging from 13.89% to 50%), and to a lesser extent, to one of the four teaching hospitals (ranging from 13.89% to 5.95%) or the research hospital (3.57%).The mean number of patients in charge to each PCPs was 1462 (SD 247), of which about 35% suffered of chronic diseases and 356 (SD 105) are over 70 years old. The specialists reported to deliver, on average, 92 (SD 123) outpatient visits per month of which about 60% are follow-up visits.
Starting from the investigation aimed at assessing the level of collaboration between specialists and PCPs, it seems that for both PCPs and specialists, the decision to refer a chronic patient to a specific colleague is often or always guided by the long-standing collaboration developed over the years among the two although, compared to specialists, PCPs show higher propensity to refer patients based on long-standing collaboration (85% and 60% respectively). The consolidated experience of the colleague on that specific chronic condition is also a key driver of the referral process both for PCPs and hospital specialists (79% and 74% respectively). On the other hand, only rarely referral decisions were based on the colleague’s good reputation (in cases of no collaboration with that specific colleague) or patients’ preferences (67% for PCPs and 66% for specialists and 77% for PCPs and 69% for specialists respectively). Results are reported in Figure 1. Percentage of all respondents (PCPs and specialists) about factors driving choice of referral. Item: “over the last year, which of the following factors guided your when referring a patient to a fellow specialist?”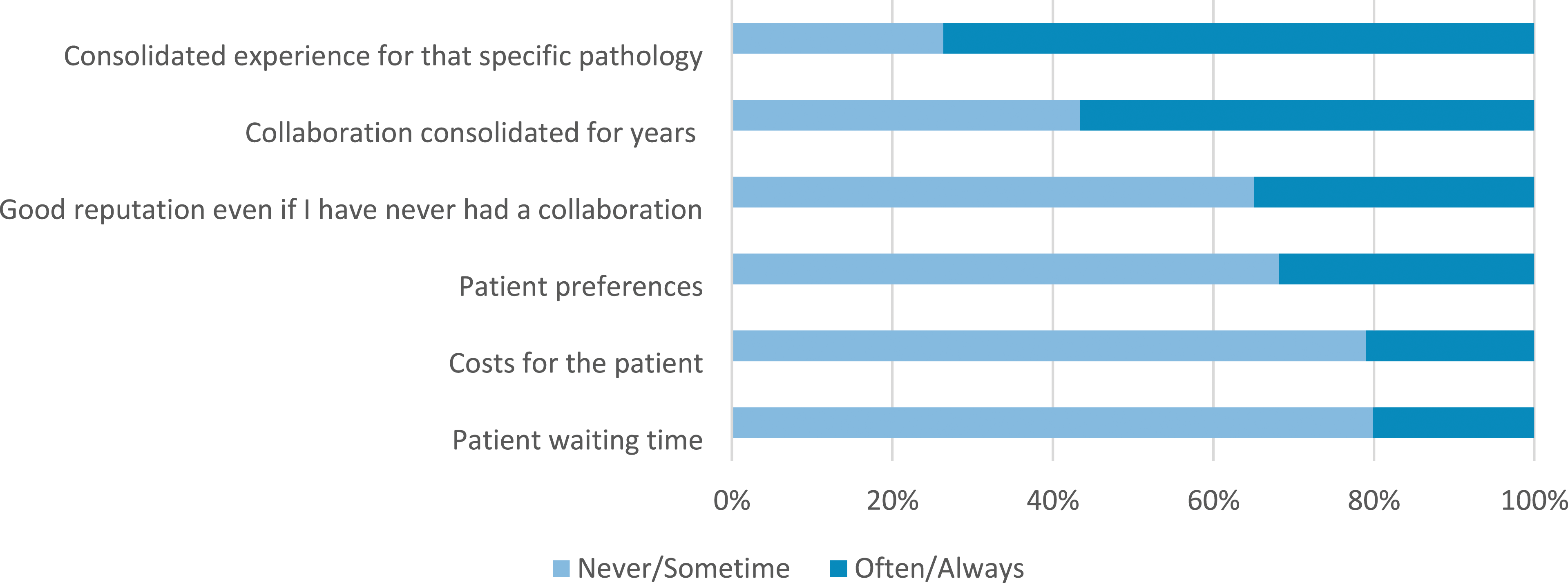
Higher interactions occur between PCPs and specialists for the diagnosis of cancer and neurological diseases (68% and 70% respectively), while diabetes, respiratory diseases, heart failure, and other chronic illnesses, appear to be more often diagnosed by the PCP alone (85%, 73%, 58%, and 90% respectively).
Additionally, PCPs are likely to refer a patient with chronic disease to the specialist when there is the need to update or modify the therapy or evaluate changes in the clinical condition only if symptoms worsen (64%) but not for regular follow-ups.
When considering the collaboration between PCPs and community professionals such as community nurses and allied health professionals for the care of chronic patients, 79% of PCPs report a quite high frequency of contacts with community nurses (4 or more times in a year), followed by physiotherapists and social workers (42% for both professional categories). On the other hand, 88% of PCPs reported having fewer than 3 yearly contacts with other healthcare professionals, such as podiatrists (Figure 2). Percentage of PCPs that collaborate with different healthcare professionals over the course of a year. Item: “For the management of patients with chronic diseases, how often do you collaborate with the following community healthcare professionals during a year?”.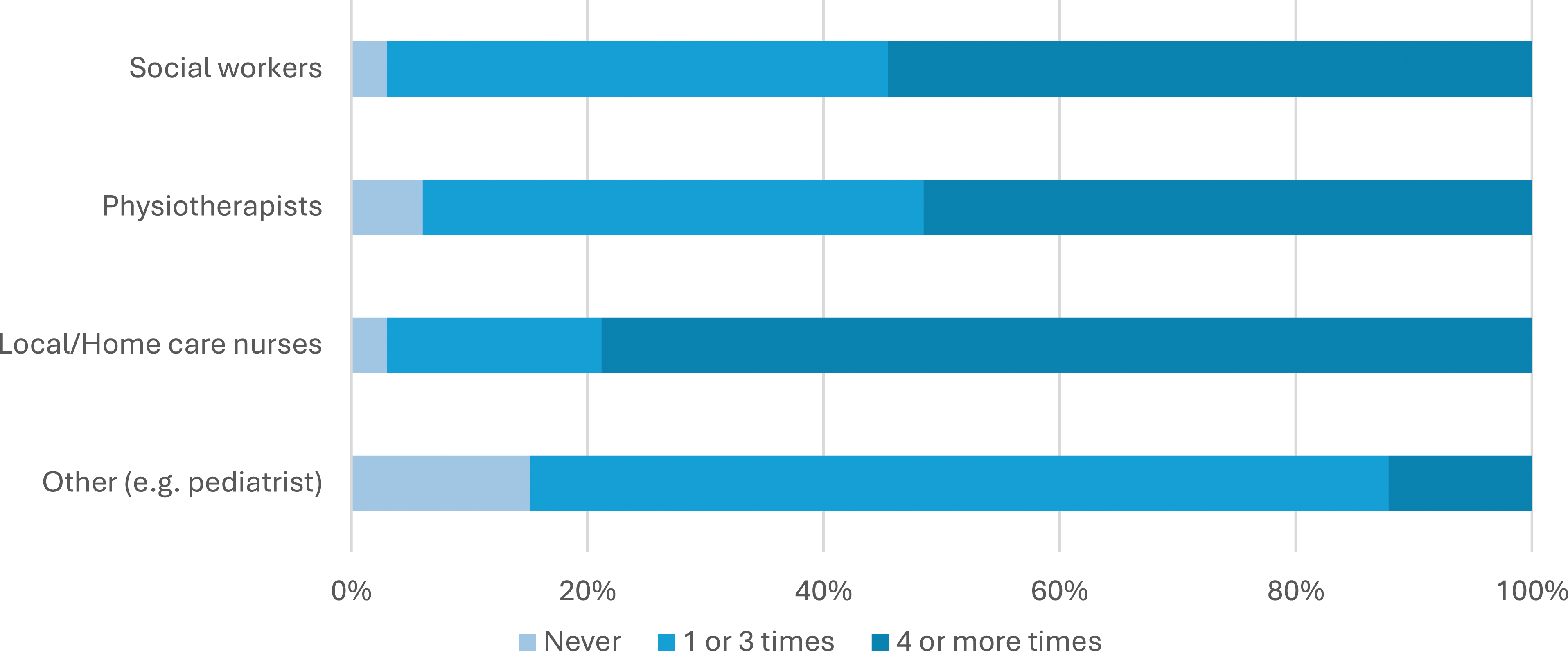
Turning the focus to the level of collaboration between PCPs and specialists, it is evident that PCPs engage in notably frequent interactions, with the highest frequency observed in their collaboration with hospital-based specialists (55%), followed closely by freelance medical specialists (48%). In contrast, interactions with other PCPs appear to be less frequent. In fact, 42% collaborate 4 or more times in a year with fellow PCPs in their own district/LHAarea. This percentage decreases further when collaboration extends to PCPs outside the district/LHA area (16%).
Regarding specialists, there is a greater propensity to collaborate with their hospital-based colleagues (78%). PCPs are the next most common collaborators, whether they belong to the specialist’s LHA area or not (collaboration rate of 64% and 62%, respectively, for 4 or more times a year). Less collaboration occur with freelance medical specialists(just 25% of specialists reporting having 4 or more contacts with colleagues in this category during the year). Notably, among various clinical disciplines within the hospital specialist group, internists, geriatricians, and pneumologists are those who report to collaborate most extensively with PCPs, compared to specialists from other disciplines (63%, 76%, 64% respectively declare to collaborate often/always with PCPs). These findings provide valuable insights into the dynamics of collaborative healthcare efforts among PCPs and specialists (Figure 3). Percentage of PCPs compared to specialists that collaborate with different medical specialists over the course of a year. Item: In a year, how often do you share the management of patients with chronic diseases with the following professionals?”.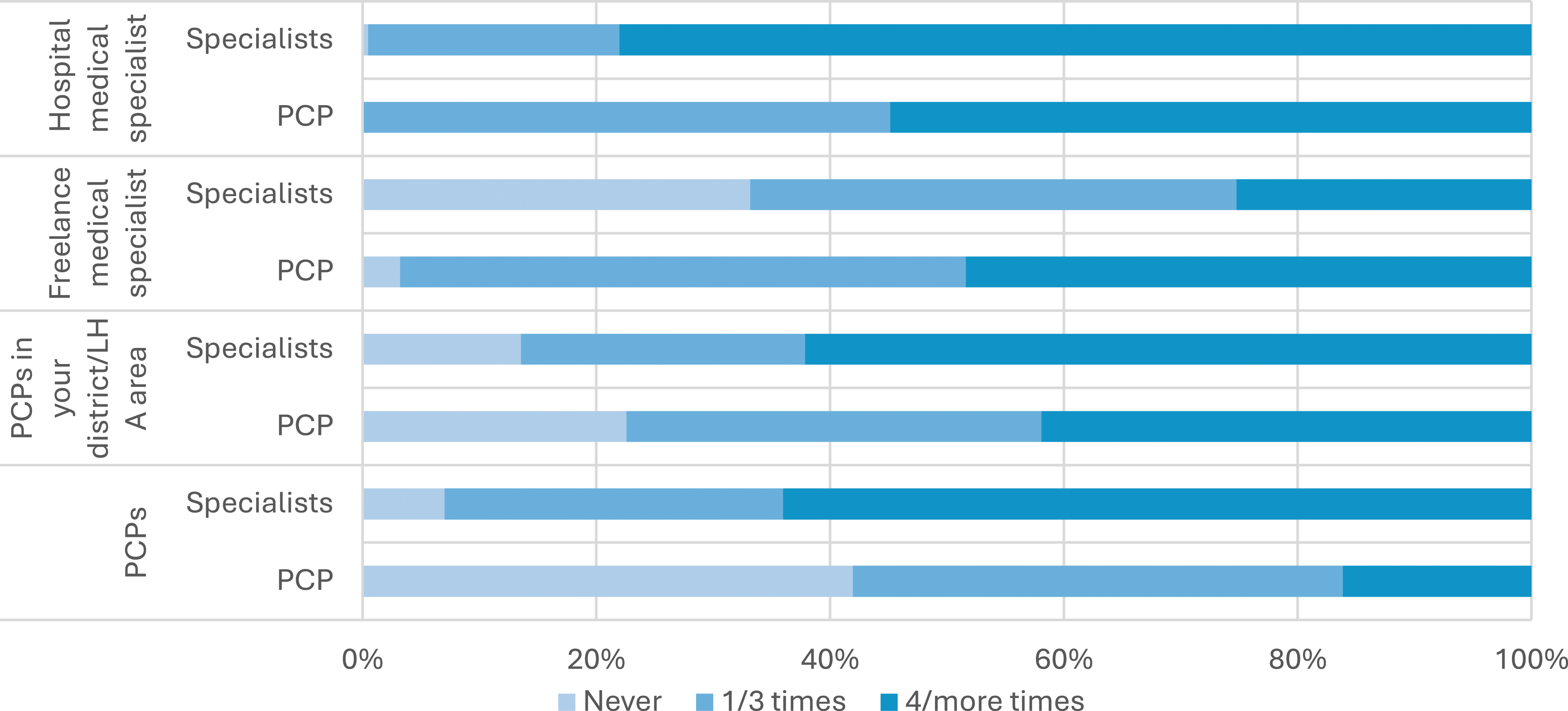
When turning the attention to the guidelines and regional measures for the integrated management of chronic population, 71% of all respondents are aware of the existence of a regional health plan for the integrated management of patients with chronic diseases, of which the majority (66%) considered it an effective tool for the organization and implementation of care services for their patients.
Three out of four respondent are also aware of the existence of clinical governance tools such as the diagnostic-therapeutic clinical protocols (i.e. pathway protocol) with specialists reporting higher percentage compared to PCPs (77% vs 64%). Considering only hospital specialists, nephrologists and geriatricians show higher awareness of pathways protocol for chronic patients (95% and 92% respectively) possibly because their care support is highly intertwined with other professionals thus requiring sharing of guidelines and protocols, while cardiologists are the less aware, only 41% declare to know about pathway protocol.
Among these respondents only 57% of respondents declared that these protocols are implemented, and 41% of the respondents believes that they are periodically updated according to the latest guidelines available, while 35% are not aware of continuous updates. Nonetheless, 46% of respondents believe that pathway protocols need improvements. Among these latter, 34% believe that they need to be updated according to the existing national guidelines, 46% would expect widespread diffusion/collective use and 20% think they should more accurately and completely describe the care network involved.
All the responses to the items were analysed by splitting the respondents into two groups: PCPs and specialists. The relative frequencies of response are shown in Table 1 (Appendix-A1).
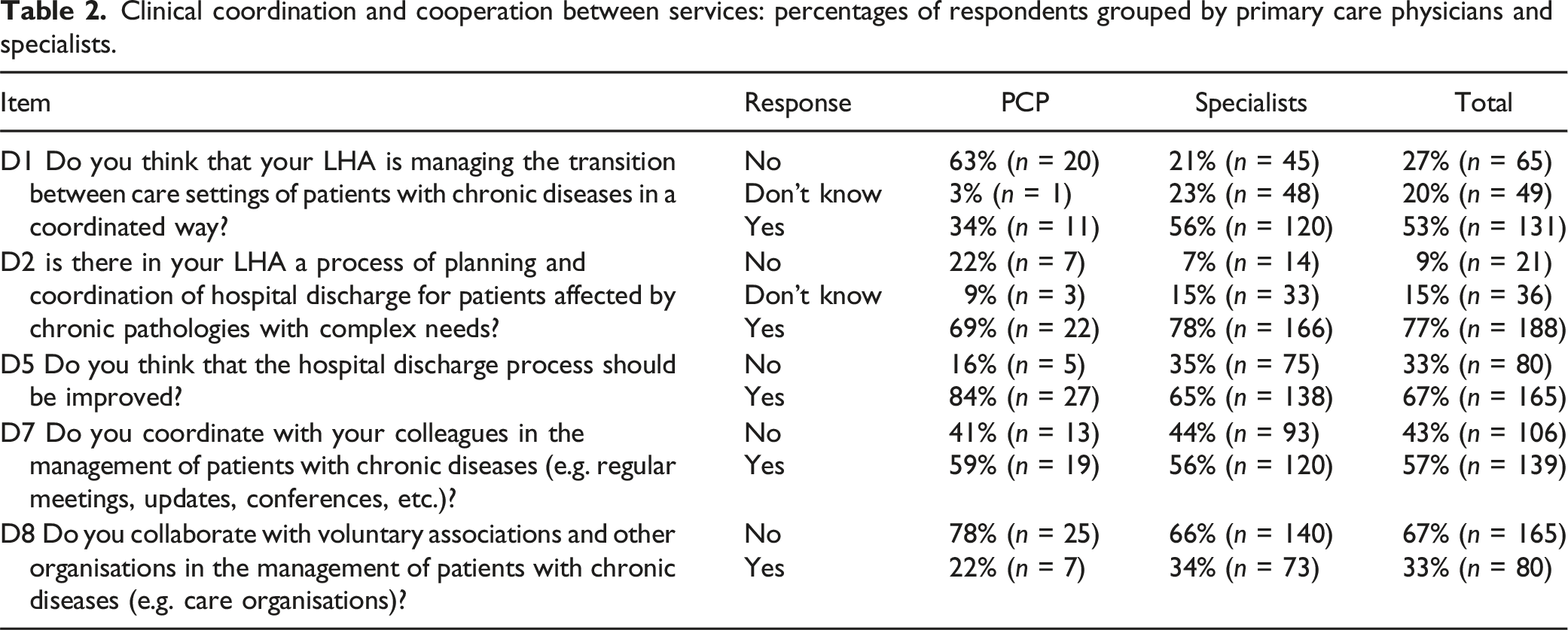
Regarding the section about clinical coordination and cooperation between services, it emerges (Table 2 in the Appendix-A1) that the perception about coordination strategies and mechanisms implemented by the health authority to support the transition of chronic patients between care settings is well managed for 53% of the respondents but hospital specialists show higher percentage compared to PCPs (56% vs 34%). There is a high level of awareness about the hospital discharge planning process for high need chronic diseases: 77% of respondents are aware of a hospital discharge planning and coordination process for these patients.
Among hospital specialists, geriatrician and internists are the professional groups showing higher percentage declaring that the hospital /health authority has a hospital-community transition process plan. Furthermore, 78% of all specialists are aware of the designated contact person responsible for organizing hospital discharges for chronically ill patients. However, 67% of them believe that the transition processes between different settings could be improved. Regarding the hospital discharge process, most respondents (84%) believe that the new model of transitional care led by a multiprofessional team (i.e., the agency for territorial therapeutic continuity) helps facilitate hospital discharge, although the service has margins for improvement (42%). Furthermore, 32.5% of respondents collaborate with voluntary associations for the management of patients suffering from NCDs.
Focusing on the sharing of clinical information between PCPs and specialists, 35.32% reported that information sharing occurs frequently/always, while 39.59% occasionally. The communication occurs through various channels (e.g., emails, phone calls, meetings), with the most used channel being the telephone (61.9%).
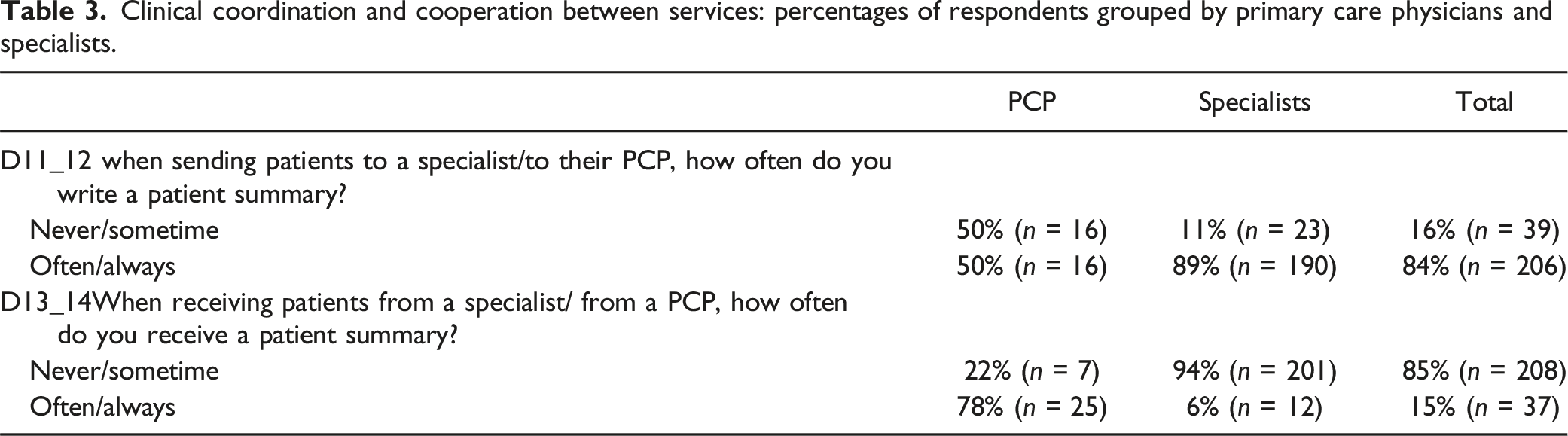
The perceptions from PCPs and specialists are different about the use of documentation as communication strategies to coordinate care among the two settings. PCPs often claim to have their patients refer to the specialist with a patient summary while the specialists claim to rarely receive from the patients the summary of their PCPs. On the other hand, the specialists report that, following a visit and/or a hospitalization, they usually provide patients with a letter to inform the PCP, this is confirmed by PCPs who claim to often receive from their patients a letter of the specialists (Table 3 in the Appendix-A1).
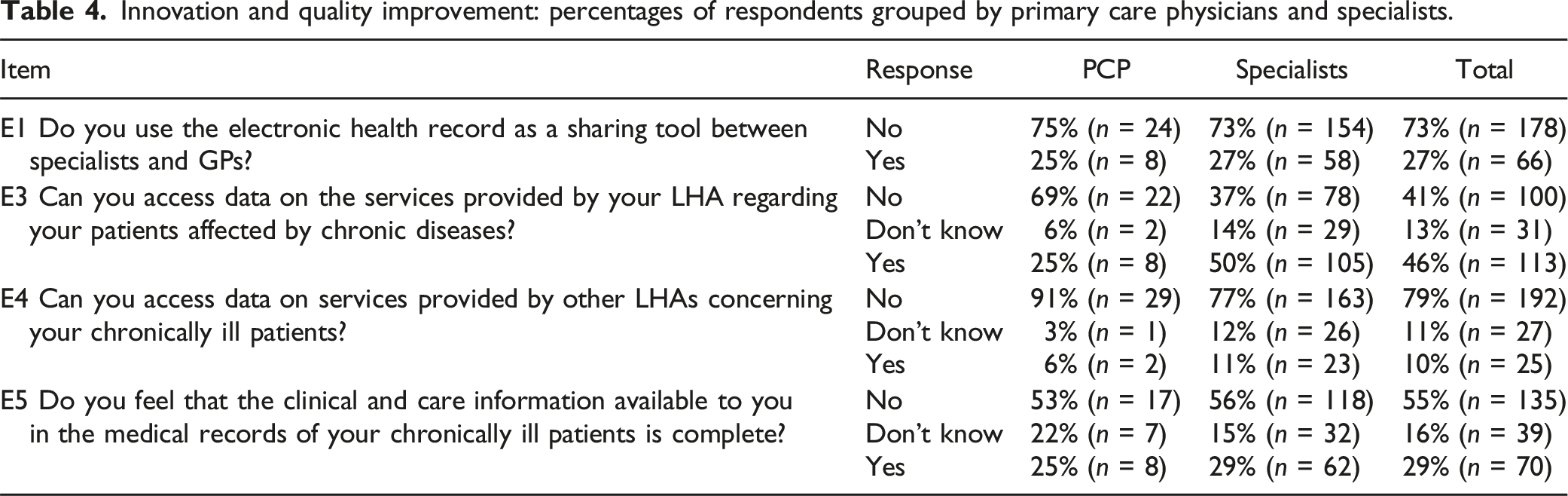
Regarding information systems (Table 4 in the Appendix-A1), 41% of the respondents cannot access to the information about their patients when care services are provided within their LHA, the difficulties are higher (78.7%) when chronic patients receive care from providers outside the LHA of the respondent. Nearly three quarters of respondents do not use the electronic patient records (EPR) as a sharing information tool.
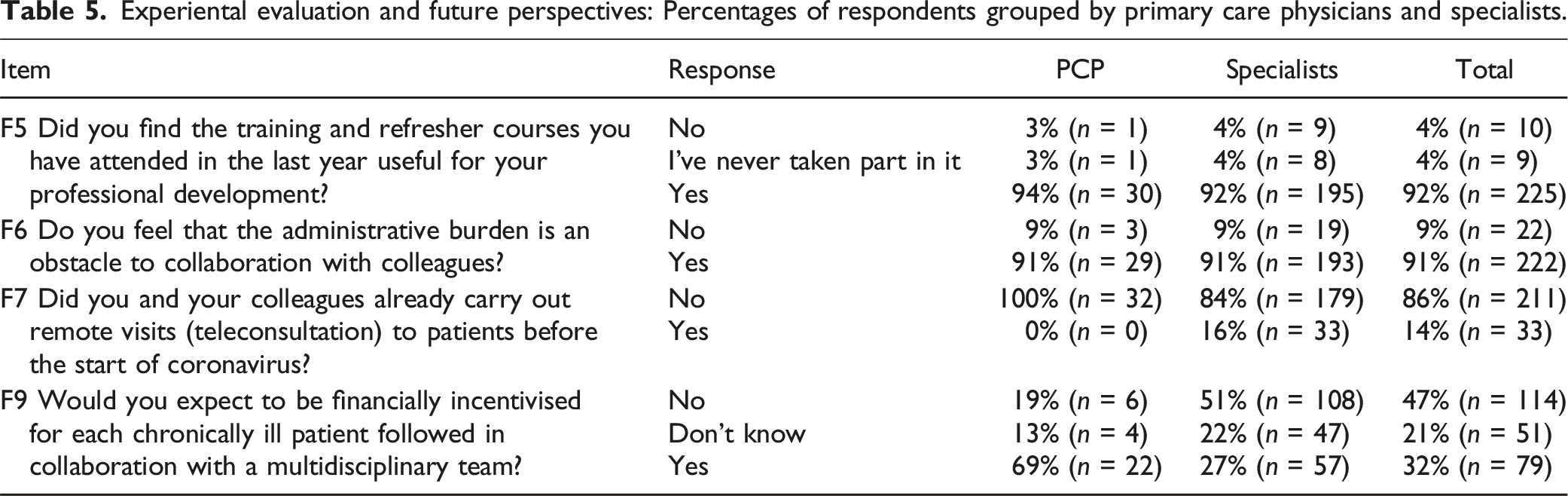
The last section of the survey investigates obstacles and incentives supporting inter-professional collaboration for the management of chronic patient (Table 5 in the Appendix-A1). The administrative burden is an obstacle factor for collaboration with colleagues for 91% of the respondents.
All PCPs who answered the questionnaire are part of a Functional Territorial Aggregation (AFT) and 66% of them often take part to regular meetings on the management of patients with chronic diseases with their AFT colleagues.
PCPs reported never conducting remote visits before the Covid-19 pandemic, while only 16% of specialists had done it. These proportions have slightly changed after the pandemic; indeed, 44% of PCPs now report rare or occasional use of telemedicine, while for specialists, the proportion of its usage increases to 68% (among rarely/occasionally/often users). 32% of the participants would expect to receive an economic incentive for each patient with a chronic disease followed in collaboration with a multidisciplinary group (21% abstain).
Discussion
The survey represents an initial evaluation of collaboration and coordination levels between PCPs and specialists in chronic patient care within Tuscany’s regional healthcare system. Professionals’ perceptions encompassed various integration aspects, ranging from cooperation (sharing of information and mutual support) to system integration (shared goals, values, joint accountability and so on). To the best of our knowledge, this study is pioneering in the Italian context, capturing various information through a survey.
The survey uncovers three key findings. Firstly, differences emerge between PCPs and specialists regarding tools and mechanisms supporting the ECCM in the regional healthcare system. PCPs demonstrate less awareness with diagnostic-therapeutic protocols issued by health authorities due to limited accessibility and guideline attitudes, contrasting with hospital specialists. This is in line with previous literature. 41 Despite this, both groups emphasize the significance of sharing and adhering to clinical guidelines for ensuring quality care for chronic patients. Secondly, perceptions diverge on service integration during care transitions, especially continuity of care from acute to non-acute care. Hospital specialists perceive better coordination strategies, especially for high-need chronic patients, whereas PCPs see lower effectiveness, likely due to their roles in observing hospital-community transitions versus planning and executing them. Despite these differences, both groups advocate for improving the transition process, suggesting that the introduction of an agency for therapeutic continuity has significant potential in this regard. This evidence reaffirms the importance of looking at professional position and its dynamics when changes are introduced into clinical practice and also recall how managerial supports should be draw into professional practice and identity and not vice versa. 42
The survey’s second noteworthy aspect highlights the necessity to reduce organizational barriers and bureaucratic burdens while favouring information sharing systems to support greater multi-professional collaboration. While respondents acknowledge the effectiveness of mechanisms supporting patient transitions, they emphasize the need for organizational enhancements over clinical improvements. Administrative burdens in routine healthcare processes are reported to hinder collaboration, urging the increased use of information systems—such as shared electronic patient records—to aid decision-making and support better population management. However, there appears to be limited enthusiasm for telemedicine in chronic patient care, with both medical specialists and PCPs expressing skepticism about their wide use for the care of chronic patients. Medical professionals might have overlooked organizational barriers when asked to report about the dynamics underlying changes in their professional position, using administrative burden as a “protective shield” 43 to preserve their socially recognized space (autonomy), their expertise and authority 44 This natural tendency towards professional conservation and status quo - together with bureaucracy-induced hurdles – appears to be a significant barrier to changes towards greater inter-professional collaboration.
Finally, our findings speak to the importance of investing in strategies encouraging the formation of stronger peer relationship between PCPs and specialists to improve collaboration (share of common strategies and objectives) and mutual practice. Usually, strategies to influence physician decisions have included pay-for-performance or other extrinsic incentives which have been elusive in their effect or have produced unintended consequences.45–47 More recently, intervention have focused on non-financial incentives that influence physicians’ behaviour such as nudges (e.g., use of defaults, public commitments or information framing) that have successfully prompted higher-value decisions48–50 or peer co-training which motivate physicians to deliver improved care through peer effect. 51 Another important strategy is to keep working toward more advanced inter-organizational performance evaluation systems to enhance shared responsibility about healthcare quality delivered by professionals working in different setting.52,53 From a performance management perspective, it is key to develop tools capable to measure the continuity of care and the integration of healthcare services within the healthcare system and beyond considering for example social assistance. A significant performance assessment tool already in place in 10 different Italian regions is the stave which assesses the value creation process across multiple healthcare organizations adopting the patient perspective for specific clinical pathways, 54 including chronic disease. 55 Nonetheless, the inter-professionals and inter-organizational performance along the care pathway is not yet fully captured.
The CoNtAcT Project, underpinning this study, aims to develop novel governance mechanisms for chronic patient care. It focuses on informal multispecialty physician networks, leveraging collective PCP and hospital specialist experiences. These networks serve as evaluation units, transcending siloed performance management, and fostering inter-professional collaboration. Through benchmarking and peer-performance coupled with the professionals’ point of view it introduces a fresh perspective for monitoring multi-professional care provision to a sizable and high-cost patient population.
This study has some limitations. The non-probabilistic sample and low PCP response rate, likely due to COVID-19, challenge generalizability. On the other hand, the different sample size between the two groups is in line with the Tuscan context (around 2300 PCPs vs 9130 specialists). Additionally, the study reflects the regional healthcare system’s context and culture, limiting generalizability to systems with diverse models and cultures. Thus, caution is warranted in interpreting these study results within these constraints. Especially for changes related to clinical management, the role of organizational settings is important and could influence the outcome of these processes of change. 56
Nonetheless, although this was a preliminary survey which could be improved in terms of questionnaire construct and allowing the analysis of a larger sample, the preliminary results provide a unique and first snapshot of professional perceptions from different care setting with regard to the level of collaboration and coordination between professionals in the delivery of care to chronic patients in a regional healthcare system.
Conclusion
The study provides evidence about perception on the collaboration and integration of interprofessional groups involved in chronic care services. Through the development of this survey, we increase the awareness among policy makers and professionals about the need to develop tools that provides insights on strategic aspects of system integration and inter-disciplinary collaboration (such as context; regulation and guidelines; clinical coordination and cooperation between services; information systems; experience and future perspectives). Results can guide healthcare managers and policy-makers on how to target efforts and resources in the ongoing pursuit of high-performing chronic care model.
Supplemental Material
Supplemental Material - Exploring collaborative practices for chronic disease management: Results from a new survey to primary care physicians and specialists in Italy
Supplemental Material for Exploring collaborative practices for chronic disease management: Results from a new survey to primary care physicians and specialists in Italy by Sofia Longhi, Chiara Seghieri, Francesca Ferrè, Lorenzo Taddeucci and Sabina Nuti in Health Services Management Research.
Footnotes
Acknowledgment
The authors wish to sincerely thank all the partners of the project, along with their dedicated staff, for their valuable suggestions in designing the survey. In particular, we are grateful to Dr. Bellandi and Dr. Arena (AUSL Toscana Nord-Ovest), Prof. De Caterina (AOUP Pisana), Prof. Passino (Fondazione Gabriele Monasterio), Dr. Montagnani (AUSL Toscana Sud-Est), Dr. Bellini (AOU Siena), Dr. Dannaoui (AOU Careggi), Dr. Sergi (AUSL Toscana Centro). A special thanks to Prof. Therese Stukel from the Institute for Clinical Evaluative Sciences (ICES), Ontario, Canada, and Dr. Zeynep Or from the Institut de recherche et documentation en économie de la santé (IRDES), Paris, France, for their insightful expertise and support.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research leading to these results has received funding from Tuscany Region (Italy), within the project CoNtAcT—Accountable networks for chronic populations: new governance mechanisms to promote professional integration and value improvement- Bando Ricerca Salute, 2018.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
Regulation and guidelines: percentages of respondents grouped by primary care physicians and specialists. Clinical coordination and cooperation between services: percentages of respondents grouped by primary care physicians and specialists. Clinical coordination and cooperation between services: percentages of respondents grouped by primary care physicians and specialists. Innovation and quality improvement: percentages of respondents grouped by primary care physicians and specialists. Experiental evaluation and future perspectives: Percentages of respondents grouped by primary care physicians and specialists.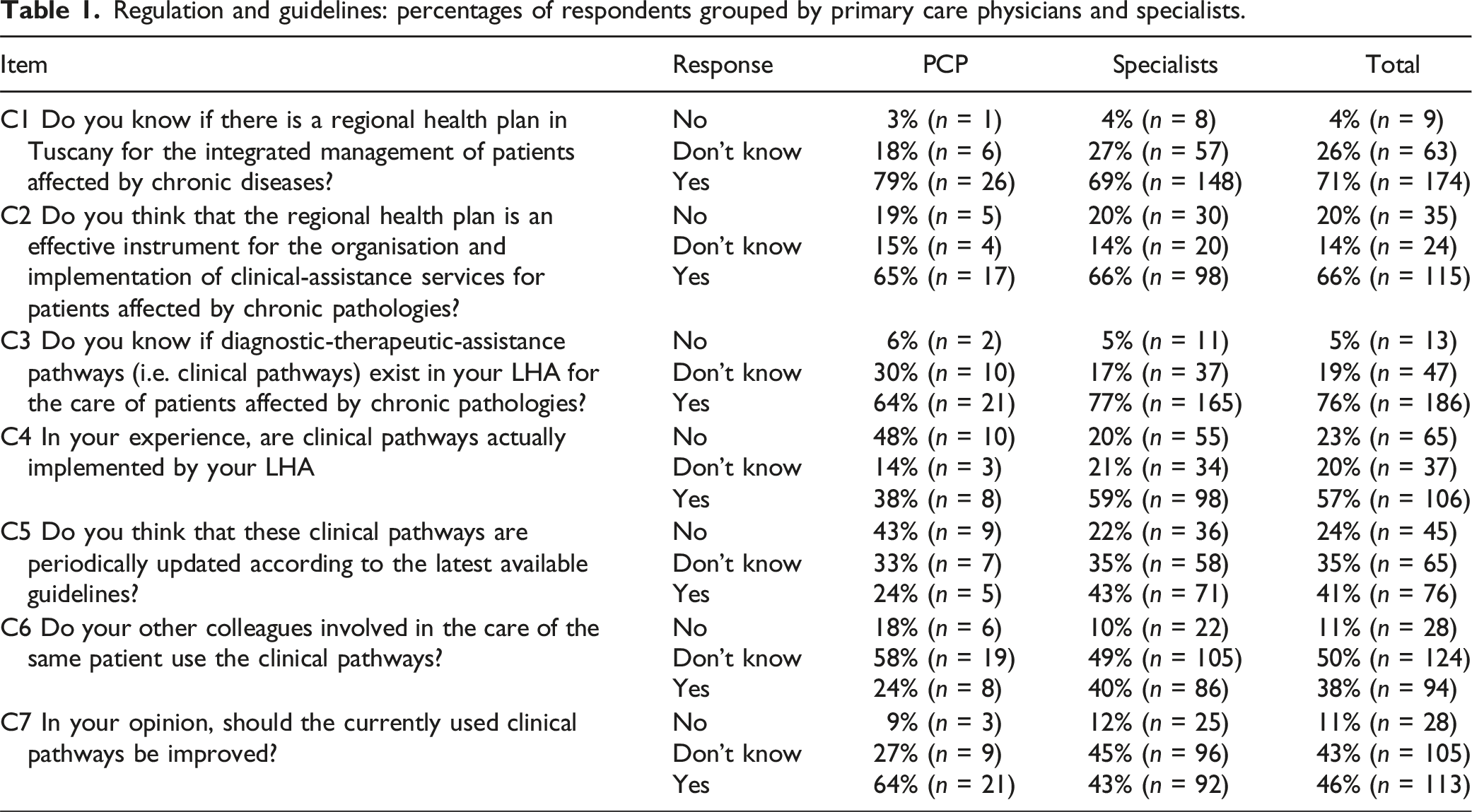
Item
Response
PCP
Specialists
Total
C1 Do you know if there is a regional health plan in Tuscany for the integrated management of patients affected by chronic diseases?
No
3% (n = 1)
4% (n = 8)
4% (n = 9)
Don’t know
18% (n = 6)
27% (n = 57)
26% (n = 63)
Yes
79% (n = 26)
69% (n = 148)
71% (n = 174)
C2 Do you think that the regional health plan is an effective instrument for the organisation and implementation of clinical-assistance services for patients affected by chronic pathologies?
No
19% (n = 5)
20% (n = 30)
20% (n = 35)
Don’t know
15% (n = 4)
14% (n = 20)
14% (n = 24)
Yes
65% (n = 17)
66% (n = 98)
66% (n = 115)
C3 Do you know if diagnostic-therapeutic-assistance pathways (i.e. clinical pathways) exist in your LHA for the care of patients affected by chronic pathologies?
No
6% (n = 2)
5% (n = 11)
5% (n = 13)
Don’t know
30% (n = 10)
17% (n = 37)
19% (n = 47)
Yes
64% (n = 21)
77% (n = 165)
76% (n = 186)
C4 In your experience, are clinical pathways actually implemented by your LHA
No
48% (n = 10)
20% (n = 55)
23% (n = 65)
Don’t know
14% (n = 3)
21% (n = 34)
20% (n = 37)
Yes
38% (n = 8)
59% (n = 98)
57% (n = 106)
C5 Do you think that these clinical pathways are periodically updated according to the latest available guidelines?
No
43% (n = 9)
22% (n = 36)
24% (n = 45)
Don’t know
33% (n = 7)
35% (n = 58)
35% (n = 65)
Yes
24% (n = 5)
43% (n = 71)
41% (n = 76)
C6 Do your other colleagues involved in the care of the same patient use the clinical pathways?
No
18% (n = 6)
10% (n = 22)
11% (n = 28)
Don’t know
58% (n = 19)
49% (n = 105)
50% (n = 124)
Yes
24% (n = 8)
40% (n = 86)
38% (n = 94)
C7 In your opinion, should the currently used clinical pathways be improved?
No
9% (n = 3)
12% (n = 25)
11% (n = 28)
Don’t know
27% (n = 9)
45% (n = 96)
43% (n = 105)
Yes
64% (n = 21)
43% (n = 92)
46% (n = 113)
Item
Response
PCP
Specialists
Total
D1 Do you think that your LHA is managing the transition between care settings of patients with chronic diseases in a coordinated way?
No
63% (n = 20)
21% (n = 45)
27% (n = 65)
Don’t know
3% (n = 1)
23% (n = 48)
20% (n = 49)
Yes
34% (n = 11)
56% (n = 120)
53% (n = 131)
D2 is there in your LHA a process of planning and coordination of hospital discharge for patients affected by chronic pathologies with complex needs?
No
22% (n = 7)
7% (n = 14)
9% (n = 21)
Don’t know
9% (n = 3)
15% (n = 33)
15% (n = 36)
Yes
69% (n = 22)
78% (n = 166)
77% (n = 188)
D5 Do you think that the hospital discharge process should be improved?
No
16% (n = 5)
35% (n = 75)
33% (n = 80)
Yes
84% (n = 27)
65% (n = 138)
67% (n = 165)
D7 Do you coordinate with your colleagues in the management of patients with chronic diseases (e.g. regular meetings, updates, conferences, etc.)?
No
41% (n = 13)
44% (n = 93)
43% (n = 106)
Yes
59% (n = 19)
56% (n = 120)
57% (n = 139)
D8 Do you collaborate with voluntary associations and other organisations in the management of patients with chronic diseases (e.g. care organisations)?
No
78% (n = 25)
66% (n = 140)
67% (n = 165)
Yes
22% (n = 7)
34% (n = 73)
33% (n = 80)
PCP
Specialists
Total
D11_12 when sending patients to a specialist/to their PCP, how often do you write a patient summary?
Never/sometime
50% (n = 16)
11% (n = 23)
16% (n = 39)
Often/always
50% (n = 16)
89% (n = 190)
84% (n = 206)
D13_14When receiving patients from a specialist/ from a PCP, how often do you receive a patient summary?
Never/sometime
22% (n = 7)
94% (n = 201)
85% (n = 208)
Often/always
78% (n = 25)
6% (n = 12)
15% (n = 37)
Item
Response
PCP
Specialists
Total
E1 Do you use the electronic health record as a sharing tool between specialists and GPs?
No
75% (n = 24)
73% (n = 154)
73% (n = 178)
Yes
25% (n = 8)
27% (n = 58)
27% (n = 66)
E3 Can you access data on the services provided by your LHA regarding your patients affected by chronic diseases?
No
69% (n = 22)
37% (n = 78)
41% (n = 100)
Don’t know
6% (n = 2)
14% (n = 29)
13% (n = 31)
Yes
25% (n = 8)
50% (n = 105)
46% (n = 113)
E4 Can you access data on services provided by other LHAs concerning your chronically ill patients?
No
91% (n = 29)
77% (n = 163)
79% (n = 192)
Don’t know
3% (n = 1)
12% (n = 26)
11% (n = 27)
Yes
6% (n = 2)
11% (n = 23)
10% (n = 25)
E5 Do you feel that the clinical and care information available to you in the medical records of your chronically ill patients is complete?
No
53% (n = 17)
56% (n = 118)
55% (n = 135)
Don’t know
22% (n = 7)
15% (n = 32)
16% (n = 39)
Yes
25% (n = 8)
29% (n = 62)
29% (n = 70)
Item
Response
PCP
Specialists
Total
F5 Did you find the training and refresher courses you have attended in the last year useful for your professional development?
No
3% (n = 1)
4% (n = 9)
4% (n = 10)
I’ve never taken part in it
3% (n = 1)
4% (n = 8)
4% (n = 9)
Yes
94% (n = 30)
92% (n = 195)
92% (n = 225)
F6 Do you feel that the administrative burden is an obstacle to collaboration with colleagues?
No
9% (n = 3)
9% (n = 19)
9% (n = 22)
Yes
91% (n = 29)
91% (n = 193)
91% (n = 222)
F7 Did you and your colleagues already carry out remote visits (teleconsultation) to patients before the start of coronavirus?
No
100% (n = 32)
84% (n = 179)
86% (n = 211)
Yes
0% (n = 0)
16% (n = 33)
14% (n = 33)
F9 Would you expect to be financially incentivised for each chronically ill patient followed in collaboration with a multidisciplinary team?
No
19% (n = 6)
51% (n = 108)
47% (n = 114)
Don’t know
13% (n = 4)
22% (n = 47)
21% (n = 51)
Yes
69% (n = 22)
27% (n = 57)
32% (n = 79)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.