
Abstract
Introduction:
The Primary Health Care approach emphasizes service integration and interprofessional (IP) collaboration, recognizing teamwork as an essential component. Despite the evidence being in favor of the application of teamwork, its adoption in primary care (PC) systems remains difficult. In Italy, a recent national policy supports the strengthening of IP teamwork in the “House of Community”—HoC (a model of Community Health Centers), but its implementation needs further evaluation. This study examines how IP teamwork has developed within a HoC in an Italian neighborhood, focusing on its transition toward a more structured collaborative practice and examining the perceptions and experiences of PC professionals.
Methods:
Nine semi-structured interviews and 2 focus-groups were conducted with PC professionals from different PC services. Then, an analytical model was proposed. Data were analyzed using both deductive and inductive approaches.
Results:
Four main themes emerged: rethinking of traditional roles and scopes of practices, leadership/management skills and time/space, IP initiatives, and early perceptions. Based on these findings, an analytical model of teamwork evolution identified 3 interconnected key areas: resource, process, and context.
Conclusion:
The integration of an IP teamwork into the broader healthcare structure can enhance the promotion of a cohesive and collaborative organization, while also recognizing and dealing with its challenges.
Keywords
Introduction
In the last decades, Primary Health Care (PHC) has attracted growing interest as a model of provision of equitable access, continuity of care, and integrated health care. PHC, as defined by the World Health Organization, 1 is a way of delivering health that is based on local socioeconomic determinants with a focus on community orientation and interprofessional (IP) coordination; a key component of this strategy is IP collaboration, which is viewed as necessary in order to improve the quality of care and the performance of services.2,3 Nevertheless, the creation and stabilization of multiprofessional primary care (PC) teams need a strong team identity, clearly defined roles, common objectives, and leadership.4,5 Moreover, the effectiveness of these teams is also influenced by a number of organizational and structural elements, including team membership, communication patterns, and institutional support.6,7
Despite the evidence being in favor of the application of IP teamwork, its adoption in PC systems remains difficult: healthcare is a complex system with many dependent factors and therefore traditional or reductionist models are not sufficient to create effective teamwork.
An increasing volume of research has explored means of improving IP collaboration in PC settings. As an example, a recent scoping review conducted by Sirimsi et al 8 identified 5 broad themes that influence effective teamwork: (a) team acceptance and readiness, (b) shift from individual to team working, (c) collective decision-making and communication, (d) coordination within primary care teams, and (e) integration of different professional competencies. Regarding the timeline needed to build the team, the Interprofessional Collaborative Relationship Building (ICRB) model suggested by Wener and Woodgate identifies 4 consecutive phases: Seeking Help, Initiating Co-location, Integrating, and Cultivating Reciprocity. 9 However, it is worth noting that in a context such as PC, where professionals come from different sectors—prevention, diagnosis, treatment—collaboration may be shaped by culture, background, tools, introducing additional layers of complexity beyond professional competencies. Moreover, IP education has emerged as a promising strategy to enhance collaboration in PC settings. 10 These models offer useful explanations of the processes by which teams can be established, evolve, and maintain collaborative functioning over time; however, their implementation in particular national healthcare is still under-investigated.
In Italy, the need to strengthen the PC services has strongly emerged during the period of the COVID-19 pandemic, 11 when deficits in the PC coordination, IP relationships, and integration with the community health services were revealed. This situation induced the Italian government to enact the Ministerial Decree No. 77/2022, with the aim to restructure the territorial provision of healthcare by establishing PC as the foundational pillar of the healthcare system with a strong focus on multidisciplinary collaboration. An important element of this reform is the establishment of Houses of Community (HoCs)—a new model of community-based and PC centers designed to facilitate collaboration between general practitioners, nurses, social workers, rehabilitation specialists, and other PC professionals. HoCs are designed to increase coordination of services, promote patient-centered care, and build IP collaboration, but their use in practice is still controversial and subjected to deep regional differences, along with the various models of multiprofessional working.
Too little is understood regarding how multiprofessional collaboration within HoCs develops over time, how PC professionals manage role adaptation, leadership structures, and workflow coordination, and what determinants make working together easier or more difficult. Completion of these knowledge gaps is necessary to enable HoCs to fulfill their desired role as effective, community-based PC hubs.
Aim
This study aims to evaluate the development process and evolution of teamwork toward collaborative practice in a PC center (HoC) in an Italian city. Specifically, it examines the perceptions and experiences of PC professionals participating in a multiprofessional team, by focusing on the perceived benefits. Moreover, the study aims at analyzing intermediate outcomes, such as changes in attitudes, knowledge, and skills, and tries to explore the building team relationships.
Methodology
Case Study Description and Study Design
The study took place in a PC center in an Italian city as a pilot, in the period from November 2022 to February 2025. It is a single-center study which employs a qualitative research design and represents a pilot study, as the initial step of a broader project aimed at identifying core elements for a new PHC model and its integration within the organizational and functional structure of the present system—the Local Health Authorities and District. To gain a comprehensive understanding of the evolution of IP teamwork, we adopted a multi-phase methodology, integrating both inductive and deductive approaches, 12 see Figure 1.

Visual representation of the phases.
The initial period of the study included an exploratory phase, where researchers engaged with PC professionals through participant observation. Drawing inspiration from grounded theory, 13 this phase focused on understanding the dynamics of the healthcare environment and exploring emergent themes in the evolving collaboration among different PC services and multiprofessional team’s activities. Supplemented by field notes and unstructured conversations with PC professionals, it provided a solid foundation for subsequent phases.
Building on the preliminary insights, an inductive approach was employed to guide the second phase, which consisted in individual semi-structured interviews (SSIs) with PC professionals. This phase enabled us to further investigate and examine the detailed features of the experiences and perspectives within the members of the multidisciplinary team.
A deductive approach characterized the third phase, which was based on focus groups (FG) to discuss the research findings with the PC professionals. They served for 2 purposes: the validation of the theories emerged in the previous phases of the study and the refinement of the framework.
In the final phase of the study, insights from SSIs and FGs were integrated to define our model of analysis of the teamwork and collaborative practice evolution within the PC center, provide its visual representation and test its validity.
Data Collection, Setting, and Participants
The facility under study is located in Central Italy, in a suburban district of approximately 100 000 inhabitants where there are 2 primary care centers in the process of being developed as HoC. The area is characterized by residential housing and the presence of university students, and a higher proportion of immigrant populations compared to the rest of the city. The facility includes various services, such as general practice, nursing services, social work, rehabilitation, maternal and child health, and specialists. PC professionals were recruited through convenience sampling among PC professionals operating in the services that are present in the facility: in particular, PC professionals who participate in collaborative practices and represent different roles and backgrounds were identified. The final number of participants was therefore determined by the availability of professionals and the observed consistency of emerging insights. While we did not employ a formal rule for thematic saturation, we noted that, after the eighth interview, new data replicated previously identified patterns, suggesting that core themes were adequately represented. The final sample study involved nine participants (seven females), including five general practitioners, one nurse, one social worker, one mental health practitioner, and one physiotherapist. All participants had been employed in the study setting, representing different stages of professional experience. An email detailing the study’s nature and purpose was sent to each identified service. After their confirmation in attending the SSIs, individual meetings were scheduled, during which researchers explained the interview content and obtained written consent for the interview. The 2 investigators (CL and GC) engaged in data collection are external to the PC center staff.
The SSIs guide was created by the research team following a narrative literature review to identify key issues concerning participants’ perspectives on IP collaboration. The individual SSI investigated the significance of the HoC as perceived by the PC professionals, how the team meetings happen, their role and experiences during team meetings, barriers and facilitators for effective IP team meetings, and influence on daily work of the PC professionals and their potential effectiveness on patients’ health and wellbeing, see Table 1. Interviews were audio-recorded, transcribed verbatim, and anonymized before analysis.
Interview’s Guide.

Two FGs were then conducted to discuss the initial data analysis with participants from the SSIs. The goal was to gain a deeper understanding of the findings and collaboratively develop a common framework to address the research question. Specifically, the first served as a discussion on preliminary results regarding the themes, the second followed to share and gain insights on the visual model of analysis, integrating with the aspects emerged by the first. The FGs enhanced triangulation among data collected and themes emerged from the analysis by cross-validating perspectives among participants and allowing researchers to refine interpretations and develop the final model. 12
Data Analysis
Data analysis combined both deductive and inductive approaches. 13 Due to the relatively small sample size (nine SSIs and two FGs), we did not use qualitative software. Instead, we employed a manual coding approach supported by Microsoft Office tools to systematically categorize and refine codes, iteratively reviewed by the research team (CL, GC, and CM). Initially, the first deductive phase performed a theory-driven analysis based on an existing theory as the coding framework of IP collaboration in PC setting. 14 Therefore, the deductive phase focused on five key themes: (1) reevaluation of roles, (2) management and leadership considerations, (3) time and space factors, (4) interprofessional initiatives, (5) and initial perceptions of collaborative care. Codes were extracted from the SSIs content according to these themes and then were grouped. Sub-themes were then inductively developed by refining and organizing related codes, providing a better understanding of specific aspects within each theme, and capturing key dimensions articulated by the PC professionals during the interviews. The relationships among themes, sub-themes, and codes were visualized through an inductive coding table and a thematic map. They were iteratively reviewed by the researchers (CL, GC, and CM), discussed within the FG and further refined through collaborative discussions within the research team. Data from SSIs, FGs, and field observations were triangulated and agreement on the final themes and sub-themes was reached to guarantee accuracy in understanding the insights from the data.15,16
Results
This section contains the findings from the pilot study involving the nine face-to-face SSIs with a range of PC professionals, representing different roles and services. Moreover, the results of the two FGs are described, involving nine and four participants in the SSIs and lasted almost 90 min (the second FG emerged as a need to better focus on some themes). Some interviewees participated to both FGs. Using the 5 themes from Goldman’s framework as a foundation, we refined and reorganized these into 4 main themes. Themes 2 and 3 from the original framework (management and leadership considerations; time and space factors) were integrated and reinterpreted as a single theme within a broader dimension of governance. Additionally, we developed a model of analysis of teamwork evolution, identifying 3 key interconnected areas—resource, process, and context—as a foundation for understanding the team-building process, see Table 2.
Themes and Sub-themes With the Corresponding Number of Interviews Where the Topic Was Discussed.
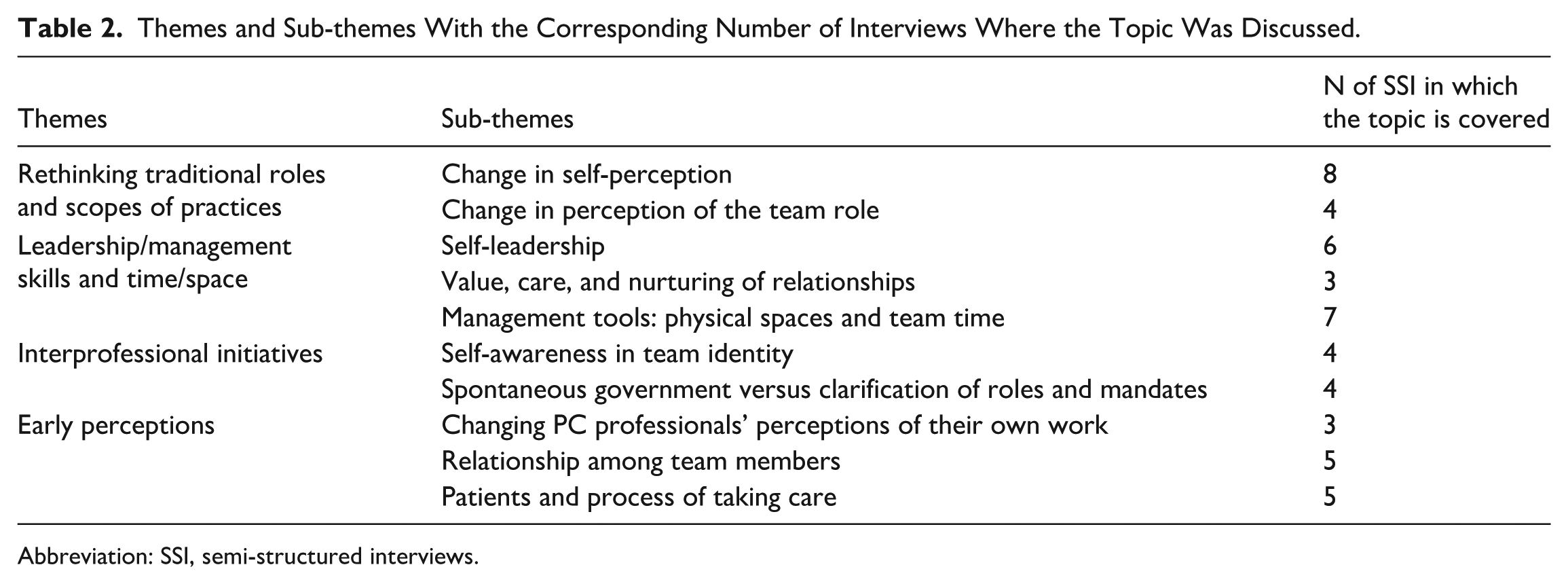
Abbreviation: SSI, semi-structured interviews.
Theme #1: Rethinking Traditional Roles and Scopes of Practices
The SSIs with PC professionals revealed changes and shifts in self-perception and perception of team roles. The following sub-themes were identified and categorized.
•
Eight PC professionals reported that observing the other team members’ roles and professional skills contributed to increase the understanding of their own role as PC professionals and in the multiprofessional team and to raise self-awareness in the experienced limitations in working alone compared with teamwork.
Interviewed 3 stated: “A very important aspect is realizing the importance of observing others in their work. I came to understand the limitations of my professional skills.”
PC professionals reported that increased integration empowers individuals to specialize professionally and provides insight into the team’s dynamics and care pathways.
Interviewed 4 remarked: “we learned a lot from collaborating with others, which influenced our approach (. . .). My role has become more focused on some aspects (. . .).”
Interviewed 6 noted: “I know that I can delegate some tasks (. . .). Consequently, it relieves me of work and sometimes it increases it, because the easier communication also informs me of changes or situations sooner.”
•
In four SSIs participants discussed changes in their perception of team roles. One participant noted that team meetings facilitated collaboration, team dynamics, and communication.
Interviewed 5 reported: “team meetings serve as a platform for collaboration, to overcome the model/way of working of knocking on the doors of the other PC professionals. Then, in the daily work practice, the team dynamic is the real tool that allows one to have the ability to interrupt more fluently.”
Additionally, they reported that the shared experience of the team meeting led to a reinterpretation of the team’s significance by each member, highlighting the importance of a common perspective in the daily practice.
Interviewed 4 noted: “we do not forget the importance of maintaining a common perspective, although each person works for himself.”
Theme #2: Leadership/Management Skills and Time/Space
This domain explores the inputs for team workflow activities, including factors that support team functioning, and promote integration and collaboration.
•
In six SSIs emerged the importance of individual elements, especially in the initial stage of the team meeting participation. They referred to aspects such as attitude toward multiprofessional work, readiness, willingness, and previous experience with multiprofessional or integrated work practices.
Interviewed 1 affirmed: “the willingness to work in this manner was determined by the willingness of all subjects involved.”
Interviewed 5 observed: “everything we built was created because we found people who were willing to work together.”
•
Three PC professionals emphasized the role of nurturing relationships in enhancing cognitive awareness of team dynamics. They reported the importance of recognizing team needs and aligning them with the community needs.
Interviewed 4 reported: “sometimes there are moments of minefields (. . .) because you have to mediate a lot. These moments are overcome by getting to know each other, being together, and being close.”
•
Tools of support—such as physical space, time management, and professional relationships—are reported as essential in seven SSIs in fostering a cohesive team environment and in harmonizing the team objectives with the community’s need.
Referring to the spatial dimension—the proximity in the physical space that hosts team meetings—Interviewed 1 stated: “interprofessional meetings benefit from the space in which they occur.”
PC professionals reported that the proximity of daily workspaces contributes to enhance team identity, share objectives, and promote IP integration.
Theme #3: Interprofessional Initiatives
PC professionals reported that the establishment of IP initiatives was linked to the development of self-awareness in team identity and to the promotion of a collaborative approach to care.
•
Four SSIs highlighted the establishment and co-creation of a team identity and mandate, emerging through reflections and actions originating within the team.
Interviewed 1 expressed: “at some point a name and a surname was given to what we were doing.”
Interviewed 4 remarked: “at some point we recognize ourselves in a group project.”
The participants reported that during the development of team identity, individual professionalism remained present and that, through shared experiences and collaboration, boundaries were perceived less rigid and new team objectives emerged.
•
The sub-theme—present in four SSIs—included the importance attributed to good intentions in the early stages of team development and in long-term sustainability and the importance attributed to the storming and norming stages of the building process. PC professionals expressed a need to clearly define roles and responsibilities, taking into account each member’s background and specific needs.
Interviewed 5: “organization arose spontaneously with need to better define some organizational elements to optimize time and effectiveness interventions.”
Interviewed 1: “Increased encounter complexity (more cases, more professional figures) require government.”
Theme #4: Early Perceptions
In the early phase of team building, it was possible to evaluate team members’ perceptions, which provided a subjective assessment of the team’s effectiveness. The following sub-themes describe the level of change perception:
●
● Relationship among team members: they were crucial for building the team, enhancing open communication and shared decision making.
● Patients and process of taking care/care pathways. PC professionals affirmed that the participation in team meetings have a positive impact on the perceived resolution, containment of burn out, acquisition of a global vision, and problem-solving skills.
Interviewed 3 stated: “a very important thing I would say is that working with others, I realize how essential it is to observe them doing their work.”
Model of Analysis of Collaborative Practice and Teamwork Evolution in the HoC
We identified three key areas—Resource, Process, and Context, —as the foundation for analyzing and understanding the team-building process. In our model, “Resource” encompasses both human resources and governance instruments that guide the team-building process and includes the themes “Rethinking Traditional Roles and Scopes of Practice” and “Leadership, Management, Time and Space”. The former highlights how team members transcend established boundaries to adopt new approaches and practices, while the latter represents governance mechanisms that provide the support to foster alignment and cohesion within the team. The “Process” area focuses on the activities and interactions that transform inputs into outputs. This dimension includes the themes “Interprofessional Initiatives” and “Early Perceptions.” The first is intended to understand the workflow of fostering awareness and promoting collaborative actions during the phases of team building. Meanwhile, the theme “Early Perceptions” reflects how team members develop a better understanding of their work activity and relationship within the team, and how this awareness influences the evolution of collaboration and the overall effectiveness of the team. This dimension, however, requires a continuous analysis and reflection in re-defining common goals and expectations among team members.
The supporting elements critical to the evolution of teamwork are encompassed within the “Context” area, which acts as a catalyst for integration or slowing the evolution. By “Context,” we refer to a comprehensive framework that includes institutional structures, operational setting, and external environment, including regulatory factors and other external influences that shape organizational dynamics, but also professional and individual factors. Together, these internal and external components form the foundation that fosters the creation and effective functioning of a team within an organization. Notably, the context is not static; it is also shaped by the dynamics of the team itself, reflecting a reciprocal relationship.
The proposed model, illustrated in Figure 2, depicts the interconnections among the 3 key areas arranged in a circular flow to represent their continuous and dynamic interactions. Context defines the foundational layer, depicted as the external element. Within the context, resources interact to drive team development. The evolving awareness of roles and responsibilities fosters the integration of professional roles (green oval) and governance mechanism (red oval), enabling the team to function as a unified entity (intersection of the 2 ovals). As a result, the team emerges as a cohesive organizational unit operating within the process flow, ultimately achieving team efficacy (yellow oval). At this point, efficacy refers to the team’s perceived ability to work efficiently and manage tasks effectively. From here, the team re-enters the flow of the context, influencing it and being influenced in return, while simultaneously reinforcing both professional and organizational resources.
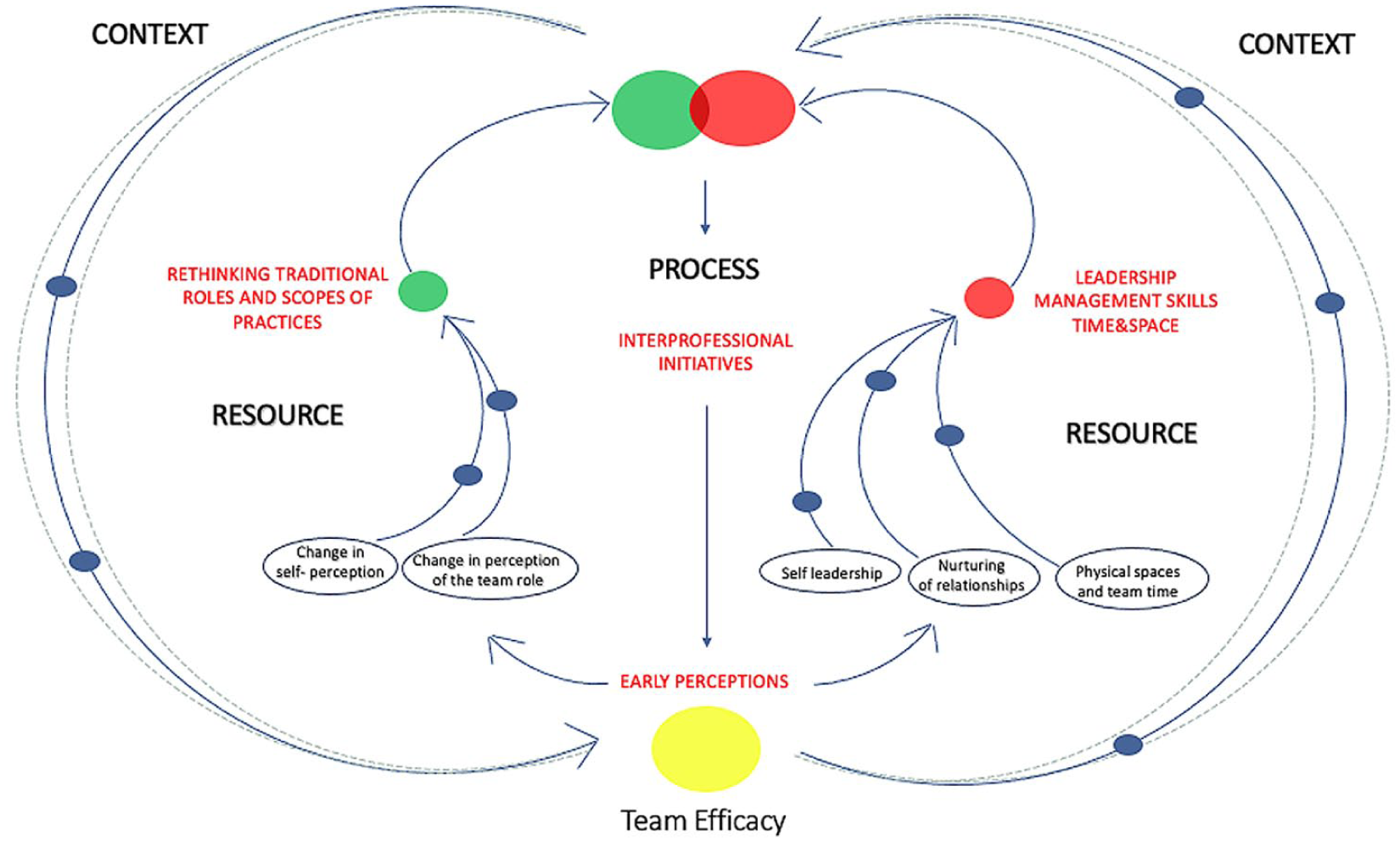
Model for analyzing collaborative practice and teamwork evolution.
Discussion
This study analyzed PC professionals’ experiences within a multiprofessional team, focusing on the evolving roles, team dynamics, and the implications for collaborative practice. We examined participants’ perceptions at both individual and team levels, providing insights into how a model of collaborative practice in PC develops and how it shapes both individual and team perspectives, professional identity and leadership. Our findings identified four themes: the rethinking of traditional roles and scopes of practices, the context—leadership, management skills and time and space, IP initiatives, and early perceptions toward teamwork. We also identified three key areas as the foundation for analyzing and understanding the team-building process: resource, process, and context. These findings highlight how collaboration among PC professionals play an essential role in shaping team identity and establishing shared norms within a framework of self-management and individual leadership. The results also underscore the strong value PC professionals place on IP collaboration, which is enhanced by internal organizational changes designed to facilitate knowledge sharing and foster more cohesive teamwork.
In our case study, key attributes of complexity theory are represented. The theme “Rethinking traditional roles and scopes of practice” highlights Complex Adaptive System’ characteristics such as self-organization, agent interactions, emergence, non-linearity, and the interplay of relationships. 17 Indeed, the SSIs described the team as a space for rethinking and reassessing roles and fostering integration among services. The professionals’ tendency toward adopting a new collaborative interaction model benefits from their personal approach. In the early stages of the team building process, PC professionals personal approach resulted in the development of a bottom-up team-building strategy. The analysis revealed a key motivation into their readiness to embrace change, including in beliefs, attitudes, and intentions toward organizational change. PC professionals showed a strong willingness to engage in this process, recognizing the importance of new work practices as a primary stimulus that enhances commitment and supports team-building efforts. 18 Individual dimensions serve as motivational levers in initiating and supporting the team-building process.
Another finding highlighted in our study is the importance of relationships and communications as pivotal factors in the team-building process, influencing both individual perspectives and the broader organizational dynamics. The interviews reported how personal roles and team roles are evolving through close relationships and communication with others. This evolution is bidirectional, enhancing self-awareness and strengthening emotional intelligence, which acts as a catalyst for change. These findings are supported by other analyses indicating that positive relationships with change agents increase individuals’ readiness to embrace change.6,9 Transformative change that deeply influences attitudes, cognition, and behavior is driven by interaction and social relationships. Behavioral science and social network analysis highlight emotional intelligence as a significant influence on professionals. 19 Self-awareness and team identity, which contribute to the development of a collective team consciousness, are crucial throughout the process of collaborative practice development. In this context, the ability to delegate becomes of primary importance, as professionals undergo a cognitive shift driven by a clearer understanding of their roles within the team. Indeed, self-awareness and team identity serve as primary drivers for the development and success of IP initiatives, which have the potential to profoundly reshape decision-making processes. By shifting responsibility from individual actors to cohesive teams, these changes promote a more unified approach to problem-solving and inter-organizational collaboration. 20 This evolution reflects the principles of team learning, emphasizing the utilization of collective intelligence to drive improvements in outcomes and foster innovation. 21 This perspective highlights individuals’ perceptions, experiences, and their intrinsic value in team dynamics.
Moreover, the analysis revealed a tension between two key aspects of the leadership structure: the informal emergence of leadership within the team and the necessity for formally defining roles and responsibilities. For the team evolution, it also emerged the potential benefit of the presence of professionals with specific skills in group leading to enhance goal definition and methodology. 22
Traditionally, leadership is handled as a tool for influencing workers’ behavior, but we encourage to consider it as the outcome of dynamic human interactions. 23 These dynamics highlight the dual forces shaping the team building: on one hand, there is a recognition of the importance of leadership within the team and the broader institutional framework; on the other hand, there is a lack of clarity regarding what “leadership” entails in this context. As part of team building, “relationship-oriented-self-leadership” integrates the principles of relationship-oriented leadership with self-leadership practices to enhance team behavior effectively. Relationship-oriented leadership focuses on building strong relationships and creating a supportive environment within the team. 24 Self-leadership, meanwhile, focuses on individuals taking personal responsibility for their actions and behaviors, highlighting self-awareness, self-regulation, and self-motivation. 25 By applying relationship-oriented principles to their own behavior, team members can enhance interpersonal connections and contribute positively to the team environment. 20
Additionally, in accordance with the Interprofessional Collaborative Relationship-building Model (ICRB), 9 the analysis revealed a strong emphasis among team members on collaboration, facilitated by the need for help among PC professionals and the physical proximity.
Our findings revealed that PC professionals are experiencing a period of change regarding how they are recognized by the healthcare organization they belong to. Recent Italian legislation, exemplified by Ministerial Decree No. 77/2022, officially recognizes multiprofessional teams as essential to healthcare delivery within HoC. However, the definition of organizational framework for IP teams in PC is still in progress. Early discussion has been started on developing new professional roles, highlighting the importance of accountability, responsibility, and regulatory compliance when navigating professional boundaries. 26 Regulation in this context ensures adherence to safe practices and professional standards. Integrating skills across professional boundaries with institutional recognition represents a well addressed theme in literature 27 and emerged in our case study while discussing IP initiatives with PC professionals. This point could partly explain why some services, such as prevention service, are not yet part of the team studied in our study and reflect the risk of maintaining a siloed organization in the current phase.
For these reasons, structural measures are necessary to ensure the success of the implementation of collaborative practices in PC settings, considering the following points: clarification of roles and the leadership structure within the teams; strengthening of institutional support; definition of IP education and training programs, providing the continuous professional development focused on teamwork, leadership, effective communication, and shared decision-making. However, reshaping these boundaries would demand an adjustment period that could lead to conflicts, considering the complexities involved in managing effective organizational change, requiring proactive regulatory frameworks to address these challenges and to support and empower multiprofessional teams while ensuring safe and effective healthcare practices. 28
Limitations and Strengths
Several aspects of the study are important and deserve to be emphasized: the study is part of a larger project that aims at investigating and identifying key elements for a new model of PHC, helping to provide insights for policy makers. The present work includes different qualitative research methodologies and focuses on different PC professionals, providing a wide range of perspectives and experiences. In addition, the focus on changes in attitudes, knowledge, and skills helped understand the impact of multi-professional teamwork on PC professionals, with potential practical implications for the promotion of effective multi-professional teams.
Despite these strengths, the study has some limitations. Firstly, the limited sample size: being a single center study, with only nine interviews participated, represents a pilot study, which may limit the generalizability of the findings to other healthcare contexts and the understanding of different perspectives. Moreover, the inclusion of other PC professionals in the sample is crucial for future development. Furthermore, the study focused on perceived benefits which do not necessarily indicate real improvements in clinical practice or patient outcomes. We suggest that future research will address analysis of changes in outcomes over time, and the inclusion of other centers and experiences.
Conclusions
The present study illustrates the evolving process of collaborative practice and the evolution of teamwork in a PC case study. We propose a framework and a model of analysis that may help to explore the topic, including the subjective perspectives of PC professionals. The integration of teamwork and collaborative practice into the structure of a healthcare organization can encourage moving beyond the traditional silos approach to professionalism, for a more integrated and cohesive healthcare service. Further research is important for a better understanding of these new processes.
Footnotes
Acknowledgements
We sincerely thank all the primary care professionals who participated in this study and shared their time and experiences. Their insights and contributions were essential to the development of this research. We also acknowledge the support of the institutions and services that facilitated the study’s implementation.
Ethical Considerations
Ethical approval was obtained from the Research Ethics Committee of the Tuscany Region, Area Vasta Centro (clearance number: prot n.CDSP0619)
Consent to Participate
Participants gave written informed consent for participating in interviews.
Author Contributions
C.M. and G.C. contributed to the conceptualization and design, coordinated data collection, and contributed to data analysis. They drafted the original manuscript and contributed to all stages of revision and editing. C.L. participated in data collection and contributed to data analysis and manuscript review. A.G. and M.d.R conducted formal analysis of the qualitative data and contributed to interpretation of findings and critical revision of the manuscript. C.L. supported methodological development and contributed to the review and editing of the manuscript. G.B. supervised the study at all stages, contributed to conceptualization and interpretation, and participated in reviewing and editing the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: we acknowledge co-funding from Tuscany region project entitled “Da Casa della Salute a Casa della Comunità” (DGRT n.1125/2021). The project was approved following “Linee di indirizzo per la realizzazione dei progetti regionali sulla sperimentazione di strutture di prossimità,” Annex 1 to the “Intesa tra il Governo, le Regioni e le Province autonome di Trento e Bolzano, Rep. Atti n. 134/CSR del 4 agosto 2021.” The views and opinions expressed are only those of the authors and do not necessarily reflect those of the Tuscany Region or the Italian Government. Neither the Tuscany Region nor the Italian Government can be held responsible for them.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the nature of the study, the full interview transcripts are not publicly available. Anonymized data may be made available upon reasonable request to the corresponding author.