
Abstract
Introduction
Coexistence of multiple medical diagnoses, referred as multimorbidity, is common in aging populations (Rijken et al., 2018), and nearly one-third of this population suffers from it (Hajat & Stein, 2018). As a critical part of healthcare providers, nursing professionals play an important role in patient care with knowledge application for patients with variety of medical problems (Cohen & Boni, 2016). As one of nursing specialties, holistic nursing could provide a unique and distinct intervention with knowledge of complementary and alternative therapies to care patients with multimorbidity (Frisch, 2001). Holistic nursing is defined as “all nursing practice that as healing the whole person as its goal” (Thornton, 2019) and it approaches patients as integrated, adaptive system, interconnected with all systems (AHNCC, 2017). Clinically, a holistic nurse may implement a holistic intervention plan to reach a patient's holistic health (AHNCC, 2017).
As a part of the management for multimorbidity from a holistic healthcare perspective, the deep breathing technique alone or as an essential part of the mind-body interventions such as Tai Chi, Yoga, and Ayurveda has often been used by practicing holistic healthcare professionals including holistic nurses (AHNCC, 2017; Liu, Miller, et al., 2022; Thornton, 2019). These mind-body interventions emphasize static and dynamic postural control, as well as an integration of body movement with deep breathing (Bao et al., 2020). Deep diaphragmatic breathing (DDB) is a commonly used exercise for people with or without medical conditions (Hamasaki, 2020; Ma et al., 2017). DDB involves slow and full contraction of the diaphragm with expansion of the belly during inspiration, and slow and full contraction of the abdominal muscles with reduction of the belly during expiration. During the time, the practitioner can place one hand on the abdomen and the other hand on the chest to ensure the abdominal puffing up with deep inspiration and sinking-in with deep expiration (Bao et al., 2020; Hamasaki, 2020). DDB can be practiced in supine, sitting, and standing positions, and can also be performed with other exercises like Tai Chi or Yoga (Bao et al., 2020; Hamasaki, 2020; Liu et al., 2016; Ma et al., 2017). This approach can be used for healthy as well as individuals with multimorbidity.
Early studies have revealed that the DDB is able to benefit patients with pulmonary, mental, gastrointestinal (GI) dysfunctions, and many other physiological problems (Hamasaki, 2020; Kocjan et al., 2017). The immediate obvious effect is to increase the tidal volume, oxygen saturation, and efficacy of pulmonary functions (Mendes et al., 2019), which makes the DDB useful for patients with chronic obstructive pulmonary disease, asthma, postoperative pulmonary function, and cardiorespiratory performance in open-heart surgery patients (Hamasaki, 2020). Also, BBD is widely applied in people with mental dysfunctions and stress disorders, including post-traumatic stress disorder, motion disorders, phobias, and other stress-related emotional disorders (Ma et al., 2017). In relation to the GI system, it is reported that the deep breathing may improve patients with gastroesophageal reflux disorder (Eherer et al., 2012) and even irritable bowel syndrome (Kayuri et al., 2015). Further, DDB can modulate the intra-abdominopelvic pressure (IAP) to assist the individual's physical and physiological behaviors like body stability, coughing, sneezing, urination, defecation, and parturition (Hamasaki, 2020). These DDB effects could be enhanced when it is combined with other mind-body exercise programs (Hamasaki, 2020; Ma et al., 2017), as the DDB is an essential part of these exercises for both cognitive and physical improvements (Bao et al., 2020; Hamasaki, 2020; Liu et al., 2016; Ma et al., 2017).
According to the American Holistic Nurse Association (AHNA) and American Holistic Nurses Credentialing Corporation (AHNCC), holistic nursing is able to advance the holistic healthcare by using the best available evidence including theories and research findings, to guide holistic nursing practice decisions throughout the holistic nursing practice (AHNA, 1998; AHNCC, 2017). Although the DDB is a promising intervention for holistic health maintenance and improvement, up to date, the mechanism for the effectiveness of DDB has not been clearly explained. Focusing on the anatomical and biomechanical approaches in consideration of the DDB may offer improved understanding of the DDB mechanism when providing this intervention and patient education for patients.
Method
Diaphragm and DDB-related literatures that investigated the diaphragm's anatomical characteristics and DDB's biomechanical effects on physical and physiological activities were searched. The following sources were included in the literature search process: Pubmed, Scopus, Medline (US National Library of Medicine), the Physiotherapy Evidence Database (PEDro), the Cochrane Controlled Trials Register (Cochrane Library), and Cumulative Index of Nursing and Allied Health Literature (CINAHL), from last the 15 years until May 2022. The search strategy used the following keywords and variations: diaphragm, respiratory diaphragm, pelvic floor, pelvic diaphragm, larynx, laryngeal diaphragm, DDB, deep breathing, deep abdominal breathing, intraabdominal pressure, IAP, physical activities, physiological activities, anatomy, morphology, neuroanatomy, neuroscience, body mechanics, and biomechanics. Published reviews and all relevant studies and their reference lists were also reviewed manually in search for other pertinent publications.
Results Descriptions
With literatures searched, reviewed, and analyzed, hereby we described the diaphragmatic anatomy; effects of deep breathing on digestive system, cardiopulmonary system, nervous system, physical and physiological activities, and mind-body exercise; as well as the neural coordination of DDB-related activities.
Anatomy of Diaphragm
The diaphragm is the most important muscle in the human body (Anraku & Shargall, 2009; Nason et al., 2012). Its functionality affects all muscles and vital organs in the body because they require oxygen to function (Bordoni et al., 2018; Kocjan et al., 2018). The diaphragm not only plays a role in respiration but also has many roles affecting the health of the body. As shown in Figure 1, anatomically, the diaphragm curves up like a dome (Kocjan et al., 2017). The central portion of the diaphragm is the central tendon with an opening called the vena cava hiatus for inferior vena cava to pass through at the T8 level, and the peripheral portion is the muscle that attached to the lower six ribs as the costal portion, to the inferior sternum and xiphoid process as the sternal portion, and to the lumbar vertebrae as the vertebral portion. There are two openings on the peripheral muscular diaphragm: the esophageal hiatus near the right crus at the left part of the diaphragm at the T10 level for the esophagus and vagus nerve plexus to pass through, and the aortic hiatus on the vertebral column between the left and right diaphragmatic crura at the T12 level for descending aorta, thoracic duct, and azygous vein to pass through. Because of the muscle attachments and structural characteristics, the diaphragm's lowest attachment is anteriorly to the xiphoid process at the T6 level; and is posteriorly to the anterior surface of the vertebral column via the median arcuate ligament at the T12 level and two diaphragmatic crura at the L1-3 levels (Figure 1). Mechanically, during inspiration, when the peripheral muscular portion of the diaphragm contracts to pull the central tendon downward, the force made by the diaphragmatic muscle makes the abdominal cavity puff up anteriorly and inferiorly. While during expiration, the diaphragm moves back up to its original position automatically at resting time or forcefully when performing deep breathing-out.
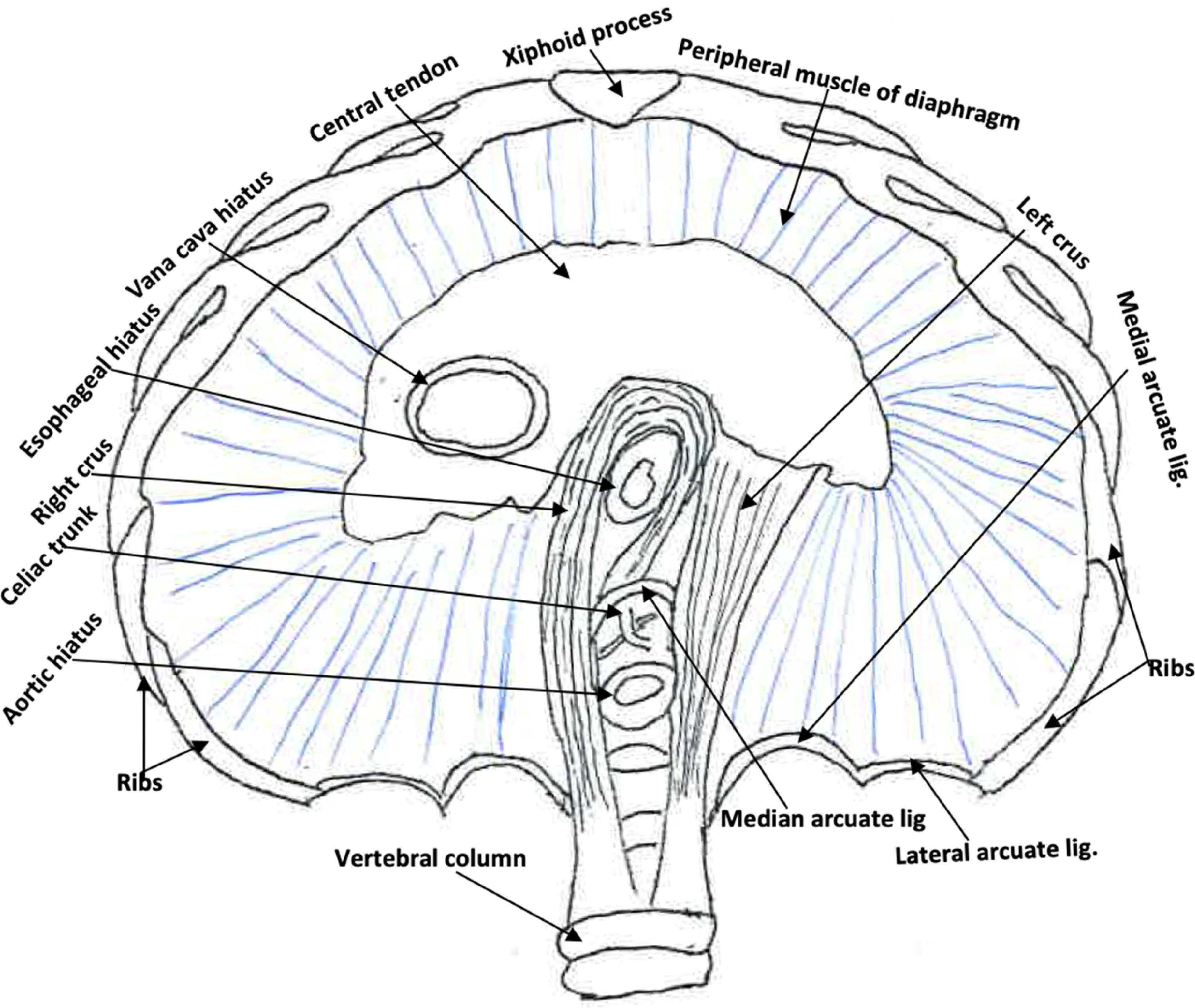
Inferior view of the diaphragm includes the central tendon, peripheral muscle, as well as three hiatuses (vena cava, esophageal, and aortic) for inferior vena cava, esophagus, and descending aorta to pass through. The esophageal hiatus is primarily surrounded by the right crus of the diaphragm as a sphincter-like structure at the lower end of the esophagus. The lowest points of the diaphragm are attached anteriorly to the xiphoid process at T6 vertebral level, posteriorly to the anterior surface of the vertebral column via the median arcuate ligament at the T12 level and two diaphragmatic crura at the L1-3 levels; and laterally on either side to the lower edge of the rib cage.
The two muscular diaphragmatic crura attached posteriorly to the sides of the L1-3 vertebral bodies and intervertebral disks with the right one larger than the left one (Anraku & Shargall, 2009). There are one single median arcuate ligament and two paired medial and lateral arcuate ligaments. The median arcuate ligament is an “n-shaped” fibrous structure that connects two crura over the aortic hiatus at T12 vertebral body level. The medial and lateral arcuate ligaments are located symmetrically on either side of the vertebral column with the medial ones from the L1/L2 vertebral body to L1 transverse process; and the lateral ones from T12 transverse process to the midpoints of the 12th ribs (Nason et al., 2012).
The left and right diaphragm receive innervation from the left and right phrenic nerves respectively. These phrenic nerves originate from lamina IX of C3-5 cervical spinal nerves and travel through the neck to enter the thorax and continue down anteriorly to the pulmonary hilum along left and right lateral surface of the pericardium individually before reaching the diaphragm where they arborize the superior and inferior surfaces of the diaphragm (Nason et al., 2012). The right phrenic nerve pierces the diaphragm near the lateral edge of the vena cava hiatus, and the left phrenic nerve pierces through the diaphragm near the tip of the cardiac apex. In the subdiaphragmatic region, both the left and right phrenic nerves form one or more phrenic ganglia to connect with the prevertebral sympathetic ganglia and the adrenal gland (Bordoni et al., 2018; Loukas et al., 2016). Therefore, the phrenic nerve contains somatic motor, sensory, and sympathetic fibers for the diaphragm. Its motor and sympathetic fibers control the diaphragmatic voluntary and autonomic movements respectively. Sensory innervation (pain and proprioception) at the central tendinous part is innervated by the phrenic nerves, while the peripheral portions are innervated by 6th to 11th intercostal nerves. The motor outputs of the phrenic nerve control breathing, but also regulating swallowing, voicing, spitting, emesis, and coordinating with pelvic floor muscles for defecation, urination, and even sexual activity (Bordoni & Zanier, 2013; Nason et al., 2012; Pickering & Jones, 2002).
Mechanically, the direction of the diaphragm movement during inspiration in the upright posture is toward anteriorly and inferiorly. The gravity plays an assistive role in pulling the diaphragm inferiorly in standing instead of supine position. Hence, this explains why the diaphragm is higher when one is in supine position than in standing (Panicek et al., 1988), and why the downward diaphragmatic movement during inspiration is much easier in standing than in supine. A rehab professional in clinical settings may use this unique characteristic of the diaphragm to design a progressive strengthening exercise program for the diaphragm.
DDB on Digestive Organs
The superior surface of the diaphragm merges into the pulmonary pleura, whereas the inferior surface merges into the peritoneum making the upper roof of the abdominal cavity (Bordoni & Zanier, 2013). In the abdominal cavity there are many ligaments (Table 1), primarily formed by peritoneal fold or thickening, that connect the internal digestive organs to the undersurface of the diaphragm, including esophagus, stomach, duodenum, colons, liver, and spleen (Bordoni & Zanier, 2013; Kocjan et al., 2017; Panicek et al., 1988). It is likely that with deep breathing, these ligaments may assist the movement of the attached internal organs to prevent potential adhesion among these organs, and enhance the peristalsis of the GI tract.
Ligaments Attached to Diaphragm in the Abdominal Cavity (Kocjan et al., 2017; Panicek et al., 1988)
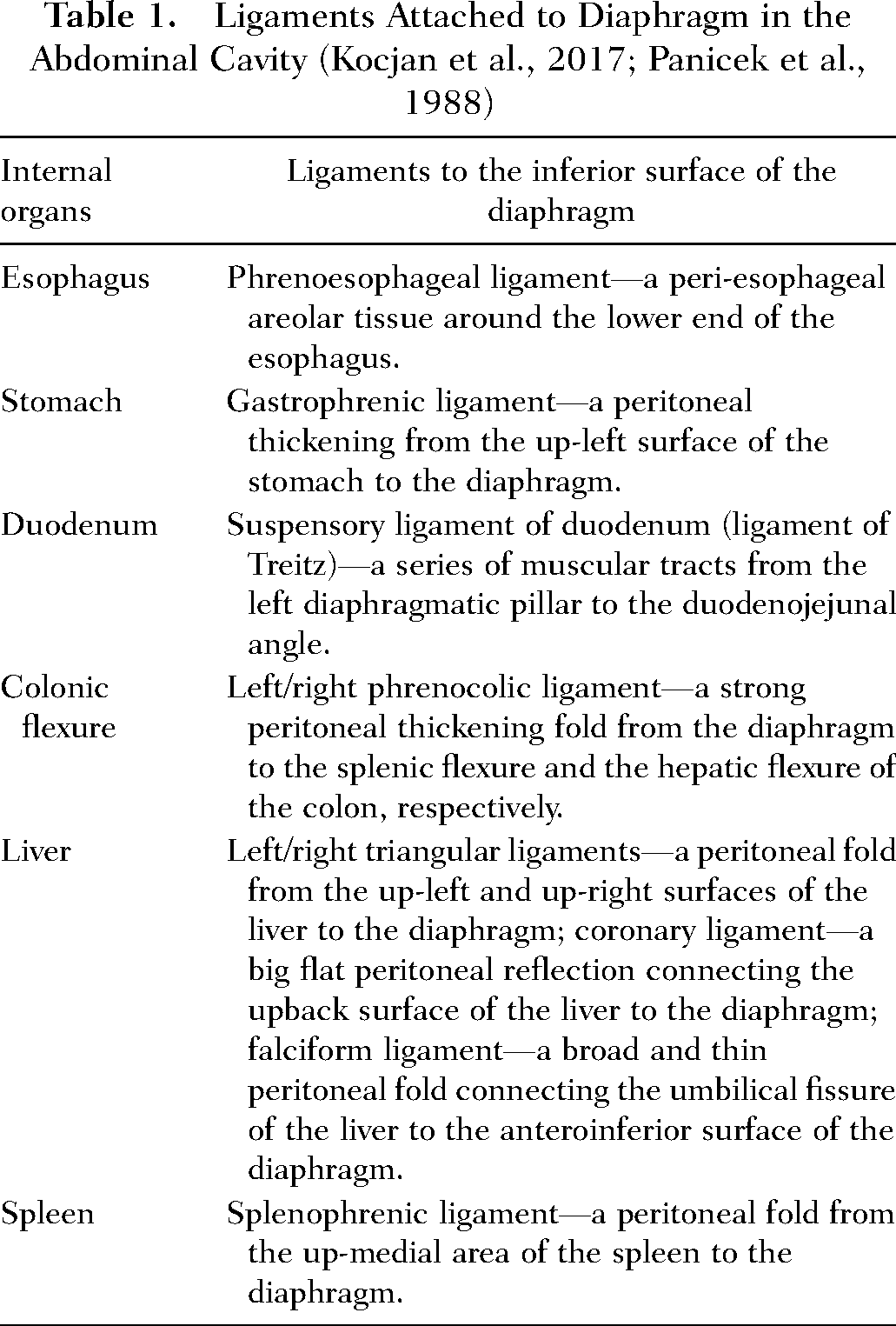
Specifically, to the lower esophagus, the internal lower esophageal sphincter is an intrinsic smooth muscle structure of the distal esophagus at the gastroesophageal junction or the esophageal hiatus area (Mittal & Goyal, 2006; Richter, 2013). At the junction, a striated muscle structure, made by fibers contributed from either the right crus in 60% of individuals or from both the left and right crura in 40% of individuals, circles around the internal sphincter to act as an external esophageal sphincter or diaphragmatic sphincter of the lower esophagus (Anraku & Shargall, 2009; Mittal & Goyal, 2006; Richter, 2013). These two internal and external sphincters together make the unique circumferential myo-architecture to “hug”, “noose”, or “squeeze” the lower esophagus where it meets the stomach (Richter, 2013; Zifan et al., 2017). This “noose” configuration functions to maintain tonic closure and augment reflex closure of the sphincter mechanism at the gastroesophageal junction during inspiration and other physical activities, which can potentially increase the pressure gradient across the sphincter (e.g., coughing, abdominal compression, and straight leg raising) (Mittal & Goyal, 2006; Richter, 2013). Dysfunction of the mechanism may lead to the gastroesophageal reflux disease (GERD) or dysphagia (Mittal & Goyal, 2006). Based on the striated muscle characteristics of this extrinsic lower esophageal sphincter, Eherer et al. (2012) conducted a prospective randomized controlled trial with the DDB as the intervention in patients with diagnosis of GERD. This 4-week study with 9-month follow-up demonstrated significant improvements in quality of life, value of pH-metry, and score of proton pump inhibitor usage (an indicator of GERD) in the intervention group than the control group.
The phrenoesophageal ligament is an areolar structure that bridges the space between the distal esophagus and the margins of the esophageal hiatus of the diaphragm (Apaydin et al., 2008; Kwok et al., 1999). It appears to have an up-leaf arising from the endothoracic fascia and a low-leaf from the transversalis fascia, composing of abundant collagen and elastic lamellae (Kwok et al., 1999). This ligament limits upward displacement of the esophagus into the thorax, and draws the esophagus back into position while minimizing circumferential traction on the lower esophageal ligament (Apaydin et al., 2008; Richter, 2013). However, it should be noted that this phrenoesophageal ligament does not contribute to the sphincter pressure profile (Richter, 2013). With all of these said, it is understandable that the DDB might play a crucial role in preventing gastroesophageal reflux, since the voluntary DDB may strengthen the striated diaphragmatic muscles including its two crura. When the DDB practiced with resistance, the diaphragmatic muscle including two crura could get stronger and more aerobic, which could lead to the stronger external esophageal sphincter to minimize the gastric reflux into the opened trachea and consequently prevent the gastroesophageal reflux disorder.
DDB on Cardiopulmonary Organs
DDB affect both cardiovascular and respiratory systems. There are ligaments that connect the heart and lungs to the diaphragm (Bordoni & Zanier, 2013). The pulmonary ligament, also called the inferior pulmonary ligament, is a visceral-parietal pleural reflection that connects the base of lungs to the superior surface of the diaphragm; while the phrenopericardial ligament connects the pericardium to the diaphragm as well (Panicek et al., 1988). Studies have revealed that the deep breathing is able to increase the intrathoracic capacity and enhance ventilation efficiency (Russo et al., 2017). Very likely these may be caused by increasing alveolar recruitment (Urell et al., 2011), expanding the lung tissue (Urell et al., 2011; Westerdahl et al., 2005), activating the hypoglossal nerve to retract the tongue (Bordoni et al., 2018), and/or widening the respiratory tract (Fregosi & Ludlow, 2014). So, during the deep diaphragmatic inspiration, the downward movement of the diaphragm along with the inferior pulling on the base of the lungs by the pulmonary ligament could cause increased negative pressure in the thoracic cavity and in the lung tissues, as a result, get more air into the lungs for ventilation.
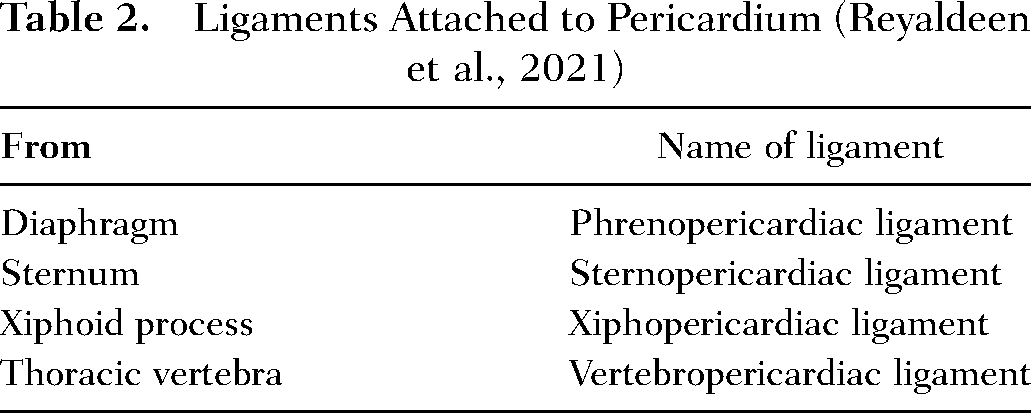
DDB may affect the cardiovascular flow through the hiatuses on the diaphragm and ligaments attached on the pericardium. During inspiration, the vena cava hiatus is stretched and enlarged and thus facilitates blood flow from abdomen back to cardiac chambers (Anraku & Shargall, 2009; Nason et al., 2012); while the aortic hiatus is retrocrural and the diaphragmatic contractions do not affect this hiatus too much (Nason et al., 2012). Anatomically there are four ligaments (Table 2) attached to the pericardium from the superior surface of the diaphragm, sternum, xiphoid process, and thoracic vertebrae (Panicek et al., 1988; Reyaldeen et al., 2021). During inhalation, the diaphragm moves inferiorly, the xiphoid and sternum move superiorly and anteriorly, while the thoracic vertebral column extends slightly. The pulling forces from these ligaments could expand the pericardial cavity and make more negative intra-pericardial pressure. Thus, the vacuum action due to both intrathoracic and intra-pericardial pressures could be the primary driving factor or the fundamental mechanism to facilitate blood flow to the heart; to increase coronary perfusion, ventricular filling, and stroke volume; and subsequently to enhance circulation to vital organs all over the body (Convertino, 2019; Russo et al., 2017). This may indicate that DDB could be a good choice for reducing cardiovascular dysfunction. For example, increased coronary perfusion might be able to decrease the occurrence of coronary artery disease.
Ligaments Attached to Pericardium (Reyaldeen et al., 2021)
DDB on IAP and Related Physical and Physiological Activities
DDB is able to improve a person's balance and trunk stability, especially during sudden dynamic voluntary limb movements (Kocjan et al., 2017). During physical activities like weight holding and lifting, walking on a narrow beam or a straight line, or physiological activities like coughing, sneezing, shouting, urinating, defecating and even ejaculating or parturition, the trunk stability with increased pressure within both the chest cavity and the abdominopelvic cavity is required. In a 3D view, the chest cavity is basically a rigid space surrounded by bones, superiorly connected with mouth and nose through the larynx, and inferiorly supported by the diaphragm. Comparatively, the abdominopelvic cavity is softer but can be rigid space when the IAP is increased. This cavity is encircled by the diaphragm superiorly, the pelvic floor inferiorly, the vertebral column and paraspinal muscles post-centrally, and the abdominal muscles in all other sides around the cavity. Such an anatomical configuration makes the chest cavity like a rigid culvert while the abdominopelvic cavity like a vacuum bag on a rod (analogue to the vertebral column). This “bag” can become a rigid but hollow structure when the air pressure is built high enough in the abdominopelvic cavity. To ensure the “bag” functions well, the vertebral column (the rod as the analogue on a vacuum) has to be stable, and the muscles surrounding the “bag” have to be strong enough to maintain the bag's hollow rigidity. Therefore, we can see how significant role the diaphragm, followed by the pelvic floor, and the larynx (particularly the rima glottidis between two true vocal folds) can play in regulating the air pressure changes in order to meet different physical and physiological needs (Figure 2).
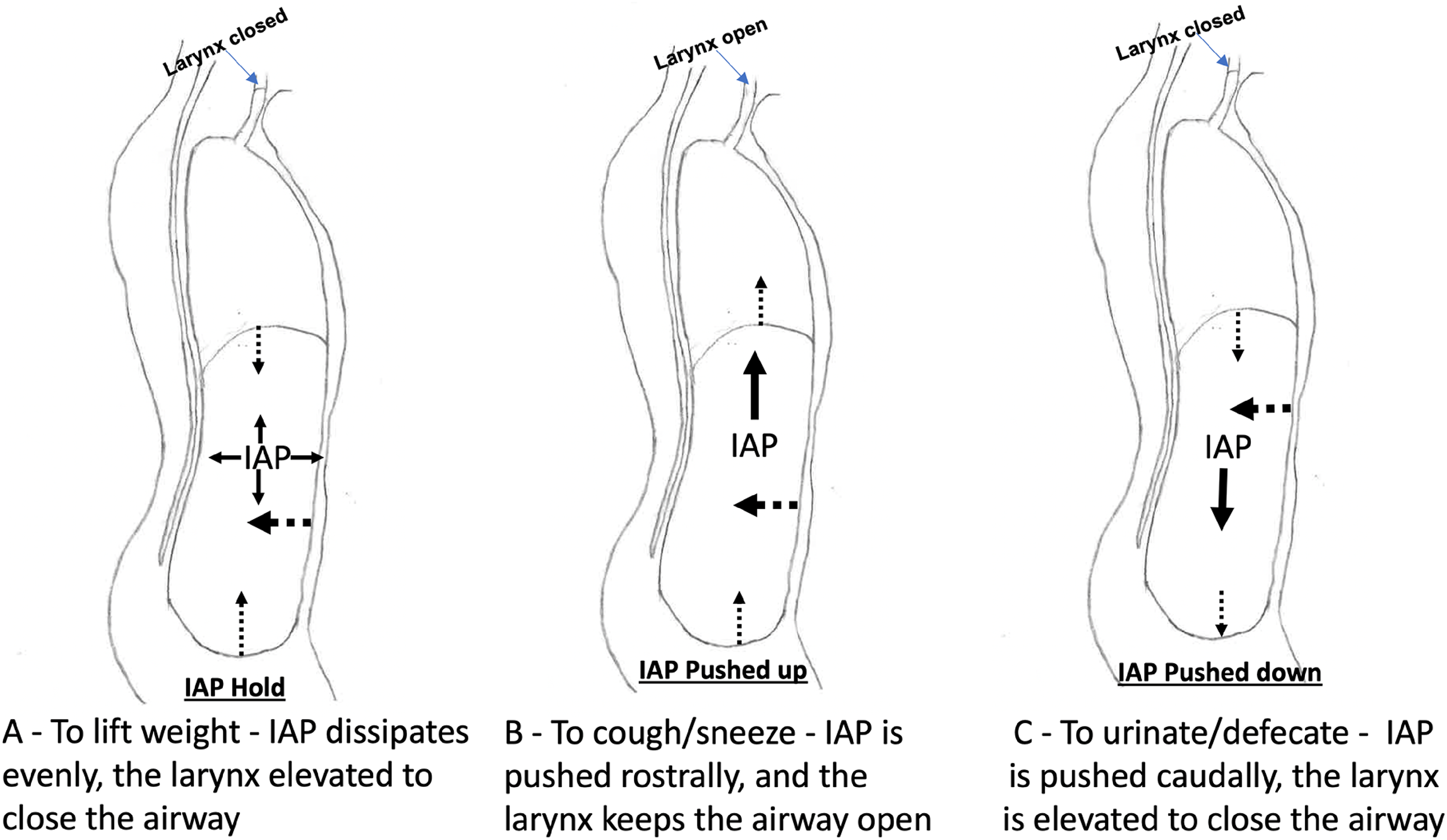
Changes of intra-abdominopelvic pressure (IAP) for different activities. (A) IAP hold time, (B) IAP-pushed upward time, and (C) IAP-pushed downward time. Thick dotted arrow: direction of pressure from abdominal muscles; thin dotted arrow: direction of diaphragm and pelvic floor muscles, respectively; solid arrows: direction of IAP.
During the quiet resting time, the diaphragmatic movement is autonomically controlled with the diaphragmatic muscle and pulmonary recoil as the driving force for breathing-in and out respectively, while the pelvic floor and abdominal muscles are relaxed (Park & Han, 2015). However, during the controlled deep diaphragmatic inspiration, the intra-thoracic pressure is decreasing while the IAP is increasing (Hodges & Gandevia, 2000; Neumann & Gill, 2002; Park & Han, 2015; Talasz et al., 2010). These are caused mainly by the diaphragm movement and contractions of accessary inspiratory muscles surrounding the chest including serratus anterior, external intercostals, levator costorum, sternocleidomastoid, scalenus, and pectoralis (if the arms are lifted), which lead to more chest expansion and more increased IAP. The IAP may dissipate down to the pelvic floor and cause the floor a small stretch or a downward movement. Further, during the controlled deep expiration, more increased IAP is expected, caused mainly by contraction of the abdominal muscles (Hodges & Gandevia, 2000; Neumann & Gill, 2002; Park & Han, 2015). The action of this controlled deep expiration prepared by the increased IAP may play a critical role in physical and physiological activities described below. Usually, these activities act out at the end of the inspiration or during the expiration time, and coordinated by nervous system (Fregosi & Ludlow, 2014; Subramanian et al., 2008; Subramanian & Holstege, 2009). The action force of expiration for the activities may depend on the IAP at the end of the deep inspiration (IAP-EDI), which further rely on well-functioned diaphragm, pelvic floor, and abdominal muscles.
Based on if the IAP-EDI is on hold or pushed to move, different physical and physiological activities could be observed. When a person's diaphragm descends down actively and the IAP-EDI could be built up with assistance of pelvic floor and abdominal muscles, this individual is then ready to perform activities with IAP-on hold, IAP-pushed upward, or IAP-pushed down. First, when the IAP is on hold, the maintained IAP-EDI is critically important for the person to keep trunk stability and hold weight up (Hodges & Gandevia, 2000; Orlikoff, 2008; Sapsford, 2004). Such physical activities require vocal folds’ air trapping or closure (Fregosi & Ludlow, 2014; Orlikoff, 2008) for the chest cavity, and also require the soda-can like abdominopelvic cavity to act as a hollow but rigid frame to sustain the weight-holding posture (Figure 2A) (Hodges & Gandevia, 2000). Second, the IAP is pushed up when physiological activities like coughing, sneezing, blowing, spitting, emesis, and even loud speaking or singing are performed. During the time, the abdominal muscles contract, diaphragm and pelvic floor move superiorly, and the glottal aperture opens up between the true vocal folds (Figure 2B). Third, the IAP is pushed down while urinating, defecating, or even ejaculating during intercourse, and parturition during birth-giving. During the time, the abdominal muscles contract, diaphragm and pelvic floor move inferiorly, and glottal aperture closes up (Figure 2C) (Fregosi & Ludlow, 2014; Hodges et al., 2007; Orlikoff, 2008; Park & Han, 2015; Sapsford, 2004; Talasz et al., 2010; Yu et al., 2021). Thus, it is understandable that strength of each involved muscle including the diaphragm, pelvic floor, laryngeal, and abdominal muscles, along with the coordination of these muscles, is significantly important for physical and physiological activities mentioned above (Hodges & Gandevia, 2000; Neumann & Gill, 2002; Orlikoff, 2008; Park & Han, 2015). Any one or more of these muscles is or are weak or dysfunctional, the activities could very likely be affected. For example, weak coughing, low/short voicing, urinary or stool retention might be resulted from the weak diaphragm and/or abdominals. Urinary or bowl movement incontinence might be caused by the weak pelvic floor muscles that are not able to sustain the increased IAP (Hodges et al., 2007; Talasz et al., 2010). Additionally, the push-down action during the bowel movement always occurs during exhalation with the glottal aperture closed (Fregosi & Ludlow, 2014; Orlikoff, 2008). If a person has a weak or dysfunctional laryngeal muscles, this may cause decreased downward pressure to the pelvic floor, which may lead to constipation, an often-seen symptom in patients with Parkinson disease.
Neural Coordination of DDB-Related Activities
Autonomically controlled breathing itself involves the respiration center in brainstem, including the pre-Botzinger complex, which receives fibers from primary motor sensory cortex, hypothalamus, amygdala, and superior colliculus and red nucleus (Yang et al., 2020). However, when deep-breathing required activities are performed, the synchronized or coordinated movements of the diaphragm, the pelvic and abdominal muscles are needed and regulated through the corticobulbar and bulbospinal pathways in the central nervous system. How the pathways influence these different muscles is still not completely clear yet in human being, but based on studies from some human and animal studies, the corticobulbar and cortico-bulbo-spinal pathways for respiration-related physical and physiological activities have been summarized by different investigators (Belyk et al., 2021; Fogarty et al., 2018; Fowler et al., 2008; Galgano et al., 2019; Schellino et al., 2020; Subramanian et al., 2008; Subramanian & Holstege, 2009) (Figure 3). Apparently, through the connections of these neural pathways, muscle actions surrounding the thoraco-abdominopelvic cavities are interconnected and interinvolved to cooperate with each other for activities and behaviors (Subramanian et al., 2008; Subramanian & Holstege, 2009) that require the deep breathing related IAP change. Literature has shown that periaqueduct gray (Galgano et al., 2019; Subramanian et al., 2008; Subramanian & Holstege, 2009) and retroambiguus nucleus (Boers et al., 2002; Galgano et al., 2019; Schellino et al., 2020; Subramanian & Holstege, 2009) and their inter-communications (Subramanian & Holstege, 2009) play significant role in coordinating these muscle actions, among which the retroambiguus nucleus acts like a pianist's hand to strike on the piano keys (analogue to different motor nuclei for different muscles) for different tones (analogue to different muscle actions on targeted organs) (Subramanian & Holstege, 2009). Therefore, in terms of enhancing the neural interaction in brain, the deep breathing exercise might be an effective exercise training to be considered.
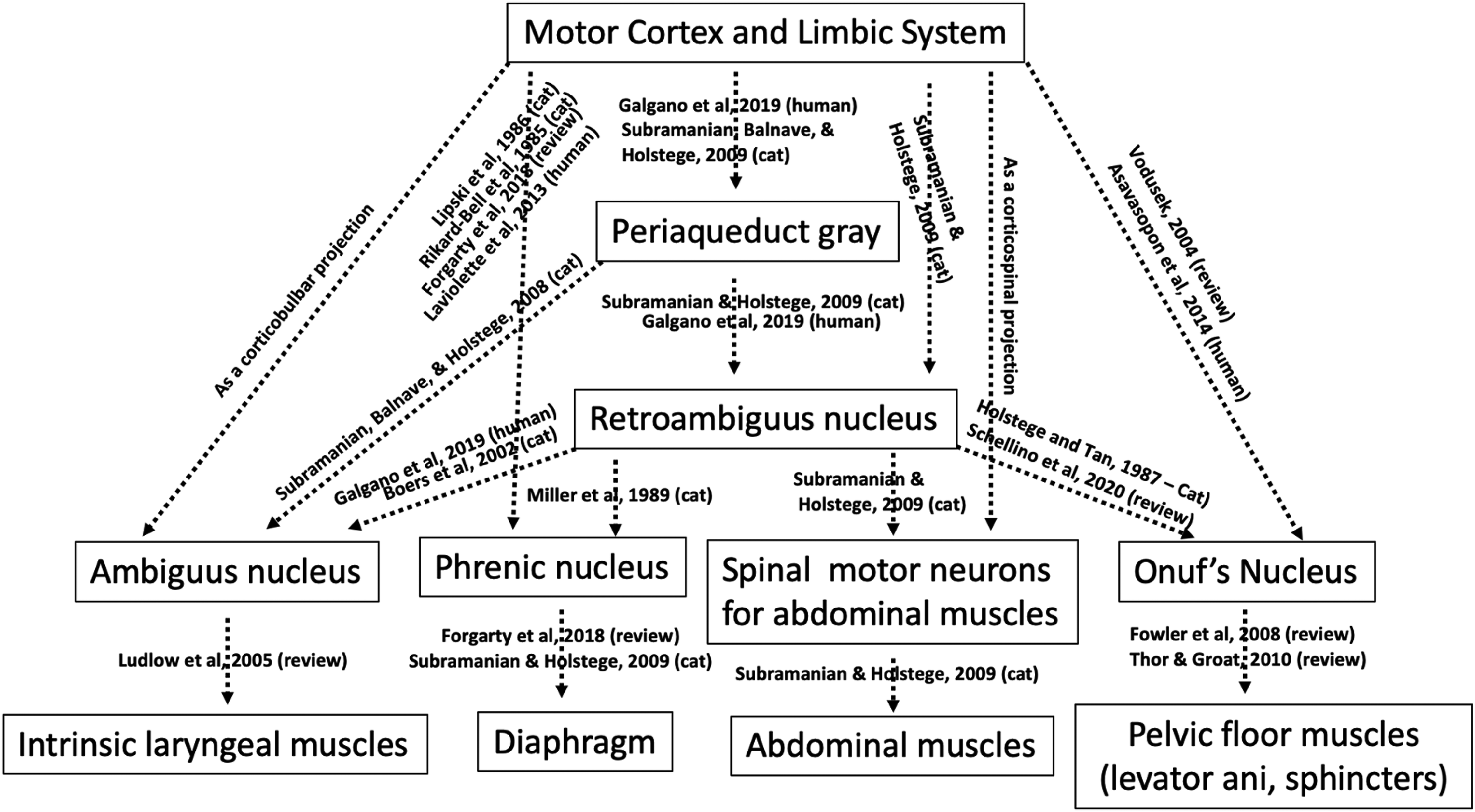
Neural pathways for coordinating and controlling actions of muscles surrounding the thoraco-abdominopelvic cavities. References are provided for each of these neural projections as indicated by dotted-line arrows in the figure.
DDB on the Nervous System
Physiologically the DDB is able to increase blood perfusion to the brain and enhance the brain's functionality (Bordoni et al., 2018). Additionally, the deep breathing could also improve cognition through five different approaches. First, neuroanatomically, the diaphragm movement is controlled by the phrenic nerve originating from the phrenic motor neurons in the phrenic nucleus at the C3-5 spinal cord, which receives bulbophrenic pathway projection from the rostral ventral respiratory group including the pre-Botzinger group neurons in the medulla (Alilain & Silver, 2009; Bordoni & Zanier, 2013; Vinit et al., 2016). The pre-Botzinger group is connected to the hypothalamus, the amygdala, the thalamus, the cortex, and the periaqueduct gray (Bordoni et al., 2018), which may indicate that the breathing may be able to affect the cognitive and emotional aspects as well as pain control through these connections. Second, electro-physiologically, the diaphragm could affect the neural oscillations or brainwaves (the rhythmic or repetitive pattern of neural activity) in variety of cortical areas as recorded in the electroencephalogram (EEG). These include both increased alpha activity and decreased theta activity. The increased alpha activity is associated with improved neural ability of alertness in quiet status, abstract-thinking, and self-control behavior; while the decreased theta activity is associated with improved concentration, reduced anxiety, and decreased distraction. Together, the changes of these two EEG waves may suggest the DDB effect on emotional control and psychological well-being (Folschweiller & Sauer, 2021; Heck et al., 2017; Zaccaro et al., 2018). Also, the gamma wave amplitude, involved in the frontal, parietal, and temporal lobes, was found increased, indicating activation of cognitive functions such as fear, despair, memory, attention, and motivation (Bordoni et al., 2018; Folschweiller & Sauer, 2021; Heck et al., 2017). Third, mechanically to the brain, the DBB can move the brain mass rostrally during deep inspiration; while moving the brain mass caudally during the expiration (Maier et al., 1994), which may facilitate the circulation of the cerebrospinal fluid. Also the breathing could decrease intracranial pressure and increase blood flow to the brain (Convertino, 2019), which provide a fundamental nutrition support of cognition-processing in the brain. Fourth, in patients with stress and depression, their sympathetic activity is continuously activated without the normal counteraction of the parasympathetic nervous system (Won & Kim, 2016). DDB is able to provide a powerful voluntary portal to entrain and modulate the sympathetic and parasympathetic balance (Noble & Hochman, 2019; Russo et al., 2017) by increasing the parasympathetic activity and decreasing the sympathetic activity, and consequently assisting in stress control, attention focus, and cortisol reduction (Ma et al., 2017; Martarelli et al., 2011; Russo et al., 2017). Fifth, neurocognitive and neuro-regenerative functions can be associated with inflammation and oxidative stress (Liu, Salem, et al., 2022; Won & Kim, 2016). Martarelli et al. (2011) reported that DDB is able to increase the antioxidant activity and reduce oxidative stress. As a result, the DDB improves the neurocognition from this perspective.
DDB as the Essence of Mind-Body Exercise in Holistic Health Care
As the number of older adults with multimorbidity increases and health care is shifting more from hospital to other clinical settings like home health, assistive living, and nursing homes, holistic health care seems to get more acknowledged and nurses’ role becomes more prominent during such changes (Eriksson et al., 2017). In nursing practice, holistic care is believed to be the core of the nursing science and recognizes a person as a whole for holistic health benefit (Eriksson et al., 2017; Strandberg et al., 2007). To become a certified holistic nurse, AHNCC listed 17 holistic therapies in the study guideline, among which mind-body exercise is one of them (AHNCC, 2017).
During the mind-body exercise, deep breathing is a key component that is constantly emphasized, for example, in Tai Chi (Hao et al., 2012; Liu et al., 2016), Ba-Duan-Jin Qigong (Bao et al., 2020; Liu, Miller, et al., 2022), and pranayama yogic breathing (Saoji et al., 2019). Studies have shown that these mind-body exercises are able to improve memory (Ye et al., 2021), cognition (Zhang et al., 2018), cancer symptoms (Duan et al., 2020), blood pressure (Ge et al., 2021), antiinflammation (Liu, Salem, et al., 2022), balance, and quality of life (Bao et al., 2020; Liu, Salem et al., 2022). In these exercises, the body part movements are coordinated with deep breathing (Bao et al., 2020; Hao et al., 2012). For instance, during Tai Chi practice, breathing-in is coordinated with the arms moving away from the body, and breathing-out is with the arms moving back toward the body. During the time, the diaphragm is concentrically contracting during deep inspiration, eccentrically contracting during deep expiration, and isometrically contracting at the end of either the deep inspiration or the deep expiration. The diaphragmatic strength might get increased via these exercise practices, particularly when resistance like extra cuff weight, waist weight, and ankle weight are applied to the DDB practice (Bao et al., 2020; Hao et al., 2012). In a recently published case report (Liu, Miller, et al., 2022), an elderly patient was able to improve strength, endurance, balance, cardiorespiratory function, gastral regurgitation, sleep, and activities of daily living after performing a 6-month DDB-based Tai-Chi Qigong exercise, indicating a favorite function of the DDB-based exercise for patients with multimorbidity.
Even in terms of the effect of deep breathing alone, prior investigations have demonstrated that DDB is an effective intervention to improve the diaphragmatic thickness (Kocjan et al., 2018), the pelvic floor muscle activity (Sorfova & Tlapakova, 2021; Yu et al., 2021), and postural stability (Kocjan et al., 2018; Sorfova & Tlapakova, 2021; Yu et al., 2021). On the other hand, the strengthening exercise of the pelvic floor is able to improve the diaphragm and pulmonary function (Park & Han, 2015). The efficiency of the deep breathing exercise can also be increased if the exercise is combined with arm open up and/or trunk extension as seen in Tai Chi or Tai-Chi related training (Bao et al., 2020; Hao et al., 2012; Liu et al., 2016). These may suggest that even DDB alone is also significantly beneficial to patients.
Theoretical Framework of DDB in Holistic Nursing Practice
Up to date, there is no pre-existing framework on the DDB. However, based on all descriptions above in this article, the theoretical framework of the DDB might be arguably described as that DDB may affect on different body systems and play a significant role in certain physical and physiological activities through its anatomical, neuroanatomical, and biomechanical characteristics. Clinically, holistic nurses work across a broad range of medical conditions, particularly for practices such as care for physical functions, cognition, mobility, and quality of life (Rijken et al., 2018; Sinnige et al., 2013). The contents in this article may provide a theoretical framework for holistic nurses to understand why the diaphragm plays a fundamental role in deep breathing-based mind-body management. The multi-system approach from the DDB practice may postulate a reasonable explanation why the DDB is effective for patients with multimorbidity to improve symptoms and signs; or even for healthy population to improve holistic well-being by preventing potential physical or physiological dysfunctions.
According to the AHNA, the primary mission of the AHNA is to advance the holistic healthcare through education and community-building among healthcare professionals and public (AHNA, 1998; Thornton, 2019). Holistic care plan with holistic approach requires the holistic nurses to know pertinent information and knowledge for the plan, formulate realistic outcomes, and develop and implement the holistic care plan (AHNCC, 2017). With knowledge in DDB for clinical practice, holistic nurses and healthcare providers could be very likely much better prepared and guided to conduct DDB-related clinical care management and patient education for people with multiple diagnoses to reach a holistic health.
Summary
The diaphragm, as the most important muscle in the human body, play a significant role in the DDB, which is a commonly used exercise in geriatric population for holistic care. The diaphragm contains three solid portions: the central tendon, the peripheral muscle, and the left and right muscular diaphragmatic crura; and three openings: vena cava, esophageal, and aortic hiatus. It is innervated primarily by the phrenic nerve containing motor, sensory, and sympathetic fibers and the intercostal nerves containing sensory fibers for the diaphragm. The diaphragmatic crura (mostly the right one) have muscular fibers circle around the gastroesophageal junction and act as an external esophageal sphincter to prevent esophageal reflux. Numerous ligaments attach the GI organs to the inferior surface of the diaphragm that can promote GI mobility and reduce possible GI organ adhesion. There are also four different ligaments including the pericardiophrenic ligament, attaching on the pericardium that may be able to increase cardiac and coronary perfusion when these ligaments pull on the pericardium and cause the intracardiac pressure to decrease during the deep inspiration time. Through the DDB, the diaphragm can work coordinately with laryngeal, pelvic, and abdominal muscles to regulate respiration-based physical and physiological activities such as weight lifting, coughing, sneezing, urinating, and defecating. The actions of these muscles might be coordinated via a variety of cortico-bulbar-spinal pathways. Through the activation of many neural pathways for breathing, improved mobility of the brain mass, improved neural oscillations or brainwaves in brain tissue, and the improved sympathetic-parasympathetic interaction on the diaphragm, the deep breathing exercise is able to improve the physical functionality and cognitive capability for an individual who practices the deep breathing as a part of the holistic care. A holistic nurse and healthcare professional are able to adopt these updated DDB knowledge to guide their clinical practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.