
Abstract
Peritoneal dialysis (PD) uptake around the globe has steadily increased over the last several decades as a viable alternative to haemodialysis. Continued success of this technique for patients is contingent on the application of continuous quality improvement (CQI) principles in PD practice which can improve patient outcomes and in turn lead to more successful PD programmes worldwide. In this installation of ‘Your Questions Answered’, we will outline an approach to quality improvement initiatives and examine the importance of CQI principles in PD practice. We will also highlight common pitfalls and provide strategies to identify potential targets for improvement within your PD programme.
Take-home points
Continuous quality improvement is a critical component of routine care offered to patients on peritoneal dialysis. Not all quality improvement initiatives will yield success; use failures as learning opportunities for future improvement. Reasons for unsuccessful projects are multifactorial and include rushing to a solution for a target problem, failure to engage key stakeholders and local context. Quality improvement in peritoneal dialysis can present unique challenges due to lack of evidence around quality indicators and limited resources.
Case vignette
A 29-year-old woman with advanced kidney disease is evaluated for the initiation of peritoneal dialysis (PD). She reports early uremic symptoms with an estimated glomerular filtration rate of 8.9 mL/min using the 2021 CKD Epidemiology Collaboration (CKD-EPI 2021) equation. She is subsequently seen by a general surgeon and is given a tentative date for a PD catheter insertion in 90 days’ time. Unfortunately, 6 weeks after seeing the surgeon, she presents to the emergency department with worsening symptoms of uraemia and is started on haemodialysis (HD). As a result of this experience, you perform an audit of your PD programme and identify that the average wait time for PD catheter insertions has been about 90 days, significantly higher than other regional centres (approximately 30 days). You suspect that the delay in wait time is due to the presence of only one operator inserting catheters. As a result, you propose an intervention that trains nephrologists to insert PD catheters at the bedside with a goal of reducing PD catheter insertion wait times. You launch the percutaneous catheter insertion by nephrologists, which is highly successful and reduces wait time for catheter insertions down to 14 days within 1 year. However, several months later the wait time for surgical intervention has increased up to 120 days, worse than prior to your intervention. There is now a greater demand for operating room time to address complications of percutaneously inserted catheters. Your quality improvement (QI) intervention to address timely access to PD catheters has amplified the problem, now posing a threat to the growth and sustainability of PD in your programme.
Why is continuous quality improvement important in PD?
In 2000, the safety culture in healthcare came under significant scrutiny with an estimated 98,000 deaths occurring annually due to medical errors in hospitals. 1 This was the dawn of a renewed commitment in healthcare to prioritise quality care and patient safety. Since then, continuous quality improvement (CQI) principles have come to the forefront in healthcare with work done by the Institute of Medicine (IOM). 2 The IOM has categorised quality care into 6 domains: safe, effective, patient-centred, timely, efficient and equitable (Table 1). Despite the emergence of CQI principles over the last few years, in theory, it has long been applied to PD practice. One of the most pertinent examples includes continuously evolving standardised protocols around peritonitis diagnosis and management, leading to better patient outcomes. 3,4 Additionally, the establishment of the Peritoneal Dialysis Outcomes and Practice Patterns Study (PDOPPS) and the Standardised Outcomes in Nephrology–Peritoneal Dialysis (SONG-PD) initiative have also paved the way for continued improvements in the quality of care provided to patients on PD around the world. 5,6 Despite these global initiatives and improvements in care, there is still a greater need for adoption of CQI in routine PD practice. In reviewing the literature, there are a few examples demonstrating the benefits of targeted CQI interventions in PD practice.
The six domains of quality in healthcare along with specific contextual examples in PD practice.a
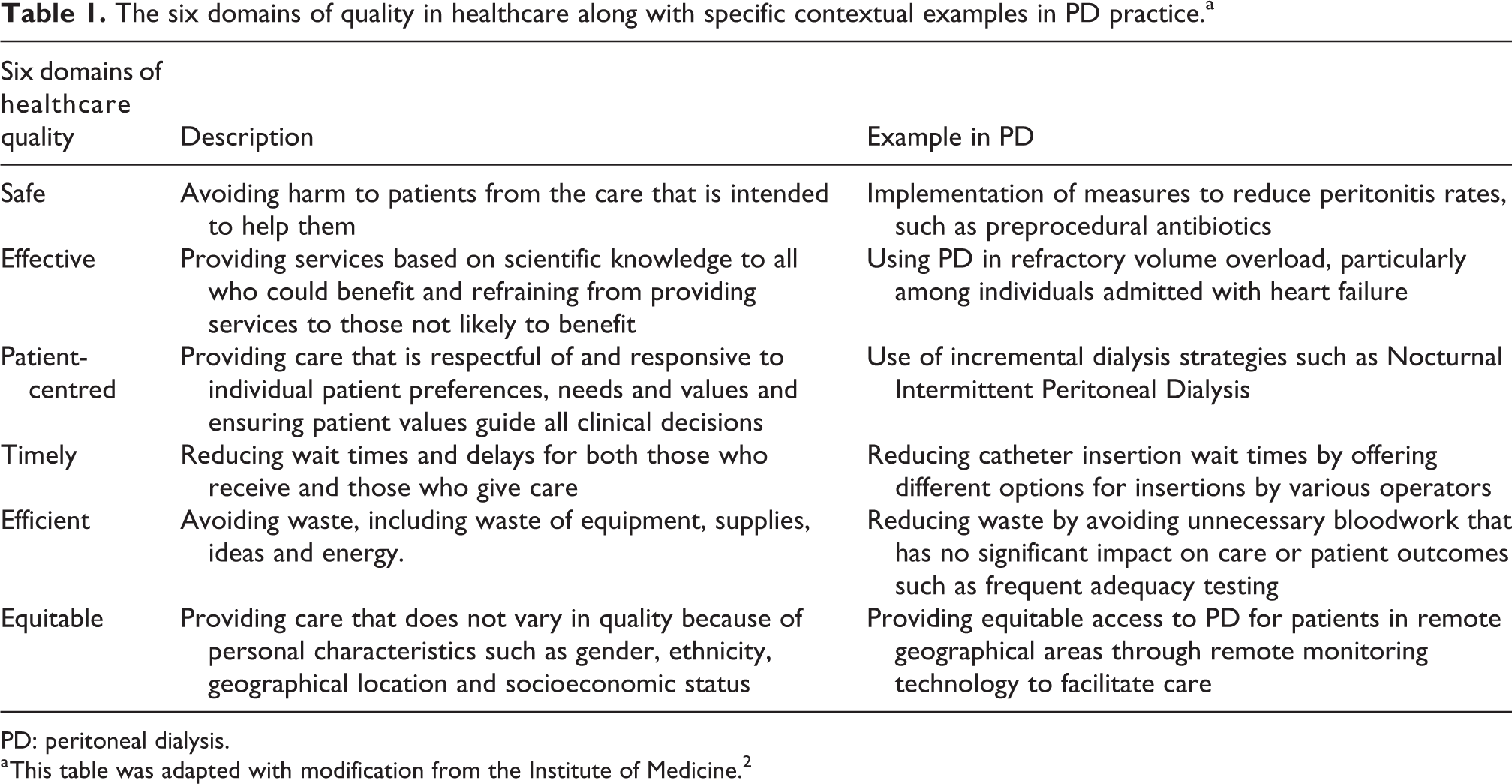
PD: peritoneal dialysis.
a This table was adapted with modification from the Institute of Medicine. 2
For example, observational data from large PD programmes in China where CQI principles have been incorporated into practice have demonstrated lower mortality, improved technique survival and lower rates of peritonitis. 7,8 Additionally, hospital registry data demonstrated that peritonitis rates reduced to 1 episode in 77.25 patient-months from 1 episode in 22.86 patient-months after implementation of a programme-wide QI initiative. 8 Given that peritonitis is well established as a leading cause of PD discontinuation, CQI strategies that reduce risk to patients are needed. 9 –11
It is for those reasons that PD practitioners should have a basic understanding of CQI principles, such as to offer innovative and high-quality care, allowing for sustained growth of PD. We must also educate trainees in QI to foster leadership skills that can facilitate organisational change that improves efficiency, saves costs and improves patient outcomes. 12,13 Given the increasing strain on various healthcare systems around the globe, there will be a growing demand for cost-effective treatment plans for patients with end-stage kidney disease. PD is cost-effective and can remain a viable alternative to HD, provided that growth is sustained without high rates of premature PD discontinuation. In adopting CQI as a part of routine practice within your local programme, you will continue to identify opportunities to improve the efficiency and quality of care offered to patients, ultimately fostering sustainable growth
How do you begin a QI project?
In beginning any CQI project in healthcare, it is imperative to identify a quality gap as the initial step. The IOM defines a quality gap as ‘the difference between health care processes or outcomes observed in practice and those potentially obtainable on the basis of current professional knowledge’. 2 In the case vignette, the quality gap identified was prolonged wait times for PD catheter insertion. An analysis of your programme performance compared to other programmes with respect to infection rates, prevalent PD growth rates and patient satisfaction through clinical audit may be a helpful starting point for identification of a QI target. 14 Once a target is identified, the next step is to establish a team which include key stakeholders of differing experiences, expertise as well as opinions. This diversity in team membership is critical for project success as it ensures broad perspectives, which are sometimes overlooked by individuals leading the initiative.
Additionally, project aims, outcomes and measures should be defined to create clear direction for all team members. The principles and approach in the development of a concise aim statement is discussed in further detail in the section ‘How to avoid common pitfalls in QI’.
Once you have formulated your aim statement and identified your outcome measure of interest, it is critically important to test your project theory in small sample sizes before implementation on a larger, time-consuming scale. These small ‘trial cycles’ are referred to as Plan–Do–Study–Act (PDSA) cycles which allow for small tests of change on a small scale (e.g. a few patients or one clinic) to determine plausibility. 15 These can be repeated many times with fine-tuning of project details each iterative cycle to optimise the chances of a successful intervention. Once the project is ready for wide-scale implementation, assigning a project champion within a multidisciplinary team that is responsible for data measurement and accountability can further enhance changes of success and broaden engagement.
Finally, several tools exist to measure and demonstrate the impact of your intervention. It is important to note that while this is a general outline on how to conduct a QI intervention, each stage can be met with various challenges that can hinder the QI process. A more detailed explanation on mitigation strategies that can be undertaken is also outlined in the section titled, ‘How to avoid common QI pitfalls in PD practice’.
How do you select a QI framework and targets for improvement in your PD programme?
There are various frameworks that define QI in healthcare delivery. A QI framework is defined as a stepwise methodical approach in planning a QI initiative that allows for the use of common language, consistency and similar mindset. 16 –18 This is particularly important in the delivery of care in complex systems such as is the case with PD, where numerous factors can influence patient outcomes. 18 The most used model within this framework is the ‘Model for Improvement’ that utilises rapid cycles of change called PDSA and is supported by a variety of organisations including the Institute for Health Improvement (IHI). 16,19 –21 The Model for Improvement was developed in 1996 by the Association for Process Improvement in conjunction with the IHI. 21 This model is simple and can be broken down into three main questions: (1) ‘What are we trying to accomplish?’ (2) ‘How will we know that a change is an improvement?’ (3) ‘What change can we make that will result in an improvement?’ (Figure 1). A major advantage of the Model for Improvement is that it is a simple, yet efficient framework that can be applied to many QI initiatives. 20 It can be also used by healthcare providers with limited QI experience or training and does not require expert consultancy. 22 However, the Model for Improvement has an important limitation in that it cannot be used to identify the cause of an underlying problem. 22 It is for this reason that the Model for Improvement is ideal for QI initiatives with clear, identifiable problems that can be addressed with evidence-based solutions. For example, a project that aims to improve patient survival and thereby maintain home dialysis prevalence by increasing Kt/V by 25% for all patients in a PD programme to improve patient outcomes is flawed from its inception. Given that that there are multiple factors that influence outcomes and numerous studies have demonstrated no mortality benefit with higher Kt/V values on PD, 23 –25 such a project would not be ideal under the Model for Improvement. However, a project that increases the proportion of patients on Renin–Angiotensin–Aldosterone System blockade therapy to preserve residual function in your programme would be more suitable project and ideal for the Model for Improvement. Furthermore, given the tenets of the Model for Improvement and its simplified framework with a focus on clearly definable aim and process measures, projects contextualised by quality gaps as measured by comparison to local or national standards of care are often well-suited to this type of QI framework. 26 It should be noted that there are other QI models used in healthcare which include LEAN 27 and Six Sigma 28 which are beyond the scope of this review, but readers should be aware that not all QI initiatives are easily addressed with the Model for Improvement using rapid PDSA cycles.
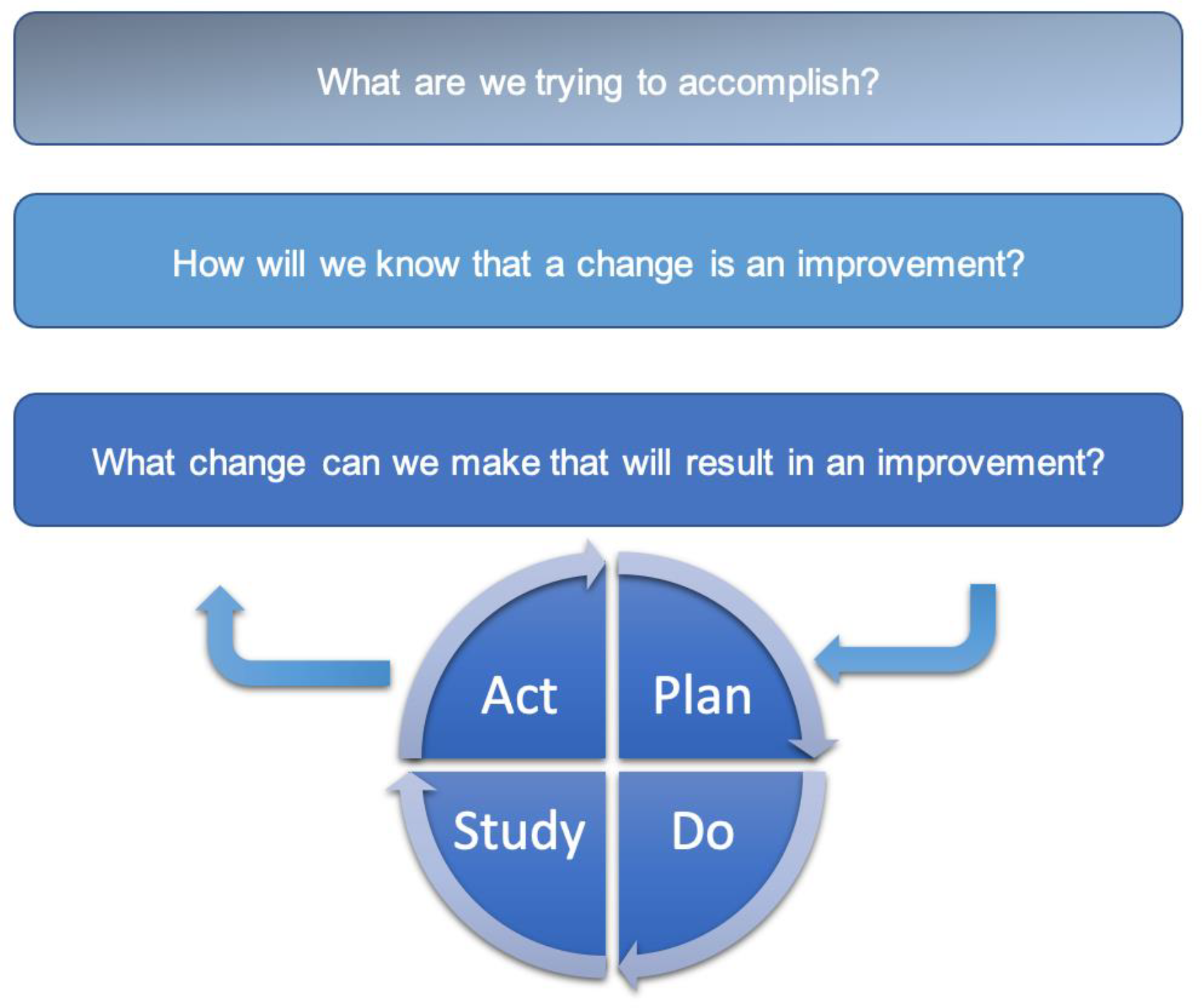
Model for improvement demonstrating the three essential questions and the PDSA cycles. Adapted with modification from Langley et al. 29 PDSA: Plan–Do–Study–Act.
As it relates to ideas for QI projects, many have been generated by provider or patient experiences related to delayed care, reducing waste and inefficient or unsafe care. 30 –34 However, what a provider may be passionate about might not be a priority for important stakeholders within an organisation. For example, your improvement idea might be to reduce waiting time during PD clinic visits. While this may be a well-intentioned project aimed at improving patient experience, it may not have the support within the organisation, who may prioritise growing the PD programme or reducing peritonitis rates instead. In instances where improvement ideas are limited, consider reviewing key performance indicators (KPIs) in your local environment that may be outlined by national or international standards. 35,36 In using KPIs, it may provide comparative metrics of how your local programme is performing in relation to established standards and other programmes. Apart from improving patient outcomes, KPIs have been shown in one Australian observational study to improve the uptake of PD. 37
In summary, using a framework to guide QI in PD can set a project up for success. The most used and most user friendly of these frameworks is the Model for Improvement. However, its limitations should be noted, and other frameworks should be considered to meet the unique needs of more advanced projects.
How can you avoid common QI pitfalls in PD practice?
In healthcare, we may be anxious to find solutions to many problems encountered in clinical practice. There may be significant pressures for rapid solutions from patients, family members, caregivers as well as administrators to address problems immediately. However, in QI, it is critically important to understand the nature of a problem before proposing solutions. 12 We may be setting ourselves up for failure with hastily proposed solutions and in fact, what we think is the cause could be a symptom of a larger problem. 38 Simply put, it is difficult to fix what we do not understand.
In addition to performing root-cause analyses, the importance of engaging relevant stakeholders for any QI initiative cannot be overstated. It is imperative to consider the perspective of stakeholders as that may provide valuable insight into potential drivers of an underlying problem. Stakeholder engagement represents an additional key component in the QI process. A stakeholder is defined as any individual or group who can influence your QI initiative in either a positive or negative way. Given that there may be many stakeholders that are linked to a particular QI project at any given time, it is important to prioritise their influence in a process called mapping
After you have identified your stakeholders, it is important to use their input to conduct an effective root-cause analysis. There are three common tools used in the root-cause analysis which include process mapping, Pareto charts and fishbone (Ishikawa) diagrams. In including important stakeholders as part of this process you are more likely to formulate an accurate depiction of the factors that may be influencing a problem you are trying to solve. Another simple root-cause analysis technique that can be utilised is ‘The Five Whys’. The root cause of a problem can often be identified by asking ‘Why?’ five times. 38 In utilising this approach, we are less likely to hastily come up with solutions before truly understanding the nature of the problem.
In the case vignette, the nephrologist identifies that a single operator is leading to the long wait times, and this could potentially be shortened by offering percutaneous bedside catheter insertions. However, the nephrologist fails to engage the surgeon, access coordinators or administrators, all of whom may provide unique perspectives, in critically evaluating the underlying cause of the problem. An effective root-cause analysis would have revealed that longer wait times for insertion were due to reduced operating room time because of staff shortages and closures due to unit for renovations. Figure 2 demonstrates an Ishikawa diagram of the potential causes for long wait times for PD catheter insertions. In starting to insert percutaneous catheters, the nephrologist has in the short term reduced the wait time for a select group of patients (those with no significant surgical abdominal history) but has limited access to the surgeon for those with more complicated insertion requirements. The surgeon and operating room time are now more occupied with treating complications and other non-functional catheters inserted by the nephrologist. Additionally, if ‘The Five Whys’ had been utilised, the nephrologist would have also appreciated that prolonged wait times were a symptom of understaffed facilities with operating room closures. This underscores the importance of effective root-cause analysis, stakeholder mapping, and engagement in QI initiatives.
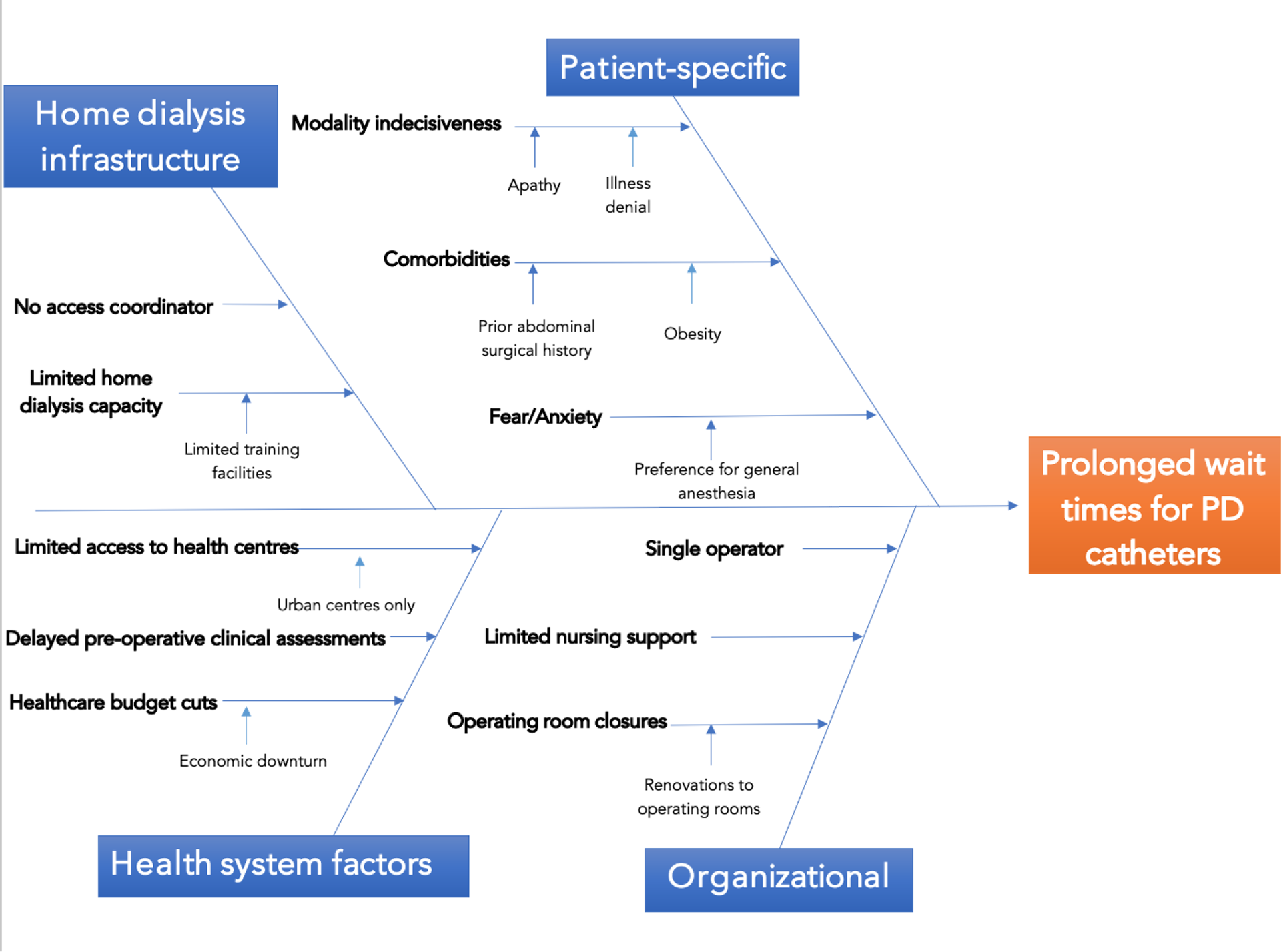
Fishbone (Ishikawa) diagram of the potential causes for increased wait times for peritoneal dialysis catheter insertions. In the case vignette, the nephrologist did not complete a comprehensive root-cause analysis such as a fishbone diagram and missed important potential causes for delay and implemented a premature intervention which ultimately further worsened the wait times.
Unintended consequences represent another challenge within QI. In our haste to see positive results, we may fail to consider undesirable downstream effects. These effects may include increased costs, worsening health inequities and patient harm. 39 In the case vignette, a desire to increase the utilisation of bedside catheter placement to grow the home programme represents a possible ‘measure fixation’ that may have led to the promotion of this type of procedure for patients who were, in retrospect, not ideal candidates for bedside catheter placement and hence developed complications. In addition to outcome measures and process measures, balancing measures are critical in the QI pathway to capture data regarding possible signals of harm. 26,40 Examples of balancing measures in this case would be peritonitis rates following insertion and 30-day primary non-function rates. A more simplified way to think of it would be, are the catheters working and if so, is there an increased risk of complications/harm to patients?
Sometimes we manage to do everything right but are often discouraged when we fail to appreciate the impact of an intervention. This may be because of a small sample size. Fidelity, which refers to the uptake of a given intervention, can be identified through rapid PDSA cycles and plays a key role in the determination of sample size. 41 Lower fidelity of implementation necessitates a larger sample size to detect the effects of change.
Finally, once you have identified a target for improvement and are planning on implementing an intervention, it is important to be ‘SMART’ about it. Being SMART means to have aims that are S-specific, M-measurable, A-achievable, R-relevant and T-timely. 12 A SMART aim clearly defines the target population, the desired improvement and the targeted timeframe. The best evidence of the effectiveness of SMART aims comes from health behavioural change data. 42,43 These data demonstrate that SMART aims may provide requisite structure and direction needed to lead change. Furthermore, a consciously set SMART aim provides a foundation to create subconscious priming which can motivate others and help in achieving the outlined goal. 44 In this way, the SMART aim framework serves as an effective and evidence-based tool for increasing the likelihood of goal actualisation. The lack of a SMART aim can lead many astray and it is a common pitfall in QI. For example, in the above case, the nephrologist indicated that the plan was to simply reduce wait times for catheter insertions. However, this aim is not clear about the extent in which the wait time would be reduced, by when and among which specific patients. In outlining a SMART aim, you must clearly articulate your vision to members of the team and remain focused on the objective. A better aim would have been ‘reduce the average wait time among patients eligible for a PD catheter inserted using a percutaneous ultrasound-guided approach by a nephrologist by 50% within one year’. In formulating a SMART aim, you are better suited in answering the first question in the Model for Improvement ‘What are we trying to accomplish?’
These common pitfalls in the QI process can significantly hinder a project in your PD practice. Awareness of these potential shortcomings from the outset and applying methodical strategies to address them will increase the likelihood of sustainable success.
How can you improve QI culture in your PD practice?
The best designed QI project or initiative will only be successful if the culture permits. To create sustainable change, your initiative must align with institutional priorities, and you must cultivate an environment that keeps staff members engaged. 45,46 Practice culture may be ingrained and hard to change even when there are data to suggest that change in practice is needed. Initiatives such as Nephrologists Transforming Dialysis Safety (NTDS) launched by the American Society of Nephrology in conjunction with the Centers for Disease Control and Prevention encourage the leadership role of dialysis physicians in pursuing a multi-faceted approach to creating change and improving care for dialysis patients. 47 However, sustainable change necessitates broad programme engagement. There are numerous strategies than can be utilised to improve the culture in your practice including visual management, improvement huddles and supporting advanced QI training among team members. 46,48,49
Broad engagement of team members in your PD programme is critically important to modulate culture. There are multiple ways by which this can be achieved. One such way is the identification of local ‘champions’ to lead specific quality interventions. The use of champions to spearhead projects is an evidence-based tool that serves the dual purpose of extending leadership roles within quality initiatives across disciplines and also improves the accountability and execution of a given project by delegating the ground-work to a specific individual while the medical director oversees the project. 50
Another way to increase engagement is by implementing monthly or quarterly huddles. These meetings can serve as opportunities to reinforce project aims and objectives which are subject to loss of enthusiasm with time. In addition, they allow for ongoing coordination of interests and provide opportunities to incorporate feedback at multiple levels which may help bring earlier attention to yet unidentified obstacles or challenges. For example, monthly or quarterly reviews of ‘gains and losses’ from the PD programme is an effective exercise. In these meetings, a closer scrutiny of technique discontinuation incidence can identify gaps in care that lead to attrition from your PD programme. Additionally, it can serve as a platform to identify missed opportunities, whereby an eligible patient had a prior expressed intent to start PD but for some reason was started on HD. These huddles allow team members to provide input about programme strengths and weaknesses, which in turn can spur ideas for targeted improvement, ultimately leading to sustainable growth in a PD programme.
Furthermore, visual management can be achieved using performance boards or process control charts in your unit to highlight areas of strength or weakness (Table 2). This can lead to positive reinforcement within your PD programme when team members see how the unit is performing in a particular area. It also lends itself to transparency and is rather simple for team members to determine whether further work is needed or if an improvement has been sustained. 46 In effect, that visual representation can be a powerful motivator to lead change or positive reinforcement to sustain change in your PD programme.
Strategies that can be utilised to build a stronger QI culture in your local PD programme.
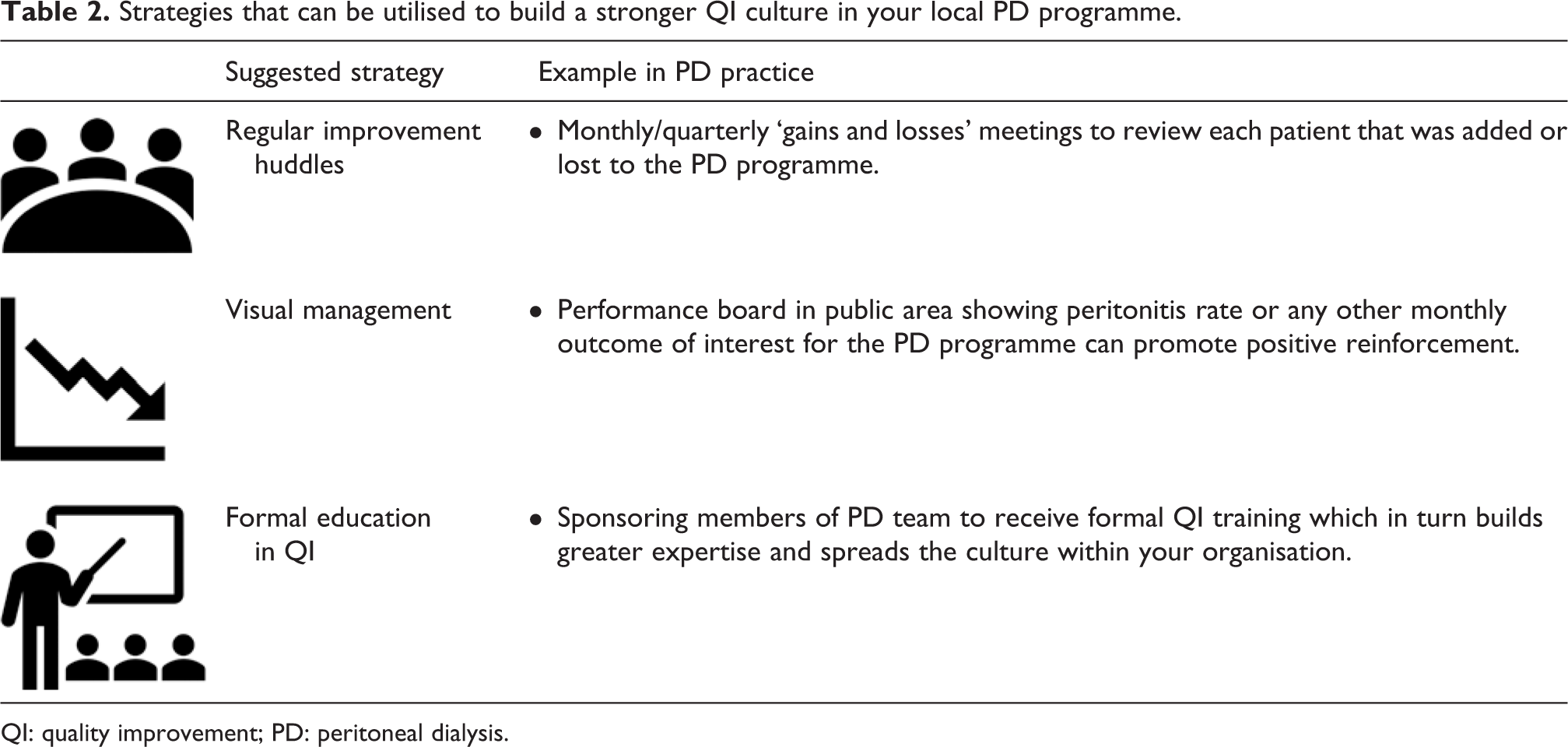
QI: quality improvement; PD: peritoneal dialysis.
Additionally, governmental policy can have a direct influence on a QI culture within a local environment. For example, initiatives like the quality assessment and performance improvement process (QAPI) have been utilised in dialysis centres in the United States with great success. QAPI involves a multidisciplinary team that includes a medical director, social worker, nurses and other healthcare providers that meet regularly to evaluate QI initiatives within their local environment to improve patient outcomes. 51 QAPI meetings are held regularly and must be done to demonstrate evidence of quality and performance improvement as outlined by the Centers for Medicare and Medicaid Services (CMS), which is a funding organisation in the US health system.
Although much of the emphasis in the United States has focused primarily on HD, there has been success in other parts of the world when CQI has been used in a PD setting. For example, in China, PD has a high rate of uptake along with excellent technique survival rates. This has been attributed to CQI programmes focusing on KPIs such as peritonitis rates, patient outcomes and technique survival rates, all of which have shown significant improvement with the implementation of CQI principles 7,52
Lastly, you should identify and encourage opportunities for formal QI training among team members within your PD programme. In acquiring basic and advanced skills in QI, your PD programme will build greater capacity to lead change. This need to build greater capacity for QI in clinical practice has also been recognised by various medical education training programmes around the globe where basic QI training is now required in most programmes. 13 Team members equipped with skills in QI will take the initiative in identifying areas for improvement which will cultivate a stronger culture of improvement within your local programme. 53
Cultural change in QI cannot be attained by simply snapping one’s fingers but it requires an ongoing process of creating an environment where QI is not seen as an additional task but rather the way of routine practice. You must therefore be patient and steadfast to reap the long-term rewards of CQI in your PD programme.
Conclusions
CQI in PD is essential to the delivery of high-quality care for patients with end-stage kidney disease. In planning initiatives in QI, you must engage stakeholders while identifying problems that are relevant to your local environment. Although some elements of QI work have occurred with the standardisation of PD practices around the globe, there remains many opportunities at the microsystem level to lead change. Practitioners must also recognise that in QI practice, not every change results in an improvement, but to achieve improvement, change is required. The results of QI work may take time to demonstrate meaningful change and it is for this reason that time should be devoted to understanding a problem well before proposing a solution. In hastily formulated solutions, QI initiatives are likely to fail, and this may amplify the scepticism among individuals who doubt the utility and significance of QI work within your PD programme.
Footnotes
Acknowledgements
None.
Author contributions
SH wrote the initial draft of the manuscript. BLA outlined the sections of the manuscript. SH and BLA edited the manuscript equally to completion. Both authors signed off and agree with the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SH has no conflicts to declare. BLA has received speaking fees from Baxter health and Amgen.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.