
Abstract
Peritoneal dialysis (PD)-associated peritonitis is a serious complication of PD and prevention and treatment of such is important in reducing patient morbidity and mortality. The ISPD 2022 updated recommendations have revised and clarified definitions for refractory peritonitis, relapsing peritonitis, peritonitis-associated catheter removal, PD-associated haemodialysis transfer, peritonitis-associated death and peritonitis-associated hospitalisation. New peritonitis categories and outcomes including pre-PD peritonitis, enteric peritonitis, catheter-related peritonitis and medical cure are defined. The new targets recommended for overall peritonitis rate should be no more than 0.40 episodes per year at risk and the percentage of patients free of peritonitis per unit time should be targeted at >80% per year. Revised recommendations regarding management of contamination of PD systems, antibiotic prophylaxis for invasive procedures and PD training and reassessment are included. New recommendations regarding management of modifiable peritonitis risk factors like domestic pets, hypokalaemia and histamine-2 receptor antagonists are highlighted. Updated recommendations regarding empirical antibiotic selection and dosage of antibiotics and also treatment of peritonitis due to specific microorganisms are made with new recommendation regarding adjunctive oral N-acetylcysteine therapy for mitigating aminoglycoside ototoxicity. Areas for future research in prevention and treatment of PD-related peritonitis are suggested.
This is a visual representation of the abstract.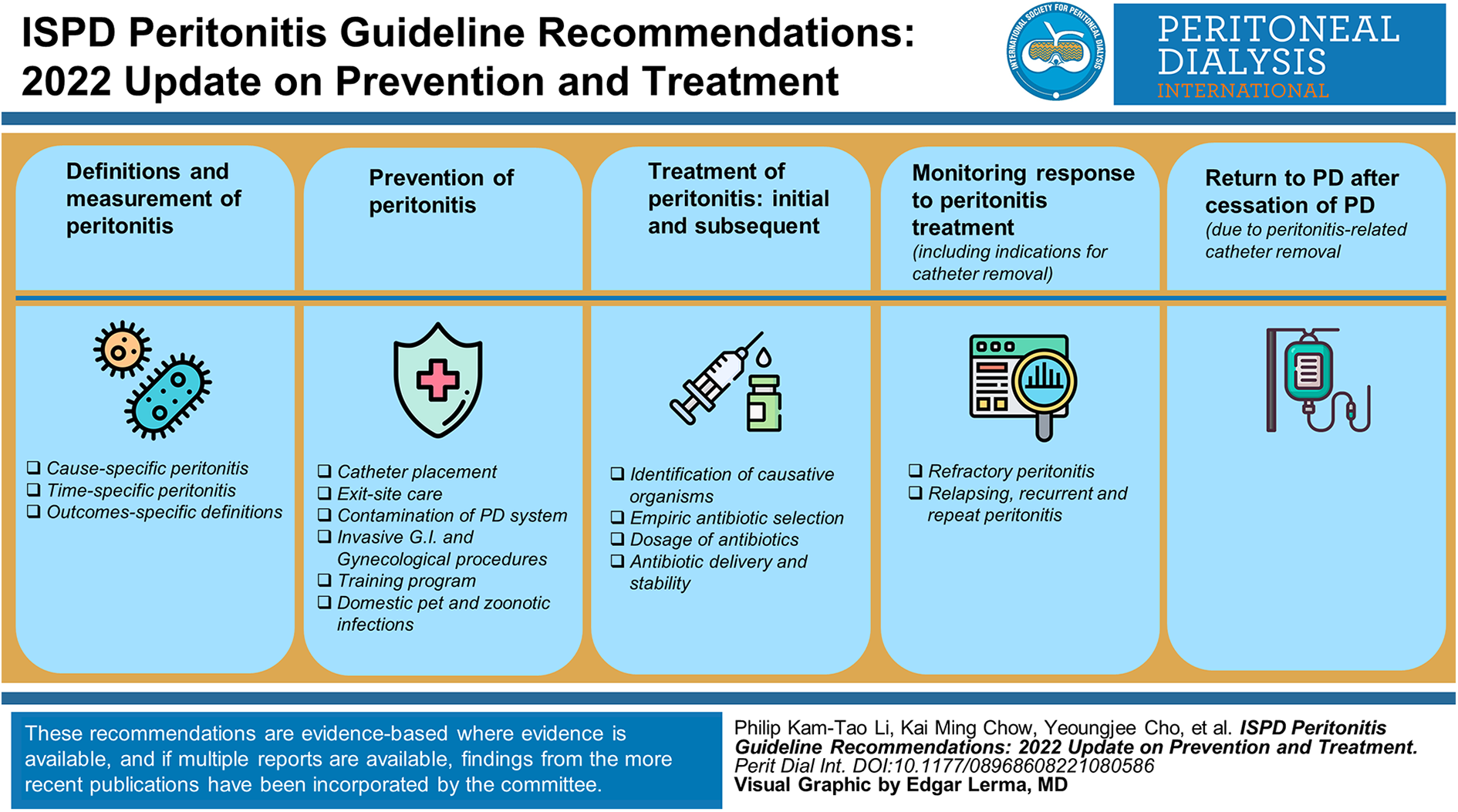
What’s new with the 2022 update of the ISPD peritonitis guidelines?
Revised, clarified definitions for refractory peritonitis, relapsing peritonitis, peritonitis-associated catheter removal, peritonitis-associated haemodialysis transfer, peritonitis-associated death and peritonitis-associated hospitalization (page 5).
Definitions for new peritonitis categories and outcomes: pre-PD peritonitis, enteric peritonitis, catheter-related peritonitis and medical cure (page 3-4).
Revised, updated recommendations for calculating and reporting peritonitis rates before and after PD commencement (page 4-6).
New targets recommended for overall peritonitis rate, proportion of patients free of peritonitis and culture-negative peritonitis (page 5).
Revised recommendations regarding management of contamination of PD systems (page 7).
Revised recommendations regarding antibiotic prophylaxis for invasive procedures (page 7).
Revised recommendations regarding PD training and reassessment (page 8).
New recommendations regarding PD patients with pets (page 9).
New recommendations regarding management of modifiable peritonitis risk factors (hypokalaemia, histamine-2 receptor antagonists) (page 10)
Update on novel diagnostic techniques for peritonitis (page 13).
Updated recommendations regarding empirical antibiotic selection (page 13) and dosage of antibiotics (page 14).
New recommendation regarding adjunctive oral N-acetylcysteine therapy for mitigating aminoglycoside ototoxicity (page 14).
Revised recommendations regarding treatment of peritonitis in patients receiving APD (page 18).
Revised recommendation regarding consideration of expectant management in patients longer than 5 days if PD effluent white cell count is decreasing towards normal, instead of mandatory PD catheter removal if effluent does not clear up by day 5 (page 19).
Updated recommendations for treatment of peritonitis due to coagulase-negative staphylococci (page 22, Corynebacteria (page 23), enterococcus (page 23), Pseudomonas (page 24, Acinetobacter (page 25), Stenotrophomonas (page 25) and non-tuberculous mycobacteria (page 30).
Introduction
Peritoneal dialysis (PD)-associated peritonitis is a serious complication of PD, 1,2 which is a critically important outcome to all key stakeholders including patients, caregivers, clinicians, researchers and policymakers. 3 It is the most common type of PD-related infection resulting in increased healthcare utilisation and is associated with significant harms including pain, treatment costs, transfer to haemodialysis and death, as well as alterations of the peritoneal membrane and peritoneal adhesions which can make long-term treatment with PD challenging. 4 –7
Recommendations on the prevention and treatment of peritonitis have been published previously under the auspices of the International Society for Peritoneal Dialysis (ISPD) in 1983, 1993, 1996, 2000, 2005, 2010 and 2016.
8
–13
The present recommendations are organised into five broad sections focusing on: definitions and measurement of peritonitis; prevention of peritonitis; treatment of peritonitis: initial and subsequent; monitoring response to peritonitis treatment including indications for catheter removal and return to PD after cessation of PD due to peritonitis-related catheter removal.
These recommendations are evidence-based where evidence is available, and if multiple reports are available, findings from the more recent publications have been incorporated by the committee. In general, these recommendations follow the Grades of Recommendation Assessment, Development and Evaluation system for classification of the level of evidence and grade of recommendations in clinical guideline reports. 14 Within each recommendation, the strength of recommendation is indicated as Level 1 (We recommend), Level 2 (We suggest) or Not Graded, and the quality of the supporting evidence if shown as A (high quality), B (moderate quality), C (low quality) or D (very low quality). 14 The recommendations related to treatment are not intended to be implemented indiscriminately and may require adaptation according to local conditions, such as pattern of infection, causative organisms and microbial resistance. Clinicians caring for paediatric PD patients should refer to the latest consensus guidelines for the prevention and treatment of catheter-related infections and peritonitis in paediatric patients receiving PD. 15
Definition and measurement of peritonitis
Definition
Standardisation of the definition of outcomes and its measures is pivotal to enabling assessment of the comparative effects of interventions for peritonitis. It also facilitates benchmarking of performance to improve and address practice variations. A systematic review of 77 studies (three randomised controlled trials) demonstrated large variability in definitions of peritonitis (29% of studies did not describe peritonitis definition used and 42% of studies modified ISPD recommended diagnostic criteria for peritonitis) and reporting of outcome measures (e.g. peritonitis rate, peritonitis-related death). 16 In another systematic review, 59 clinical trials of PD-related infections included 383 different outcome measures. 3 The definitions related to peritonitis can be further classified according to cause, association with exit-site/tunnel infections, timing in relation to previous episodes and outcomes.
Peritonitis
We recommend that peritonitis should be diagnosed when at least two of the following are present:
clinical features consistent with peritonitis, that is, abdominal pain and/or cloudy dialysis effluent;
dialysis effluent white cell count > 100/µL or > 0.1 × 109/L (after a dwell time of at least 2 h), with > 50% polymorphonuclear leukocytes (PMN);
positive dialysis effluent culture (1C).
Cause-specific peritonitis
We recommend a diagnosis of peritonitis according to organisms identified on culture (e.g., Staphylococcus aureus peritonitis; 1C).
We suggest culture-negative peritonitis is defined when peritonitis is diagnosed using the criteria above (criteria one and two), but no organism is identified on culture of dialysis effluent (Not Graded).
We suggest catheter-related peritonitis is defined as peritonitis that occurs in temporal conjunction (within 3 months) with a catheter infection (either exit-site or tunnel 17 ) with the same organism at the exit-site or from a tunnel collection and in the effluent or one site sterile in the context of antibiotic exposure (Not Graded).
We suggest enteric peritonitis be defined as peritonitis arising from an intestinal source involving processes such as inflammation, perforation or ischemia of intraabdominal organs. If a peritonitis episode in this context is culture negative, we suggest that it be classified/recorded as enteric peritonitis rather than as culture-negative peritonitis (Not Graded).
The cause of peritonitis can be broadly divided according to organism or concomitant event (e.g. tunnel infection) to inform treatment. When no organism is identified after the culture of dialysis effluent, culture-negative peritonitis is diagnosed. 11 All cases of culture-negative peritonitis that meet the ISPD diagnostic criteria for peritonitis should be counted in the peritonitis statistics. Culture-negative peritonitis can be due to infectious or non-infectious causes. For example, infectious causes may occur in the context of recent antibiotic exposure, suboptimal sample collection or culture methods or misclassification from slowly growing atypical organisms (e.g. mycobacteria, fungus). Non-infectious causes may include eosinophilic or chemical (e.g. icodextrin) peritonitis but neutrophil predominance of the elevated white blood cells (WBC) count may not be present. 11 Hemoperitoneum, characterised by the predominant presence of red blood cells in the dialysis effluent, should not be confused with peritonitis.
The association between catheter-related infections, such as exit-site and tunnel infections, and peritonitis is well established. 18,19 Catheter-related peritonitis can be diagnosed with a high degree of certainty when it occurs concomitantly with an exit-site and/or tunnel infection. Alternatively, one site (e.g. exit-site or PD effluent) may be culture negative in catheter-related peritonitis in the context of recent antibiotic exposure for treatment of the initial infection. However, at present, there are no data available to inform the precise temporal criterion for diagnosing catheter-related peritonitis. 20 Interestingly, a case–control study of 962 incident PD patients demonstrated that the odds of peritonitis after an exit-site infection by organism class at 3, 6 and 9 months were significantly more likely to be from the same class of organism at 3 months (odds ratio (OR) at 3 months: 2.00, 95% confidence interval (CI) 1.15–3.47, p = 0.01), especially for gram-positive organisms (OR at 3 months: 2.27, 95% CI 1.19–4.31, p = 0.01 compared to at 9 months: OR 1.91, 95% CI 1.29–2.83, p = 0.001). 18
Peritonitis from enteric causes (e.g. strangulated bowel, ischemic colitis, appendicitis) can pose a diagnostic challenge with attendant delays in appropriate treatment and resultant increased morbidity and a mortality rate of approximately 50%. 21,22 Identification of multiple organisms (particularly both gram-positive and gram-negative) is highly suggestive of an enteric cause for peritonitis; however, this has been reported to occur in less than 20% of cases of enteric (sometimes known as ‘surgical’) peritonitis. 21,23 Enteric peritonitis can present as culture negative if the process involves the peritoneal membrane through a contiguous, non-infective, inflammatory reaction (e.g. pancreatitis). 24
Time-specific peritonitis
Pre-PD peritonitis (before PD commencement)
∘ We suggest pre-PD peritonitis be defined as a peritonitis episode occurring after PD catheter insertion and prior to commencement of PD treatment. The date of PD initiation is defined as the day when the first PD exchange is performed with the intention of continuing long-term PD treatment from that day (i.e. first day of PD training or PD treatment in a hospital or at home with the intention of continuing PD long-term, whichever occurs first). The intermittent flushing of a PD catheter for the purpose of maintaining catheter patency does not qualify as PD initiation (Not Graded).
∘ For the purpose of pre-PD peritonitis rate reporting,time at risk starts from the day of PD catheter insertion and ends with PD commencement, PD catheter removal or death, whichever comes first (Not Graded).
PD-related peritonitis (after PD commencement)
∘ We suggest that, for the purpose of standard peritonitis rate reporting for PD-related peritonitis, time at risk starts from the day of PD commencement (i.e. first day of PD training or PD treatment in hospital or at home with the intention of continuing PD long-term, whichever occurs first) and continues while a patient remains on PD regardless of the setting (home, hospital, residential aged care facility, etc.) or who is performing the PD exchanges (Not Graded).
PD catheter insertion-related peritonitis
∘ We suggest that PD catheter insertion-related peritonitis be defined as an episode of peritonitis that occurs within 30 days of PD catheter insertion (Not Graded).
Peritonitis occurring prior to PD training is an under-recognised problem. Most units, including clinical registries, only capture peritonitis after patients commence PD. One observational study in Hong Kong reported the incidence of pre-training peritonitis to be 4.2% in 1252 patients newly started on PD. 25 Another long-term study in Germany confirmed that peritonitis incidence would be underestimated by 0.03 per patient-year at risk if peritonitis episodes occurring before completion of PD training were not counted. 26
In line with the ISPD Guidelines on Creating and Maintaining Optimal PD Access in the Adult Patient, 27 PD catheter insertion-related peritonitis is defined as an episode of peritonitis that occurs within 30 days of PD catheter insertion and should be <5% of PD catheter insertions (Table 1).
Outcome specific definition following peritonitis.
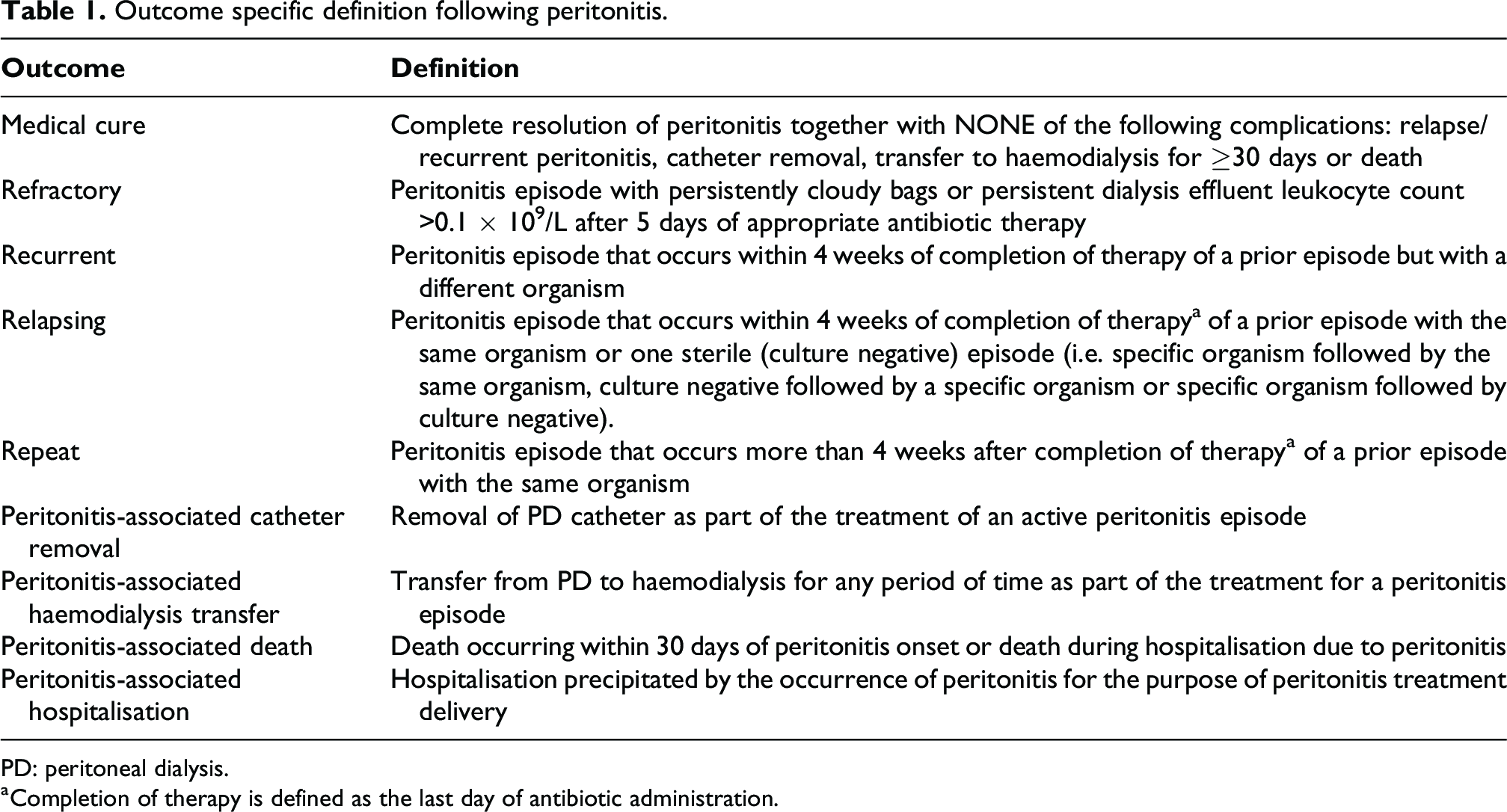
PD: peritoneal dialysis.
a Completion of therapy is defined as the last day of antibiotic administration.
Measurement and reporting of peritonitis.
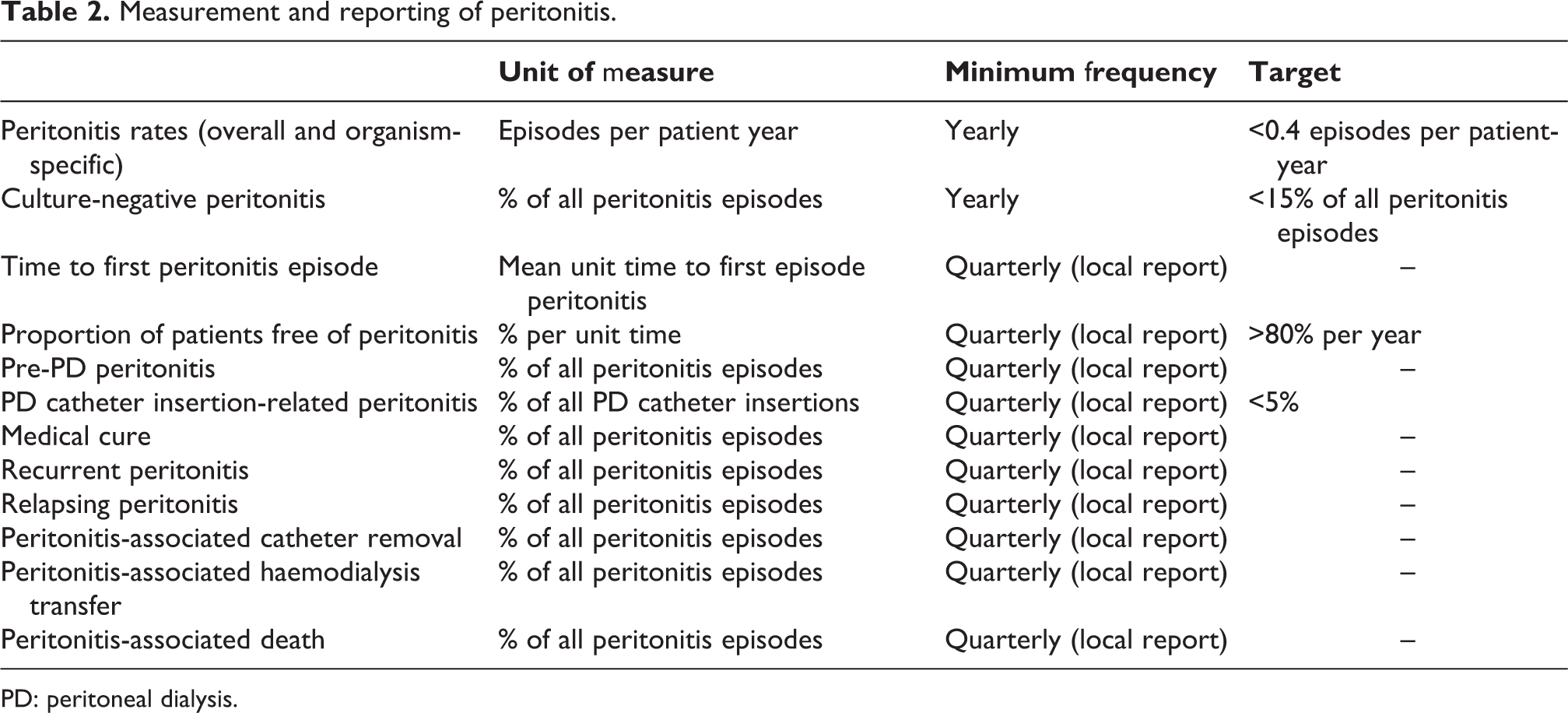
PD: peritoneal dialysis.
Outcome-specific definitions of peritonitis
We recommend using the definitions outlined in Table 2 to describe outcomes following peritonitis (Not Graded). All outcomes associated with the peritonitis episode should be captured.
Measuring, monitoring and reporting peritonitis
We recommend that every programme should monitor, at least on a yearly basis, the incidence and outcomes of peritonitis (1C).
We recommend that the parameters monitored should include the PD-related peritonitis rate, organism-specific peritonitis rates, antimicrobial susceptibilities of the infecting organisms, culture-negative peritonitis and peritonitis outcomes (1C).
We suggest PD units also measure and report other peritonitis parameters, including mean time to first peritonitis episode (where time counts from the first day of PD commencement), percentage of patients free of peritonitis per unit time (target >80% per year) and pre-PD peritonitis (2C).
We suggest that the rate of peritonitis be reported as number of episodes per patient-year (Not Graded).
We suggest that organism-specific peritonitis rates should be reported as absolute rates, that is, as number of episodes per year (Not Graded).
We recommend that the overall peritonitis rate should be no more than 0.40 episodes per year at risk (1C).
In addition to reporting peritonitis rate measured as number of episodes per patient-year, we suggest the culture-negative peritonitis be reported as a percentage of all peritonitis episodes per unit time (Not Graded).
We recommend the proportion of culture-negative peritonitis should be less than 15% of all peritonitis episodes (1C).
At regular intervals, all PD programmes should monitor the incidence of peritonitis as part of a continuous quality improvement (CQI) programme. 28 Application of a standardised metric to measure outcomes is critical to benchmark performance and monitor progress. Peritonitis rate should be measured as number of peritonitis episodes divided by number of patient years at risk (i.e. number of years on PD starting from the time of PD commencement), reported as episodes per patient years. For the purpose of calculating peritonitis rates, PD commencement is defined as the first day on which the first PD exchange was performed with the intention of continuing ongoing PD treatment (i.e. the first day of PD training or PD treatment in a hospital or at home with the intention of continuing PD long-term, whichever occurs first); this does not include intermittent flushing post-surgery to maintain catheter patency. Number of patient years at risk should be fully inclusive counting circumstances such as hospitalisation episodes where patients may not be performing their own PD. In terms of episodes, all subsequent relapsing episodes should be considered as an extension of the original episode and only the original episode captured as part of the peritonitis rate determination. Peritonitis episodes that occur during hospitalisations where nurses, patients or caregivers perform PD should also be counted as events for the purpose of calculating peritonitis rates. For quality improvement purposes, they should preferably be identified and characterised separately.
A recent study has proposed an alternative simplified formula for calculating peritonitis rates in which the denominator of patient years at risk is replaced by the average of the numbers of patients at the start and beginning of a year. 29 While this demonstrated reasonable overall agreement against the gold standard method when analysing Australian, New Zealand and French registry data, we suggest that peritonitis rates only be calculated using the gold standard method (i.e. number of episodes per patient year at risk) for the purpose of benchmarking using a standardised approach, and because the accuracy of the simplified method is sensitive to centre characteristics (i.e. less accurate in smaller centres or when centres are rapidly or unevenly losing or gaining patients over a year). The simplified method has also not been validated over shorter time periods than a year or outside of Australia, New Zealand and France.
Globally, there is a substantial (up to 20-fold) variation in peritonitis rates between PD units in different countries. 30 The PD Outcomes and Practice Patterns Study (PDOPPS) similarly reported variation in overall peritonitis rates from participating PD units (7051 adult PD patients in 209 facilities from seven countries) ranging from 0.26 (95% CI 0.24–0.27) episodes/patient-year in the United States to 0.40 (95% CI 0.36–0.46) episodes/patient-year in Thailand. 31 In separate studies, peritonitis rates have been reported to be as low as 0.16–0.20 episodes/patient-year in some PD units in China. 32 –34 In a systematic review based on a random-effects Poisson model of registries from 33 countries, the peritonitis rate has been steadily decreasing from 0.60 to 0.30 episodes/patient-year from 1992 to 2019. 35 We recommend that the overall peritonitis rate should be no more than 0.40 episodes per year at risk. 13 This is an improvement of standard of 0.5 episodes per year at risk as endorsed in the 2016 guideline. 13 From global review of data of reports from registries and studies, this is an achievable standard and should be used as an initiative to reduce peritonitis rates worldwide.
In addition to overall peritonitis rates, regular monitoring of organism-specific peritonitis and associated antimicrobial sensitivities can be helpful in informing appropriate empirical antibiotic regimens at a local level. Culture-negative peritonitis has been reported to affect between 13.4% and 40% of all episodes of peritonitis. 36 –38 The large variability in incidence of culture-negative peritonitis has been attributed to differences in the definition and technique of microbiological isolation. 39 Direct inoculation of sediment from centrifuged PD effluent into culture bottles has been shown to be most effective in identifying organisms responsible for peritonitis where appropriate resources are accessible. 39 The culture-negative peritonitis rate should be reported as percentage of all peritonitis episodes. We recommend the proportion of culture-negative peritonitis should be less than 15% of all peritonitis episodes.
We also suggest PD units measure and report other peritonitis parameters including, time to first peritonitis episode (where time counts from the first day of PD training/commencement), percentage of patients free of peritonitis per unit time (target >80% per year) and pre-PD peritonitis (episodes per year). Death associated with peritonitis may also be collected at a unit level, which can be defined as described in Table 1. 5 These additional outcomes may be captured and reported at a unit level on a monthly basis or at least quarterly to inform local practice (Table 2).
Prevention of peritonitis
Catheter placement
We recommend that systemic prophylactic antibiotics be administered immediately prior to catheter placement (1A).
Detailed description of the recommended practice of PD catheter insertion has been covered in the 2019 ISPD position paper. 27 There are four randomised, controlled trials on the use of perioperative intravenous cefuroxime, 40 gentamicin, 41 vancomycin 42 and cefazolin 41,42 as compared to no treatment. The overall benefit of prophylactic perioperative intravenous antibiotics was confirmed by a systematic review of these four trials, but its effect on the risk of exit-site/tunnel infection is uncertain. 43 Although first-generation cephalosporin may be slightly less effective than vancomycin, 42 the former is still commonly used because of the concern regarding vancomycin resistance. Each PD programme should determine its own choice of antibiotic for prophylaxis after considering the local spectrum of antibiotic resistance. No data exist on the effectiveness of routine screening and eradication of S. aureus nasal carriage before catheter insertion (such as intranasal mupirocin).
Exit-site care
Detailed description of exit-site care to prevent peritonitis should be referred to another guideline from ISPD. 17 At present, topical application of antibiotic cream or ointment to the PD catheter exit site is recommended although such practice varied among centres internationally. 44 Proper PD catheter immobilisation and avoidance of mechanical stress on the exit site may be useful to lower exit-site infection rate. 45 Prompt treatment of exit-site or catheter tunnel infection is mandatory to reduce subsequent peritonitis risk. 17 –19
Contamination of PD system
We suggest advice be sought immediately from the treatment team if contamination during PD exchange is noted (Not Graded).
We suggest prophylactic antibiotics after wet contamination of the PD system to prevent peritonitis (2D).
PD patients should be instructed to immediately seek advice from their dialysis centre if the sterility of PD exchange has been breached. When patients report contamination during an exchange procedure, the need for treatment is driven by distinguishing ‘dry contamination’ (contamination outside a closed PD system, such as disconnection distal to a closed clamp) from ‘wet contamination’ (referring to contamination with an open system, when either dialysis fluid is infused after contamination or if the catheter administration set has been left open for an extended period). Examples of wet contamination include leaks from dialysate bags, leaks or breaks in tubing proximal to the tubing clamp, breach of aseptic technique or touch contamination of the connection during a PD exchange. Prophylactic antibiotics is only recommended after wet contamination. 46,47 If it is unclear whether the tubing clamp was closed or open during contamination, wet contamination should be considered, for benefit of doubt. The common practice is thus change of a sterile transfer set. A PD effluent should preferably be obtained for cell count and culture after wet contamination. 47 A wet contamination should be monitored closely for an extended period, and a broader spectrum of organisms might lead to peritonitis, particularly in tropical centers. 48
One retrospective study involving 548 episodes of touch contamination revealed a relatively low rate of peritonitis (3.1%), and peritonitis occurred only after wet contamination (5.6%). Most episodes were coagulase-negative staphylococcal or culture-negative episodes, and the risk was significantly reduced by prophylactic antibiotics. 46 There is no standard regimen of prophylactic antibiotic.
Although short course of oral fluoroquinolones has been used previously, 46 the drug has now been discouraged by Food and Drug Administration (FDA) 49 unless there is no alternative options. One dose of intraperitoneal (IP) cefazolin is a reasonable option.
Invasive gastrointestinal and gynaecological procedures
We suggest antibiotic prophylaxis prior to colonoscopy (2C) and invasive gynaecological procedure (2D).
We suggest drainage of PD fluid to keep the abdomen empty before endoscopic gastrointestinal and invasive or instrumental gynaecological procedures (2D).
Peritonitis commonly follows endoscopic gastrointestinal and invasive or instrumental gynaecological procedures (e.g. gastroscopy, colonoscopy, hysteroscopy) in PD patients. 50 –57 The highest peritonitis complication rate after endoscopic or instrumental procedures is reported after invasive gynaecological procedures, ranging from 26.9% 57 to 38.5%. 58 Reported rates of peritonitis after colonoscopy without antibiotic prophylaxis ranged between 3.4% and 8.5%. 55,56 The rates of peritonitis after gastroscopy in PD patients range from 1.2% 58 to 3.9%. 59
Concerns about invasive or instrumental gynaecological procedures and peritonitis in PD patients come from the proximity of the pelvis to the peritoneal cavity. The most commonly reported bacterial pathogens in reported cases are Streptococcus, followed by Escherichia coli, Enterococcus, Staphylococcus and infrequently Candida. 57 Data supporting antibiotic prophylaxis come from two small retrospective studies. 57,58 In a retrospective study of 26 gynaecological procedures on 18 PD patients, none of the 11 procedures with antibiotic prophylaxis was followed by peritonitis, as opposed to a peritonitis occurrence of 47% among those procedures performed without antibiotic prophylaxis. 57 An earlier study reported a similar finding of less common peritonitis occurrence after antibiotic prophylaxis, but the difference did not reach statistical significance: none of four patients with prophylactic antibiotic administration developed peritonitis whereas 55.6% without antibiotic prophylaxis developed peritonitis. 58 Because of limited data, there is no standardised recommendation of antibiotic choice and administration route. However, reasonable regimens should cover gram-positive and gram-negative (aerobic and anaerobic) bacterial isolates from the upper tract of female reproductive tracts. Examples include intravenous cefazolin or ceftriaxone before the procedure or oral cefadroxil 500 mg once daily for 3 days. 57
More than half of reported peritonitis episodes occurring after colonoscopy are caused by E. coli. 55 , 60 In a single-centre study of 97 colonoscopies performed in 77 continuous ambulatory peritoneal dialysis (CAPD) patients, none of the 18 patients having a colonoscopy procedure with antibiotic prophylaxis developed peritonitis, as opposed to a 6.3% peritonitis occurrence among those undergoing colonoscopy without antibiotic prophylaxis. 50 This is consistent with a more extensive multicentre study of 236 colonoscopy procedures, in which none of the 65 patients who received antibiotic prophylaxis developed peritonitis, compared to a peritonitis rate of 3.8% for those without prophylactic antibiotics. 55 Furthermore, therapeutic procedures, such as polypectomy and endoscopic mucosal resection, are predictive of peritonitis. 55,60 The optimal antibiotic regimen for preventing peritonitis after colonoscopy has not been determined by clinical study. The only randomised controlled trial of prophylactic antibiotics used IP ceftazidime (1 g IP 1 h before the procedure) and recruited 93 patients receiving APD without a history of peritonitis in the last 12 months from a single centre in Saudi Arabia. The peritonitis rate did not differ with (6.5%) and without (8.5%) IP ceftazidime prophylaxis (p = 0.27). 56 For intravenous antibiotic prophylaxis, potential choices include cephalosporins (such as ceftriaxone or ceftazidime), amoxicillin–clavulanate, ampicillin–sulbactam, ampicillin plus aminoglycoside, 50,58 with an aim to target most of the organisms described above that cause peritonitis after colonoscopy. Interestingly, the alternative option of oral antibiotic prophylaxis was suggested by a recent case series of 49 PD patients who received oral ampicillin 1000 mg, ciprofloxacin 500 mg and/or metronidazole 250 mg 1 to 2 h before colonoscopy and did not experience any post-procedure episodes of peritonitis. 61 Finally, PD effluent should be drained to keep patient’s abdomen empty before colonoscopy (and gynaecological) procedure. 62 The argument for emptying the abdomen before colonoscopy is to enhance host defence, 63 because the peritoneal macrophage phagocytic function and polymorphonuclear cell function are suppressed by the presence of dialysate. 64 Furthermore, high fluid volumes can compromise efficiency of bacterial killing by disrupting the volume-to-surface-area ratio. 65
The risk of PD patients developing peritonitis after gastroscopy is more uncertain. Other than case reports 66,67 and a small case series, 58 a single-centre observational study of 408 gastroscopy procedures in 216 PD patients showed a 3.9% incidence of peritonitis within 1 week of endoscopy. 59 Patient’s age and the number of endoscopic biopsies predicted peritonitis risk. One-quarter of the 16 peritonitis episodes were polymicrobial, commonly caused by organisms either enteric in origin or arising from the oral cavity, such as Streptococcus. 59 Although there is insufficient evidence to recommend antibiotic prophylaxis prior to gastroscopy in PD patients, the study confirmed a lower odds of peritonitis after gastroscopy, after adjustment for confounding factors, when antibiotics were used within 7 days of gastroscopy. 59
Training programme
We suggest that the characteristics of an optimal PD training programme (how, how long, where, when and by whom) remain uncertain (2C).
We recommend that PD exchange technique and knowledge be regularly reassessed and updated, with an emphasis on direct inspection of practice of PD technique (1C).
Detailed description on the recommended practice of PD training has been covered in another ISPD guideline, 68,69 which each PD programme should consult while preparing the trainer and developing a specific curriculum for PD training. Unfortunately, limited data are available to guide when, how or how long PD training is optimal. The PDOPPS noted marked variation in training practices across 120 facilities across seven countries; timing of commencement, duration of training, location or use of competency assessments were not predictive of peritonitis risk. 70 Taken together, flexibility should be allowed to deliver training according to local resources and individualised to patients’ needs. Furthermore, distance learning and remote monitoring have been increasingly utilised. Previously, hybrid PD education programme with online video material has been developed and shown to be associated with lower peritonitis rate. 71 On the other hand, a single-centre study reported that face-to-face patient–doctor contact intervals less frequent than every 2 months was associated with higher peritonitis rate. 72
In essence, all PD trainers should receive adequate education to perform training and further education to update and hone their teaching skills. Each programme should have an established curriculum that is followed in teaching the patient the procedure, theory of PD and self-care, taking into account the individual’s learning style. Testing the patient’s practical skills at the end of training is essential.
After PD training is completed and patients are started on home PD, a home visit by the PD nurse is often helpful in detecting problems with exchange technique, adherence to protocols and other environmental and behaviour issues which increase the risk of peritonitis. Observational studies reported a non-significantly lower peritonitis rates associated with home visit programmes in paediatric 73 and adult 74 PD patients. Another registry data set showed an independent association of nurse visits before starting PD with a lower likelihood of peritonitis. 75
In addition to the initial training, refresher course or retraining plays an important role in reducing mistakes according to learning specialists. 76 Previous studies showed that adherence with exchange protocols was significantly associated with peritonitis rate, 76 which applied even during the coronavirus pandemic when behaviour for personal hygiene is anticipated to be enhanced. 77 The purpose of retraining is to target patients who have begun to take shortcuts or simply deviate from the standard steps which they were taught previously. An observational study found that 6 months after the initiation of PD, around half of the patients took shortcuts, modified the standard exchange method, failed to follow appropriate hand hygiene protocols properly or follow the aseptic technique. 78 Despite common usage of the term ‘retraining’ in literature, the healthcare providers should be mindful of the implicit negative connotation of this word. Emphasis for updating of knowledge and technique should be used to address the benefit. Home visits by PD nurses or trained personnel may be a good way to determine which patients require retraining. 76 Other indications of retraining are listed in Table 3 68,79 Certainly, all patients must be retrained whenever the equipment to perform PD is changed. Evidence for retraining PD is evolving as an increasing number of randomised controlled trials have been completed. 80 –82 The optimal timing and frequency of retraining remain uncertain but a randomised controlled trial lends strong support for more frequent retraining at home. As compared to 53 PD patients receiving conventional retraining (two home visits within two months after starting dialysis), 51 incident PD patients randomised to frequent retraining (regular repeated home visits every 1–3 months over 2 years) showed a significantly lower rates of exit site infection and peritonitis. 80 Moreover, subgroup analysis demonstrated a significant beneficial effect on the first episode of peritonitis in patients older than 60 years. 80 Their results were not able to be replicated in another randomised controlled trial, with a larger sample size, of retraining intervention targeting incident PD patients who failed regular testing of PD knowledge and practical PD skill assessment. 81 Furthermore, it has been proposed that practical assessment of PD technique is more important than testing of theory. Patients might not be aware of their making mistakes in PD procedures until the visiting nurse discovers them. The best support for emphasis on practical assessment of patients’ techniques comes from a controlled trial randomising incident PD patients to retraining via technique inspection, oral education or usual care. 82 The oral education group (retraining every 2 months using a checklist and focus on knowledge) did not reduce the risk of peritonitis, whereas the technique inspection group (retraining every 2 months and focus on behaviour by nurses’ inspection of PD technique) demonstrated a lower risk of first non-enteric peritonitis. 82 In other words, the most effective learning is through direct feedback immediately after return demonstration of PD steps.
Indications for PD Retraining.
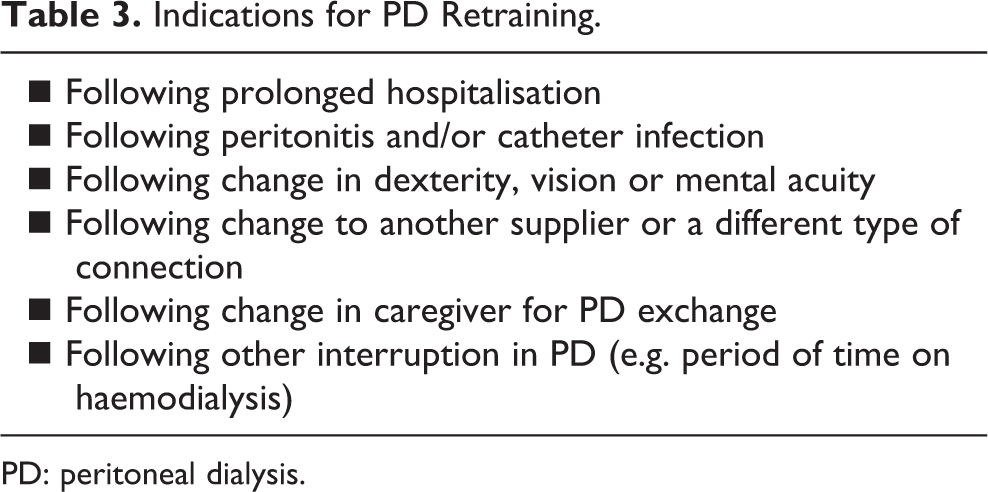
PD: peritoneal dialysis.
Domestic pet and zoonotic infection
We recommend PD patients take extra precautions to prevent peritonitis if domestic pets are kept (1C).
We suggest pets not be allowed in the room where PD exchange takes place, and where dialysis tubing, equipment and machine are stored (2A).
PD patients should be asked about pets during training and home visits or after a diagnosis of unusual organisms suspicious of zoonoses because peritonitis due to zoonotic organisms can occur in the context of close contact with companion animals. 83,84
With regard to cats, more than 40 cases of Pasteurella multocida peritonitis have been reported in the literature. 85 Despite the name ‘cat-bite peritonitis’, 86 the aerobic gram-negative coccobacillus P. multocida is found in the upper respiratory tract and oral cavity of many domestic and wild animals including dogs and hamsters. Direct contact with animals, either through close contact with PD equipment or patient, bites or scratches, can be implicated in PD-related infections. The prevalence of colonisation with P. multocida is higher in cats, including their claws. 87 Other cat-related organisms include Capnocytophaga canimorsus, Capnocytophaga cynodegmi and Neisserria species. 84,88 The frequency of cat-related peritonitis is higher in patients on APD than CAPD, possibly secondary to the longer tubing required or the prolonged environmental contact time of equipment for APD. Cycler tubing moving with the action of the cycler pump is another stimulus that may entice a cat to play with the instrument. Furthermore, cats enjoy the warmth of the cycler heat plate and may lay on the dialysis machines. 85
The hidden pet-related damage to PD tubing that occurs when animals bite or scratch the tubing should be emphasised as the damage may go unnoticed when APD patients are sleeping. The small pinhole-shaped damage, as opposed to a complete tear, can also be challenging to detect until leakage of PD solution occurs. Such minor but serious tubing defects have been reported in PD patients who cohabitate with pets including cats, hamsters and cockatoo. 86,88 –93
With the bonds between owners and domestic pets being potentially very strong, and possible emotional and quality-of-life benefits, it is not always possible to discourage keeping pets. Around one-fifth of PD patients surveyed in a single PD centre were keeping pets. 94 To minimise the risk of pet-related peritonitis, PD patients should adhere to stringent hand washing before and after PD exchanges and handling pets, as well as ensuring high home environment hygiene standards. Domestic pets should be strictly kept away from the dialysis equipment and should not be allowed into the room during the dialysis treatment procedure.
Other modifiable risk factors
We suggest that avoidance and treatment of hypokalaemia may reduce the risk of peritonitis (2C).
We suggest that avoiding or limiting the use of histamine-2 receptor antagonists may prevent enteric peritonitis (2C).
A number of other modifiable risk factors for PD peritonitis have been described. One of the investigation tools is the undertaking of a large international cohort study, such as the Peritoneal Dialysis and Outcomes Practice Patterns Study (PDOPPS), to collect detailed information in a uniform manner. 31,70,95,96 The results obtained from PDOPPS provide a high-level overview of peritonitis risk factors and outcomes across countries and PD centres but require further prospective interventional studies to establish causation.
Gastrointestinal problems, such as constipation and enteritis, have been reported to be associated with peritonitis due to enteric organisms. 97 PDOPPS also reported an association of higher peritonitis risk with gastrointestinal bleeding. 31 A previous study reported an association of hypokalaemia with a higher risk of enteric peritonitis. 98 International data from seven countries, under PDOPPS, showed that hypokalaemia persistent for 4 months was associated with 80% higher subsequent peritonitis rates after adjustment for confounders. 95 The causative organisms underpinning the excess of peritonitis were mostly gram positive and culture negative. This concurs with another Brazilian propensity-matched score study linking hypokalaemia with higher infection-related mortality and peritonitis risk. 99 In addition to the degree of hypokalaemia, the duration of hypokalaemia was associated with the risk of peritonitis in PD patients. 100 Although there is no compelling evidence that treatment of hypokalaemia, constipation or gastroenteritis mitigates the risk of peritonitis, such problems, which are common in the PD setting, merit treatment in their own right. Based on previous observational and mechanistic studies of hypokalaemia in PD studies, the main contributory factor of hypokalaemia is low dietary potassium intake, rather than increased potassium excretion or intracellular shift. 101,102 Dietary intervention is recommended to mitigate hypokalaemia. Observational data from a single-centre study suggested that regular lactulose use is associated with a lower rate of peritonitis. 103 However, the benefit of lactulose to reduce peritonitis rate, compared with sennosides, has not been confirmed in a single-centre randomised controlled trial. 104
There are emerging data to suggest that gastric acid suppression, especially with histamine-2 receptor antagonists, is a modifiable risk factor for enteric peritonitis in PD patients. The hazard ratio for enteric peritonitis, as demonstrated in an observational cohort of 119 PD patients on histamine-2 receptor antagonists, was 1.67 (95% confidence interval 1.02–2.80). The increase in infectious mortality among histamine-2 receptor antagonist users further supported the burden of this risk. 105 However, the risk of peritonitis associated with proton pump inhibitors is less consistently reported. 106 –108 A similar finding of heightened risk conferred by the use of histamine-2 receptor antagonists, but not proton pump inhibitors, was found in a case series of peritonitis after gastroscopy. Of note, histamine-2 receptor antagonist users had a significantly higher post gastroscopy peritonitis rate (9.4%) compared to non-users (2.9%). 59 A meta-analysis of six non-randomised studies involving pooled data of 829 PD patients showed that histamine-2 receptor antagonist use was associated with an increased odds of enteric peritonitis (OR 1.4, 95% CI 1.01–1.93). 108 Notably, even though the association between proton pump inhibitor use and peritonitis is less compelling, other concerns with proton pump inhibitors (including but not limited to Clostridioides infection) do not justify a routine switching of histamine-2 receptor antagonist to proton pump inhibitor therapy.
Secondary prevention
To prevent fungal peritonitis, we recommend that anti-fungal prophylaxis be co-prescribed whenever PD patients receive an antibiotic course, regardless of the indication for that antibiotic course (1B).
The majority of fungal peritonitis episodes are preceded by courses of antibiotics. 109 –112 A number of observational studies 113 –120 and randomised trials 121,122 have examined the use of either oral nystatin (500,000 units qid) or fluconazole (200 mg every 48 h) as prophylaxis during antibiotic therapy. In essence, two randomised control trials 121,122 and a systematic review 43 showed a significant benefit. Most of the other reports on the prophylactic use of antifungals during antibiotic administration were non-randomised studies and have yielded mixed results. Unfortunately, nystatin is not available in some countries. Observational data 118 –120 and one randomised controlled trial 122 showed that prophylactic fluconazole is effective. The randomised controlled trial of oral fluconazole included patients who received antibiotics for treating exit-site and tunnel infection, in addition to the treatment of peritonitis 122 . However, there are potential problems (including drug interactions, emergence of resistant strains) with fluconazole prophylaxis. Overall, a Cochrane meta-analysis of the two randomised controlled studies on antifungal prophylaxis with oral nystatin or fluconazole showed a risk ratio of 0.28 (95% CI 0.12–0.63) for fungal peritonitis occurring after a patient has had an antibiotic course. 43
Furthermore, each episode of peritonitis should be considered a preventable event and hence evaluated. 47 The CQI programme provides a means in secondary prevention. For each peritonitis episode, a root-cause analysis should be performed to determine the aetiology and, whenever possible, an intervention directed against any reversible risk factor should be made to prevent another episode. For example, Streptococcal viridans peritonitis could have indicated dental problems although such link is based on isolated case reports only. 123,124 Peritonitis episodes caused by coagulase-negative staphylococcal species are associated with touch contamination, while S. aureus infections have been associated with touch contamination or catheter infections. Identification of aetiology may involve review of the exchange technique. Retraining is sometimes necessary. Rarely, an outbreak of culture-negative peritonitis or peritonitis secondary to unusual organisms should trigger epidemiological investigation and field visit to look for environment risk factors such as PD fluid, hospital air or water contamination. 125 –127
Initial presentation and management of peritonitis
The algorithm of initial management for PD patients presenting with a clinical diagnosis is summarised in Figure 1.
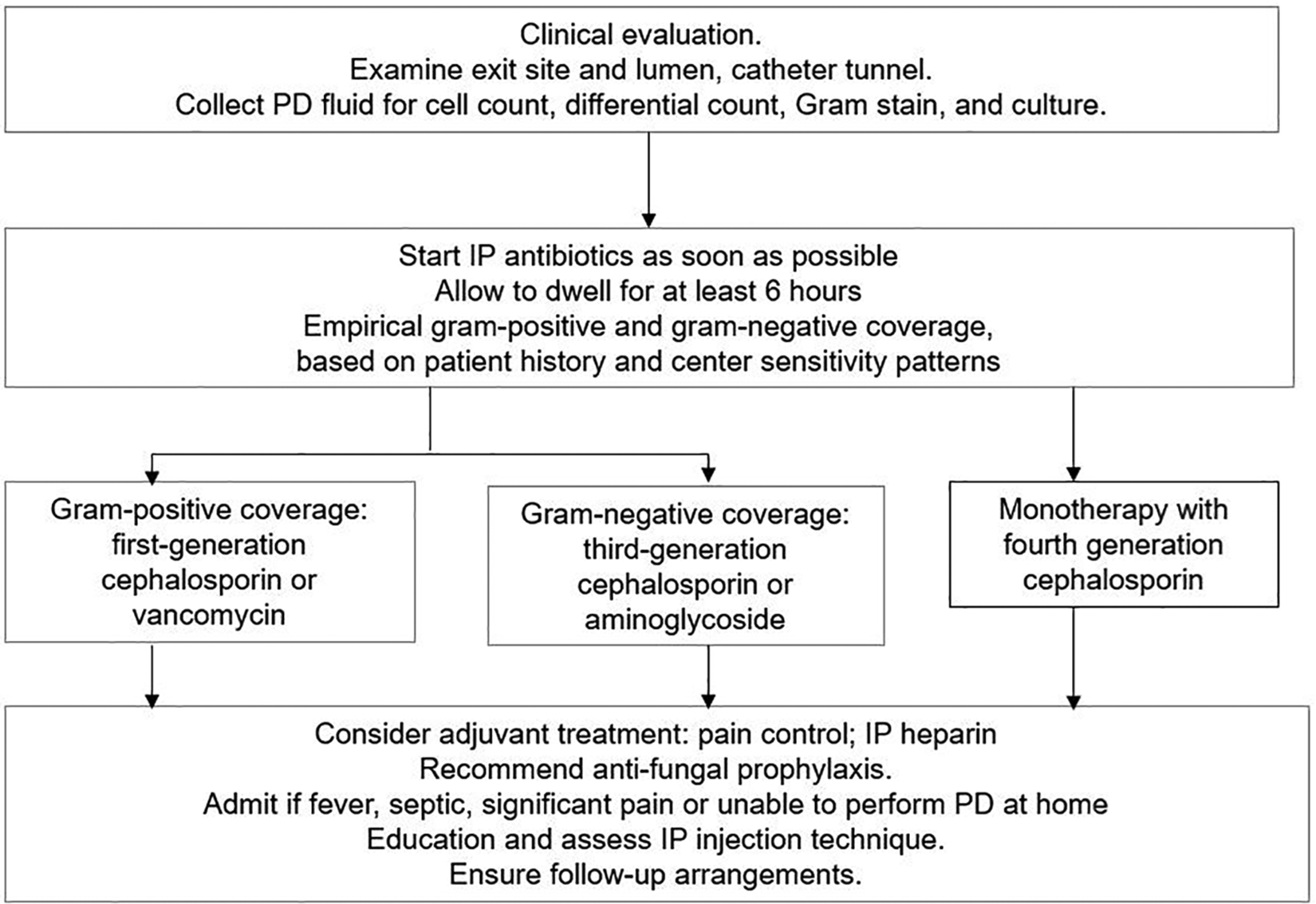
The algorithm of initial management for PD patients presenting with a clinical diagnosis of peritonitis. PD: peritoneal dialysis.
We recommend that peritonitis always be diagnosed when at least two of the following are present: (1) clinical features consistent with peritonitis, that is, abdominal pain and/or cloudy dialysis effluent; (2) dialysis effluent white cell count >100/µL or >0.1 × 109/L (after a dwell time of at least 2 h), with >50% PMN; and (3) positive dialysis effluent culture
We recommend that PD effluent be tested for cell count, differential, gram stain and culture whenever peritonitis is suspected
We recommend that PD patients presenting with cloudy effluent be presumed to have peritonitis and treated as such until the diagnosis can be confirmed or excluded
Patients with peritonitis usually present with cloudy PD effluent and abdominal pain. Cloudy effluent almost always represents infectious peritonitis, although there are other differential diagnoses classified according to cellular and non-cellular causes (Table 4). 128 Some patients present with cloudy effluent but no or minimal abdominal pain. On the other hand, peritonitis should also be included in the differential diagnosis of the PD patient presenting with abdominal pain, even if the effluent is clear. In addition to the presenting symptoms, the patient should be questioned about any recent contamination, accidental disconnection, endoscopic or gynaecological procedures, as well as the presence of constipation or diarrhoea. In addition, the patient should be questioned about past history of peritonitis and exit-site infection.
Differential diagnosis of cloudy effluent.
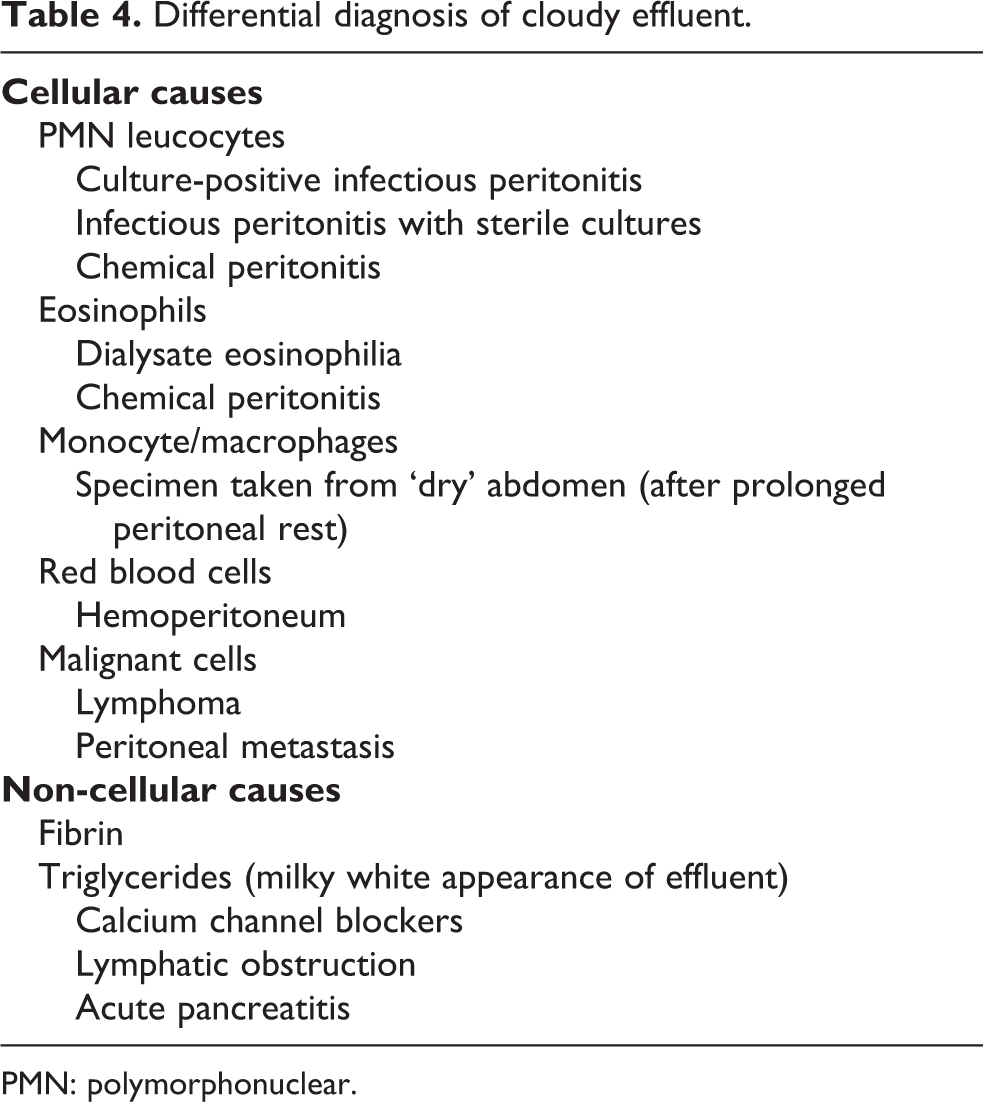
PMN: polymorphonuclear.
On physical examination, abdominal tenderness is typically generalised and is less often associated with a rebound. Localised pain or tenderness should raise the suspicion of underlying surgical pathology. Physical examination should also include a careful inspection of the catheter tunnel and exit site. Any discharge from the exit site should be cultured. Erythema, tenderness and the presence of fluid collections (which may be confirmed with ultrasound) along the PD catheter tunnel may be indicative of a tunnel infection. The degrees of abdominal pain and tenderness are important factors in deciding whether a patient requires hospital admission. In general, patients with minimal pain could be treated on an outpatient basis with IP antibiotic therapy if this can be arranged. Follow-up within 3 days is advisable to confirm resolution and appropriateness of the antibiotic choice.
When peritonitis is suspected, dialysis effluent should be drained, carefully inspected and sent for cell count with differential, Gram stain and culture. 129 An effluent cell count with WBC > 100/µL (after a dwell time of at least 2 h), with > 50% PMN, is highly suggestive of peritonitis. 130 Abdominal X-ray is generally not necessary and may be potentially misleading since pneumoperitoneum is common (around one-third of CAPD patients) 131 secondary to air entry into the peritoneal cavity via the PD catheter during exchanges. Peripheral blood cultures are usually negative 132 and can be omitted unless the patient is clinically septic 133 or on immunosuppression. 134 Bacteraemia during peritonitis should raise the possibility of other intra-abdominal events. 135,136 To prevent delay in treatment, antibiotic therapy (see below) should be initiated once the appropriate dialysis effluent specimens have been collected, without waiting for the results of laboratory testing.
The WBC count in the effluent depends in part on the length of the dwell. For patients on APD with rapid cycle treatment, the clinician should use the percentage of PMN rather than the absolute WBC count to diagnose peritonitis, and a proportion above 50% PMN is strong evidence of peritonitis, even if the absolute WBC count is less than 100/µL. 130 On the other hand, APD patients without a daytime exchange presenting with abdominal pain during the daytime may have no effluent to drain. In this case, 1 L of dialysis solution should be infused, dwelled for 2 h, and then drained for inspection and laboratory testing.
Identification of causative organisms
We recommend that the blood culture bottle(s) be the preferred technique for bacterial culture of PD effluent (1C).
We suggest that sampling and culture methods be reviewed and improved if more than 15% of peritonitis episodes are culture negative (2C).
Gram stain of the PD effluent should be performed even though the result is often negative. 137,138 An additional benefit of Gram stain is its effectiveness in early detection of fungal elements, facilitating timely diagnosis and management of fungal peritonitis. 139 The diagnostic yield of the Gram stain is increased if it is performed on a centrifuged specimen. An appropriate method of culturing PD effluent is the most important step in establishing the causative organism. In some specialised centres, it has been possible to achieve a culture-negative peritonitis rate of less than 10%. Identification of the organism and subsequent antibiotic sensitivities help to guide the choice of antibiotic, and the type of organism often indicates the possible source of infection. Bedside inoculation of 5–10 mL effluent in two (aerobic and anaerobic) blood-culture bottles has a reasonable sensitivity, and the culture-negative rate is typically around 10–20%. 140 -143 The yield of peritoneal fluid culture is enhanced by inoculating the fluid directly into rapid blood-culture bottle kits (e.g. BACTEC, Kent, UK; Septi-Chek, Roche Diagnostics, Basel, Switzerland; BacT/Alert, Biomerieux, Inc., Basingstoke, UK), centrifuging PD fluid and culturing the pellet or the lysis centrifugation technique as compared to inoculation into standard blood-culture bottles. Specifically, centrifugation of 50 mL PD effluent at 3000 g for 15 min, followed by resuspension of the sediment in 3–5 mL supernatant and inoculation on solid culture media or standard blood-culture media, increases the yield by 5–10 times. 39,142,143 The combination of water lysis, Tween-80 blood agar and Triton-X treatment of the PD effluent is also a sensitive culture method. 144,145 The specimens should arrive at the laboratory within 6 h. If immediate delivery to the laboratory is not possible, the inoculated culture bottles should ideally be incubated at 37°C. Inoculated bottles should not be refrigerated or frozen, since it may kill or retard the growth of some microorganisms. 146 The solid media should be incubated in aerobic, microaerophilic and anaerobic environments. To fully assess yeast and filamentous fungal pathogens, appropriate fungal media should be selected; incubation of inoculated media under two temperature conditions (room temperature and 35–37°C) can increase the diagnostic yield. 146
The speed with which bacteriological diagnosis can be established is very important. Concentration methods not only facilitate microbial identification, but also reduce the time needed for a positive culture. In over 75% of cases, microbiologic diagnosis can be established in less than 3 days. When the causative microorganism has been identified, subsequent cultures for monitoring may be performed by only inoculating the effluent in blood-culture bottles.
In a prospective study using facility-level data over 22 PD centres, immediate transfer of specimens or inoculated bottles to laboratories and the practice of PD effluent centrifugation are associated with lower culture-negative peritonitis rates. 146 Notably, experience of the centre is important because culture-negative peritonitis rates frequently show an inverse relationship with the PD centre size. 38,146
When cultures remain negative after 3–5 days of incubation, PD effluent should be sent for repeat cell count, differential count, fungal and mycobacterial culture. In addition, subculture on media with aerobic, anaerobic and microaerophilic incubation conditions for a further 3–4 days may help to identify slow-growing fastidious bacteria and yeasts that are undetectable in some automated culture systems. Furthermore, culture of the PD catheter can improve the diagnostic yield, especially for detection of fungi and enterococci. 147
Other novel diagnostic techniques
A number of novel diagnostic techniques have been explored for the early diagnosis of peritonitis, including leukocyte esterase reagent strips, 148 biomarker assays (matrix metalloproteinase-8 and -9, 149 neutrophil gelatinase-associated lipocalin 150 and procalcitonin), polymerase chain reaction (PCR) for bacterial-derived DNA fragments, PCR/electrospray ionisation–mass spectrometry assay, 151 16 S rRNA gene sequencing, 152 matrix-assisted laser desorption ionisation-time of flight mass spectrometry 153 and pathogen-specific ‘immune fingerprints’. 154,155 However, none of them has been proved to be superior to conventional techniques. Immune fingerprint, for instance, by multicolour flow cytometry and multiplex enzyme-linked immunosorbent assay, has been shown to discriminate between culture-negative, gram-positive, gram-negative episodes of peritonitis but provides no information on antibiotic resistance. 155 Further refinement using mathematical machine-learning algorithms can characterise specific pathogens like streptococcal species and coagulase-negative staphylococci in a point-of-care manner. 154 Utility of PD effluent phenotyping approach or immune fingerprinting remains to be validated before application to clinical use. In addition, a point-of-care device measuring levels of matrix metalloproteinase-8 and interleukin-6 has been tested to expedite diagnosis of peritonitis but is more useful to exclude peritonitis with a high negative predictive value over 98%. 156
For rapid diagnosis of fungal peritonitis, PD effluent and serum galactomannan index might offer a faster turnaround time than the conventional culture method, but with a diagnostic accuracy of 65.2% sensitivity, 85.0% specificity only. 157,158 False-positive galactomannan results 159 leading to unnecessary use of antifungals is a definite concern.
Empiric antibiotic selection
We recommend that empirical antibiotic therapy be initiated as soon as possible, using either IP or systemic route, after appropriate microbiological specimens have been obtained (1B).
We recommend that empirical antibiotic regimens be centre-specific and cover both gram-positive and gram-negative organisms (1C).
We recommend that gram-positive organisms be covered by a first-generation cephalosporin or vancomycin and gram-negative organisms by a third-generation cephalosporin or an aminoglycoside (1B).
We suggest that cefepime monotherapy may be an acceptable alternative for empirical antibiotic regimens (2B).
Once the diagnostic investigations have been completed, empirical antibiotics should be started to achieve rapid resolution of inflammation, reduction of pain and preservation of the peritoneal membrane. No single antibiotic regimen has been proven to be superior to others, 160 and the choice should be centre-specific. There should be adequate coverage for both gram-positive and gram-negative organisms. A national registry confirmed that centres with higher proportions of peritonitis episodes receiving complete empirical coverage for both gram-positive and gram-negative organisms at presentation had higher odds of peritonitis cure by antibiotics. 161 For the coverage of gram-positive organisms, vancomycin or first-generation cephalosporin is recommended. Cefazolin might be preferred to vancomycin when there is concern about emergence of organisms resistant to the latter. However, vancomycin should be considered in centres with a high prevalence of methicillin-resistant organisms. 162 The threshold prevalence of methicillin resistance that justifies empirical use of vancomycin remains controversial. No discernible difference in peritonitis cure rate was found between empirical cefazolin and vancomycin use for gram-positive or culture-negative peritonitis, according to observational data from PDOPPS. 96 For the gram-negative coverage, third-generation cephalosporin or aminoglycoside is suggested. Observational studies 163,164 and one randomised controlled trial 165 showed that aminoglycoside does not accelerate the loss of residual kidney function. However, repeated or prolonged aminoglycoside treatment was associated with a high incidence of vestibular toxicity or ototoxicity. 166 It is also important to mention that treatment failure with ceftazidime is high with rising prevalence of extended-spectrum beta-lactamases (ESBL)-producing organisms. A recent analysis from PDOPPS reported that, for treatment of gram-negative peritonitis, empirical aminoglycoside was associated with a higher likelihood of medical cure than ceftazidime. 96 Monotherapy for empirical treatment of peritonitis, instead of combination therapy, has now been accepted as an effective strategy. Two randomised controlled trials 167,168 and one observational prospective study 169 testing the use of IP cefepime monotherapy have been published. Although there were differences in cefepime dosing (intermittent, continuous, with and without adjustment for residual kidney function), all three studies showed primary response rates exceeding 80% on day 10. 167 –169 In particular, the largest study used a non-inferiority design and specified adjustment for residual kidney function by increasing the loading and maintenance doses of cefepime by 25% for urine volume more than 100 mL daily. Cefepime monotherapy was shown to be effective and non-inferior to standard dual therapy with cefazolin plus ceftazidime. 168 In contrast, monotherapy with quinolones is not recommended because of the concern with emergence of resistant organisms and declining effectiveness. 162,170
It is important to note that prompt administration of antibiotics has been consistently shown to be associated with better outcome of peritonitis treatment. In a prospective multicentre study of 159 peritonitis episodes in Western Australia, the contact-to-treatment time was independently associated with treatment failure, defined as either catheter removal or death at 30 days. For each hour of delay in administering antibiotic therapy from the time of presentation to a hospital facility, the risk of PD failure or death was higher by 5.5%. 171 In another retrospective study of 109 peritonitis episodes, a delay of starting IP or intravenous antibiotics treatment from the sign of peritonitis by 24 h conferred a threefold risk of peritoneal catheter removal by multivariate analysis. 172 For logistics consideration, immediate IP antibiotic administration might not be feasible in the emergency department or wards in which staff are not familiar with PD. In order to avoid the adverse outcome of delayed peritonitis treatment, the systemic route should be started as a temporary measure when there is a foreseeable delay, such as long wait for dialysis unit bed or presentation outside the working hours of the ambulatory PD unit. However, the route of administrating antibiotics should still be switched to IP as soon as possible.
Dosage of antibiotics
We recommend that IP antibiotics be the preferred route of administration as long as the compatibility and stability of the IP antibiotics allow, unless the patient has features of systemic sepsis (1B).
We suggest that IP aminoglycoside be administered as daily intermittent dosing (2B).
We recommend that prolonged courses of IP aminoglycoside be avoided (1C).
We suggest that adjunctive oral N-acetylcysteine therapy may help to prevent aminoglycoside ototoxicity (2B).
There is insufficient evidence to make a recommendation as to whether patients on APD should be temporarily switched to CAPD during treatment of peritonitis (Not Graded).
The recommended dosage of antibiotics for the treatment of PD-related peritonitis is summarised in Table 5 (IP antibiotics) and Table 6 (systemic antibiotics). However, the recommended dosages of many antibiotics are based on published clinical experience rather than formal pharmacokinetic studies. Most studies of IP antibiotics have been conducted in patients on CAPD rather than in patients on APD.
IP antibiotic dosing recommendations for treatment of peritonitis.
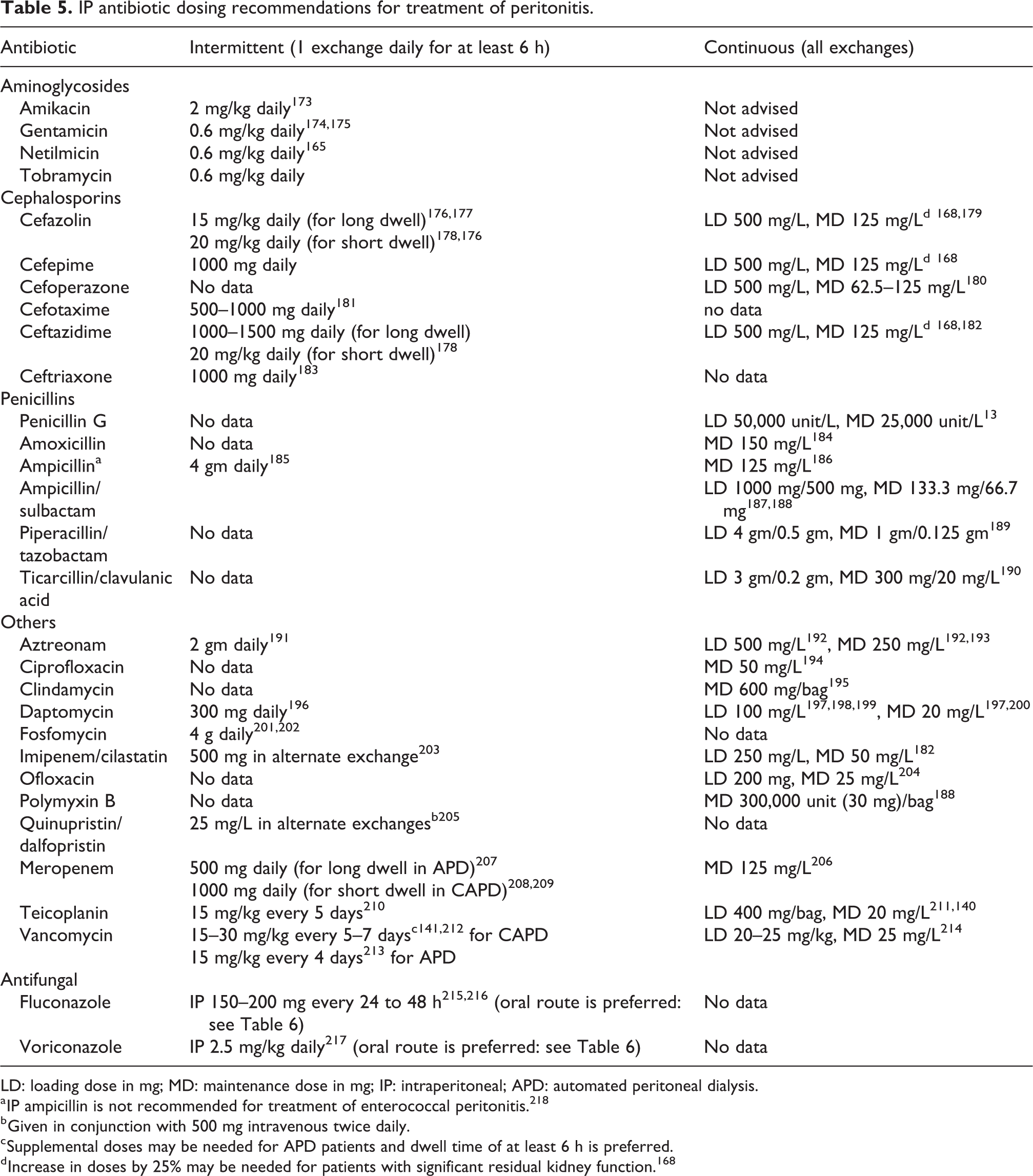
LD: loading dose in mg; MD: maintenance dose in mg; IP: intraperitoneal; APD: automated peritoneal dialysis.
a IP ampicillin is not recommended for treatment of enterococcal peritonitis. 218
b Given in conjunction with 500 mg intravenous twice daily.
c Supplemental doses may be needed for APD patients and dwell time of at least 6 h is preferred.
d Increase in doses by 25% may be needed for patients with significant residual kidney function. 168
Systemic antibiotic dosing recommendations for treatment of peritonitis.
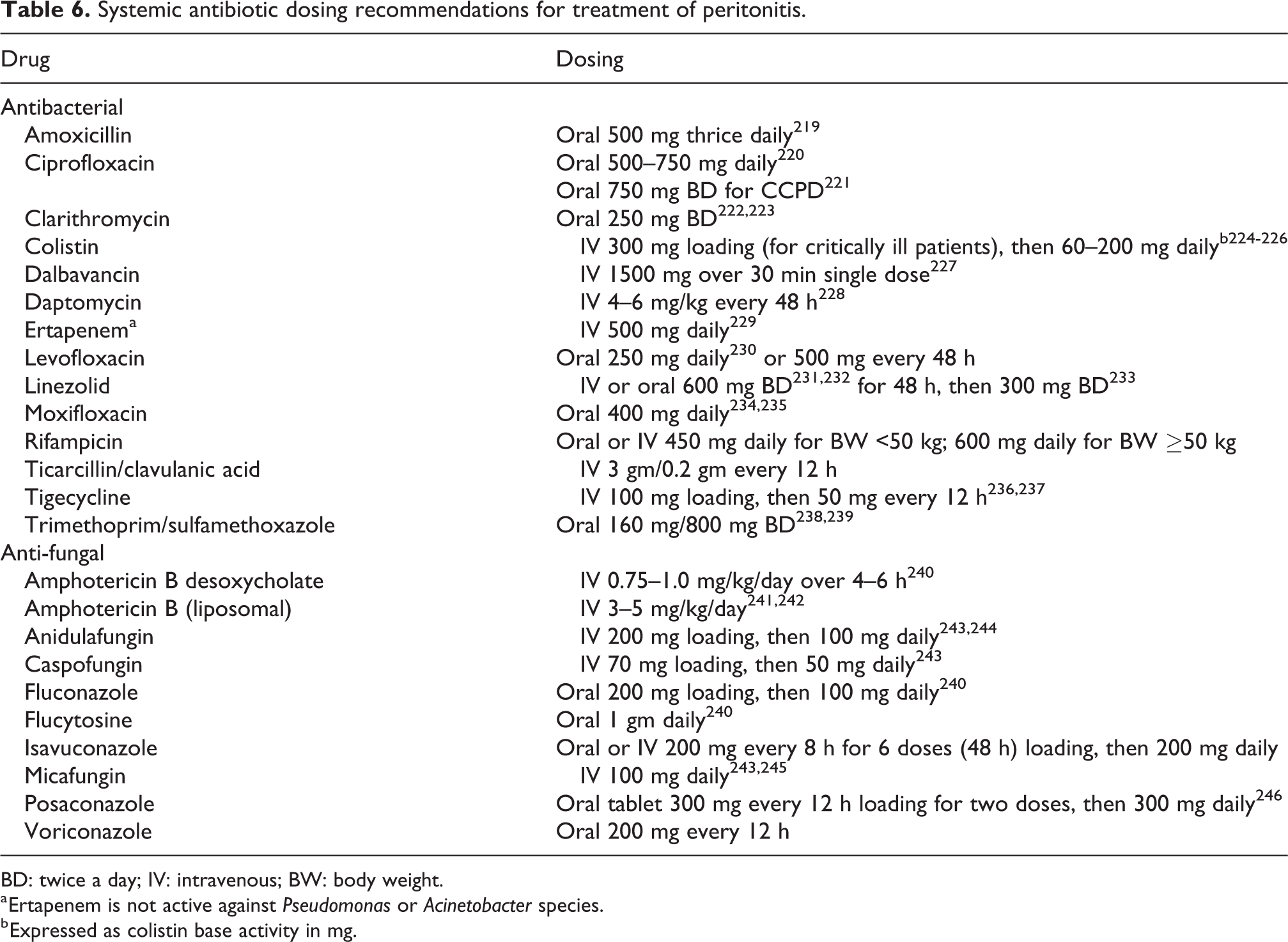
BD: twice a day; IV: intravenous; BW: body weight.
a Ertapenem is not active against Pseudomonas or Acinetobacter species.
b Expressed as colistin base activity in mg.
The importance of adequate dosing of antibiotics was supported by an observational study of 339 episodes of gram-positive, gram-negative and culture-negative PD-related peritonitis, in which treatment failure was higher for patients with greater residual kidney function defined as urinary creatinine clearance more than 5 mL/min. 247 The observation suggests that better clearance of antibiotics might lead to lower concentration of antibiotics, and hence the reduced time above the minimum inhibitory concentration (MIC). Optimal dosing of antibiotics in patients with significant residual kidney function remains unknown, although fixed dosing irrespective of residual kidney function might not be the best solution for antibiotics (such as cephalosporin) that exhibit time-dependent killing effects. Limited data are available to guide the adjustment of antibiotics dosing, except a recent randomised controlled study advocating a 25% increase in the loading and maintenance dose of cefepime, cefazolin and ceftazidime when PD patients have residual urine volumes of more than 100 mL daily. 168
Vancomycin is the drug of choice in centres with a high prevalence of methicillin resistant gram-positive bacteria or for directed therapy in patients with relevant pathogens. IP administration is preferred because nearly 90% is absorbed in the presence of peritonitis. 248 The superiority of treatment success rate with IP versus intravenous vancomycin is supported by Cochrane systematic review. 160 Optimal dosing of IP vancomycin is unknown, and guideline recommendations are variable regarding whether to prefer fixed dosing or target-guided dosing according to serum trough level. Although fixed dosing of IP vancomycin had been reported in a randomised controlled trial, 234 it is unknown whether inter-individual variability of vancomycin bioavailability warrants adjustment of maintenance dose according to therapeutic drug monitoring of steady-state serum vancomycin concentration. A retrospective study reported that 60% of patients had subtherapeutic trough level following the loading dose after a fixed dosing of IP vancomycin 30 mg/kg every 5 days for CAPD and every 3 days for CCPD, irrespective of the residual renal function. However, all subsequent serum vancomycin levels were above 15 mg/L. 249 Several observational studies did not show correlation between trough levels and cure rates of peritonitis. 250,141 On the other hand, one observational study reported a higher rate of peritonitis relapse with intravenous vancomycin use when the cumulative 4-week mean trough vancomycin levels were less than 12 mg/L. 251 Another study of peritonitis due to methicillin-resistant coagulase-negative staphylococci showed that higher serum trough vancomycin levels achieved by IP vancomycin were associated with a lower relapse rate. 252 Regarding the practice of trough-guided vancomycin dosing, there was no consensus on the preferred timing of obtaining trough vancomycin concentration. Based on a retrospective analysis of 61 episodes of gram-positive or culture-negative peritonitis, serum vancomycin levels lower than 10.1 mg/L on day 5, but not the level on day 3, were associated with worse outcomes (including transfer to haemodialysis, death, persistent infection and relapse). 208 Recently, trough-guided vancomycin dosing has been increasingly replaced by the area under the 24-h time-concentration curve (AUC)-guided dosing to optimise the management of severe S. aureus infection. Although the clinical significance of AUC pharmacokinetic parameters for monitoring vancomycin dosing in peritonitis treatment is incompletely understood, accumulating evidence suggests that trough level might not be the best option. A recent study of anuric patients on APD reported that peak serum concentration level (30 min after IP administration), but not trough vancomycin level, was associated with cure of gram-positive peritonitis. 212
Aminoglycosides remain useful for treating gram-negative peritonitis. Since aminoglycosides exhibit concentration-dependent activity, their maximal bacterial killing occurs at high peak drug concentrations. In addition, aminoglycosides continue to suppress bacterial growth even after drug concentration falls below MIC of the bacteria, a characteristic known as the post-antibiotic effect. 253 As a result of the post-antibiotic effect and concentration-dependent bactericidal characteristics, we favour intermittent daily dosing of IP aminoglycosides to minimise toxicity and adaptive resistance while maintaining drug efficacy. This has been confirmed in a randomised controlled trial comparing once-daily gentamicin dose versus continuous dosing; treatment success and relapse rate did not differ between the two regimens. The once-daily dosing strategy, nevertheless, was associated with lower trough serum gentamicin level. 174 After the initiation of IP aminoglycosides, a significant fraction of the drug can be absorbed into the systemic circulation, especially when the peritoneal solute transfer rate is increased during the acutely inflamed phase. High mass active transfer coefficients for IP gentamicin and tobramycin were consistently reported in pharmacokinetic studies of patients with active peritonitis. 175,254 In a case series of 24 PD patients with peritonitis, 76% of the IP gentamicin dose was absorbed into the systemic circulation and was higher among those with high and high average membrane solute transfer rates. 175 Two studies in which outcomes were compared between patients with different gentamicin levels have not demonstrated any difference in gram-negative or culture-negative peritonitis cure rates. 141,255 A major concern with aminoglycoside use in PD patients is ototoxicity. At the currently recommended peritonitis treatment dosage of aminoglycosides, ototoxicity could occur in PD patients, resulting in either vestibular or cochlear damage. Such ototoxicity was reported even in the context of therapeutic serum concentrations. 256,257 Not unexpectedly, ototoxicity occurs with IP aminoglycosides, similar to systemic administration, as confirmed in both animal models 258 and human. 259,260 According to an observational study of PD patients, risk factors for hearing loss include older age, episodes of peritonitis and cumulative doses of amikacin and vancomycin. 166 The mechanism of aminoglycoside ototoxicity is incompletely understood. Besides genetic predisposition, reactive oxygen species damage to the inner ear is the most accepted hypothesis. Based on three randomised controlled trials of N-acetylcysteine, the preventive approach with antioxidant protection of aminoglycoside-induced ototoxicity appears promising. The largest study involved 60 CAPD patients who received IP vancomycin and amikacin. Compared with the control group, patients randomly assigned to oral N-acetylcysteine 600 mg twice daily had significantly better protection from ototoxicity as measured by pure tone audiometry assessment of high-frequency hearing function at the first and fourth weeks. 261 Similar findings were reported in two other randomised trials of N-acetylcysteine for PD patients receiving amikacin. 262,263 Only one of the three trials included a control group with a placebo; the other two were open-label. A protective benefit using the same dose strategy of oral N-acetylcysteine on high tone frequency ototoxicity had also been demonstrated in haemodialysis patients receiving intravenous gentamicin for dialysis catheter-related bloodstream infection. 264 None of these randomised controlled trials assessed vestibular function. The pooled relative risk for otoprotection at 4–6 weeks was 0.14 (95% CI 0.05 to 0.45) according to meta-analysis. 265 Notwithstanding the potential risks of bias of these trials with relatively small sample size, it is reasonable to consider co-administration of N-acetylcysteine at 600 mg twice daily for PD patients requiring aminoglycoside. In the absence of high-quality evidence to ameliorate potentially irreversible aminoglycoside ototoxicity, the best measure is to minimise prolonged or repeated administration. When an alternative drug of choice is available, early switch has been shown to have comparable clinical outcomes compared with continuing IP gentamicin. 141 In other words, avoiding prolonged aminoglycoside should be advocated to prevent aminoglycoside ototoxicity.
Fluoroquinolones, including ciprofloxacin 266 and moxifloxacin, 267 have been confirmed to be compatible with PD solutions and shown to be highly active and bactericidal in PD fluids with concentration-dependent activity. 268 A small randomised controlled study supported the safety and efficacy of IP vancomycin plus oral moxifloxaicin but was not powered to be a non-inferiority trial. 234 Oral administration is an alternative and more convenient choice for susceptible organisms, as both ciprofloxacin and moxifloxacin can achieve adequate levels within the peritoneum. 235,221 Oral ciprofloxacin should be administered in a once-daily dose of 500–750 mg instead of as a 250 mg twice daily dosing regimen, 220 although higher dosing at 750 mg every 12 h has been suggested in CCPD patients. 221 Patients should be instructed to avoid concomitant use of aluminium-containing antacids and oral phosphate binders (including calcium carbonate, lanthanum 269 and sevelamer 270 ) to avoid interference with absorption (and hence lower peak concentration) of fluoroquinolones. 271
Antibiotic delivery and stability
Stability and compatibility of antibiotics in PD solution (Table 7), as reviewed recently, 272 is one of the factors which influences treatment success.
Summary of IP antibiotics stability.
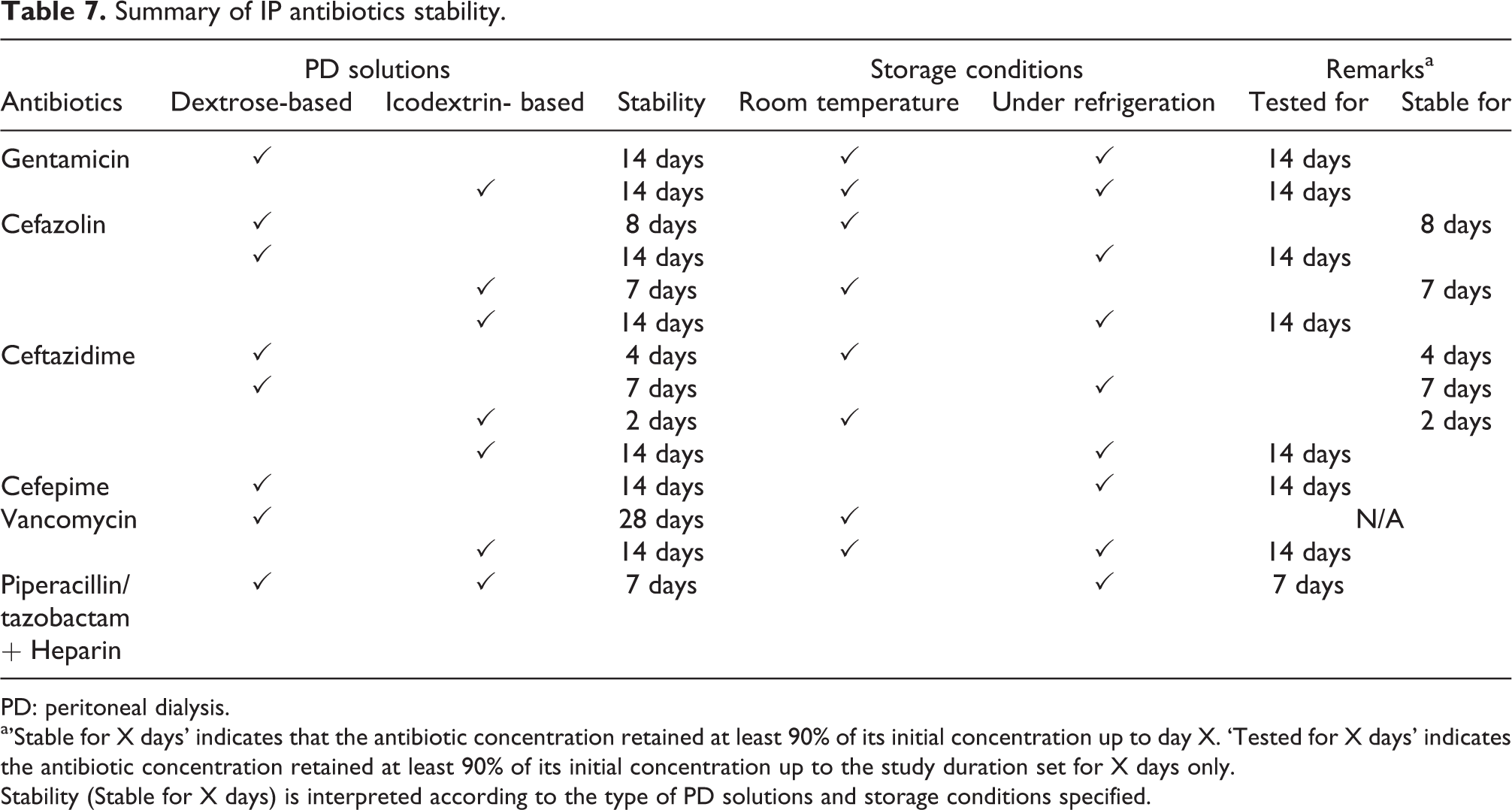
PD: peritoneal dialysis.
a’Stable for X days’ indicates that the antibiotic concentration retained at least 90% of its initial concentration up to day X. ‘Tested for X days’ indicates the antibiotic concentration retained at least 90% of its initial concentration up to the study duration set for X days only.
Stability (Stable for X days) is interpreted according to the type of PD solutions and storage conditions specified.
Gentamicin is stable for 14 days both at room temperature and under refrigeration in both dextrose-based and icodextrin-based PD solutions, but the duration of stability is reduced by admixture with heparin. 13,273,274
Cefazolin is stable for 8 days at room temperature or for 14 days if refrigerated in dextrose-based PD solutions; addition of heparin has no adverse effect. 13,275 In icodextrin-based PD solution, cefazolin is stable for 7 days at room temperature or for 14 days if refrigerated. 273 Ceftazidime is stable for 4 days at room temperature or 7 days if refrigerated in dextrose-based PD solutions. It is stable in icodextrin-based PD solution for 2 days at room temperature or 14 days at refrigerated temperature. 273 Cefepime is stable for 14 days in dextrose-based PD solutions when refrigerated. 13,276
Vancomycin is stable for 28 days in dextrose-based PD solutions at room temperature, but the duration of stability is reduced at higher ambient temperatures. 274 Stability of vancomycin in icodextrin-based PD solution has been confirmed for 14 days at 4°C and 25°C. 273
For compatibility of combined antibiotics in PD solutions, aminoglycosides and penicillins should not be added to the same bag due to chemical incompatibility. 275 There are several antibiotics which can be mixed in the same PD bag; gentamicin is compatible with cefazolin or vancomycin, and ceftazidime is compatible with cefazolin or vancomycin. 272,273,277
Emerging data of piperacillin/tazobactam showed that, when admixed with heparin in dextrose-based and icodextrin-based PD solutions, both drugs are stable for 7 days when refrigerated. 278
Data on the stability of newer antibiotics and PD solutions are important to prepare the readiness for clinical use. Potential candidates include ceftolozane-tazobactam for gram-negative bacilli producing ESBL and Pseudomonas aeruginosa; the drug’s stability in PD solution has been confirmed. 279
Special considerations for APD
Extrapolation of antibiotic dosing from CAPD to APD is not recommended. First, patients on APD may have greater peritoneal antibiotic clearance. The implication of shorter antibiotic half-lives during the cycler exchanges is inadequate serum and dialysate drug concentrations throughout 24 h.
An important concern for treating APD patients with peritonitis is the potential of underdosing, especially for antibiotics that exhibit time-dependent killing. Under such circumstances, it is important to use a dosing strategy that allows antibiotic concentrations to exceed the MIC for at least 50% of treatment time.
Sufficient dwell time should be allowed for drug absorption. Limited data are available to guide the optimal dwell time of antibiotics. A close correlation between vancomycin dwell time and bioavailability has been shown in pharmacokinetic study of APD patients. 213 Minimal dwell time of 4 h should be used for vancomycin to achieve adequate peritoneal concentration according to previous APD experience, 280 although dwelling for 6 h may be a more reasonable strategy. 212
While conversion to CAPD is not always feasible for pragmatic reasons, this may be considered for antibiotics requiring continuous dosing. When the conversion to CAPD is difficult to implement, the treatment dose of IP antibiotics administered to short dwells should ideally be validated. For short-dwell automated cycling exchanges, cefazolin and ceftazidime can still be used based on pharmacokinetic studies on patients with 281 and without peritonitis. 178
Adjunctive treatments
We suggest that augmented peritoneal lavage should not be performed for the purpose of improving peritonitis cure (2B).
We suggest that icodextrin be considered for volume overload which occurs during acute peritonitis (2C).
Many patients with PD-related peritonitis could be managed on an outpatient basis. According to a PDOPPS analysis of 1689 episodes of peritonitis internationally, only half of them had a hospitalisation within 14 days of peritonitis onset. 31 The decision to hospitalise a patient depends on many factors, including social support, hemodynamic status of the patient, severity of signs and symptoms and, for APD patients, the type of treatment schedule chosen as well as the ability to provide IP antibiotics as an outpatient and the reliability of the patient. The rationale for anti-fungal prophylaxis has been discussed in a previous section (see Secondary prevention section).
Patients with cloudy effluent may benefit from the addition of heparin 500 units/L IP to prevent occlusion of the catheter by fibrin. Depending on the severity of symptoms, some patients require analgesics for pain control. At the initial presentation and before IP antibiotics are initiated, one or two rapid PD exchanges are often performed for pain relief, although there are no data supporting this approach. Two randomised controlled trials showed that more extensive rapid-cycle peritoneal lavage, during the first 24 h of peritonitis 282 or from day 3 to 5, 283 did not improve the rate of complete cure or relapse.
IP urokinase has been advocated for the treatment of biofilm, which may be the cause of refractory or relapsing peritonitis. A retrospective study found that IP urokinase and oral rifampicin, in addition to conventional antibiotics, could facilitate catheter salvage among patients with persisting asymptomatic infection following coagulase-negative staphylococcus peritonitis. 284 However, three randomised controlled trials failed to show any benefit of IP urokinase for the treatment of refractory peritonitis. 285 –287 The rates of complete cure, catheter removal or relapsing episodes as well as overall mortality were not affected by adjunctive treatment with IP urokinase. In contrast, one randomised controlled study showed that simultaneous catheter removal and replacement was superior to IP urokinase in reducing relapsing peritonitis episodes. 288
Peritoneal permeability to water and solutes typically increases during peritonitis. Reduced ultrafiltration is commonly observed and may result in the complication of fluid overload. In addition to temporary use of hypertonic exchanges, management of fluid overload might require short dwell times, which can theoretically compromise local defence mechanisms (owing to decreased macrophage phagocytic capacity and immunoglobulin G concentration). 289 Temporary use of icodextrin solution during acute peritonitis has been shown to be a better therapeutic option in one randomised controlled study. 290 The primary cure rate of peritonitis was similar between the icodextrin and original glucose-based dialysis solution treatment groups in the study, 290 although PDOPPS reported that icodextrin use was associated with a higher cure rate. 96 Because of rapid glucose absorption, glycemic control may worsen in diabetic patients. Blood glucose monitoring with appropriate adjustments of insulin dosage may be needed. Protein loss during peritonitis is also increased. Screening for malnutrition should be undertaken in patients with prolonged peritoneal inflammation. There are currently no high-quality, randomised studies that have examined the effects of dietary interventions or nutrition supplements in patients with peritonitis.
Subsequent management of peritonitis
We recommend that antibiotic therapy be adjusted once results and sensitivities are known (1C).
The management algorithms for bacteria identified in dialysis effluent are summarised in Figures 2 to 4. Within 48 h of initiating therapy, most patients with PD-related peritonitis will show considerable clinical improvement. The effluent should be visually inspected regularly to determine if clearing is occurring. Catheter lumen and exit site, tunnel should be re-examined. If there is no improvement after 48 h, cell counts and repeat cultures should be performed. In addition, monitoring of WBC count in PD effluent may also predict treatment response. A retrospective study with a validation cohort showed that dialysis effluent WBC count ≥1090/µL on day 3 was an independent prognostic marker for treatment failure. 291 Another retrospective study further confirmed a prediction model incorporating a dialysis effluent WBC count >1000/µL on day 3–4 is associated with a substantially higher likelihood of treatment failure. 292
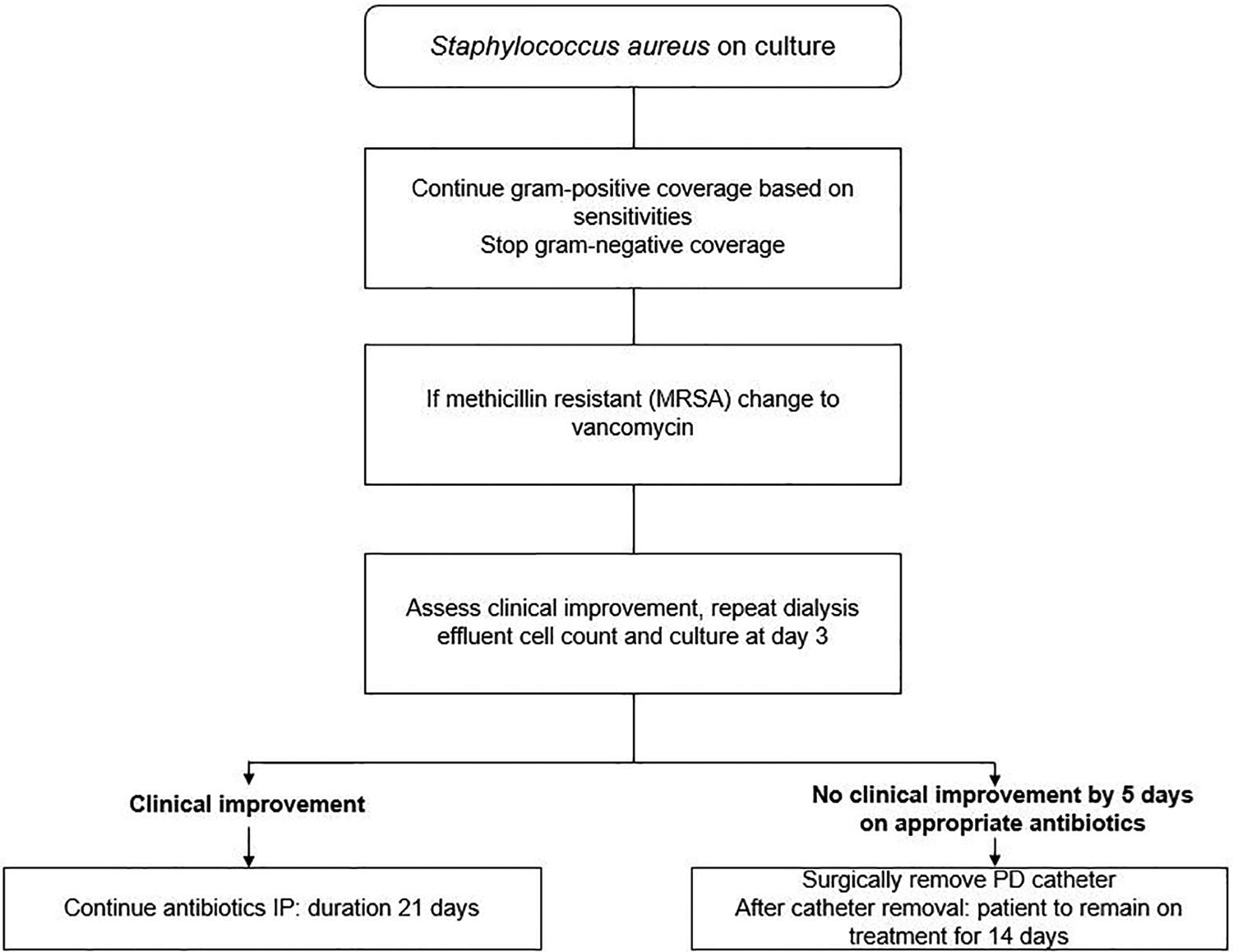
Management algorithm for Staphylococcus aureus peritonitis.
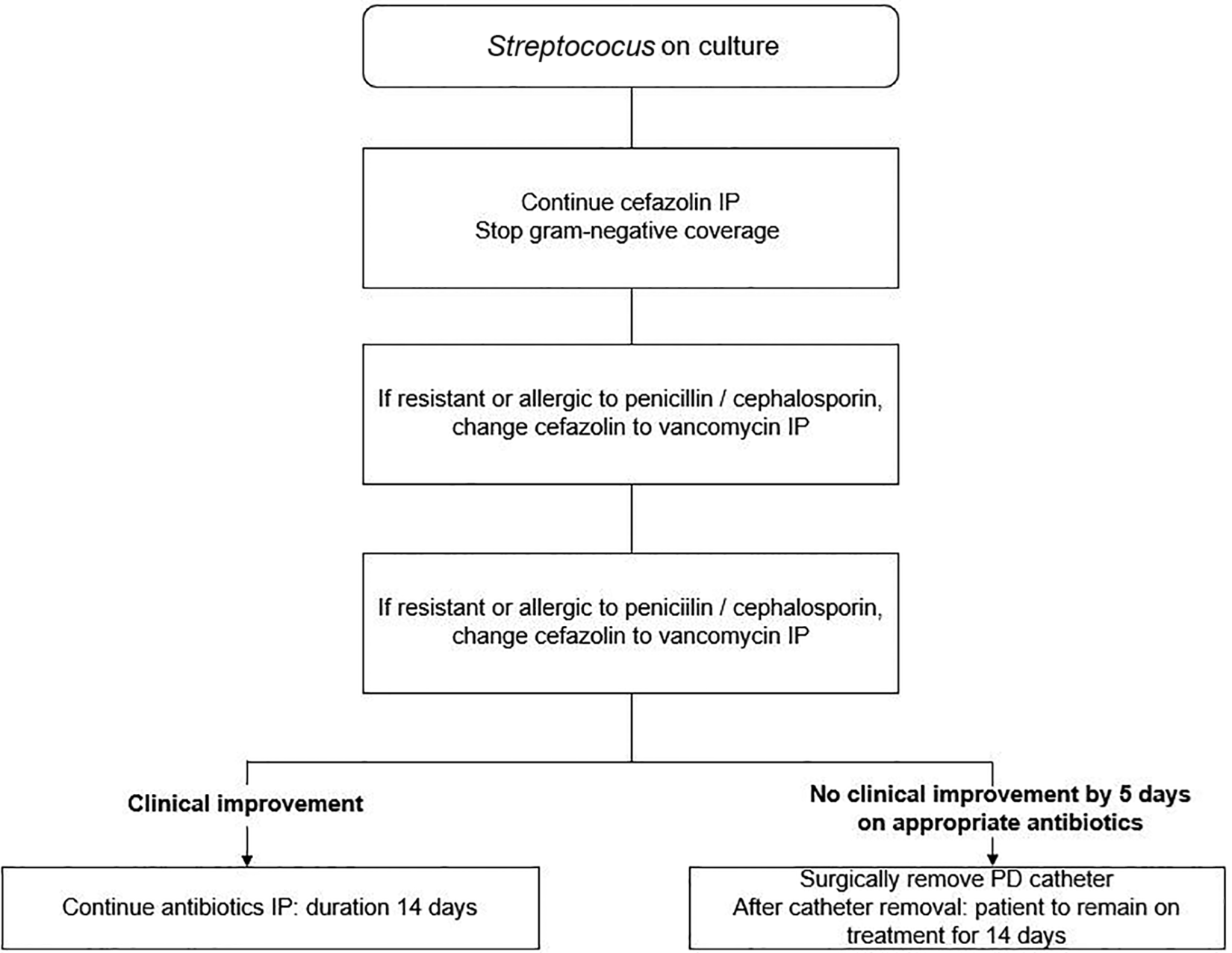
Management algorithm for Streptococci identified in dialysis effluent.
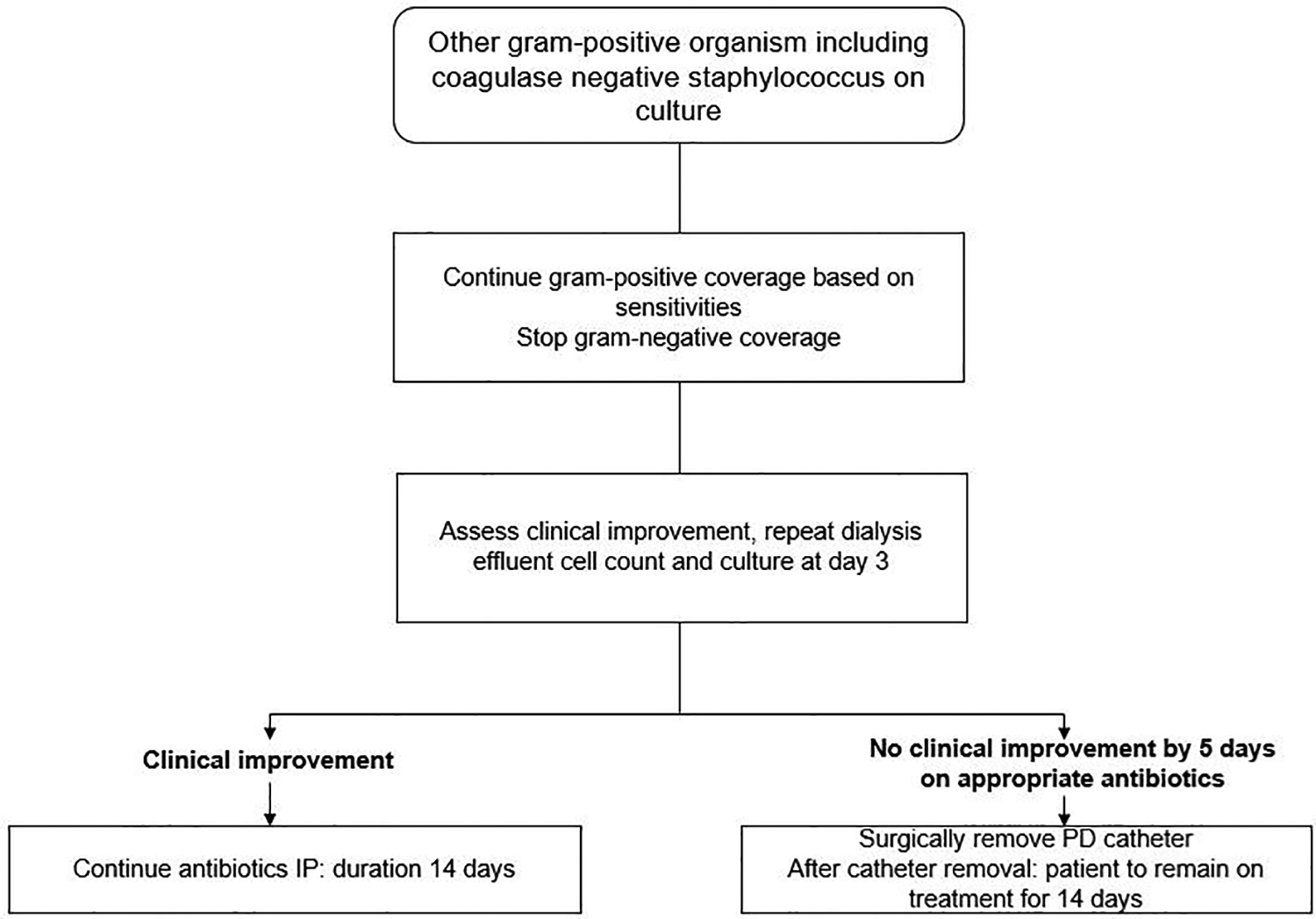
Management algorithm for other gram-positive organism including coagulase-negative Staphylococcus identified in dialysis effluent.
Nonfermenting gram-negative bacilli are important nosocomial pathogens contributing to serious peritonitis. Notably, P. aeruginosa, Acinetobacter baumannii and Stenotrophomonas maltophilia are known to have a high intrinsic resistance and deserve special attention in relation to the choice of antimicrobial agents (see below).
Refractory peritonitis
We recommend that PD catheter be removed in refractory peritonitis episodes, defined as failure of the PD effluent to clear after 5 days of appropriate antibiotics (1D).
We suggest that observation for antibiotic effect longer than 5 days is appropriate if PD effluent white cell count is decreasing towards normal, instead of mandatory PD catheter removal if effluent does not clear up by day 5 (2C).
After initiation of antibiotic treatment, there is usually clinical improvement in 72 h. Refractory peritonitis is defined as failure of the PD effluent to clear up after 5 days of appropriate antibiotics (Table 1). Catheter removal is indicated in cases of refractory peritonitis, or earlier if the patient’s clinical condition is deteriorating, in order to preserve the peritoneum for future PD as well as prevent morbidity and mortality. Prolonged attempts to treat refractory peritonitis by antibiotics without catheter removal are associated with extended hospital stay, peritoneal membrane damage, increased risk of fungal peritonitis and excessive mortality. 293,294
The cut-off of 5 days in deciding PD catheter removal should be considered an arbitrary reference tool. Data to compare long-term outcomes between 5-day decision rule and longer wait for antibiotic effect are lacking. In a single-centre study including 190 consecutive peritonitis episodes, substantial variation of PD effluent white cell count was reported. 295 The approach to less virulent organisms should probably be less aggressive to minimise premature or unnecessary PD catheter removal. Instead of a ‘one-size-fits-all’ rule on day 5, the trajectory of effluent white cell count should be taken into consideration. A large observational study of 644 peritonitis episodes tracked the longitudinal change of effluent white cell count. Three patterns of treatment outcome were analysed: early response, delayed response (defined by gradual decline in effluent white cell count but still above 100/µL on day 5) and treatment failure (defined as peritonitis not cured by antibiotics, change to haemodialysis either temporarily or permanently or peritonitis-associated death). 296 This study highlighted the varying rate or trajectory of effluent white cell count decline. In one-fifth of the cases, patients showed delayed response with 34% reduction of effluent white cell count by day 5, without the need for PD catheter removal. 296 Thus, expectant of peritonitis episodes with longer antibiotic treatment duration without immediate catheter removal can be an option if the effluent white cell count is decreasing, albeit not reaching the nadir 100/µL by day 5.
Relapsing, recurrent and repeat peritonitis
We recommend timely PD catheter removal be considered for relapsing, recurrent or repeat peritonitis episodes (1C).
We suggest that simultaneous PD catheter removal and reinsertion be considered after culture of the PD effluent has become negative and the PD effluent white cell count is below 100/µL, in the absence of concomitant exit site or tunnel infection (2C).
The definitions of relapsing, recurrent and repeat peritonitis are summarised in Table 1. Retrospective studies showed that relapsing, recurrent and repeat peritonitis episodes are caused by different species of bacteria and probably represent distinct clinical entities. 297 –301 When compared to non-relapsing episodes, relapsing ones are associated with a lower rate of cure, more ultrafiltration problems and higher rates of technique failure. 297 Recurrent peritonitis episodes had a worse prognosis than relapsing ones. 297,298 Centres with larger PD sizes are associated with lower rates of relapsing and recurrent peritonitis. 161
To manage or reduce the risk of relapsing, recurrent or repeat peritonitis, simultaneous removal and reinsertion of PD catheters have been proposed. 302 This allows a continuation of PD without transfer to HD. Such a strategy should be considered only after culture of PD effluent has been confirmed negative following appropriate treatment, with a PD effluent white cell count lower than 100/µL and in the absence of concomitant exit-site or tunnel infection. 27 Before the bacterial culture became negative, it would be inappropriate to attempt simultaneous removal and reinsertion of catheter because there could still be planktonic bacteria. To optimise the eradication success rate, we suggest deferring the procedure until the culture is negative, indicating absence of planktonic bacteria (when the bacteria are sequestered in biofilm). The simultaneous removal and reinsertion of catheter procedure should be carried out under perioperative antibiotic coverage. 27,303 The long-term benefit of simultaneous removal and reinsertion of PD catheters has been replicated in several series, with reported 1-year technique survival of 64% 304 and median technique survival of more than 5 years. 303
On the other hand, prolonged antibiotic treatment is not recommended. A randomised controlled study showed that extending antibiotic treatment duration for an additional week beyond that recommended by the ISPD is not advisable because such a strategy does not reduce the risk of relapsing, recurrent or repeat peritonitis and may increase the risk of repeat peritonitis. Another downside to prolonged antibiotic use is the risk of developing secondary fungal peritonitis. 305
A previous study suggested that bacterial DNA fragment levels in PD effluent are significantly higher 5 days before and on the date of completion of antibiotics amongst patients who subsequently develop relapsing or recurrent peritonitis. 306 Despite the prognostic value of bacterial DNA fragments, a subsequent study showed that bacterial DNA levels do not decrease significantly with extended antibiotic therapy. 305
Coagulase-negative Staphylococcus
We suggest that coagulase-negative staphylococci be treated with IP cephalosporin or vancomycin, according to susceptibility, for a period of 2 weeks (2C).
We suggest that retraining be considered for patients with coagulase-negative staphylococcal peritonitis (Not Graded).
The leading cause of pathogenic coagulase-negative staphylococci peritonitis is Staphylococcus epidermidis, followed by Staphylococcus haemolyticus. 307
Despite lower virulence properties than S. aureus, coagulase-negative staphylococci are more common, partly because host fibrinogen antimicrobial defences can eliminate the former but not coagulase-negative staphylococci. 308 Coagulase-negative staphylococcal peritonitis is also challenging due to the large proportion of methicillin-resistant strains and biofilm formation. The methicillin resistance rate of coagulase-negative Staphylococcus causing peritonitis has been increasing to more than 50% in most centres 309 –311 and up to 70%. 162,307 Such a high prevalence of methicillin resistance is now considered a rationale to use empirical vancomycin for coagulase-negative staphylococci peritonitis in some centres. As long as adequate antibiotic levels are achieved, a treatment duration of 2 weeks is generally sufficient (Figure 4). There was no difference in primary response rate or complete cure rate between episodes treated with 2 and 3 weeks of antibiotics. 312 However, there is a high risk of relapse when cephalosporin-resistant cases were not treated with vancomycin despite clinical improvement with cefazolin, 313 or when adequate vancomycin levels were not achieved. 252
They key to the success in managing coagulase-negative staphylococci is handling the root cause of infection. Patient’s exchange technique should be reviewed to prevent further touch contamination and peritonitis recurrence. Another concern in relation to tackling coagulase-negative staphylococci is the high risk of refractory and repeat peritonitis, often in the second month after the completion of antibiotic treatment. 314 Reported rates of repeat coagulase-negative staphylococci peritonitis were around 12% in two large case series. 307,312 These episodes are likely secondary to colonisation of the PD catheter with biofilm, in particular, with the presence of mecA gene (which encodes a low-affinity penicillin-binding protein) and biofilm-related gene icaAD. 307 Under these situations, catheter removal should be considered. When the PD effluent becomes clear with antibiotic therapy and culture became negative, many of these patients could have simultaneous re-insertion of a new catheter as a single procedure under antibiotic coverage. 315 This strategy obviates interruption of PD, and temporary haemodialysis could therefore be avoided. Other suggested options include adjunctive antibiotics and fibrinolytic therapy. 314 One series reported use of intraluminal urokinase 100,000 IU for 2 h and oral rifampicin 600 mg daily for 3 weeks; the success rate of catheter salvage was 64%. 284 Another smaller series suggested intraluminal alteplase 6 mg for 6 h, plus IP vancomycin, IP gentamicin, oral rifampicin 300 mg twice daily for 3 weeks; eradication of infection was achieved in all four cases of repeat coagulase-negative staphylococci peritonitis. 316
Staphylococcus aureus
We suggest that S. aureus peritonitis be treated with effective antibiotics for 3 weeks (2C).
Peritonitis episodes caused by S. aureus are often secondary to exit-site or tunnel infection, although touch contamination can be contributory. Figure 2 refers to the suggested treatment algorithm. If the bacterial isolate is methicillin-sensitive, a first-generation cephalosporin is the drug of choice. Two retrospective studies, with more than 700 cases in total, found that the initial empiric antibiotic choice between vancomycin and cefazolin had similar clinical outcomes. 317,318
If the isolate is methicillin-resistant, IP vancomycin is the drug of choice. Another study showed that the use of adjuvant rifampicin for 5 to 7 days was associated with a 50% relative risk reduction in relapse or repeat S. aureus peritonitis. 317
Observational data suggest that treatment with effective antibiotics for 3 weeks is needed. 317,318 If the response to vancomycin is unfavorable, IP daptomycin with or without oral rifampicin can be used as salvage therapy. 197 For patients with concomitant S. aureus exit-site or catheter tunnel infection, however, catheter removal should be considered.
Teicoplanin is not preferred because its activity on MRSA biofilm is impaired in PD solutions. 319
Streptococcal peritonitis
We suggest that streptococcal peritonitis be treated with appropriate antibiotics for 2 weeks (2C).
The reported cure rate of streptococcal peritonitis exceeds 85%, and most patients can continue PD. 320,321
An increasing trend of streptococcal peritonitis has been observed in longitudinal studies, 321,322 mostly secondary to viridans groups (including oralis, sanguis and gordonii). For viridans group streptococci, there is emerging evidence of mixed or polymicrobial strains with lower susceptibility to ampicillin, penicillin and ceftriaxone being encountered. 162,322
Peritonitis episodes caused by streptococci usually respond well to antibiotic treatment (Figure 3), but viridans streptococcal peritonitis poses a higher risk of relapse. 323
Corynebacterium peritonitis
We suggest that Corynebacterium peritonitis be treated with effective antibiotics for 2 weeks (2D).
We suggest that peritonitis due to beta-lactam-resistant strains, such as Corynebacterium jeikeium, should be treated with vancomycin (2C).
Corynebacterium species are gram-positive bacilli and belong to the natural flora of the skin. Infections due to Corynebacterium have been increasingly recognised over the past decades, largely due to improved recognition and microbiological techniques. Three outcome studies of Corynebacterium peritonitis came to somewhat differing conclusions as to whether antibiotics should be extended beyond 2 weeks. The cure rate for Corynebacterium peritonitis, according to the largest study of 162 episodes, did not differ between cases with initial treatment with vancomycin and cefazolin. 324 Catheter removal rate was 15%, and treatment duration beyond 14 days did not confer additional benefit. 324 Another retrospective study supported a treatment duration of 2 weeks, but advocated for early instead of delayed catheter removal if the patient did not show clinical improvement. 325 Otherwise, there was a high chance of permanent haemodialysis transfer if the catheter was removed more than one week after the onset of peritonitis. For patients who had initial clinical response, another study reported that nearly half developed repeat Corynebacterium peritonitis after stopping antibiotics; such repeat episodes were usually able to be managed with a 3-week course of IP vancomycin. 326
The controversy regarding antibiotics treatment duration could have been related to different isolates of corynebacteria and antibiotic susceptibility; species determination within the genus Corynebacterium was not available in the previously published series. 324 –326 In particular, we believe treatment should be vancomycin for species characterised by increasing antimicrobial resistance to beta-lactams, such as Corynebacterium jeikeium and Corynebacterium striatum. 327 –329 For patients with concomitant exit-site or catheter tunnel infection caused by Corynebacterium, early catheter removal should be considered.
Enterococcus peritonitis
We suggest that enterococcal peritonitis be treated for 3 weeks with oral amoxicillin (for ampicillin-susceptible enterococci) or IP vancomycin (2C).
For peritonitis due to vancomycin-resistant Enterococcus (VRE) which are ampicillin-resistant, we suggest treatment with oral or intravenous linezolid or IP daptomycin, or teicoplanin if susceptibility is confirmed (2D).
Enterococci causing intra-abdominal infections are often enteric in origin, 330 and sometimes enter the slime layer of intra-abdominal portion of PD catheter forming biofilm. 331,332 Enterococci coexisting with other organisms can cause polymicrobial infection episodes, which have much worse outcomes than single-organism Enterococcus peritonitis episodes. Single-organism enterococcal peritonitis and polymicrobial enterococcal peritonitis appear to behave as two disease entities with different clinical courses and severities according to three large cohorts. 330,186,219 Polymicrobial enterococcal peritonitis has been reported to consistently cause longer hospitalisation, lower primary response rates and higher catheter removal rates. Notably, there is a threefold 330 to fourfold 219 higher mortality rate for polymicrobial than for single-organism enterococcal peritonitis.
In addition to distinguishing between single-organism and polymicrobial enterococcal peritonitis, proper selection of antibiotics is needed (Figure 5). Specifically, cephalosporin should not be used to treat enterococcal peritonitis because of intrinsic resistance. Oral amoxicillin treatment for 2–3 weeks has been shown to have primary response and complete cure rates of 76% and 56%, respectively, for enterococcal peritonitis. 219 This convenient treatment option, with comparable response to IP vancomycin for Enterococcus faecalis, should be considered if the local prevalence of ampicillin resistance is not high. Because vancomycin exposure is a known risk factor for VRE colonisation among PD patients, 333,334 there now exists a strong rationale for using oral amoxicillin for ampicillin-susceptible enterococci isolates to minimise the risk of provoking vancomycin-resistant strains. Oral amoxicillin is less preferred in polymicrobial enterococcal peritonitis and not recommended for Enterococcus faecium. 219 IP vancomycin is reserved for peritonitis due to ampicillin-resistant enterococci with susceptibility to vancomycin.
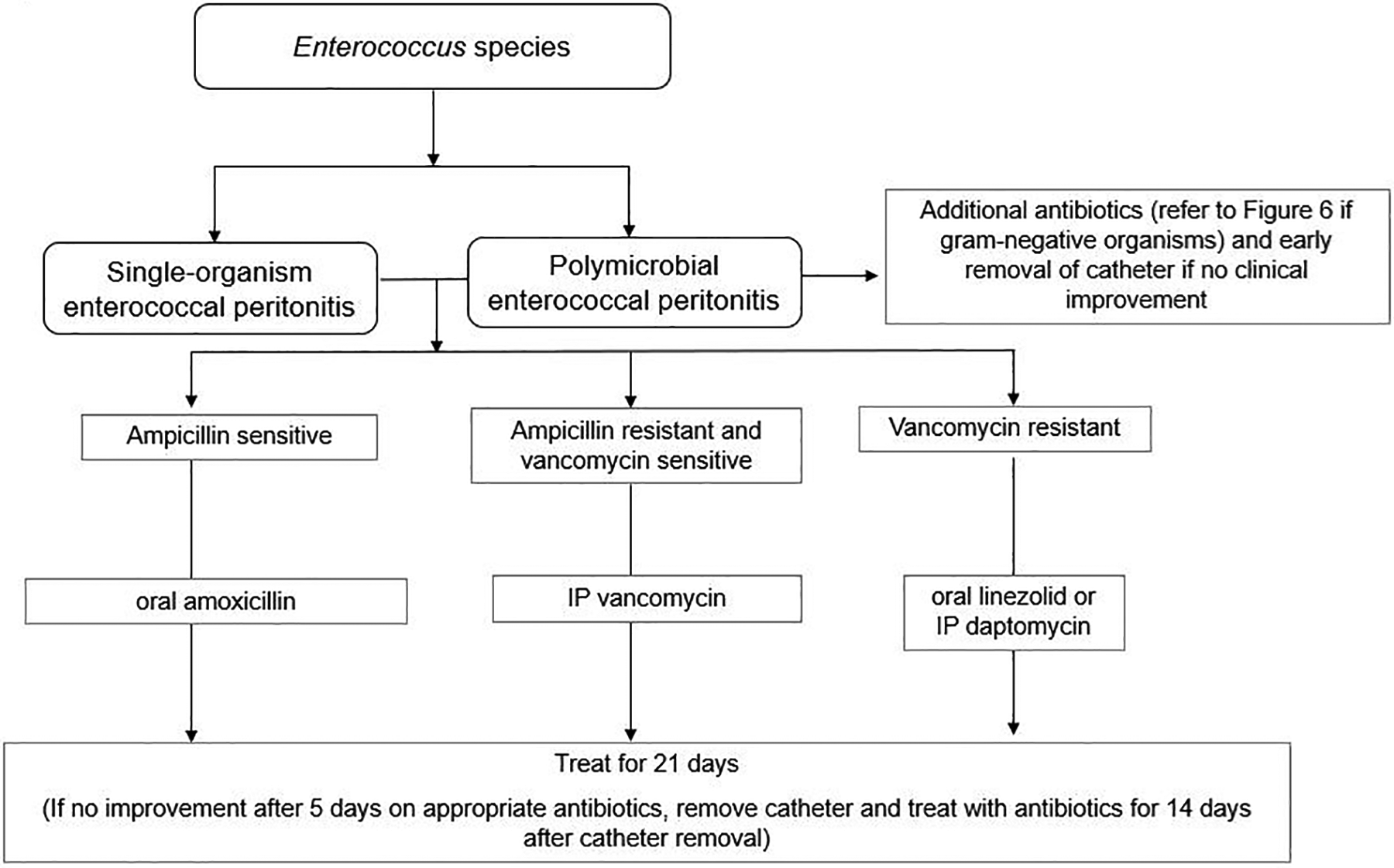
Management algorithm for enterococcal peritonitis.
For VRE causing peritonitis, infectious disease specialists or microbiologists should be consulted for advice. Aminoglycosides are not suggested because enterococci are relatively impermeable to aminoglycosides; very high concentrations of aminoglycosides would have been required to achieve bactericidal activity. Oral or intravenous linezolid 231,232,335 and IP daptomycin 198,336 have been used with variable success. Before the availability of these new treatment options, the mortality of VRE peritonitis was more than 50% when chloramphenicol was used. 337 Among previously suggested treatment options, quinupristin/dalfopristin 205 is less preferred because the peritoneal concentration achieved by intravenous dosing might not be adequate to exceed the MIC of VRE 338 ; moreover, its prior approval of VRE infection treatment by US FDA has been removed. The efficacy of quinupristin/dalfopristin against E. faecalis is even lower. Daptomycin, on the other hand, has established stability in PD solutions (including dextrose, amino acid-based fluids and icodextrin) 218 and effective peritoneal concentrations have been achieved by IP administration. 196
With the emergence of VRE isolates showing resistance to currently available drugs, newer agents, including dalbavancin 227 and combination treatment strategies (including tigecycline, fosfomycin), are potential options.
Notably, the IP route administration for ampicillin and linezolid is not recommended because there is a dramatic reduction of their bacteriostatic effects on E. facaelis by the peritoneal fluid. 218 IP use of dalbavancin is also not recommended because of the concern about chemical peritonitis. 227
Pseudomonas peritonitis
We suggest that Pseudomonas peritonitis be treated with 2 antibiotics with different mechanisms of action and to which the organism is sensitive for 3 weeks (2C).
We suggest that Pseudomonas peritonitis with concomitant exit-site and tunnel infection be treated with catheter removal (2D).
If there is no clinical response after 5 days of effective antibiotic treatment, we suggest that Pseudomonas peritonitis be treated with early catheter removal instead of using three antibiotics as an attempt to salvage (2D).
Pseudomonas peritonitis is often severe and associated with less than 50% complete cure rate. 339,340 Pseudomonas aeruginosa accounts for the majority of the species, followed by Pseudomonas stutzeri. 294,339 Retrospective studies show that PD can be resumed in less than 40% of cases requiring catheter removal, 294,339 but the chance of returning to PD was nominally higher for those with early catheter removal than deferred removal. 294,339 Furthermore, catheter removal was associated with a lower risk of death after Pseudomonas peritonitis. 339
Although the antibiotic resistance rate of Pseudomonas species causing peritonitis has been stable over the years, 294,339 the unfavourable response of Pseudomonas peritonitis with high chances of hospitalisation and catheter removal suggest other virulence factors such as biofilm production. Among different non-fermenting gram-negative bacilli (Figure 6), Pseudomonas species are associated with the highest rate of biofilm production, 173 partly accounting for the high treatment failure rate to antibiotics even when the in vitro susceptibility of planktonic cells to antibiotics suggests otherwise.
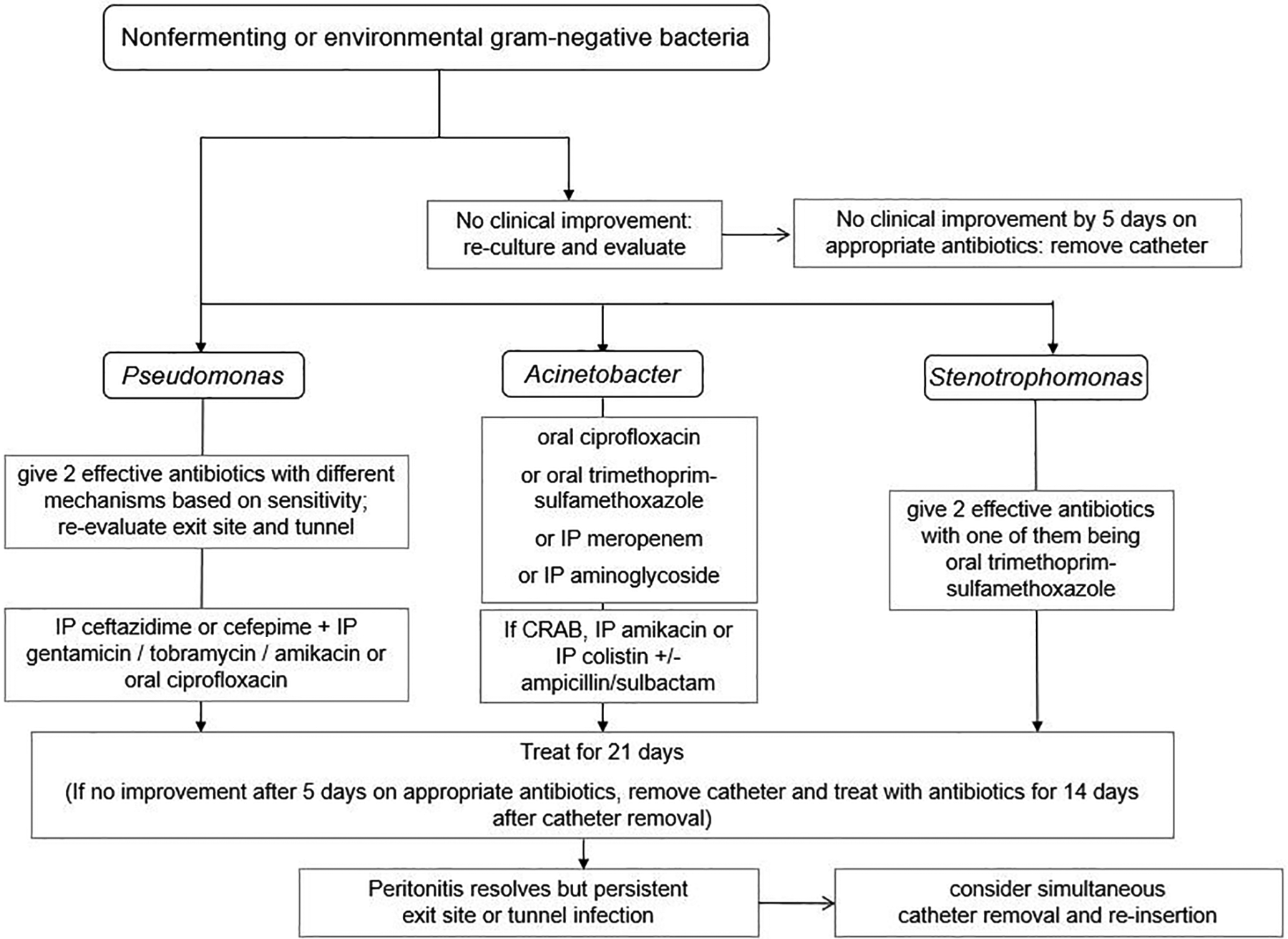
Management algorithm for non-fermenting or environmental gram-negative bacteria including Pseudomonas, Acinetobacter and Stenotrophomonas identified in dialysis effluent. CRAB: Carbapenem-resistant Acinetobacter baumannii
Retrospective case series showed that the use of two anti-pseudomonal antibiotics is associated with better outcomes, 339 but the use of three anti-pseudomonal antibiotics does not further improve complete cure or relapse rate. 294 Instead of using three antibiotics, catheter removal is often needed to minimise prolonged peritoneal inflammation or repeat peritonitis episodes. Another observed untoward effect of protracted antibiotic treatment of Pseudomonas peritonitis is a significant decline in residual kidney function. 294
Acinetobacter peritonitis
We suggest that carbepenem-resistant Acinetobacter peritonitis be treated with aminoglycoside and a sulbactam-containing agent (2C).
Outcomes of Acinetobacter peritonitis are considered more favourable than those of Pseudomonas peritonitis. 341 Empirical antibiotic therapy for Acinetobacter should be selected based on local susceptibility patterns (Figure 6) and should consist of a broad spectrum cephalosporin, a combination beta-lactam/beta-lactamase inhibitor (combination including sulbactam) or a carbapenem (except ertapenem). Although carbapenems and aminoglycosides are the potential treatment of choice of Acinetobacter baumannii, these organisms are increasingly reported to possess aminoglycoside-modifying enzymes and carbapenemases. Epidemiologic studies in Asia and South American countries have demonstrated an increasing prevalence of multidrug resistant and carbapenem-resistant Acinetobacter peritonitis. 173, 342
Stenotrophomonas maltophilia peritonitis
We suggest that Stenotrophomonas maltophilia peritonitis be treated with trimethoprim–sulfamethoxazole (2D).
We suggest that S. maltophilia peritonitis be treated with two different classes of antibiotics for at least 3 weeks (2D).
Clinical efficacy data for the use of antibiotics in the setting of S. (Xanthomonas) maltophilia peritonitis are limited 343 –345 ; the approach is extrapolated from data for other infection (Figure 6). 150 The recommended first-line agent is trimethoprim–sulfamethoxazole at the higher end of the dosing range to achieve bactericidal effect. 150,344,346 However high-dose trimethoprim-sulfamethoxazole is generally not recommended 347 or utilised 348 in patients with renal failure. Therefore standard-dose trimethoprim-sulfamethoxazole in combination with fluoroquinolones 349 (levofloxacin or moxifloxacin), intravenous ticarcillin/clavulanic acid, minocycline or tigecycline and ceftazidime is suggested. 346 These can be used as alternatives if trimethoprim–sulfamethoxazole is contraindicated or not tolerated. Most case reports of successful treatment of S. maltophilia peritonitis are combination antibacterial therapy. 344,345 Based on these limited observational data, we suggest therapy with two antibiotics for at least 3 weeks.
Enteric gram-negative bacteria peritonitis
We suggest that enteric gram-negative peritonitis be treated with effective antibiotics for at least 3 weeks (2C).
Besides non-fermenting gram-negative bacilli with high resistance to antibiotics, several Enterobacterales species, such as E. coli, are reported to have increasing resistance and treatment failure rates. 350 The Enterobacterales order comprises several bacteria genera, including E. coli, Klebsiella and Enterobacter species. E. coli, the commonest member, 162,346 accounts for one-third of single-organism non-Pseudomonas gram-negative peritonitis in Australia. 351
Treatment algorithms of enteric gram-negative peritonitis depend on the resistance pattern (Figure 7).
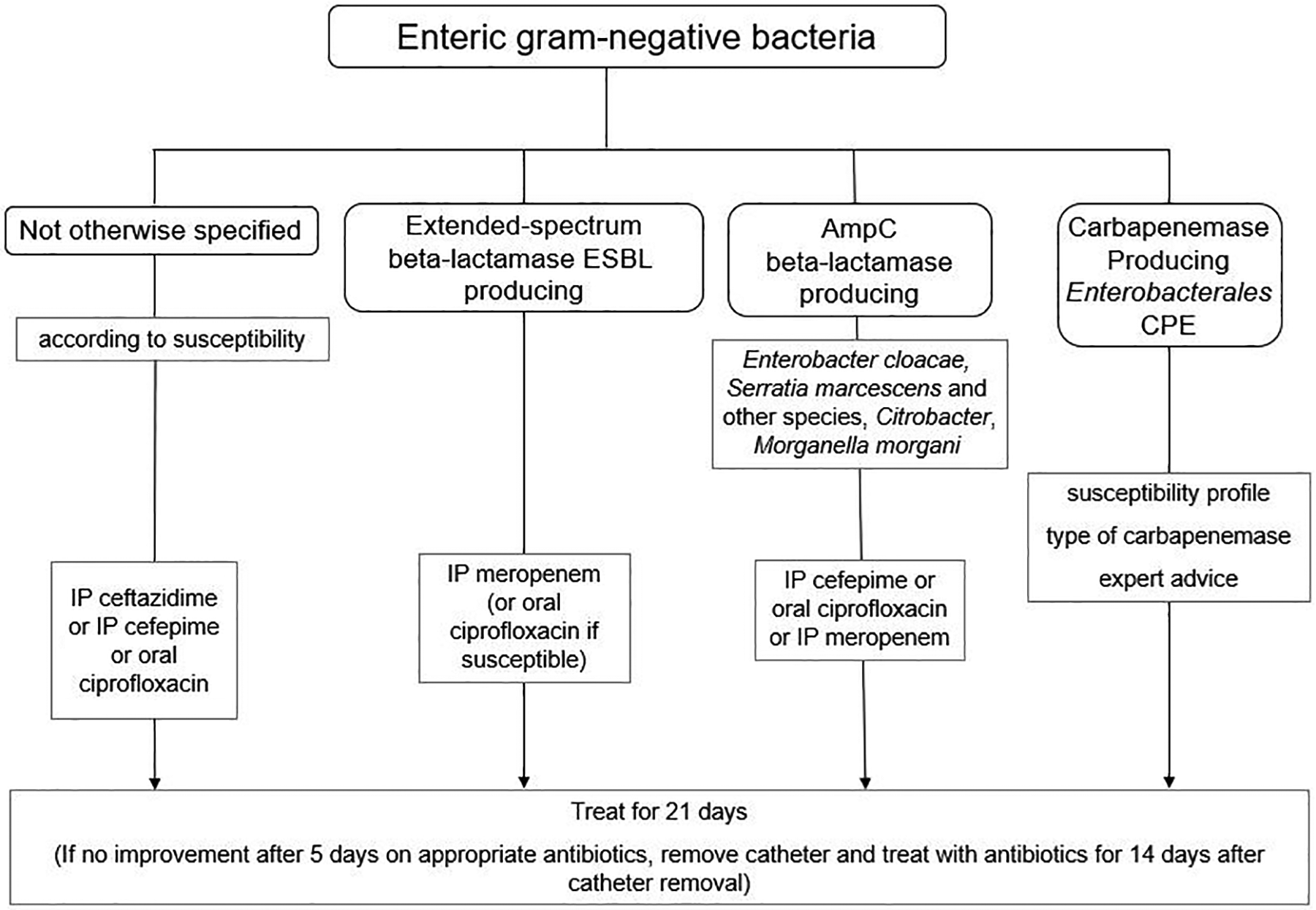
Management algorithm for enteric gram-negative bacteria identified in dialysis effluent.
Extended-spectrum beta-lactamases are a heterogeneous family of primarily plasmid-mediated enzymes that inactivate beta-lactam antibiotics. ESBL producers are associated with worse clinical outcomes. Many ESBL producing strains are also resistant to fluoroquinolones and aminoglycosides. 352 The ESBL-producing E. coli strains causing peritonitis has increased to 47% in China, 350 whereas resolution of E. coli peritonitis occurred in less than half of cases in Brazil. 353 The treatment failure rate of E. coli peritonitis correlates with resistance to second- and third-generation cephalosporins and fluoroquinolones. 354 For such susceptibility patterns, there should be a low threshold for PD catheter removal.
Chromosomally encoded ampicillin hydrolysing (AmpC) enzymes are variably induced on exposure to beta-lactam antibiotics such as cephalosporins. ‘SPICE’ organisms (namely, Serratia, Providencia, indole-positive Proteus, Citrobacter freundii and Enterobacter species) are the primary producers of AmpC enzymes, although they are also found in other Enterobacterales organisms. 355 Because the production of AmpC can lead to clinical failure with cephalosporins, peritonitis caused by such bacteria (Figure 7) should be assumed to be resistant to early-generation cephalosporins even with in vitro susceptibility. 356 Fourth-generation cephalosporin (cefepime), quinolones or carbapenem should be considered.
In case of peritonitis caused by carbapenemase-producing Enterobacterales (Figure 7), early consultation with microbiology or infectious disease experts is recommended, as optimal microbiological therapy will be determined by the specific carbapenemase genes detected. 357
Peritonitis from bacteria not otherwise specified
Treatment duration for peritonitis from unusual organisms should preferably be guided by published literature and microbiologists. An example is peritonitis secondary to Gordonia, which should be treated by combination of carbapenem and aminoglycosides for at least 3 weeks. 358,359
Peritonitis secondary to Pasteurella multocida, a gram-negative coccobacillus mostly related to domestic cats and sometimes dogs, can be treated with cefazolin, ceftazidime or oral amoxicillin–clavulanic acid for 14 days. 360
Polymicrobial peritonitis
When multiple enteric organisms are grown from the PD effluent, there is a possibility of intra-abdominal pathology (Figure 8). Presentation with hypotension, sepsis, lactic acidosis or elevated dialysis effluent amylase level usually represents an abdominal catastrophe. 361 When a surgical cause of peritonitis is suspected, the antibiotics of choice are metronidazole plus vancomycin, in combination with ceftazidime or an aminoglycoside. Monotherapy with a carbapenem or piperacillin/tazobactam may also be considered. Assessment by a surgeon is needed. Computed tomographic (CT) scan may help to identify the pathology, especially in the presence of haemodynamic instability. A study in which abdominal imaging (mostly CT scan) was performed in 68 cases of peritonitis, abnormalities were detected in nearly half of them, including bowel obstruction, intra-abdominal collection and biliary abnormalities. The peritonitis organism did not help predict imaging abnormalities, whereas ICU admission was highly predictive of imaging abnormalities. 362 If laparotomy is needed, the PD catheter is usually removed and antibiotics are continued intravenously.
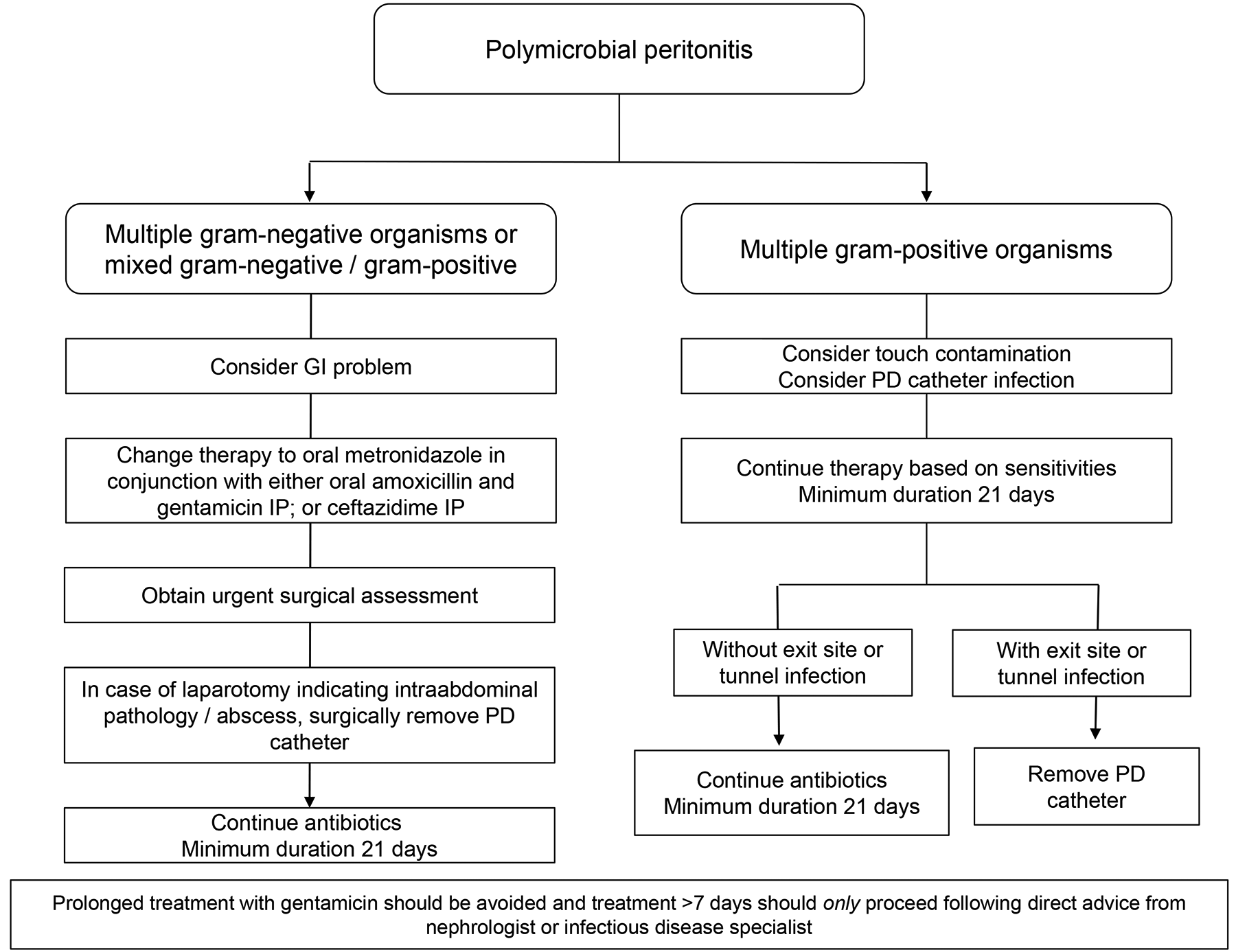
Management algorithm for polymicrobial peritonitis.
In contrast, polymicrobial peritonitis due to multiple gram-positive organisms often has a favourable prognosis. In a case series of 39 consecutive polymicrobial peritonitis episodes secondary to only gram-positive organisms, about 90% showed a primary response, and more than half had a complete cure. 23,363 Similar conclusions were reached in another report of polymicrobial peritonitis in which pure gram-positive peritonitis had the best clinical outcomes. 23 In general, their clinical behaviour is similar to peritonitis episodes caused by single gram-positive organisms, and the aetiology may well be touch contamination. Conservative management with antibiotic therapy is often effective without catheter removal. 363 In other words, the higher hospitalisation rate, surgical intervention requirement and mortality of polymicrobial peritonitis appear to be limited to those episodes with isolation of enteric bacteria, fungus and/or E. faecium. 364
Fungal peritonitis
We recommend immediate catheter removal when fungi are identified in PD effluent (1C).
We suggest that treatment with an appropriate anti-fungal agent be continued for at least 2 weeks after catheter removal (2C).
Treatment failure and mortality rates of fungal peritonitis remain high, despite a slightly improved outcome with early catheter removal based on observational studies. 365,366
Because identification of the fungi can take time, diagnosis of fungal peritonitis can be supported by the Gram stain. Prompt empirical treatment with antifungal therapy should be initiated even based on the Gram stain. The subsequent choice of antifungal regimen depends on the correct identification of the pathogens and their susceptibility profiles. Candida albicans and Candida parapsilosis are the most common pathogens, although the frequency of the latter is reported to exceed that of C. albicans species. 111 The antifungal treatment of choice for C. albicans is usually fluconazole, whereas other Candida organisms sometimes require an echinocandin (caspofungin, micafungin or anidulafungin) or voriconazole. 367,215 The route of echinocandins administration should be intravenous 243 because of the concern that PD fluid significantly impairs the activity of echinocandins against Candida species biofilm. 368 Voriconazole administration is preferably oral, because of the concern with accumulation of the intravenous vehicle cyclodextrin in dialysis patients. Furthermore, oral voriconazole has been shown to quickly achieve good peritoneal concentration with minimal peritoneal clearance. 369
Aspergillus peritonitis treatment requires intravenous amphotericin B or new azole derivatives such as voriconazole, posaconazole or isavuconazole. 370 Drug-drug interactions during therapy with these new azoles require careful review of patient’s concurrent medication use. Figure 9 is a proposed algorithms for choosing antifungal treatment.
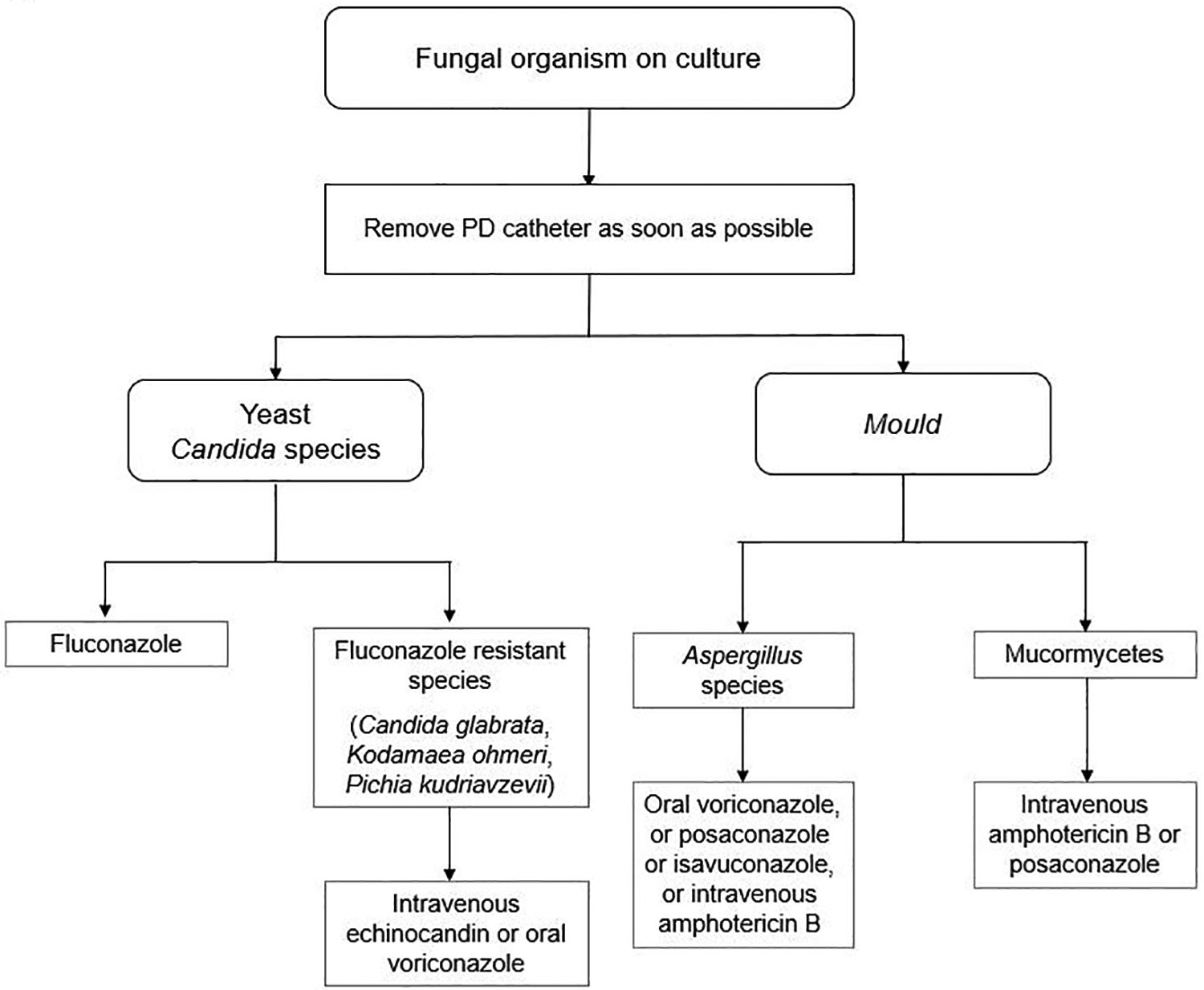
Management algorithm for fungal peritonitis.
Despite the availability of newer antifungal drugs, catheter removal remains the cornerstone of managing fungal peritonitis. Previous studies have reported a mortality of 50% 110 to 91% 109 among patients without catheter removal; the fatality rate is about two to three times that of those who are treated with catheter removal. Furthermore, early catheter removal should be encouraged as this has been reported to be associated with lower mortality and a better chance of resuming PD. 110,366 The benefit of early versus late catheter removal, on the other hand, was not confirmed in another study in Australia, where late removal was defined as more than 5 days after diagnosis of fungal peritonitis. 371 In view of the high biofilm production observed in fungal peritonitis, 367 we recommend immediate catheter removal as the best option to reduce the high mortality of fungal peritonitis.
Although there are insufficient data regarding the antifungal treatment duration, it should be continued for at least 2 weeks after catheter removal, and sometimes up to 4 weeks. 109 Irrespective of the treatment duration, catheter reinsertion and resumption of PD have been reported after a median period of 15 weeks in less than one-third of cases. 365
Culture-negative peritonitis
Reported risk factors for culture-negative peritonitis include recent antibiotic usage and improper culture technique. 37,38,372
Data regarding the treatment outcomes of culture-negative peritonitis based on large case series were in general favourable. Many culture-negative peritonitis episodes resolved with medical therapy; the cure rate by antibiotics alone ranged from 67.5% to 82.3%. 37,373,374 For culture-negative peritonitis episodes which improve promptly with antibiotics, they are probably caused by gram-positive organisms and initial therapy should be continued (Figure 10). Duration of therapy should be limited to 2 weeks because treatment outcomes were similar between episodes with treatment durations of 2 weeks and 3 weeks. 373
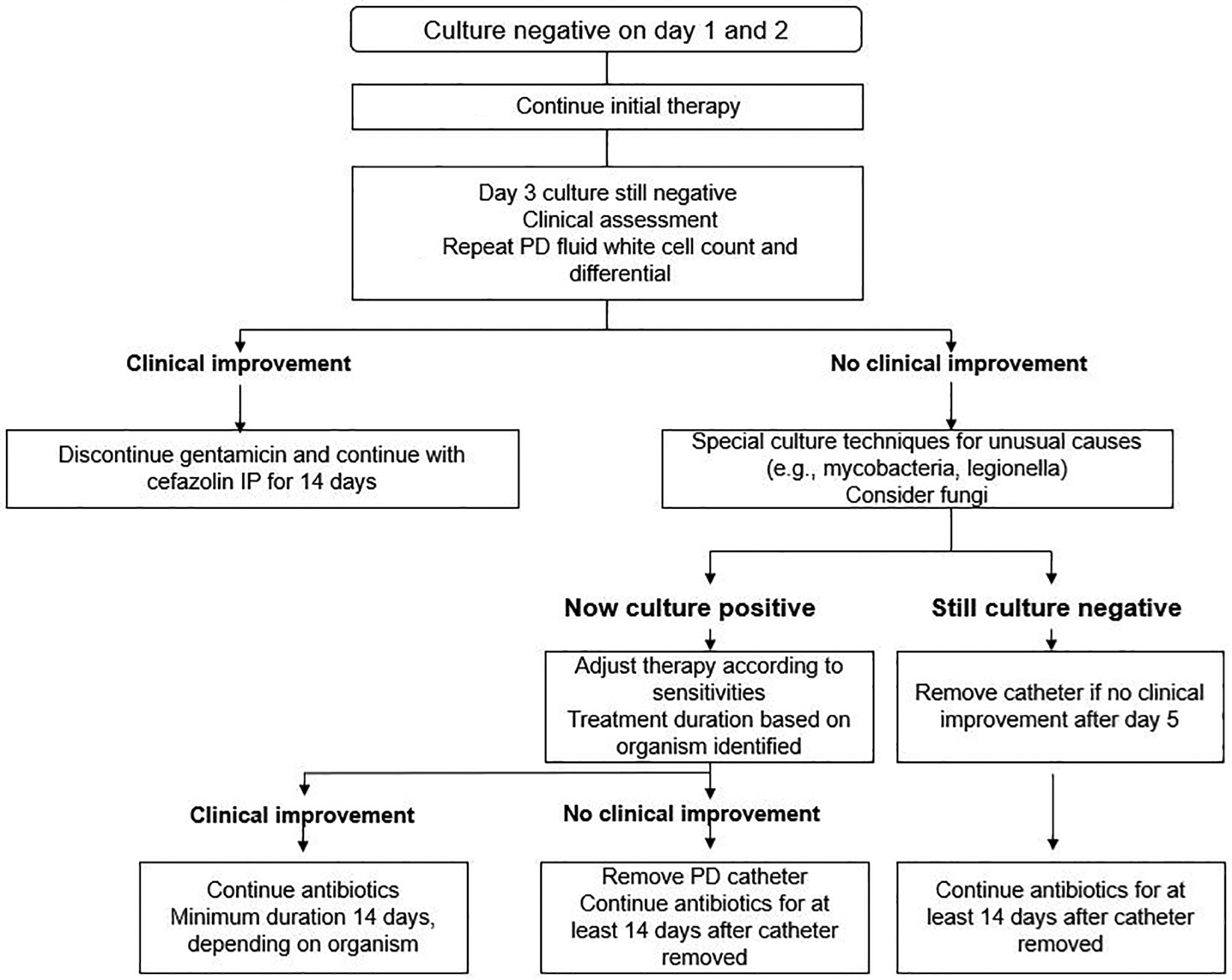
Management algorithm for culture-negative peritonitis.
On the other hand, for patients whose PD effluent yields no growth after 3 days, a repeat WBC count with differential should be obtained, together with special culture request to exclude unusual organisms such as mycobacteria, nocardia, filamentous fungus and other fastidious bacteria. The results of recent or concurrent exit-site cultures might not provide adequate information to adjust the antibiotic based on published study correlating the organisms between exit-site infection and subsequent peritonitis. 19 Although there was a six-fold higher hazard of peritonitis (around 20% being culture negative) within 30 days of exit-site infection, the respective causative organisms were often different. 19 Reported regimens for culture-negative peritonitis with suboptimal initial responses include a combination of ampicillin–sulbactam and amikacin, which demonstrated a response in 80% of 10 cases. 187
PD catheter removal was required in around 10% of cases of culture-negative peritonitis. 37,373
Tuberculous peritonitis
We suggest antituberculous therapy, instead of PD catheter removal, as the primary treatment of peritonitis caused by Mycobacterium tuberculosis (2C).
The presenting symptoms of tuberculous peritonitis are abdominal pain in 89% and fever in 81% of PD patients. 375 Tuberculous peritonitis could mimic bacterial peritonitis, leading to delay in appropriate treatment. Difficulty in recognising the diagnosis is the common presentation with polymorphonuclear cell predominant pleocytosis of dialysate during the initial phase of the disease, as reported in 65 to 78% of published cases. 375 –377 Since requests for cultures for acid-fast bacilli are often delayed and the times for the cultures (current gold standard for diagnosis) to become positive are lengthy, the mean time from presentation to initiation of treatment of tuberculous peritonitis was 6.7 weeks in a review of 52 PD patients. 378 Measurement of adenosine deaminase in the peritoneal dialysate is a screening test but its specificity is not sufficiently high enough. Another reliable and more rapid adjunctive tool is PCR analysis to detect M. tuberculosis DNA, 377,379 although its sensitivity is insufficient to exclude tuberculosis.
The recommended dosages of drugs for treating tuberculous peritonitis in PD patients are depicted in Table 8. In general, initial drug treatment of pan-susceptible tuberculosis consists of four drugs for a total of 2 months followed by two drugs (isoniazid and rifampicin) given for at least a total of 12 months. There is a paucity of scientific evidence regarding the optimal drug dosage of tuberculous peritonitis treatment, but preliminary pharmacokinetics data show no need for dose adjustment of isoniazid and pyrazinamide in PD patients whose peritoneal fluid drug concentrations were maintained above the MICs for M. tuberculosis. 380 However, oral rifampicin might not be able to achieve satisfactory peritoneal fluid concentration. 380 Furthermore, PD patients started on oral rifampicin should be monitored for blood pressure control because of its potent inducer activity of hepatic cytochrome p450 leading to reduced levels of most antihypertensive agents (including amlodipine and metoprolol). 180 With the need for prolonged treatment, PD patients should be monitored for side effects such as retrobulbar neuritis related to ethambutol and isoniazid-induced neuropathy characterised by paresthesia and burning symptoms of extremities. 381 Ethambutol should be omitted or suspended if or when M. tuberculosis is known to be fully susceptible to other agents.
Drug dosing recommendations for treatment of tuberculous peritonitis.
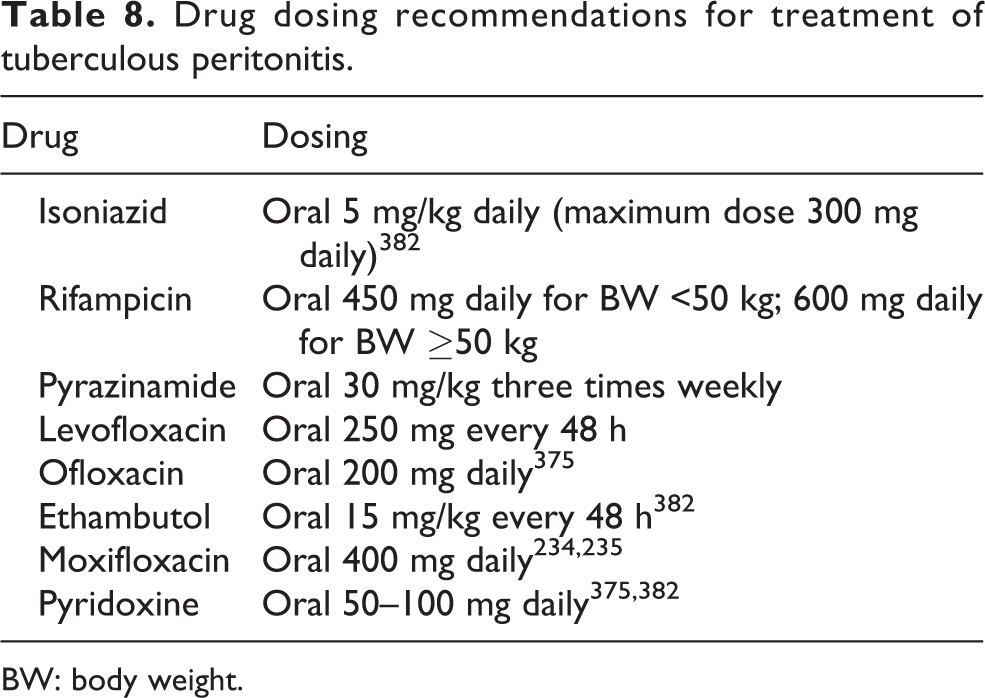
BW: body weight.
Many patients respond to anti-tuberculous therapy without catheter removal, although an attributable mortality of 15% has been reported. 378 In a scoping review 216 cases of Mycobacterium tuberculosis peritonitis in patients on PD, 377 catheter removal occurred in 52.4% of cases. Most of the cases requiring catheter removal were empirical, based on the rationale of failed treatment of ‘bacterial’ peritonitis before the diagnosis of tuberculous peritonitis was recognised. PD catheter removal was not associated with an increased probability of survival. 377 Early diagnosis is essential in the management of tuberculous peritonitis complicating PD because treatment delay is the only significant factor predicting mortality.
Non-tuberculous mycobacterial peritonitis
We suggest that Ziehl–Neelsen staining for acid-fast bacilli be requested when there is a clinical suggestion of non-tuberculous mycobacterial (NTM) peritonitis, including persistent culture-negative peritonitis (2D).
We suggest that NTM peritonitis be treated with both effective antibiotics and catheter removal (2D).
Mycobacterium fortuitum and chelonae account for the majority of NTM peritonitis episodes. 383 –385 Published case series have highlighted the pitfall of late NTM diagnosis, with a median delay ranging from 6 to 30 days. 384,386 Given the chance for these organisms to be mistaken for diphtheroids or Corynebacterium species on Gram stain, examination for acid-fast bacilli by Ziehl–Neelsen staining should be requested on peritoneal dialysate fluid. Negative cultures with persistent symptoms of peritonitis, often with concomitant exit-site infection, should also raise concern for the possibility of NTM infection. When suspected, the laboratory should be notified to prolong the incubation times of standard bacterial cultures to 7 days, in addition to using specific mycobacterial culture media. 386
There are few data on the optimal treatment duration of antibiotic therapy for NTM peritonitis. An observational study of 27 consecutive episodes showed a low complete cure rate of 14.8% despite treatment durations of more than 2 months. 384 Most experts recommend two agents to which the isolate is susceptible for a minimum of 6 weeks. 387 Antibiotic therapy should be guided by the isolated species (hence the susceptibility pattern) and then in vitro antimicrobial sensitivities. Microbiologists or infectious disease specialists should be consulted in the selection of combination antimycobacterial therapy. The majority of NTM are sensitive to amikacin, but in vivo resistance to clarithromycin often occurs due to active inducible macrolide resistance genes. 384,388 Although aminoglycoside trough level monitoring for PD peritonitis treatment is not mandatory (see above), therapeutic drug monitoring might be considered if amikacin is used, given the prolonged drug treatment requirement for NTM. 389 Based on the principle of managing NTM, surgical source control or removal of the infected source is the recommended approach. In addition to our suggestion to remove PD catheters for the treatment of NTM, previous studies showed that less than 20% of patients could be resumed on PD. 383 –386,390
Future research
Like all evidence-based guidelines, the current 2022 ISPD guideline is limited by the available evidence for monitoring and managing peritonitis.
In particular, evidence is lacking on how best to reduce culture-negative peritonitis or peritonitis episodes without identification of organisms. Studies examining novel diagnostic tools other than traditional microbiological culture are under way. Diagnostic difficulty with microbiological culture test alone has spurred interest in proteomics research. 391 These new biomarkers can potentially serve the prognostic purpose, and further guideline treatment decisions. Pathogen-specific immune fingerprints are promising clinical applications, 154,155,392 although machine learning application remains underutilised in nephrology research. 393,394
There is a paucity of research on IP drug dosing for APD, as opposed to CAPD. Further pharmacokinetic data are needed for managing peritonitis in patients on APD because it is not always feasible to convert such patients to CAPD. Furthermore, randomised controlled trials are needed to compare the efficacy and safety of different antibiotic regimens.
We also recognise the need of better strategies to prevent peritonitis. Notwithstanding the recognition of risk factors of peritonitis from observational data including international results from PDOPPS, 31 lack of interventional randomised controlled trials often lowers the level of evidence for the proposed recommendations. Clinical trials are also required in order to assess the benefit and harm of antibiotic prophylaxis before gastroscopy and dental procedures. Patients’ perspectives and understandings of peritonitis should be addressed. While recommendations for swimming, water sports or saunas have been published by the Global Renal Exercise Network, 395 many remain supported by a limited evidence base. Research in this area would benefit PD patients.
Supplemental Material
Supplemental Material, sj-pdf-1-ptd-10.1177_08968608221080586 - ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment
Supplemental Material, sj-pdf-1-ptd-10.1177_08968608221080586 for ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment by Philip Kam-Tao Li, Kai Ming Chow, Yeoungjee Cho, Stanley Fan, Ana E Figueiredo, Tess Harris, Talerngsak Kanjanabuch, Yong-Lim Kim, Magdalena Madero, Jolanta Malyszko, Rajnish Mehrotra, Ikechi G Okpechi, Jeff Perl, Beth Piraino, Naomi Runnegar, Isaac Teitelbaum, Jennifer Ka-Wah Wong, Xueqing Yu and David W Johnson in Peritoneal Dialysis International
Supplemental Material
Supplemental Material, sj-pdf-2-ptd-10.1177_08968608221080586 - ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment
Supplemental Material, sj-pdf-2-ptd-10.1177_08968608221080586 for ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment by Philip Kam-Tao Li, Kai Ming Chow, Yeoungjee Cho, Stanley Fan, Ana E Figueiredo, Tess Harris, Talerngsak Kanjanabuch, Yong-Lim Kim, Magdalena Madero, Jolanta Malyszko, Rajnish Mehrotra, Ikechi G Okpechi, Jeff Perl, Beth Piraino, Naomi Runnegar, Isaac Teitelbaum, Jennifer Ka-Wah Wong, Xueqing Yu and David W Johnson in Peritoneal Dialysis International
Supplemental Material
Supplemental Material, sj-pdf-3-ptd-10.1177_08968608221080586 - ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment
Supplemental Material, sj-pdf-3-ptd-10.1177_08968608221080586 for ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment by Philip Kam-Tao Li, Kai Ming Chow, Yeoungjee Cho, Stanley Fan, Ana E Figueiredo, Tess Harris, Talerngsak Kanjanabuch, Yong-Lim Kim, Magdalena Madero, Jolanta Malyszko, Rajnish Mehrotra, Ikechi G Okpechi, Jeff Perl, Beth Piraino, Naomi Runnegar, Isaac Teitelbaum, Jennifer Ka-Wah Wong, Xueqing Yu and David W Johnson in Peritoneal Dialysis International
Supplemental Material
Supplemental Material, sj-pdf-4-ptd-10.1177_08968608221080586 - ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment
Supplemental Material, sj-pdf-4-ptd-10.1177_08968608221080586 for ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment by Philip Kam-Tao Li, Kai Ming Chow, Yeoungjee Cho, Stanley Fan, Ana E Figueiredo, Tess Harris, Talerngsak Kanjanabuch, Yong-Lim Kim, Magdalena Madero, Jolanta Malyszko, Rajnish Mehrotra, Ikechi G Okpechi, Jeff Perl, Beth Piraino, Naomi Runnegar, Isaac Teitelbaum, Jennifer Ka-Wah Wong, Xueqing Yu and David W Johnson in Peritoneal Dialysis International
Supplemental Material
Supplemental Material, sj-pdf-5-ptd-10.1177_08968608221080586 - ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment
Supplemental Material, sj-pdf-5-ptd-10.1177_08968608221080586 for ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment by Philip Kam-Tao Li, Kai Ming Chow, Yeoungjee Cho, Stanley Fan, Ana E Figueiredo, Tess Harris, Talerngsak Kanjanabuch, Yong-Lim Kim, Magdalena Madero, Jolanta Malyszko, Rajnish Mehrotra, Ikechi G Okpechi, Jeff Perl, Beth Piraino, Naomi Runnegar, Isaac Teitelbaum, Jennifer Ka-Wah Wong, Xueqing Yu and David W Johnson in Peritoneal Dialysis International
Supplemental Material
Supplemental Material, sj-pdf-6-ptd-10.1177_08968608221080586 - ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment
Supplemental Material, sj-pdf-6-ptd-10.1177_08968608221080586 for ISPD peritonitis guideline recommendations: 2022 update on prevention and treatment by Philip Kam-Tao Li, Kai Ming Chow, Yeoungjee Cho, Stanley Fan, Ana E Figueiredo, Tess Harris, Talerngsak Kanjanabuch, Yong-Lim Kim, Magdalena Madero, Jolanta Malyszko, Rajnish Mehrotra, Ikechi G Okpechi, Jeff Perl, Beth Piraino, Naomi Runnegar, Isaac Teitelbaum, Jennifer Ka-Wah Wong, Xueqing Yu and David W Johnson in Peritoneal Dialysis International
Footnotes
Authors’ note
Philip Kam-Tao Li and David W Johnson are Co-Chairs of the ISPD Peritonitis Guidelines Working Group.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.