
Abstract
Cognitive and behavioral aspects may mask posttraumatic stress disorder (PTSD) in people with dementia. PTSD severely lowers quality of life in people with dementia. Proper recognition of PTSD is essential to ensure adequate treatment. However, a valid diagnostic tool for PTSD in dementia is lacking. A Delphi study was conducted among 20 Dutch and 6 international experts in the field of PTSD and dementia care or research. The aim was to reach consensus in 3 rounds on the added value, form, content, and application for developing such an instrument. The first round confirmed the need for a new diagnostic tool for research and clinical practice. Consensus was reached on 23 statements regarding the support base and 19 related to content of the instrument. In the third round, opinions on several conceptual problems were gathered. Based on the experts' opinions, a draft version of an instrument, the TRAuma and DEmentia-interview (TRADE-interview), was developed. Clinical and research implications of this new measure are discussed.
Objective
Although posttraumatic stress disorder (PTSD) is a common psychiatric diagnosis in the general population (7-8%),1,2 PTSD is not often diagnosed in older adults (1-3%).3,4 Evidence has been accumulated for important links between PTSD and dementia,5-8 with comorbidity rates of PTSD in people with dementia at 4.7-7.8%. 9 Globally, the number of patients with dementia is estimated to be 35.6 million in 2010 and will double almost every 20 years to approximately 115.4 million by 2050. 10 Based on the findings, affected patients with comorbid PTSD could be between 2.5-4.2 million (53.4*4.7-7.8%) in 2020 and increasing to 5.4-9.0 million (53.4*4.7-7.8%) in 2050. However, due to the lack of a structured diagnostic tool for PTSD in these patients, these are probably underestimates. 4 While the nature of the associations between dementia and PTSD is still unclear, several hypotheses about possible underlying mechanisms have been postulated.11-16 For example, PTSD and dementia share many comorbidities (e.g., impairments in attention and memory, depression, substance abuse, cardiovascular diseases).17-19
A decrease in perceived quality of life is known in both dementia and PTSD.20,21 It can therefore be assumed that the simultaneous occurrence of PTSD in people with cognitive impairment or dementia may further negatively affect the quality of life in many aspects. Dementia and PTSD are both common and place a significant burden on patients, family members and other caregivers. Pinciotti, Bass, McCarthy, Judge, Wilson, Morgan, Snow, Kunik 22 reported more difficult behavioral symptoms in people with dementia and comorbid PTSD than without PTSD, which also increased the burden on caregivers and, therefore, increase health care costs. Problem behavior can be a real challenge for informal caregivers and, in addition to dementia, has a huge impact on the quality of life of patients, relatives and others involved. 20 Better recognition of PTSD in people with dementia is essential to optimize personalized care to improve the quality of life and reduce problem behavior through less: intensive nursing care, medication, medical consultations, freedom-restricting or other coercive interventions.
Developments in the field are hampered by the current lack of a structured diagnostic tool for PTSD in individuals with dementia, which meets the standards of the classical test theory.23-25 Clinical assessment, assessing for exposure to potentially traumatic events and current PTSD symptoms, seems to be the most common method.23,26-30 Instruments that have been most often used for assessing PTSD symptoms in those with dementia are: Impact of Event Scale-Revised (IES-R), 31 Post Traumatic Stress Screen for the Cognitively Impaired (PTSS-CI), 24 PTSD Checklist-Civilian Version (PCL-C), 32 Clinician-Administrated PTSD Scale for DSM-V (CAPS-V)32,33 and the Mini International Neuropsychiatric Interview (MINI). 32
However, none of these instruments have been validated through the classical test theory in a population with dementia. 24 For example, they are based on self-report and/or anamnestic interviews, which are not conceivable in cognitively impaired populations. 34 Besides, these instruments often use complicated wording and response categories which are too complex for this population. Though the PTSS-CI was specifically developed for those with cognitive impairments, this screening instrument has not been validated through the classical test theory in older adults. The PTSS-CI is furthermore limited as it has been designed as a screening tool, and not a diagnostic instrument (which is the aim of the present study). Another important limitation in diagnosing PTSD in those with dementia is that published case reports show that most people with comorbid PTSD and dementia may not show enough symptoms to meet the criteria for a formal psychiatric diagnosis.23,26,30,32,35 For example, avoidance symptoms were in most cases not expressed. Many older adults with dementia may live in long-term care facilities, and thus experience and expression of their avoidance may be different and not endorsed. Also, older adults may also not connect their current symptoms with their past traumatic experiences, or may have modified their lifestyle so that avoidance is automatic rather than effortful (e.g., systematically avoiding interactions with other people or only going out when they are unlikely to confront others). 9 Furthermore, behavioral expression of PTSD symptoms could be misinterpreted and classified as being part of the dementia syndrome such as Behavioral and Psychological Symptoms of Dementia (BPSD). For instance, re-experience symptoms occurring during the night may induce perception of danger and thereby to nightly wandering and be classified as BPSD.23,28,30 In line with previous suggestions, 23 we have postulated that BPSD may also be linked to comorbid (yet undetected) PTSD, and that this link may be especially relevant in those with a delayed onset course. 36 Interestingly, thus far only one study reported higher levels of BPSD in people with dementia with comorbid PTSD compared to those without PTSD 22 . As PTSD, dementia, and BPSD all impact negatively on quality of life, 37 the combination may further decrease well-being. Thus, both in clinical practices as in research, there is a need for a structured method to diagnose PTSD in people with dementia. Recognition of PTSD can help health care practitioners give direction to management possibilities.23,38 For example, personalized trauma-focused psychotherapy, namely Eye Movement Desensitization (EMDR), has been shown to relieve BPSD in those with severe dementia.30,39
In order to improve knowledge on PTSD in dementia, increase treatment possibilities, decrease health care burden, and improve the quality of life in those with dementia, we aimed to investigate the added value of a new instrument to diagnose PTSD in people with dementia among international experts, and to assess the optimal form, content, and application of such a measure. The current Delphi study is the first initiative to develop such a diagnostic tool and its usability by using an international expert team.
Method
The Delphi methodology (i.e., soliciting opinions of experts through a series of questionnaires together with information and opinion feedback with the aim to establish convergence of opinion) was used for the present study. This method is most often employed when there is little to no empirical evidence or clinical consensus on the topic of interest.40,41 A Delphi design was used to reach consensus about statements with experts in PTSD and/or dementia. The survey rounds addressed: 1) the need for a structured method to assess PTSD in dementia, and whether current instruments might already be sufficient; 2) which domains and items should be included in the new instrument (TRAuma and DEmentia-interview; the TRADE-interview); and 3) scoring of items, diagnosis criteria, and severity measurement.
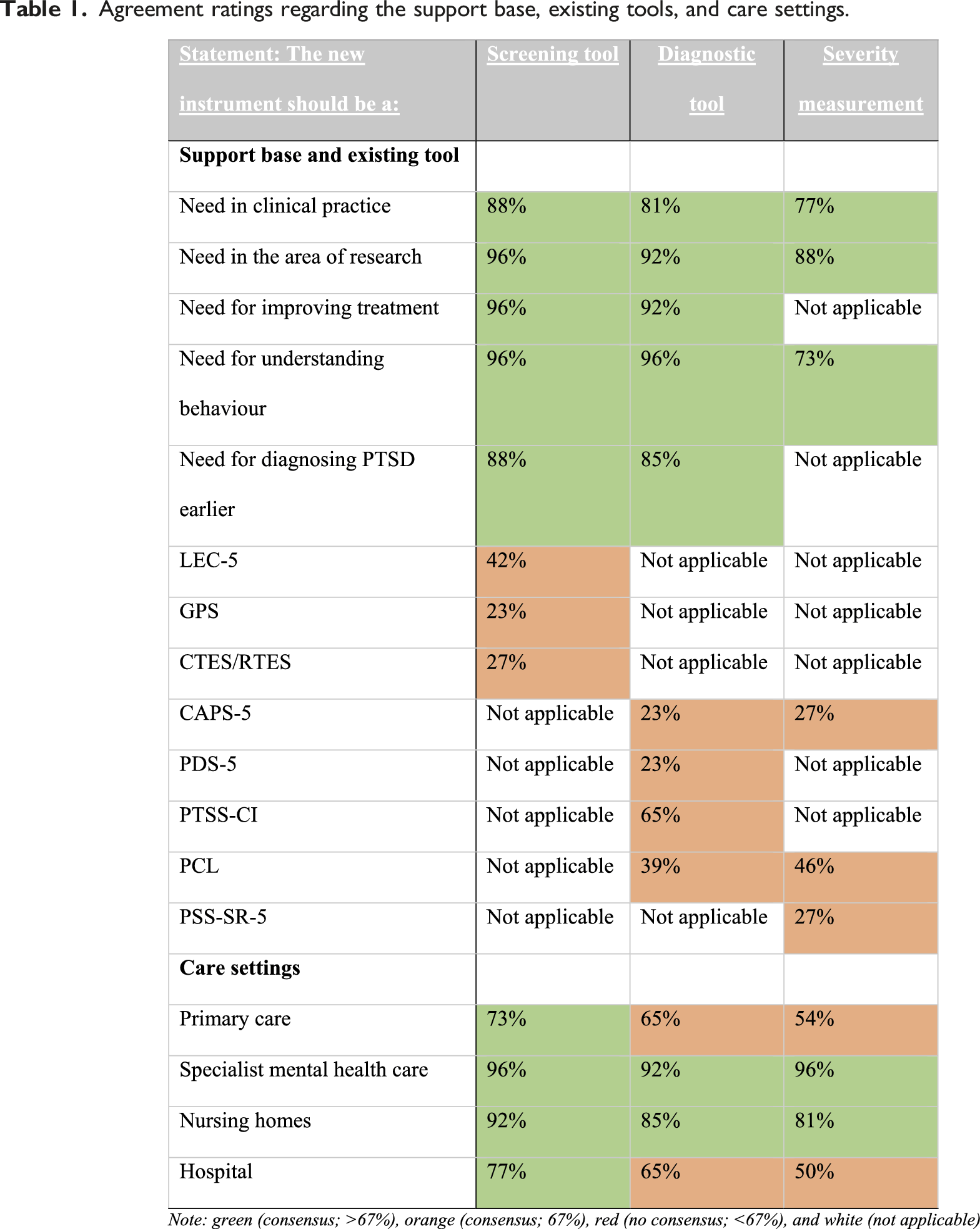
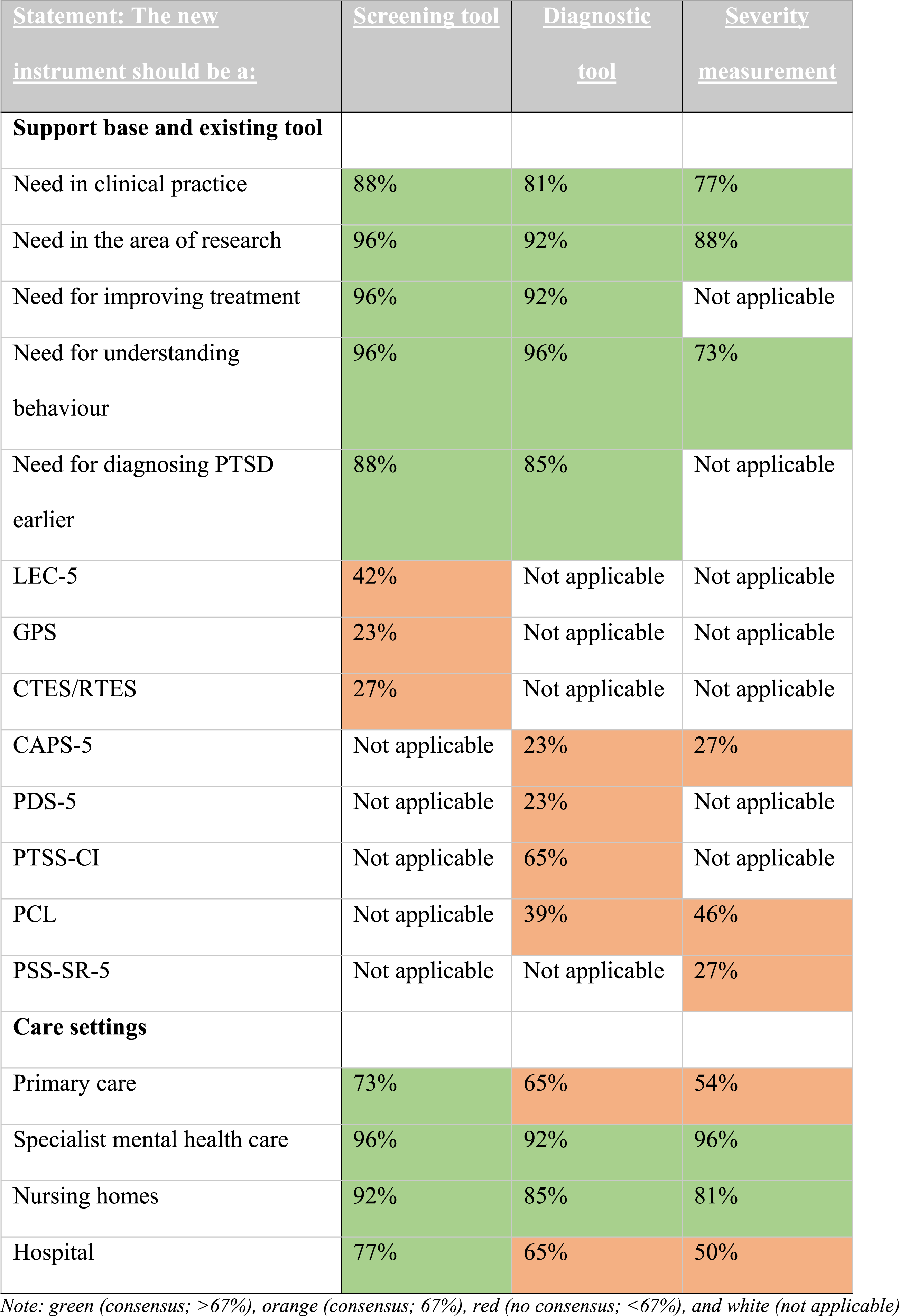
Agreement ratings regarding the support base, existing tools, and care settings.
Recruitment of Experts
The international and national experts were selected through: (1) an online search of relevant peer-reviewed publications on PTSD (i.e., in older adults) and/or BPSD and dementia; (2) consultation of national associations such as ‘Nederlandstalige Vereniging voor Psychotrauma’ (NtVp) and the Dutch association of specialists in geriatric medicine ‘Verenso’; (3) approaching international associations for trauma
The expert group consisted of psychologists, behavioral scientists, medical doctors all working in the field of psychiatry and/or geriatric care who met the following criteria: (1) had at least five years of clinical, research, educational, diagnostic or treatment experience with PTSD (trauma expert) or in the field of people with dementia (dementia expert); and (2) had an identifiable affinity with diagnostics, older adults and/or dementia when they were trauma expert, or they had an identifiable affinity with stress, PTSD, BPSD when they were dementia expert.
Procedure
The Delphi study’s statements were compiled through a literature search and supplemented with the research teams’ clinical and academic experiences (D.H., S.S., M.v.d.V, S.v.A., F.V. & B.R.). Each topic was briefly introduced (e.g., elements, main criteria, and sub-criteria), after which the experts were asked to indicate a level of agreement with each statement using a five-point Likert scale (i.e., Strongly agree, Agree, Neither agree nor disagree, Disagree or Strongly disagree). Responses of ‘Strongly agree’ and ‘Agree’ were grouped and categorized as agreement. The responses of ‘Disagree’ and ‘Strongly disagree’ were grouped and categorized as disagreement. Consensus was achieved when at least 66,7% agreed with a statement (strongly agree and somewhat agree). 42 Participants were given a chance to elaborate or express their opinion on the free-response comments. The results of the last part of round 3 were not designed to gain consensus, but rather to increase depth of experts' opinion. After each round, results were analysed and assessed in Microsoft Excel and implemented in the following round. Findings were discussed with the research team. Between the rounds, participants were provided a summary of the panel’s responses.
Between May and June 2020, experts received 3 questionnaires via Qualtrics, an online survey software tool that facilitates design and conducts online questionnaires. Experts were given 5 working days to reply in each round. If a participant did not respond after five days, they were excluded from the further rounds. The experts were reminded twice during these 5 working days through e-mail to complete the round. The average length of time between rounds was 5 to ten days.
Approval for this study was obtained from the Ethics Review Committee Psychology and Neuroscience (ERCPN) of the University of Maastricht. Before starting the study, an information letter was sent to the potential participants regarding the study’s aims, purpose, and requirements for participation. The participants were informed that the study was voluntary and that they had the right to drop out of the study at any time. Completion of the survey was deemed as consent.
Data were collected digitally using Qualtrics research software and were exported to Microsoft Excel for statistical analysis. The consensus was calculated for each statement using frequency, mean, and standard deviation formulas.
Results
A flow chart summarizing each round of the Delphi study and panel characteristics is shown in Figure 1. The appendix contains an extensive table with the results. Based on the experts’ opinions, a draft version of the TRADE-interview has been developed. Summary Delphi study and panel characteristics.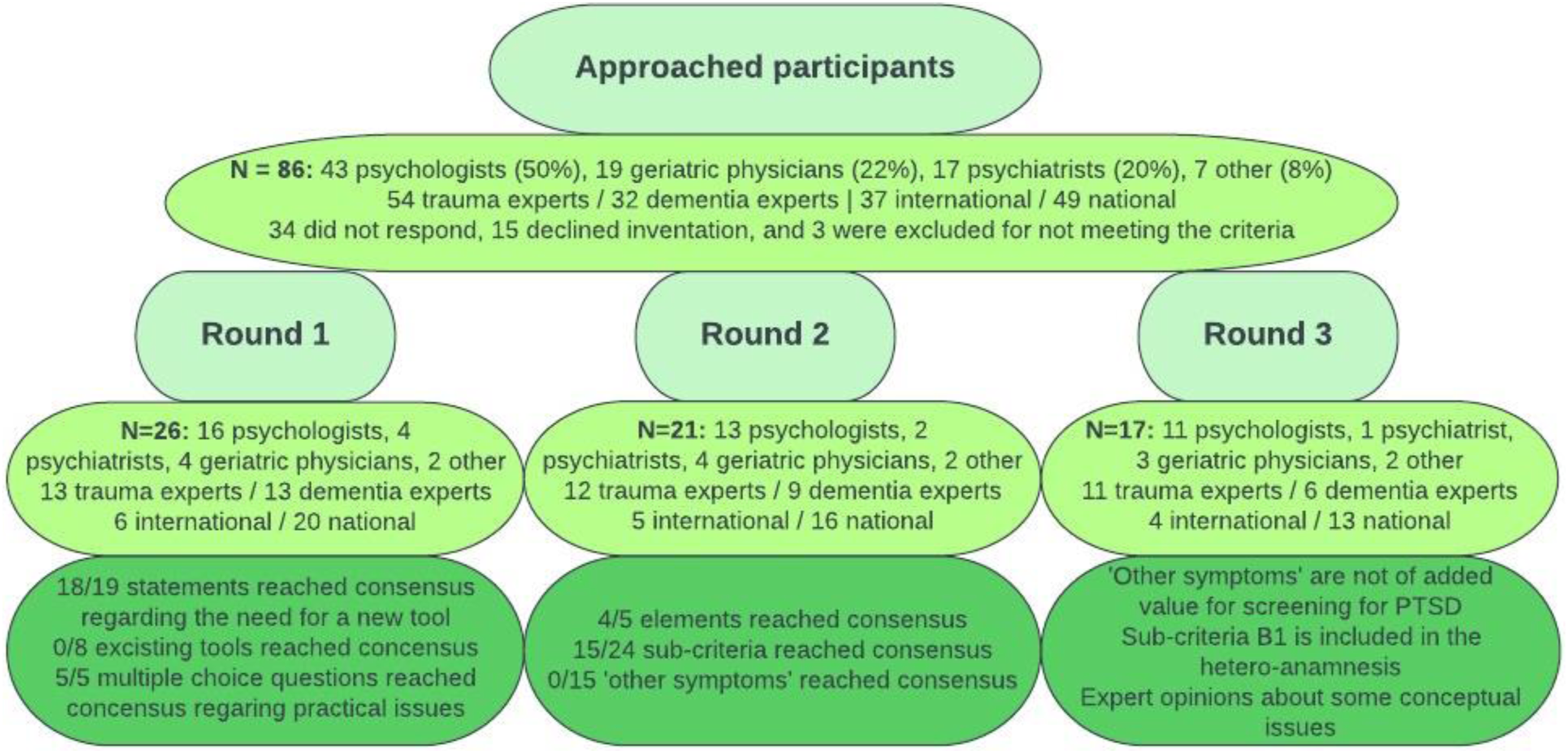
Support Base
Consensus was reached for developing a new instrument for the screener, the PTSD diagnostic, and the severity measurement of PTSD
The last part of round one was related to which health care disciplines the development of a new tool for screening, diagnosing, and measuring severity could be relevant
Content of the TRADE-Interview
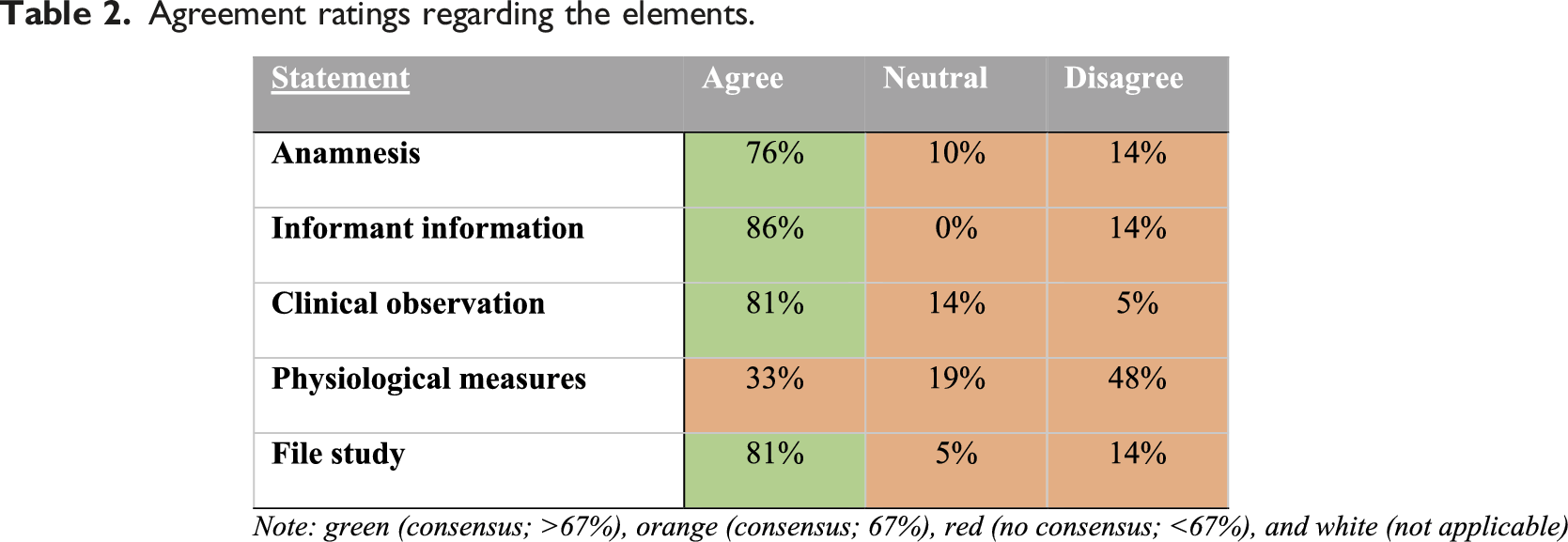
Agreement ratings regarding the elements.
Agreement ratings regarding sub-criteria and other symptoms.
Conceptual Issues
Conceptual issues regarding the implementation of the new instrument.
The second application issue was about how the new instrument can be used to diagnose PTSD, because in round 2 the experts indicated that nine sub-criteria of PTSD were excluded. The experts had very different answers to this question. There was no clear majority in any option, but most indicated that the diagnosis should be made based on a certain number of sub-criteria (29%) or chose the option ‘other’ (29%). Most indicated that before such cut-offs should and could be considered, we must await actual testing and observation. The third application issue contained the question of how the severity measurement would be determined at the observation part and at the end of the new instrument. No severity scale is added to the anamnesis and hetero anamnesis because the experts indicated several times that it is complicated for people with dementia and their relatives or friends to indicate severity reliably. Most of the experts chose the ‘other’ option, indicating that the severity should be assessed by determining how the symptoms impair function on a zero to 2 scale (41%). Moreover, 35% indicated that the severity should be assessed by the interviewer based on frequency and suffering.
Discussion
The main goal of the present study was to reach consensus among international experts about the added value of a new instrument to diagnose PTSD in people with dementia, as well as the form, content, and application of such a measure. This study is the first in addressing the need and requirements for a new instrument aimed at PTSD in those with dementia where the focus was on both diagnosis and severity, used simple language, adhered to DSM-5 criteria, and was not too long. The experts agreed on the need for this new instrument (TRAuma and Dementia-interview; TRADE-interview).23,24,44
In 3 rounds of discussions experts concluded that the ‘other symptoms’ and several sub-criteria (e.g., flashbacks, irritability, hyper-vigilance) should not be included because these were not specific for PTSD and could also be symptoms of BPSD or related to ageing.22,23,45 However, clinical presentations show that ‘other symptoms’, such as memory problems, screaming, and wandering are often described in those with dementia and PTSD.26,27,30 Thus, we suggest that the presence of 'other symptoms' can be used as an indicator for conducting the TRADE-interview. This also applies to the ‘physiological measurements’, for which several studies have shown that increased physiological reactivity related to trauma-related triggers is an excellent indication of a PTSD diagnosis.46,47 Much is still unknown about the 'other symptoms' and the ‘physiological measurements. It is possible that in the future, more knowledge about those aspects will become available and could be useful for future practical applications of the TRADE-interview. Further, especially for people with advanced dementia, these data could be valuable because the anamnesis is then even more limited.
At the end of the study, suggestions for application were made. Concerning the scoring of the items it was decided that 'yes' to at least one of the 3 components should be answered to meet a PTSD sub-criterion for the highest reliability.45,48 Regarding the diagnosis of PTSD, it was decided that one sub-criterion for the main criteria A (trauma), B (intrusion), and E (arousal symptoms) must be met to receive a diagnosis. The DSM-5 shows that these were the main essential criteria in cognitively impaired patients. 43 This can be explained by case reports in the literature that indicate that criterion C (avoidance symptoms) were rarely reported.23,49 Notably, most sub-criteria of criterion D (negative cognition and mood symptoms) were excluded in the TRADE-interview because they are indistinguishable from BPSD. Most experts indicated that before such cut-offs should and could be considered, actual testing and observation in practice should take place. When validating the instrument, it can be examined whether this is feasible or needs to be adjusted.
Although this study used the DSM-5 criteria to identify PTSD in people with dementia, ICD-11 should also be under consideration. The DSM-5 includes 20 symptoms, while the proposed ICD-11 criteria include only 6 qualifying symptoms for a more focused approach. 50 The ICD-11 has a unique way to identify PTSD avoiding overshadowing other disorders such as depression. 51 As a result, it could be expected that people with dementia, who are known to show less PTSD symptoms, are more likely to meet the diagnosis according to the ICD-11 compared to the DSM-5. However, a study from Fox, Hyland, McHugh Power, Coogan 52 found more older adults met the diagnostic criteria of PTSD based on the guidelines of the DSM-5 compared to the ICD-11. A shared limitation in diagnosing PTSD using the ICD-11 and DSM-5 is the required presence of one of the core elements ‘avoidance symptoms’, which a literature review show are not recognized in people with dementia.23,49
The development of the TRADE-interview has added value for both clinical practice and research. The TRADE-interview offers opportunities to conduct methodologically solid and consistent research into this complex target group. Clinically, this instrument can help in evaluating the indication for trauma-focussed therapy, such as EMDR and Prolonged Exposure therapy. Furthermore, the TRADE-interview can possibly differentiate potentially undiscovered PTSD in BPSD. In addition, more insight can be gained into the magnitude of the problem and about the occurrence of the impact of the PTSD symptoms in those with dementia. In future investigations, the TRADE-interview should be tested to assess its psychometric properties using classical test theory (i.e., diagnostic accuracy). 25 In addition, we hope to be able to investigate for which stages of dementia the instrument is suitable and possibly work towards an instrument that is useful for multiple stages of dementia. But most importantly, the first steps are made to improve diagnosing PTSD in people with dementia.
The primary limitations of this study were on the composition of the expert group which might have affected the finding. That is, the contribution of international experts (n = 4, 24%) was low compared to the Dutch experts (n = 13, 76%). However, as the opinions of international experts were overall in agreement with Dutch experts, that information bias is likely low. It is notable that 65% of the experts were psychologists, with the remaining psychiatrists (5%), geriatric physicians (18%) and other (12%). It was also a challenge to include experts who were experienced in the field of both dementia and PTSD. Nevertheless, 60% of the psychologists were experts on working with PTSD in the older population. Thus, the current composition of the expert panel seemed well-suited for the development of the TRADE-interview. It may be that the composition of the expert team was also influenced by the COVID-19 crisis, as the start of the study was scheduled in March 2020, which was in the early stages of the pandemic. The study had to be postponed to May, though there were a few participants (n = 6) who had withdrawn before starting due to the crisis. Another limitation of the current study is the use of the DSM-5 rather than looking into both DSM-5 and ICD-11. The ICD-11 has been included in the discussion, but in future it is important that the new instrument will also be translated to the ICD-11 guidelines. In addition, the expert panel decided to exclude some sub-criteria in the new instrument. This ensures that the symptoms are more specific to PTSD rather than explaining the dementia or other psychiatric diagnosis. However, with this we also risk missing symptoms, and this will therefore have to be investigated through the classical test theory (i.e., diagnostic accuracy) in further research.
The study results confirm the need for a diagnostic tool for PTSD in dementia patients for both scientific research and clinical practice. In accordance, with help of an international expert panel, we developed the TRADE-interview, which can be applied by health care professionals, particularly psychologists and doctors in primary care, specialist mental health care, nursing homes, and hospitals. In order to improve care of people with dementia with PTSD there are still multiple challenges beginning with testing its psychometric properties using classical test theory (i.e., diagnostic accuracy). Developing this tool may be the first step in discovering the impact of potentially traumatic life events in people with dementia and may hopefully lead to further initiatives to improve their care, treatment, and research.
Supplemental Material
Supplemental Material - The Need for a Diagnostic Instrument to Assess Post-Traumatic Stress Disorder in People with Dementia: Findings from a Delphi Study
Supplemental Material for The Need for a Diagnostic Instrument to Assess Post-Traumatic Stress Disorder in People with Dementia: Findings from a Delphi Study by Demi C.D. Havermans, Sebastiaan P.J. van Alphen, Miranda Olff, Mariëlle Van der Velden- Daamen, Frans Verhey, Bart P.F. Rutten, Peggy Stuijts, Joan M Cook, and Sjacko Sobczak in Journal of Geriatric Psychiatry and Neurology
Footnotes
Author Contributions
All authors contributed to the design of the various Delphi rounds, interpretation of results, reviewed and critically revised the article, and approved the final version for submission. After the study, D. Havermans, S. Sobczak, P. Stuijts and M. Olff were involved in developing the TRADE-interview.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received a grand by EMDR-Europe (2019-04) and is partially sponsored by University Fund Limburg (SWOL).
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.