
Abstract
We examined how family caregivers react, and what interventions they use in response to delusions exhibited by relatives with dementia in a community setting. Structured interviews were conducted with 68 family caregivers whose relatives were described as experiencing delusions based on the BEHAVE-AD or the NPI. Quantitatively, we cross-tabulated the type of response to delusion by the type of person providing the response and by the type of delusion manifested. Qualitatively, we analyzed open-ended responses to understand the types of caregivers’ responses to delusions, the contextual circumstances, and the impact of the responses. Caregiver responses to delusions included “Explaining that the delusion was wrong” (34% of responses), “Trying to calm down” (27%), “Agreeing with the delusion” (13%), “Distracting” (12%), and “Ignoring” (10%). Responses including “Anger, yelling or scolding,” were rare. The vast majority of reactions were by family caregivers of the persons with dementia. The relative frequency of the type of reaction tended to be consistent across delusion types. The qualitative analyses added some categories of reactions, but mostly highlighted issues to be considered when examining responses and their efficacy, including the use of multiple responses, and the manner and mood in which responses are conveyed. To cope with delusions, family caregivers develop intuitive intervention techniques. Understanding those interventions and reactions by caregivers and their relative efficacy can inform guidance programs for family caregivers. Improved support for family caregivers has the potential to positively influence the behavior of caregivers and older adults with dementia and improve their respective quality of life.
Introduction
Delusions are often considered a psychological and behavioral symptom in dementia, 1 yet findings concerning their prevalence at different stages of dementia have been inconsistent, possibly attributable to different study designs, procedures, and varying operational definitions of delusions. 2 The assumption that delusions manifested by persons with dementia (PwD) represent psychotic symptoms has been challenged as studies have shown that for most PwD, delusions may not be psychotic symptoms, but rather an expression of dementia-related deficits. 3 This paper utilizes a revised version of the Iterative Model of Environment and Delusion in Dementia, 4 according to which delusions represent reality for many PwD as they experience it through the prism of their sensory and memory deficits, as well as their past experiences. The combination of the content of the delusion, its impact on PwD behavior and affect, and caregiver background all affect caregivers’ reactions and interventions. Those, in turn, may impact the PwD’s behavior and affect in response to the delusion (Figure 1).
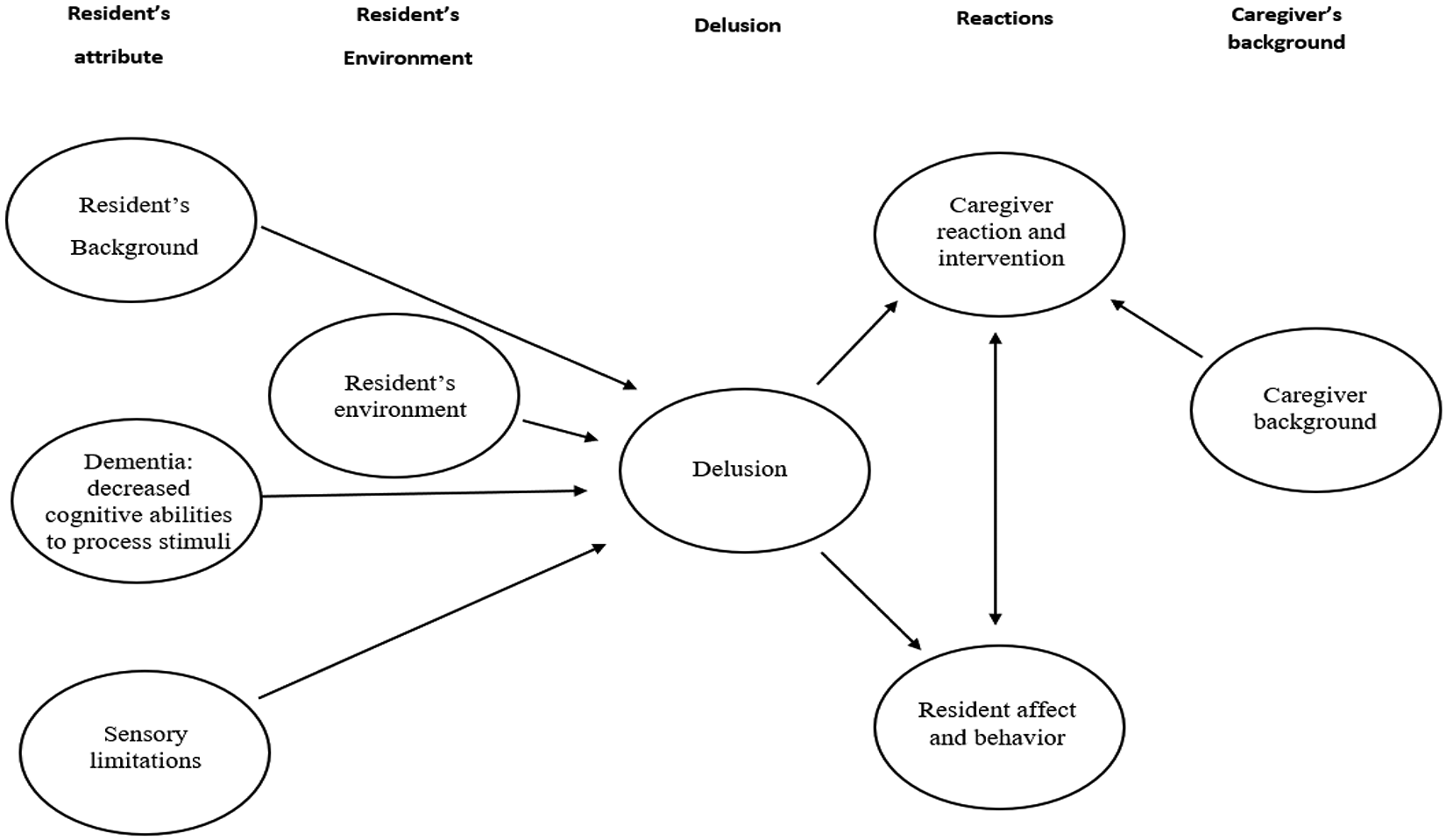
The iterative model of environment and delusion in dementia—revised.
Understanding both the phenomenon and how caregivers react when PwD exhibit delusions are prerequisites for providing optimal treatment for the management of delusions.
Despite gaps in knowledge about dementia symptoms, pharmacological interventions are frequently used,5-7 often accompanied by serious side effects.6-8-11 An alternative is the use of nonpharmacological interventions,12,13 offering a more personalized approach to care that does not solely focus on the patient as the cause of the problem, but takes into account PwDs’ interactions with their environment, caregiver, and system of care. 14 Such interventions should be incorporated into guidance for formal and informal caregivers of PwD to help manage delusions, which have been reported to be one of the dementia symptoms that generates the most burden and distress among caregivers.15-19
The inadequacy of approaches to delusions by caregivers 20 may worsen the manifestations of delusions, or other challenging behaviors. 21 In a focus group-based study of family and PwD interactions around behavioral and psychological symptoms of dementia, family caregivers described using negative coping methods (e.g. “confronting the behavior” or “bursting out in anger”) and developed more positive strategies (e.g. “pacifying” or “preventing cause of behavior”) after they better understood the patients’ needs. 22 Song et al argued that positive strategies were more successful in calming PwD or stopping the symptom. Both formal 4 and informal caregivers 22 may not always be aware of the different options and best strategies to address challenging behaviors of PwD.
Further research about informal caregivers’ interventions is particularly needed since most PwD are cared for by informal caregivers. 23 Informal caregivers were reported to be more distressed than formal caregivers when confronted by what they perceive as delusions, 24 and they reported higher rates and greater severity of delusions and being more emotionally involved with the older adult. 25 Consequently, there is a need to further investigate the nature of informal caregivers’ reactions and interventions in order to promote a higher level of well-being for PwD and reduce the burden for informal caregivers. Accordingly, we examined how family caregivers react and what interventions they use in response to the specific types of delusions exhibited by their relatives with dementia in a community setting.
Methods
Participants
Participants were 68 family caregivers of persons with a diagnosis of dementia who were at least 65 years old. The largest group of participant-caregivers were adult children (43 - 33 daughters, and 10 sons); followed by spouses (21); daughters-in-law (2); a sister (1); and other family members (3). Participants were recruited from 15 adult day centers, 8 support groups for caregivers of PwD, and an online advertisement. Inclusion criteria were: PwD not having a known acute or unstable medical condition, and capable of at least a minimal level of verbal communication.
Although 151 participants were recruited, we include only those caregivers who reported that the older person for whom they cared displayed a delusion that is designated on the Behavioral Pathology in Alzheimer’s Disease (BEHAVE-AD 26 ) or the Neuropsychiatric Inventory (NPI 27 ), and caregivers who responded to the study question regarding reaction to the delusion (n = 68).
Standard Protocol Approvals, Registrations, and Patient Consents
Written informed consent was obtained from the legally responsible family member after the nature of the study and its procedures were fully explained. The IRB of Tel Aviv University and the Helsinki committees of the Shoham Geriatric Center and the Sourasky Medical Center approved this study.
Assessments
NPI
Each type of delusion (being in danger, stolen from, spouse having an affair, thinking people are not who they say they are, believing fictional characters are present, and other unusual occurrences) experienced during the month prior to the interview is marked as either occurring or not occurring. Cronbach’s alpha for internal consistency was α = .91 for the entire sample (n = 151).
BEHAVE-AD
Each type of delusion (e.g., “people are stealing things,”) is rated on a 4-point scale, from 0 (symptom not present) to 3 (severe presentation of the symptom including violent action). Cronbach’s alpha for internal consistency was α = .81 for the entire sample (n = 151).
Etiological assessment of psychotic symptoms in dementia (EAPSID)
The EAPSID is an assessment tool developed for this study, which provides a functional analysis of psychotic symptoms which have been assessed via the NPI or the BEHAVE-AD. It evaluates psychosis in dementia from an etiological perspective, based on the nomenclature described by Cohen-Mansfield. 28 Questions inquired about the type of delusion, reactions of others to the delusions, PwDs’ verbal expressions of the delusions, and ways of reacting to the delusion. Some questions were specific to the identified delusion (e.g., What does the PwD claim was stolen from him/her? (Theft)).
Functional status was assessed using an Activities of Daily Living (ADL) questionnaire and Instrumental Activities of Daily Living (IADL), both based on the Older Americans’ Resources and Services. 29 The scores range between 0-14 for the ADL and 0-16 for the IADL, with a higher score indicating higher function.
The Mini Mental State Examination 30 was administered to participants unless it had been administered up to 3 months prior to the interview and was available from the PwD chart. We were unable to administer the MMSE to 14 of the PwD who were reported to experience a delusion, either because of participant or caregiver refusal. In those cases, we extrapolated the MMSE score on the basis of the Brief Cognitive Rating Scale (BCRS), 26 which included 4 questions regarding concentration, recent and past memory, and orientations.
Procedure
The assessment measures described above were translated from English to Hebrew by 2 independent translators. A third translator examined discrepancies and revised the translation after consultation with the researchers.
Structured interviews were conducted with the family caregivers to obtain data about the background and context of the older persons’ delusions and others’ reactions to them.
Analytic Approach
Quantitative approach
We conducted 2 cross-tabulation analyses to clarify the responses to delusions. The first cross-tabulated the type of response by the type of person providing the response, and the other examined the type of response by type of delusion.
Qualitative approach
We analyzed open-ended responses qualitatively to gain an understanding of viewpoints and motives that guided responses to delusions as well as their contextual circumstances, 31 and to explore the impact of those responses. This approach also enabled us to check for additional interventions or reactions that may not have been apparent from the quantitative data.
We used a thematic approach for the qualitative analysis, 32 drawing on Castleberry and Nolen 33 ’s five-step-model: (1) compiling through transcription of the data, (2) disassembling data into meaningful categories through coding, (3) reassembling the data by connecting the codes into relevant themes based on the research question and the literature review. This process was conducted independently by different members of the research team, (4) ongoing interpretation of the data in relation to the research question, and (5) drawing conclusions responding to the questions. Quotes exemplifying themes are identified by participant number, type of relationship to PwD, age of participant caregiver, and type of delusion, followed by age and sex of PwD.
Results
Quantitative Analysis
The background characteristics of the older persons who experienced delusions are displayed in Table 1.
Characteristics of Participants (n = 68).
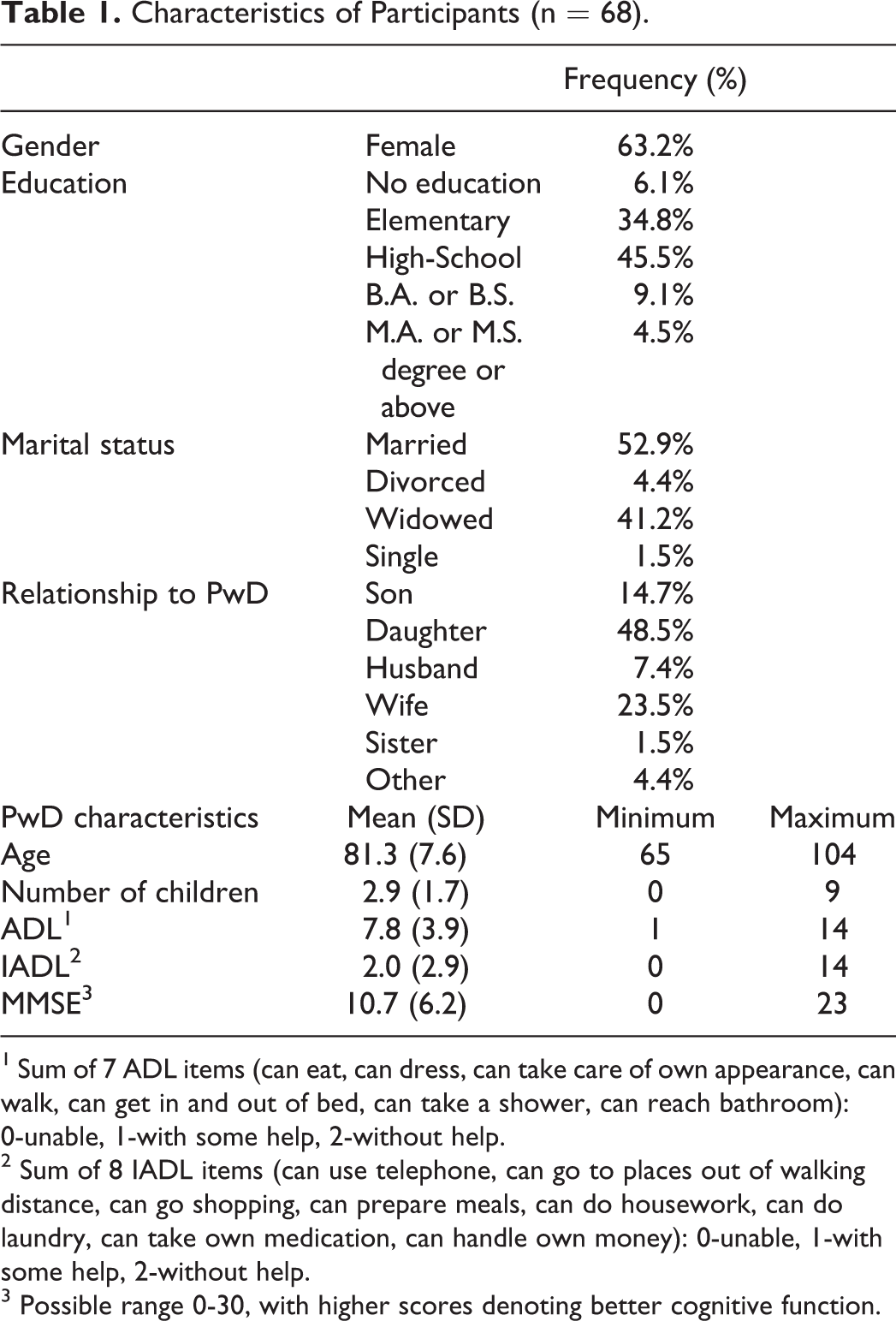
1 Sum of 7 ADL items (can eat, can dress, can take care of own appearance, can walk, can get in and out of bed, can take a shower, can reach bathroom): 0-unable, 1-with some help, 2-without help.
2 Sum of 8 IADL items (can use telephone, can go to places out of walking distance, can go shopping, can prepare meals, can do housework, can do laundry, can take own medication, can handle own money): 0-unable, 1-with some help, 2-without help.
3 Possible range 0-30, with higher scores denoting better cognitive function.
Their average age was 81 and 63% were female. About a third received an elementary school education and close to half received a high school education. About half were married and around 40% were widowed. The average MMSE score was 10.7 (s.d. 6.2) with a very broad range of cognitive function (0-23).
The severity of delusions by type of delusion according to the BEHAVE AD is presented in Table 2, showing that delusions were present at all levels of severity, with the lowest level—of the delusion being present—reported for 61% of the delusions, and the highest severity—of violent manifestations—reported to occur in 10% of the delusions overall. According to reports of delusions on the NPI, 27% occurred less than once a week, 23% about once a week, 20% several times a week but less than once a day, and 30% once or more per day. The severity according to NPI was mild for 51%, moderate for 26% and marked for 23%.
Frequency of Delusions by Type and Severity on the BEHAVE-AD.
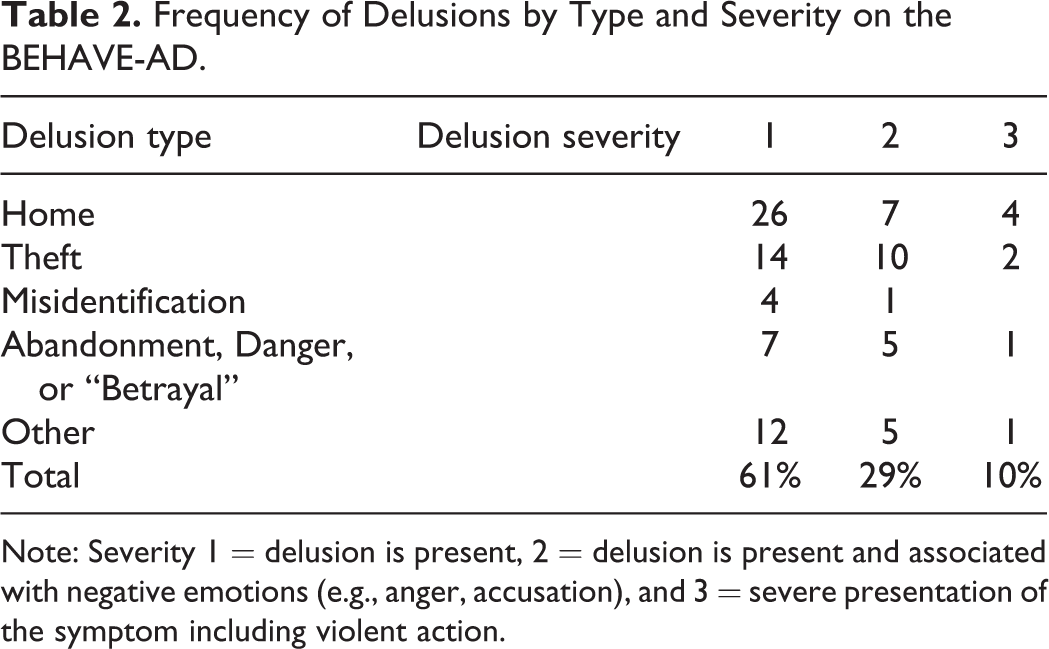
Note: Severity 1 = delusion is present, 2 = delusion is present and associated with negative emotions (e.g., anger, accusation), and 3 = severe presentation of the symptom including violent action.
Responses to the delusions were provided mostly by relatives of the PwD (91% of all responses), with only small numbers described as originating by senior daycare staff, other participants at the center, or visitors (Table 3).
Responses and Interventions Reported to Occur in Response to the Delusions by Identity of Person Responding.
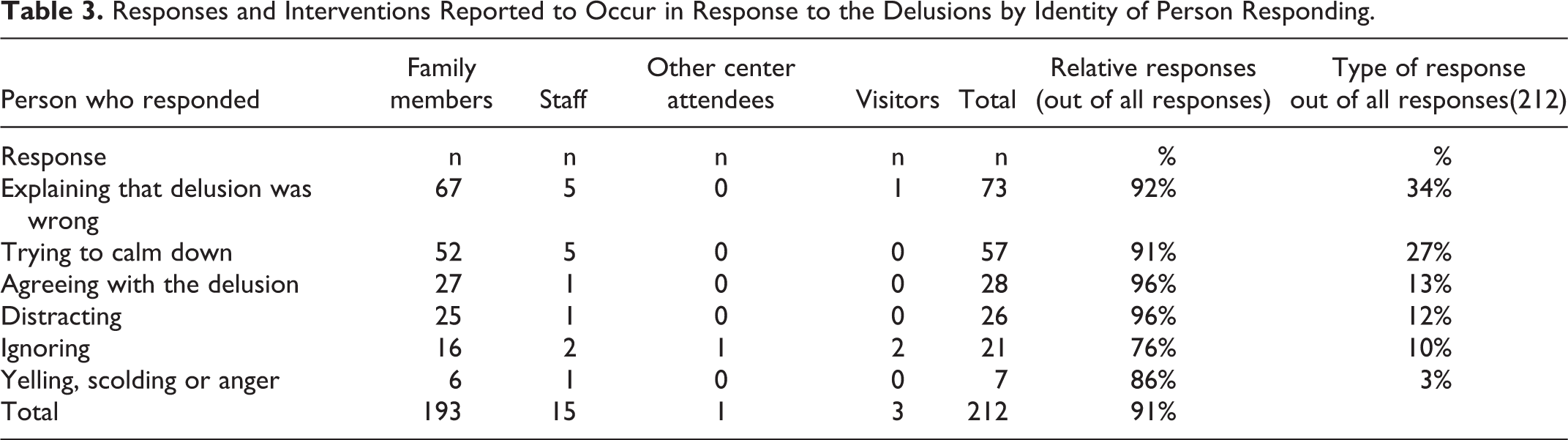
The most common response, directed toward the PwD, was “Explaining that the delusion was wrong,” which represented over a third of the responses. This was followed by the responses: “Trying to calm down” (27% of responses), “Agreeing” with the delusion (13%), “Distracting” (12%), and “Ignoring” (10%). Other types of responses, including “Anger, yelling or scolding,” were relatively rare.
The cross-tabulation of reactions to delusions by type of delusion is presented in Table 4.
Number of Responses and Persons Receiving Them by Type of Delusion.
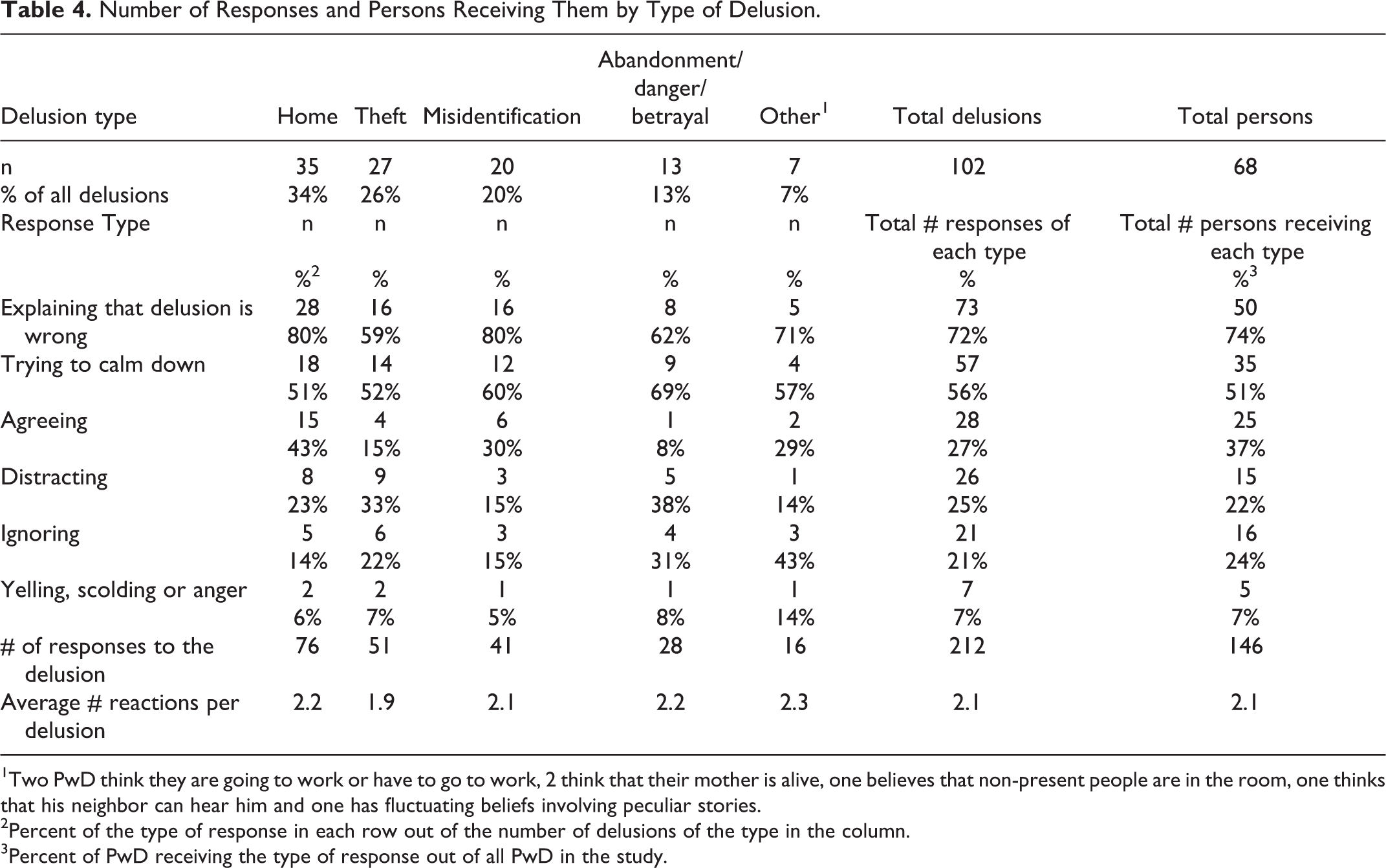
1Two PwD think they are going to work or have to go to work, 2 think that their mother is alive, one believes that non-present people are in the room, one thinks that his neighbor can hear him and one has fluctuating beliefs involving peculiar stories.
2Percent of the type of response in each row out of the number of delusions of the type in the column.
3Percent of PwD receiving the type of response out of all PwD in the study.
The most common delusions were “Believing where they live is not their home” (34%), “Theft” (26%), and “Misidentification” (20%). In contrast, delusions of “Abandonment” (5%), “Danger” (4%), and “Betrayal” (4%) were quite rare and therefore combined, given that they all convey a sense of fear and danger. On average, 2.1 reactions or interventions were reported per delusion. For all types of delusions we examined, the most common responses were “Explaining that the delusion was wrong” (displayed in 72% of delusions on average, Table 4) and “Trying to calm down” (56%). “Explaining that the delusion was wrong” was a response to 80% of delusions of “Believing where they live is not their home” and the same percent for “Misidentification.” Other relatively common reactions to delusions were “Agreeing”—most common for the delusion of not living in one’s home (43%), “Distracting,” most common in cases of delusions of “Abandonment, Danger, or Betrayal” (38%) or of “Theft” (33%), and “Ignoring”—most common in delusions of “Abandonment, Danger or Betrayal” (31%). Reports of “Yelling, scolding or anger” were relatively rare (displayed in 7% of all delusions).
Qualitative Analysis
Interventions and Reactions
Explaining that the delusion was wrong
Some responses attempted to explain that the delusion was wrong, “Explaining to her that she has no money, [there is] nothing to steal” (Participant # 1701, Caregiver: daughter, age 50, delusion type: Theft, PwD: female (f), age 71), or “[I] just explain and make her realize she has nowhere else to go except a senior home.” (Note: Having tried living in a senior home, the PwD moved to her son’s home 2 years prior to the interview; # 3561, son, 50, Believing where they live is not their home (Home), PwD-f-89). This intervention sometimes included the intention to reassure the PwD and to restore a feeling of safety. For example, one PwD mistook his spouse for his mother or his sister, and his wife tended to respond by explaining and reassuring, “Talking to reassure, explaining that mother died, his sister died and the other sister is in Brazil” (# 1231, wife, 74, Misidentification, PwD, (m) male, 84).
Another form of “Explaining that the delusion was wrong” was offering proof that challenges the delusion, for example, “Never say [what she says] is wrong but rather that it is her home and show her her things” (# 3431, daughter, 48, Home, PwD-f-87). Offering “proof” is exemplified by “Trying to prove to her, [showing] the ID of the son and death certificate of the father” (# 1551, daughter, 66, Misidentification, PwD-f-90). Another participant reported that confronting the PwD with the reality of the death of a loved-one by providing an appropriate ceremony had been beneficial for her:
Trying to explain to her that they have passed away, that she is already 80 and that it does not make sense that her mother would be alive. We took her to the grave and it was very helpful. It helped her get closure and she stopped talking about it for now (# 1511, daughter, 55, Other: worry about parents, that they may need her, she wants money to travel to search for them, PwD-f-80).
Other examples of this intervention’s success in stopping the delusion were, “When he returns home, he is not always sure it’s his house, but if I tell him it’s his home, he believes me” (# 1081, wife, 74, Home, PwD-m-76). However, “offering proof” was often reported as having no effect on the delusion, for example, “Suddenly she said she wanted to go from here [from the house]. When asked “Where to?” she said “Home.” So she was told that this is her home and she repeated that she wanted to go home” (# 1271, daughter, 55, Home, PwD-f-89), or “She accepts that the object shown to her was not stolen, but she claims she meant another object and the idea of theft still remains” (# 3341, daughter, 60, Theft, PwD-f-82). When explanations were not efficacious, caregivers’ intentions were directed toward calming the PwD and providing a proof, “Soothing and resolving here and now rather than explaining—the explanation is irrelevant to her—providing the reassurance solved the problem. Like showing her the item that was allegedly stolen from her” (# 3441, son, 61, Theft, PwD-f-87).
Trying to calm down
“Calming down” was not only a goal, but a strategy. Many participants described reassurance as an effective way of dealing with a delusion, for example, “As much as possible to make him feel safe” (# 1841, wife, 86. Home, PwD-m, 92), or “Assure her that I will be back” (# 1611, daughter, 40, Abandonment, PwD-f, 75).
Touch was often used to calm the PwD down, for example, by hugging (# 1281, wife, 70, Abandonment, PwD-m-84), or hugging and kissing (# 1081, wife, 74, Home, PwD-m-76).
Trying to calm down was also described as effective, as in, “I told her that everything was fine, she was enjoying relaxation and her mind was already somewhere else” (# 1251, daughter-in-law, 54, Abandonment, PwD-F-82).
Agreeing
In contrast to “Explaining that the delusion is wrong,” some participants preferred to simply agree with the delusion, “Agree and reassure and seek what is allegedly stolen” (# 1141, sister, 72, Theft, PwD-m-73), or “Flow with it, not resist” (# 3141, son, 56, Misidentification, PwD-f-80). One of the reasons given for “Agreeing” is that it is not possible to convince the PwD that the delusion is wrong (# 1171, daughter, 50, Home, PwD-m-73).
“Agreeing with the delusion” was also described as an adequate response when the delusion was seen as beneficial for the PwD. In the following example, a daughter described that her father speaks to himself in the mirror, imagining a friend:
Every time he sees himself in front of the mirror it happens to him. Also, he does it on purpose—he goes to the mirror to talk with the “friend.” At first, we thought of taking the mirrors out of the house, and it was difficult for us to let the grandchildren see it [the delusion]. Then we realized it calms him down, we treat it as something creative on his part, and that’s fine with us. (# 3171, daughter, 40, Other, PwD-m-70)
Distraction
In order to calm the PwD, participants reported that they tried to distract the PwD, for example: “Taking her for a walk outside to calm her down” (# 1531, female relative, 61, Home, PwD-f-90), or “Just move the mind to something else, to do things she loves” (# 1251, daughter-in-law, 54, Danger, PwD, f-82). Sometimes, this intervention was combined with explaining or providing a proof: “To cooperate, not to ignore, but to distract him from the topic. I show him that this is his home, ask him if it’s good for him at home, he says yes—’then this is your home’” (# 3171, daughter, 40, Home, PwD-m-70).
Distraction was described as a relatively efficient intervention, e.g. “Distract her. It helps. In this [way] she does not repeat herself like a record, in contrast with other situations” (# 3241, son, age unknown, Home, PwD-f-80).
Ignoring
There seemed to be two ways in which this intervention was used. Some participants used it as a strategy to wait for the PwD to calm down, for example, “Waiting for her to relax because I know that she will forget and it will pass” (# 1721, daughter, 53, Theft, PwD-f-80). Yet, ignoring also emerged as an expression of resignation on the part of the caregiver, when no other intervention seemed to stop the delusion, “I used to be angry with my mother and argue with her but today [I know] there is nothing else to do except to ignore it because no matter what I say you can’t persuade her otherwise” (# 3321, daughter, 68, Betrayal, PwD-f-89). Another participant, who reported ignoring the delusion described it as ineffective: “There is no solution in my opinion [to deal with the delusion]” (# 1691, husband, 84, Home, PwD-f-80).
Yelling, scolding or anger
In some cases, participants scolded the PwD, for example: “I threaten him—if I’m not his wife then he should not sleep with me tonight and instead stay in the living room” (# 1961, wife, 65, Misidentification, PwD-m-65), or “I tell him that it is wrong and not logical” (# 1971, wife, 80, Betrayal, PwD-m-83), or “Her daughters are usually unwilling to listen to mother, and are yelling at her [about the delusion]” (#1101, son, 56, Home, PwD-f-80). Since this intervention was rarely reported, there were no explicit descriptions about its efficacy, but one participant stated that she feared that the anger that she expressed as a response to the delusion may have explained the delusion (# 1961, wife, 65, Other, PwD-m-65), suggesting that the delusion was a response to her anger.
Other interventions
Other reported interventions included “Pretending/deceiving,” “We take her for a walk around the house and return her as if she had arrived at her house” (# 1551, daughter, 66, Home, PwD-f-90); improving the PwD’s environment, “If [the PwD] had a bigger house, more space, less loneliness [the delusion could be dealt with]” (# 1531, female relative, 61, Home, PwD-f-90), and “To spend more time with her, to keep her engaged and occupied. The family can’t come all the time and now we are trying to get someone to volunteer or a caregiver to keep her busy” (# 1311, daughter, 50, Other, PwD-f-75), or “To arrange a specific and permanent place for her belongings like money” (# 3251, daughter, 54, Theft, PwD-f-82), or “I tried to hang a large calendar, a big clock for her, to give her instructions for the Sabbath, and to write everything down for her” (# 1681, daughter, 53, Other, PwD-f-82). Pretending or deceiving was often referred to as a successful intervention, “She approaches the door and wants to go to her home; sometimes it’s enough to take her outside and come back and sometimes it is necessary to go downstairs to calm her down” (# 3431, daughter, 48, Home, PwD-f-87).
Discussion
This paper provides preliminary data on the range of nonpharmacological interventions used by caregivers to manage delusions experienced by community dwelling PwD, and examples of the efficacy of specific strategies. The quantitative analyses found that the vast majority (over 90%) of reactions/interventions reported were performed by close relatives. The most common interventions were, in declining prevalence, explaining that the delusion was wrong, trying to calm the PwD down, agreeing with the delusion, distracting the PwD, and ignoring the delusion. The most common delusions were, in declining prevalence, believing where they live is not home, theft, and misidentification. Despite varying rates of prevalence of different interventions to different delusions, the ordinal level was maintained across types of delusions, such that “explaining that the delusion was wrong” was the most common intervention—with the exception of the combination of “abandonment, danger or betrayal,” where it was a close second to “calming down.” “Agreeing” was third, with the exception of theft, and abandonment/danger/betrayal, where “distraction” and “ignoring” were more common than “agreeing,” probably because caregivers found it more difficult to agree when they were personally implicated as having caused harm to the PwD.
The qualitative analysis validated most of the categories used in the quantitative analysis and clarified their nature and circumstances. It also suggested that a more refined nomenclature could improve the understanding of the results. For example, the intervention of explaining that the delusion was wrong may need to be divided into those that are verbal, and those that utilize forms of providing “proof.” In many cases, interventions were complex in that they involved multiple strategies, such as trying to calm down, distracting, and explaining that the delusion is wrong. This needs to be examined in future research. Another factor that emerged was the influence of mood conveyed by caregiver on intervention impact, being either soothing and calm, or angry and impatient. Similarly, the components of “calming down,” such as tone, hugging, kissing, verbal assurance warrant further study. The interaction between the impact of delusion and the intervention was illustrated by the example of the man who talked with his image in the mirror, where the family learned that the delusion was positive for the person (as has also been found in multiple examples in Cohen-Mansfield, Cohen, Golander and Heinik 34 ).
The qualitative analysis also aimed to examine the efficacy of different strategies. The impact of explaining that the delusion was wrong emerged as mixed, potentially dependent on the manner in which the explanation was provided, or the nature of proof presented, or the circumstances, such as with the distraction of a walk outside. Trying to calm down, agreeing, and distracting were generally reported as effective. Ignoring emerged as an intervention of last resort.
The qualitative analysis revealed additional interventions that need to be examined quantitatively, namely pretending/deceiving, and environmental change, and the difference between “explaining” and “explaining while providing a proof.” The interventions of environmental changes reflected what could or should be done, rather than actual interventions, and their impact is yet to be examined.
The role of lying as part of the treatment of PwD has been discussed in James and Caiazza 35 and Lorey 36 . It appears to be a component of the agreeing strategy and the pretending/deceiving strategy. On the one hand, such strategies are often perceived as efficacious in that they result in calmer responses by PwD than alternative strategies, yet they can impair the relationship between caregiver and the PwD, through loss of trust by PwD and loss of respect by caregiver. In contrast, “explaining that the delusion was wrong” would seem like telling the truth, yet, that often results in conflict between caregiver and PwD. Understanding the nuances of telling the truth and using of alternative approaches described in this paper may help caregivers avoid lying to their relatives. Future study should explore their efficacy, and the effect on both parties.
A larger perspective of considering the alternatives of providing the truth (telling the PwD the delusion is wrong) vs. agreeing with the person may be clarified by examining the intervention approaches of reality orientation 37 vs. validation therapy. 38 While participating family caregivers obviously were not aware of those approaches, this paper demonstrates that family members develop sets of intuitive alternative intervention techniques in order to cope with delusional restlessness. The extent to which the choice of intervention represents a continuation of prior communication patterns or reflects the relationship between caregiver and care-receiver, or is based on the needs of the PwD or those of the caregivers (see 39 ) needs to be examined in future research.
This study extends previous findings on reactions and interventions for delusion. 4 The previous research involved a smaller sample of nursing home residents in contrast to community-dwelling PwD in the current study. It reported “calming down” as the most common intervention, followed by “agreeing” and “arguing.” The differences in frequency of use may be due to more training of staff in nursing homes, or to ambiguity as to the meaning of terms such as “calming down,” and to the use of different terminologies, such as “arguing” vs. “explain that the delusion was wrong.” Similar to Song, Park, Park, Cheon and Lee 22 , we found that interventions of pacifying and distracting were sometimes effective. However, Song, et al’s study examined behavioral and psychological symptoms of dementia (BPSD) in general, and the examples given referred to aggressive behaviors, agitation, and delusions. It is likely that these behaviors differ in their etiology and that a more specific approach to each type of BPSD is warranted, which is the approach taken in this study.
A better understanding of family caregivers’ reactions and interventions, and specifically nonpharmacological treatments for dementia, can help inform training programs for family caregivers. Previous research about training interventions for family caregivers of PwD demonstrated their effectiveness in enhancing caregivers’ knowledge of everyday skills in caring for PwD 40 and in decreasing caregiver burden and care-recipients’ problem behaviors. 41 Improved guidance for relatives would include the full range of options available to them, potentially decreasing the stress felt by them and PwD when relatives’ strategies fall short.
Further research is warranted in more diverse contexts as this study is limited to Israel. Another limitation is the social desirability bias as family caregivers may have positively tainted their responses to delusions. However, the family caregivers we interviewed were the main caregivers for the PwD in our study and there was no objective informant observing their reactions.
Future work can use our findings to expand the range of interventions to be examined quantitatively, to systematically examine the utilization of multiple interventions, and the perception of efficacy of single and co-occurring interventions. Another limitation is the preliminary way of classifying the responses/interventions and the need to add dimensions to these characterizations, including caregivers’ mood, and tone in addition to behavior during the intervention. Future studies also need to quantify the impact of interventions on calming the PwD and stopping the manifestation of the “delusion” as well as their impact on the caregiver’s calmness and acceptance of the manifestations.
Nevertheless, this is the first study to examine caregivers’ nonpharmacological interventions for delusions in a sample of community-dwelling PwD. It expands the range of potential interventions, clarifies their relationship with type of delusion, and provides preliminary information about their efficacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Israel Science Foundation grant 1067/07, by the Israel Ministry of Health, Grant 3000004003, and by the Minerva Foundation, Grant number 31583295000.