
Abstract
Objective
Mirrored self-misidentification syndrome (MSMS) is a rare form of delusional misidentification syndrome characterized by the inability to recognize one’s own reflection. We conducted a systematic review aiming to describe the epidemiology, clinical presentation, and management of individuals with MSMS.
Methods
A comprehensive literature search was performed using original case reports/series on patients with MSMS. Univariate analyses were performed to assess patient demographics, clinical, paraclinical, and treatment-related characteristics. The methodological quality of included articles was evaluated using a standardized tool.
Results
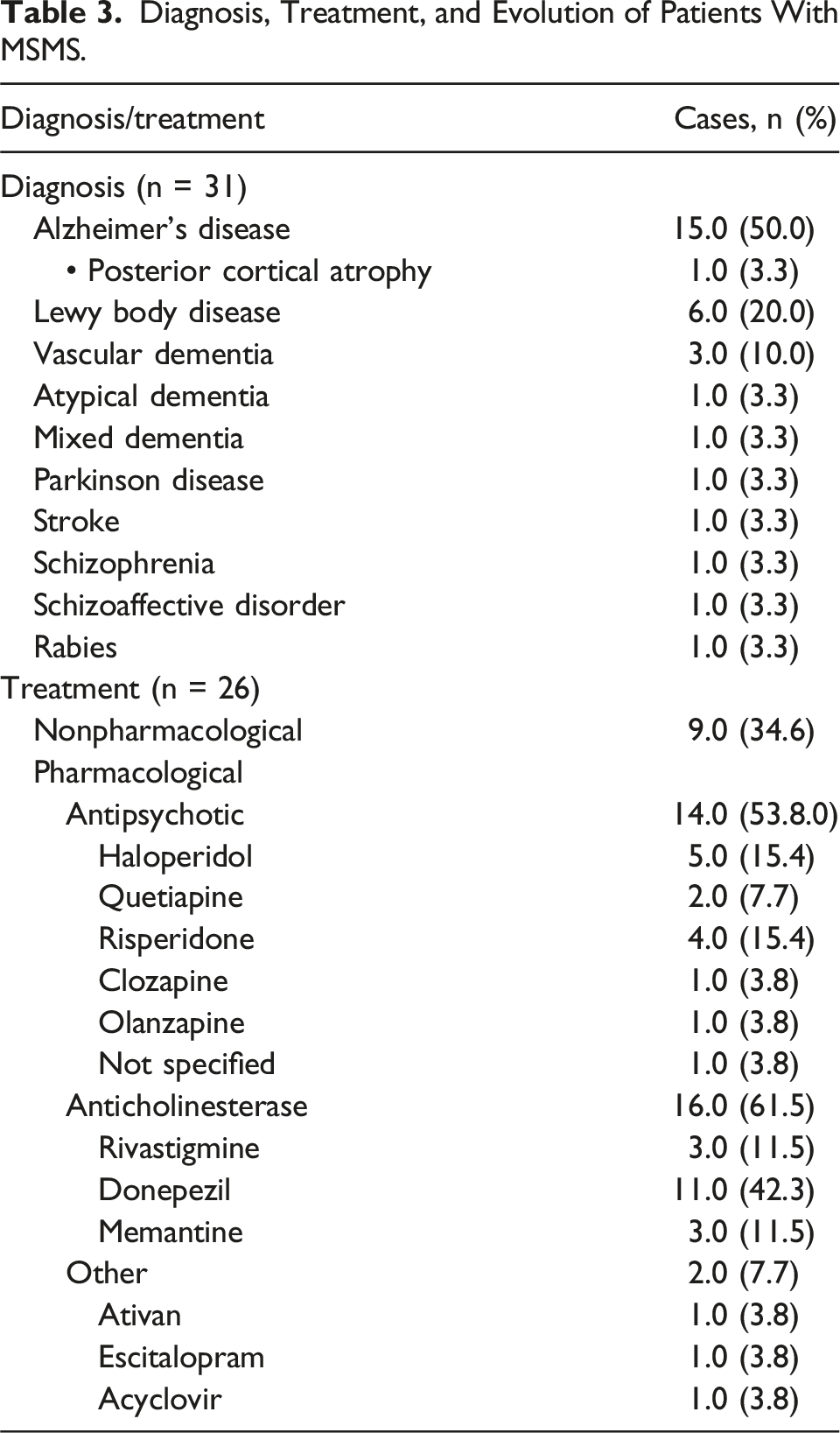
Of 76 articles screened, 28 were included, with 36 patients analyzed. Median age was 77.0 (interquartile range: 72.0, 80.0) years; most patients were female (60.7%). Over half of the cases had a diagnosis of dementia, mostly Alzheimer’s disease (50.0%), Lewy Body Disease (20.0%), and vascular dementia (10.0%), while the other diagnosis included stroke (3.3%), schizophrenia (3.3%), schizoaffective disorder (3.3%), and rabies (3.3%). Initial clinical manifestations included psychiatric symptoms (66.7%) and cognitive decline (70.0%). Brain magnetic resonance (MRI) was reported in 31 cases, with 14 cases (45.1%) showing right hemisphere dysfunction. Pharmacological interventions were effective for twelve cases (48.0%), and non-pharmacological interventions such as covering mirror were effective for 8 cases (32.0%). Most included articles (64.3%) were evaluated to be at low risk of bias.
Conclusions
MSMS are rare conditions that mostly present in patients with dementia. Despite the varied clinical presentations, frontal and right hemisphere dysfunctions appear to play a role in the pathophysiology of MSMS, adding to the evidence supporting “a neuroanatomy of the self” in the non-dominant hemisphere.
Introduction
Mirrored self-misidentification syndrome (MSMS) is a form of delusional misidentification syndrome (DMS). In this group of delusions, an individual forms a false belief about the identity of a person, place, or object. 1 In MSMS, the individual misidentifies their own reflection; they do not recognize themselves in the mirror and instead identifies their reflection as a separate individual. 1 MSMS is sometimes referred to as the mirror sign.2,3 MSMS has been proposed to be a form of Capgras syndrome, another DMS.4,5 In Capgras syndrome, the affected individual believes someone they know has been replaced by an identical impostor. 4 MSMS has thus been conceptualized by some experts as a Capgras syndrome exclusively directed at an individual’s own mirror image.1,5 MSMS has also been described as part of various mirror phenomena, such as mirror agnosia. In MSMS, the affected individual retains an intact understanding of mirror function and can correctly identify others’ reflections as mirror images. However, they specifically fail to recognize their own reflection, perceiving it as a distinct individual. In contrast, individuals with mirror agnosia do not recognize any reflection neither their own nor others’ as a mirror image, and they may attempt to physically interact with it as if it was real. 6
MSMS has been observed in individuals with a number of conditions, such as Alzheimer’s disease, Lewy body dementia, 7 Parkinson’s disease, 8 and schizophrenia. 9 While the exact mechanisms behind this syndrome remain unknown, some researchers have suggested an association between MSMS and facial processing deficits. 10 Others have found a relation between MSMS and right hemisphere dysfunction, 1 likely involving right prefrontal11,12 and right frontoparietal cortex12,13 which are the major areas driving self-recognition networks. While MSMS has been reported in dementia patients, its underlying mechanisms, remain poorly understood. The existing literature is mostly composed of isolated case reports and small case series. Previous systematic reviews have examined MSMS, our study aimed incorporates a larger dataset identifying additional cases that were not included in prior analyses. 1 In this study, we aimed to summarize the epidemiology, clinical presentation, and management of MSMS by conducting a systematic review of case reports and series.
Methods
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 14 The protocol for this review was registered on PROSPERO (CRD42022328086).
Search Strategy
A comprehensive literature search was conducted using the PubMed, MEDLINE, OVID Embase, OVID APA PsycINFO, Web of Science, and Google Scholar databases to identify relevant case reports and series of patients with MSMS. We used the truncated versions of the terms mirror, misidentification, agnosia, and delusion in our search strategy (see Supplemental Table 1 for the full strategy). No restrictions were imposed on language or publication date. We searched the reference lists of studies which passed the selection phase for additional articles of interest. We also searched the following sources of grey literature: the Metalib U.S. Government Publishing Office and the New York Academy’s Grey Literature Report. The search was first conducted in June-July 2022 and updated in June 2024.
Study Selection
Data selection was performed using Covidence. We sought to include case reports or series describing individuals with MSMS. Non-original research, research only implicating animals, and research only describing other forms of mirror phenomena (eg, mirror agnosia) were excluded. In June-July 2022, two reviewers (NR and AK) independently screened all the titles and abstracts for case reports/series on MSMS. The full-length articles were then screened by these 2 reviewers for final eligibility. The same procedure was repeated in June 2024 by 2 reviewers (EP and LPC) on research published from 2022 onwards. Any disagreements between the reviewers were resolved through discussion, with third party (JL) involvement if necessary.
Data Extraction and Analysis
Data from the first search in 2022 were independently extracted by 2 reviewers (AH and NR) to a structured Excel spreadsheet. The data from the 2024 search were extracted in the same manner by 2 reviewers (EP and LPC). Article-related data included the following: title of the study, authors, publication journals, and publication dates. Patient-related data included demographic information (age and sex), past medical history, clinical presentation, physical exam, paraclinical findings (including imaging), treatments used, and clinical evolution. During the data extraction, any duplicate articles were automatically removed by Covidence. Additionally, the 2 reviewers manually reviewed the data to eliminate any remaining duplicates. To ensure that no patients were doubly included, especially in cases where single case reports might overlap with case series, the 2 reviewers verified that no patients shared the same age or other distinguishing characteristics. All statistical analyses were performed using R version 4.3.0. 15 Univariate analyses were performed to assess relevant data. Results are presented using medians (interquartile ranges) for continuous variables and count (frequency) for proportion. Missing data were handled using pairwise deletion.
Quality Assessment
Once the studies met the inclusion criteria, a quality assessment was conducted according to the criteria suggested by Murad et al, based on the Bradford Hill criteria and the Newcastle Ottawa scale. 16 This tool, specifically designed for case reports and series, includes 8 items divided into 4 domains: selection, ascertainment, causality, and reporting. The fifth and sixth items, related to drug effects, were not used in our study. Our adapted scoring system included the following 6 questions: (1) does the patient represent the whole experience of the investigator, (2) was the MSMS adequately ascertained, (3) were the “outcomes” (eg, clinical presentation, treatments used, and clinical evolution) adequately ascertained, (4) were other alternative causes that may explain the clinical observations ruled out, (5) was follow-up long enough for “outcomes” to be measured, and (6) is the case of MSMS described with sufficient details to allow other investigators to replicate the research? Each question receiving an answer of “yes” was attributed a point, with a maximum of 6 points per article. Studies scoring 4 or more points were considered high quality with a low risk of bias, while those scoring 2 to 3 points were classified as having an intermediate risk of bias. Studies scoring below 2 points were deemed to have a high risk of bias. One author (AH) independently assessed the validity and risk of bias of the included studies using this tool, while another author (JL) reviewed the assessments.
Results
A total of 28 studies describing 36 cases were included in our systematic review.1,3,4,6,8-10,17-37 Figure 1 provides a detailed PRISMA flow diagram of the selection process. Study selection flow chart. MSMS = Mirrored self-misidentification syndrome.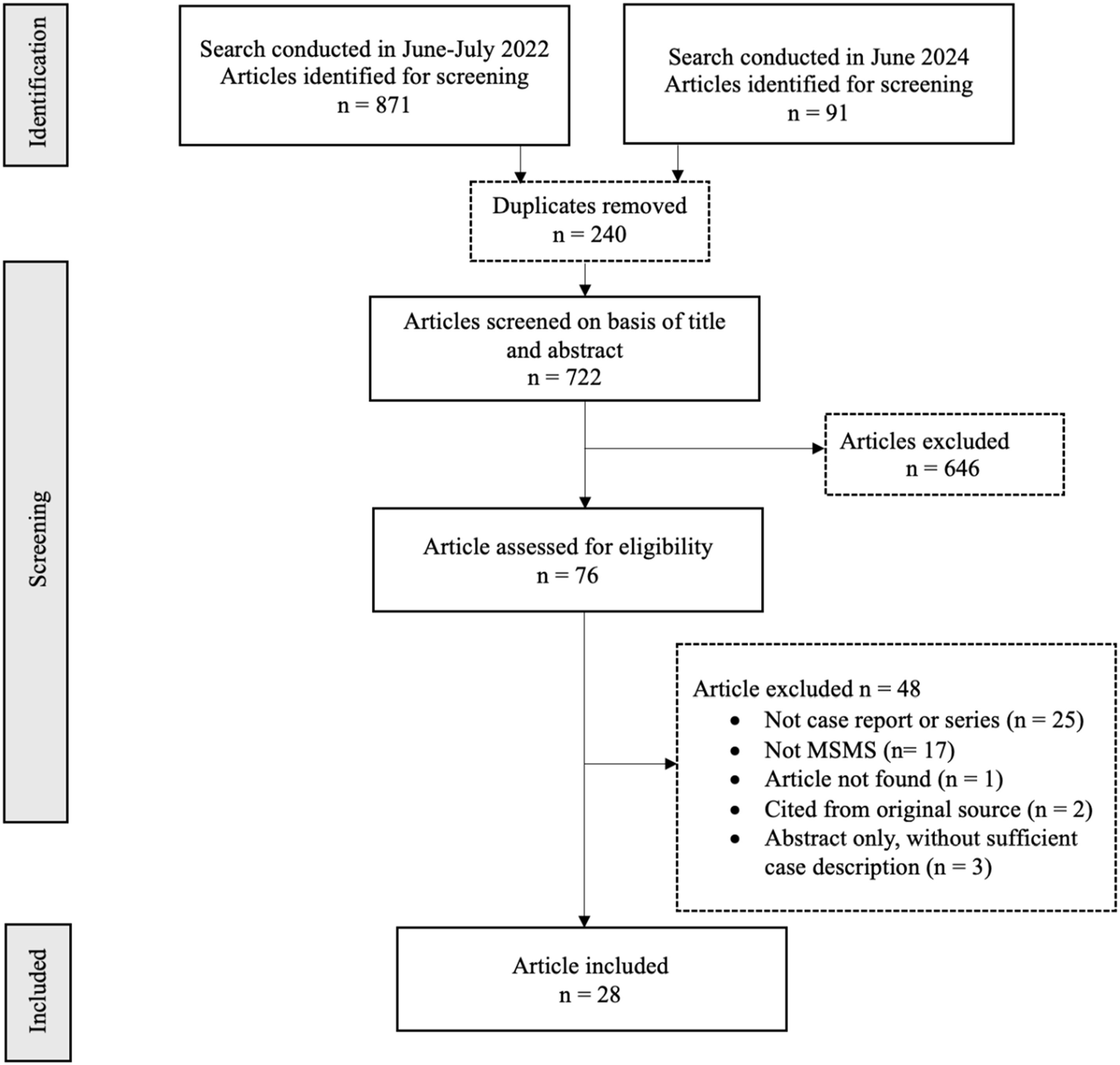
Patient Characteristics
Median age was 77.0 (72.0, 80.0) years, with 21 patients (60.7%) being of female sex. Past medical history was reported in 31 patients; relevant past pathologies are listed in Figure 2. The most prevalent past pathologies included hypertension in 11 cases (35.5%), dyslipidemia in 4 cases (12.9%), cardiac conditions in 5 cases (16.1%), and cancer in 4 cases (12.9%). Diabetes was reported in 5 cases (16.1%), and 3 patients (9.7%) had a history of traumatic brain injury. Additionally, 5 patients (16.1%) had previous neurological conditions: 2 patients had a temporo-parietal ischemic stroke (6.5%), 1 had a transient ischemic attack (3.2%), 1 had epilepsy (3.2%), and another had meningitis (3.2%). Past pathologies in patients with MSMS. COPD = Chronic obstructive pulmonary disease; MSMS = mirror self-misidentification.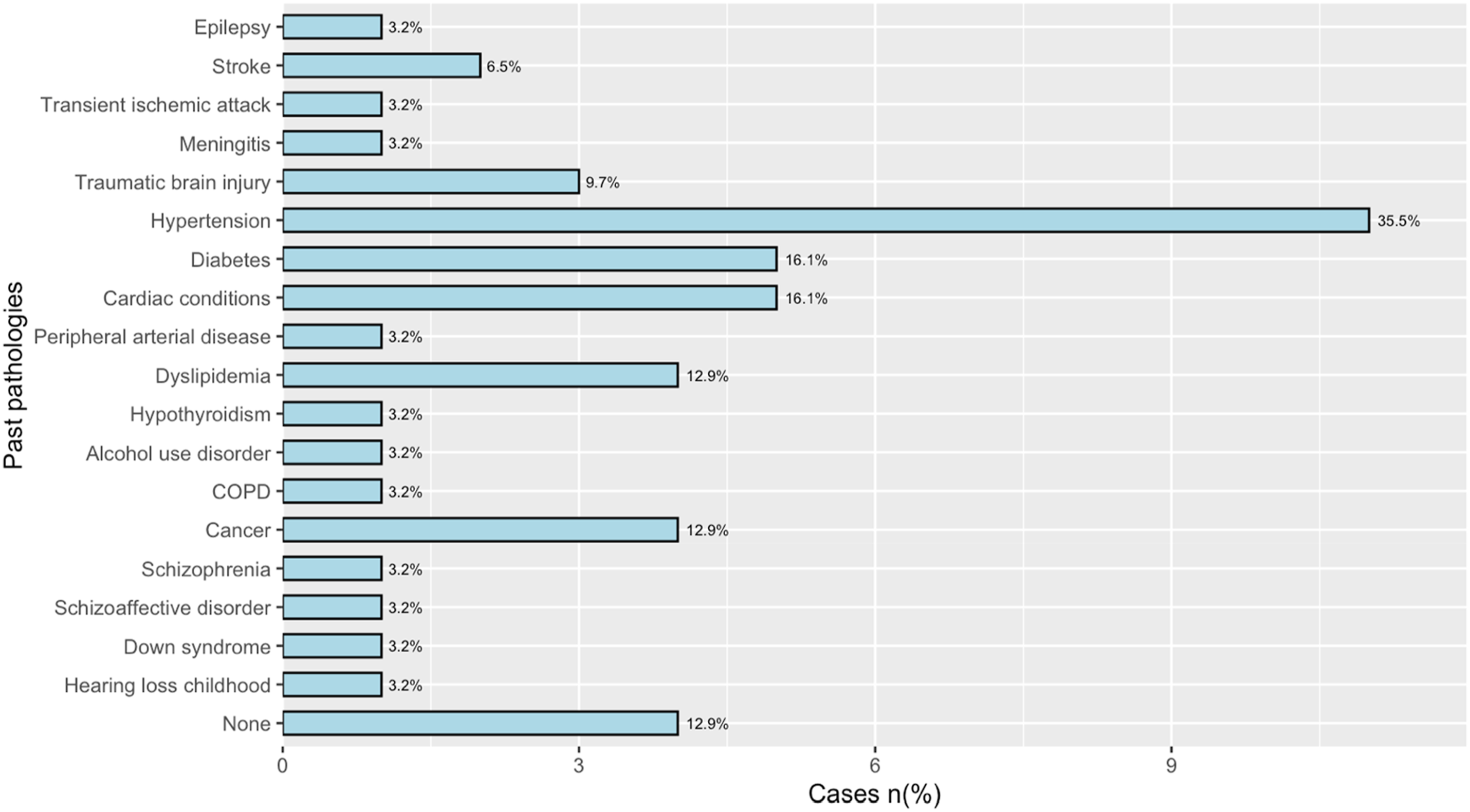
Clinical Presentation
Clinical Manifestations of Patients With MSMS.
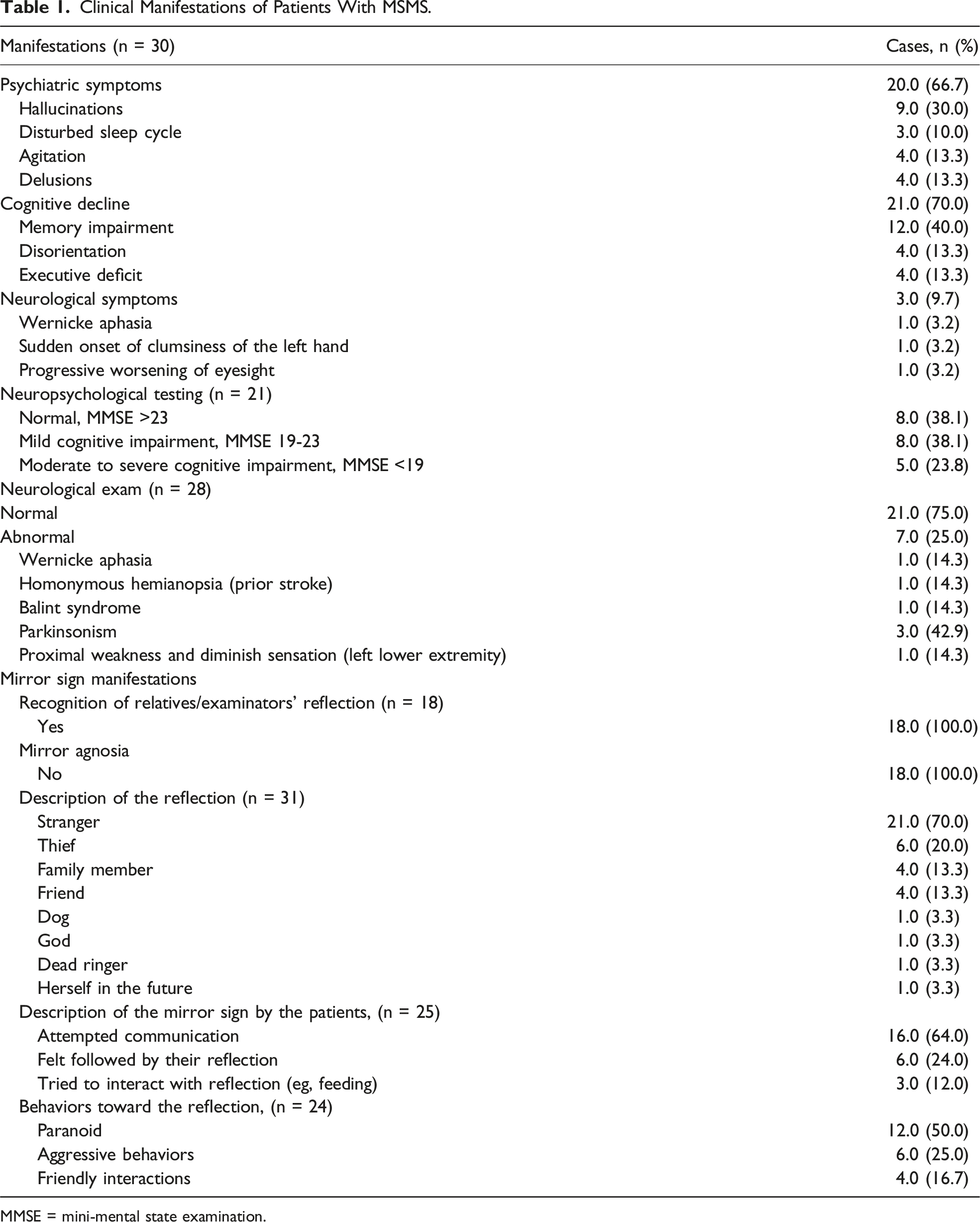
MMSE = mini-mental state examination.
Mirror Sign
Detailed descriptions of MSMS were provided for 30 cases. The manifestation of MSMS varied among patients, with 21 patients (70.0%) perceiving their reflection as a stranger. Among these patients, 6 (20.0%) perceived their reflection as a thief. Four patients (13.3%) mistook their reflection for a family member, 4 (13.3 %) as a friend, 1 (3.3%) as her future self, 1 (3.3%) as God, and another (3.3%) as a dog, as shown in Table 1.
Interaction with the mirror was reported in 24 cases. Among these, 6 patients (20.0%) described their reflection as following them everywhere and 16 (66.7%) attempted to communicate with their reflection, with 3 (10.0%) finding it disturbing that the reflection did not respond and another 3 (10.0%) trying to bring food to their reflection. Patients with MSMS presented various behaviors, of which detailed descriptions were provided for 24 cases. While 2 patients were undisturbed (8.3%) by their reflection, twelve cases (50.0%) exhibited paranoid responses and 6 (25.0%) displayed aggressive behaviors. Otherwise, 4 patients (16.7%) maintained a friendly relationship with their reflection. Among 18 cases with available data, semantic knowledge of mirrors was intact for all 18 patients (100.0%), who could define what a mirror and a reflection were, and all the 18 patients (100.0%) were able to recognize their relatives’ reflection.
Paraclinical Findings
Paraclinical Findings of Patients With MSMS.
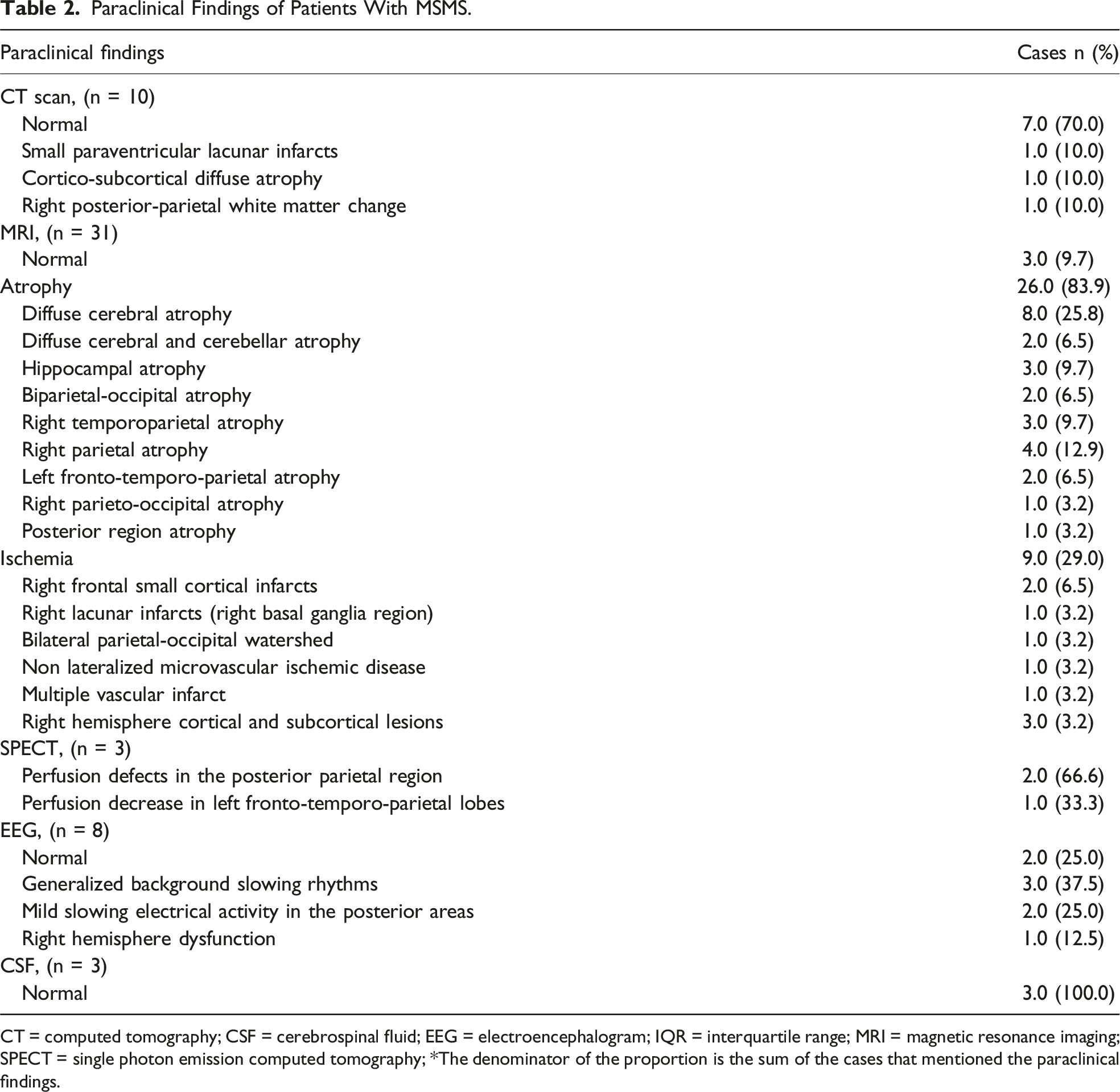
CT = computed tomography; CSF = cerebrospinal fluid; EEG = electroencephalogram; IQR = interquartile range; MRI = magnetic resonance imaging; SPECT = single photon emission computed tomography; *The denominator of the proportion is the sum of the cases that mentioned the paraclinical findings.
Diagnosis and Treatment
Diagnosis, Treatment, and Evolution of Patients With MSMS.
Clinical Evolution
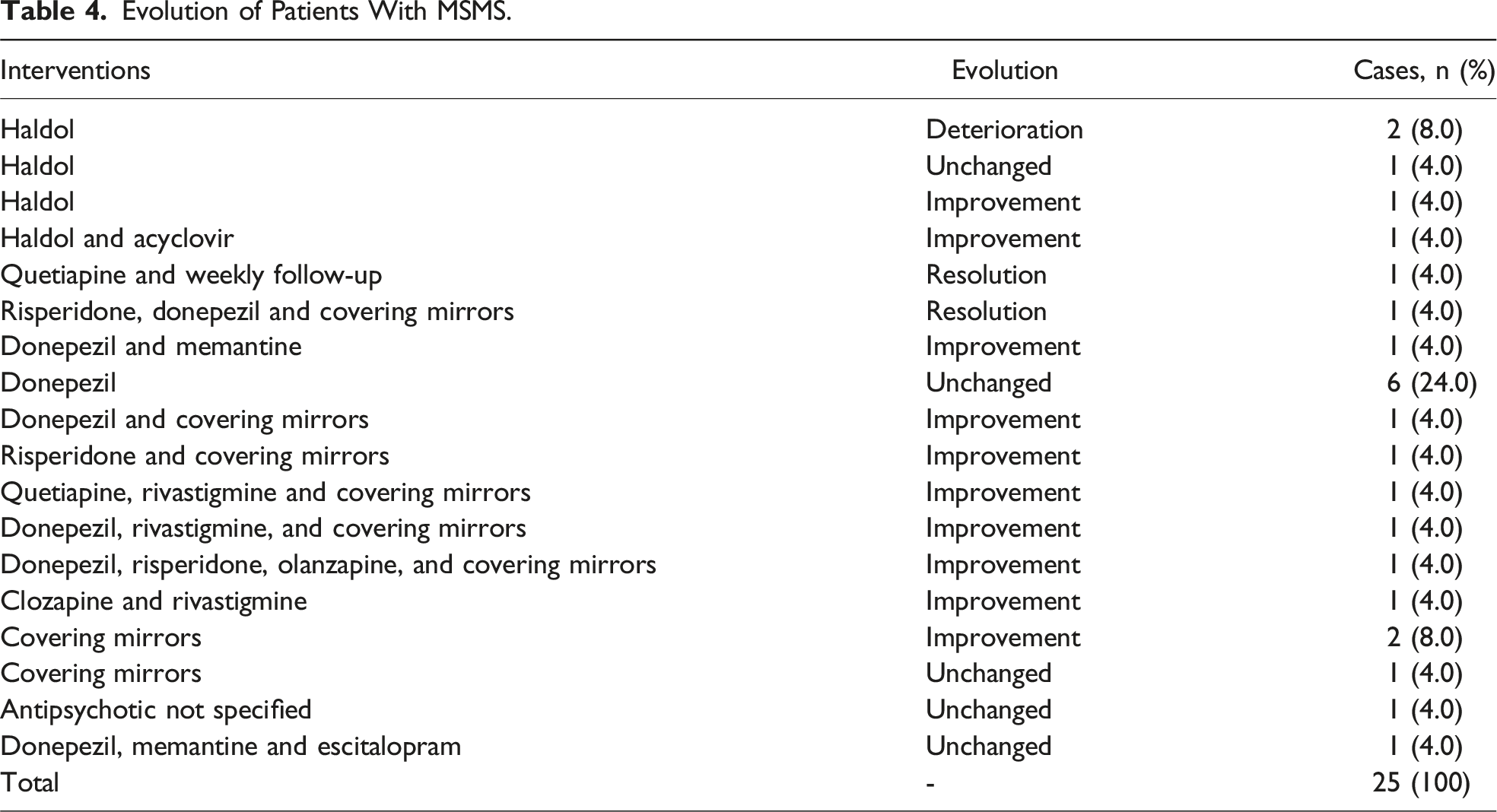
Evolution of Patients With MSMS.
Study Quality Assessment
Among the 28 articles, 18 studies (64.3%) were assessed to be at low risk of bias, scoring 4 or higher using Murad’s tool. 16 Ten articles (35.7%) were evaluated to be at moderate risk of bias.
Discussion
We conducted a systematic review investigating the reported clinical data of 36 cases with MSMS with the goal of describing the epidemiology, the clinical presentation, and the management of this syndrome.
MSMS are often described as rare conditions, however previous studies, have shown rates of 2%–10% in people with dementia, this rarity appears to be more related to the limited number of documented cases in the literature. While early studies have proposed that DMS occur exclusively in people of female sex, it has now been established that men can also be affected. 38 In our review, we found that MSMS is most frequently described in elderly women with a past medical history of cardiovascular risk factors. At presentation, most patients had psychiatric and cognitive symptoms, such as memory impairment, disorientation, and executive deficits. Notably, over half of the patients included in this review had evidence of dementia, mostly Alzheimer’s disease, followed by Lewy body dementia, and vascular dementia. The other diagnosis included 1 case of stroke 1 case of schizophrenia, 1 case of schizoaffective disorder, and 1 case of rabies. MSMS appears associated with neurodegenerative processes. In a retrospective study of 400 patients conducted by Nagahama et al, MSMS was identified in 3.0% of cases with Alzheimer’s disease, and 4.5% of cases with Lewy body dementia. 7 These findings align with the observations of Connors & Coltheart, who described different levels of mirror-use impairment in dementia patients. Their review highlighted that individuals with severe dementia are the most likely to develop MSMS, often perceiving their reflection as that of a stranger. In contrast, patients with moderate dementia exhibited mirror agnosia, while those with mild dementia struggled to correctly identify parts of their body in the mirror. 39 While DMS typically manifest in later stages of dementia, they can also appear early in patients with Alzheimer’s disease. 40 Among the cases in our study, we noted that 6/25 patients (24%) and 10/25 (40%) had normal or mildly impaired cognitive performance respectively. Other authors have proposed that MSMS may serve as an indicator of rapid cognitive decline, highlighting the need for greater attention to MSMS in dementia patients. 3
The manifestations of MSMS can vary. Patients in this review mostly misidentified their reflection as strangers or thieves, but sometimes also as family members or even entities such as a dog or God. Individuals with MSMS maintain firm delusional beliefs regarding their reflection.10,31 These beliefs imply that MSMS involves complex perceptual and cognitive dysfunctions. Several mechanisms have been proposed to explain MSMS. One prominent theory revolves around right hemisphere dysfunction and frontal damage, leading to perceptual abnormalities, loss of familiarity, and loss of judgment with the inability to correct wrong beliefs.1,19,20,22,41,42 In his research, Dr Todd E. Feinberg has proposed that DMS, including MSMS, are a component of the “neuropathologies of the self,” disorders of the self that affect aspects of the identity, including perturbations of the bodily, relational, and narrative self. Dr Feinberg has proposed that right brain dysfunction, especially medial-frontal and orbitofrontal lesions, causes a disturbance of ego boundaries and functions, leading to the emergence of immature psychological defenses, including denial, projection, splitting, fantasies, and paranoia.5,42 There are also dramatic changes in fundamental aspects of personality in the non-dominant variant of FTD, supporting the concept of a “neuro-anatomy of the self”. 43 Interestingly, more than half of the patients in our review had abnormalities in the right hemisphere area, due to ischemia or atrophy. In a study evaluating areas activated during patients’ recognition of their own faces, investigators found activation in the right occipito-temporo-parietal junction, in the frontal operculum, and in the left fusiform gyrus. 44 These authors hypothesized that in dementia, there is an early breakdown of these neural circuits. 30 In our review, we identified 4 patients with MSMS without dementia; 1 had a history of acute stroke, 1 had schizophrenia, 1 had schizoaffective disorder, and another had rabies. Thus, MSMS may not be exclusive to neurodegenerative disorders but may also be associated with other neurological and psychiatric conditions.
In this review, we found that paranoid and aggressive behaviors were common features of MSMS. Instances of these responses included patients fighting with their reflection, breaking mirrors, or calling the police, mistaking their reflection to be a thief stealing their jewelry. In 1 dramatic case, a patient attempted to jump out of a window to attack the misidentified stranger. 3 Paranoid behaviors are often associated with Capgras syndrome, a DMS in which individuals believe that familiar people have been replaced by body doubles. 45 There have even been multiple reported cases of patients with Capgras syndrome displaying homicidal behaviors.46,47 Interestingly, MSMS has been hypothesized to be as a form of Capgras syndrome confined to the mirror image. 4 While MSMS is often confused with prosopagnosia and mirror agnosia, all patients in our review could recognize their relatives’ reflections, and their semantic understanding of mirrors remained intact in all cases.
The management of MSMS is challenging. While most patients in our review showed improvement with some even experiencing complete resolution, others deteriorated, resulting in complete dependency and necessitating maximal assistance with daily activities. As MSMS is frequently due to dementia, and dementia is a progressive condition with no curative treatment, deterioration is not unexpected. Non-pharmacological approaches have shown promise in managing MSMS. Interventions such as modifying the patient’s environment by removing or covering the mirrors are useful.25,26 Although data on pharmacological treatment for MSMS are limited, anticholinesterase treatments have demonstrated effectiveness in some cases.17,25 Published studies highlight the limitations of antipsychotics in treating MSMS, only recommending their use when behavioural response is not achieved with anticholinesterase treatments. 26
Our study presents several limitations. First, because MSMS is rarely documented in the literature, our systematic review included only a limited sample of case reports and case series, making it difficult to draw definitive conclusions. Second, publication bias was likely, as with most systematic reviews of case reports and series. Cases that are more interesting, dramatic, or unusual are more likely to be published, while less impressive cases remain unpublished. MSMS is probably underdiagnosed, and many cases might be harmless and resolve on their own, but these less significant cases are often not described in the literature. Thus, our findings may overrepresent severe or atypical cases. Third, the variability in the methodological quality of the included studies adds a layer of complexity to the interpretation of our results. One-third of the studies present a moderate risk of bias due to missing information on long-term outcomes, imaging, and neuropsychological testing. We could only interpret studies with available data, making it difficult to compare patients from different studies accurately, limiting our understanding of MSMS.
Conclusion
This systematic review provides a comprehensive description of the clinical and paraclinical features of patients with MSMS. MSMS are rarely documented in the literature that mostly present in patients with dementia, exhibiting a variety of manifestations, with some patients misidentifying their reflection as a stranger, a thief, or even God, leading to paranoid and aggressive behaviors. Despite the varied clinical presentations, right hemisphere and frontal dysfunction appear to have central roles in the pathophysiology of MSMS. While non-pharmacological interventions have shown promise in managing symptoms, there is limited evidence supporting the effectiveness of pharmacological treatments, including agents with anticholinesterase properties. While MSMS is rarely documented in the literature, prevalence studies suggest that it may be more common than previously thought, particularly among patients with neurodegenerative diseases. Further research with a larger sample size is necessary to enhance our understanding of MSMS and its underlying mechanisms.
Supplemental Material
Supplemental Material - Mirrored Self-Misidentification Syndrome: A Systematic Review of Cases
Supplemental Material for Mirrored Self-Misidentification Syndrome: A Systematic Review of Cases by Amal Hagouch, Natacha Rouillon, Aysha Kabbadj, Léa Proulx-Chartier, Ève Parenteau, Jimmy Li, Christian Bocti, and Dènahin Hinnoutondji Toffa in Journal of Geriatric Psychiatry and Neurology
Footnotes
Author Contributions
AH: Data extraction, data analysis, manuscript writing, corresponding author. NR: Screening, data extraction, manuscript writing. AK: Screening, data extraction, manuscript writing. JL: Study conceptualization, data analysis, drafting, manuscript revision. CB: Manuscript revision. DHT: Study conceptualization, manuscript revision, principal investigator.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AH, NR, AK, LPC, EP, and DHT have nothing to disclose. JL is supported by the Fonds de recherche du Québec – Santé. CB holds equity in Imeka.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.