
Abstract
Personality traits have been reported to predict difficulties in performing instrumental activities of daily living (IADL) in old age, such as preparing meals or shopping. However, little is known about the reciprocal effects on personality. In this study, we examined bidirectional relationships between personality traits and the capacity to perform IADL using four waves of longitudinal data from 3540 older adults (aged 65 years and older) from the Health and Retirement Study. We applied a random-intercept cross-lagged panel model to separate between- and within-person effects across time and compared it to a traditional cross-lagged panel model. At the between-person level, higher neuroticism and lower conscientiousness were associated with more IADL limitations. Within individuals across time, increases in neuroticism and decreases in conscientiousness and extraversion were associated with increases in IADL limitations 4 years later. In contrast, increases in IADL limitations only predicted increases in neuroticism and decreases in extraversion. These results indicate that some personality traits affect and are affected by limitations in functional capacities in old age. Results of the within-person model build a strong foundation for future personality interventions as a pathway to maintain high functioning in old age.
Keywords
In an ageing society, promoting older adults’ functional capacities and independence becomes a societal priority: Independent older adults have higher quality of life and require less complex care (Connolly et al., 2017; Lafortune et al., 2009). Older adults represent a heterogeneous group (Lowsky et al., 2014) in the sense that they differ in the extent to which they maintain their functional independence and capacity to perform daily activities of living (e.g. preparing food and going grocery shopping). Understanding these individual differences in functional capacities, their predcitors and their development over time, is crucial for creating a realistic picture to guide personalized preventive health care policies and clinical interventions (Santoni et al., 2015). One predictor that could account for these individual differences is personality (Hill & Allemand, 2020). Given that the construct of personality is in itself subject to developmental lifespan changes, it should be explored as both an antecedent and as a consequence for functional capacities (Mueller et al., 2017; Murray & Booth, 2015). Building and extending on previous research, this study aims to investigate the reciprocal associations between functional capacities and personality traits (i.e. neuroticism, conscientiousness, extraversion, agreeableness and openness) in older adults. As the goal of psychological research is also to prepare the ground for personalized clinical interventions (Allemand & Flückiger, 2017), the association between personality and functional capacities is investigated using both a between-person approach (i.e. studying the association of the variables across persons) and within-person approach (i.e. studying intra-individual association of the variables across measurement occasions).
Functional capacities in old age
Development takes place across the entire lifespan, from conception to death (Baltes, 1987). Old age, referring to the later period in the adult lifespan (i.e. 65 years of age and older), is most often characterized by some challenges impacting everyday functioning, such as general decline in sensory and sensorimotor capacities (e.g. decreasing vision and hearing), and higher incidence of chronic diseases (e.g. diabetes and hypertension) and dementia (Lindenberger & Baltes, 1997; Marengoni et al., 2011; Niccoli & Partridge, 2012). In this study, we focus specifically on age-related decline in functional capacities. Functional capacities, or one’s ability to independently carry out daily activities (Carmona-Torres et al., 2019) can be divided into basic activities of daily living (BADL) and instrumental activities of daily living (IADL). BADL are the most basic activities of independent living, such as bathing, walking or dressing, while IADL describe more complex tasks, including housekeeping, shopping, transportation, preparing meals, managing money, taking medication and doing laundry. Compared to BADL, which portray more severe physical disabilities, IADL require better cognitive functioning and higher personal autonomy, thus representing indices for both physical and cognitive health (Jekel et al., 2015; Millán-Calenti et al., 2010). Limitations in IADL capacities usually occur earlier and are more frequent than impairments in BADL (Judge et al., 1996), and are therefore of interest for clinical interventions aimed at preventing more severe BADL shortfalls in older adults (Orellano et al., 2012). In Europe, reports show that on average, 8.4% of the adults older than 65 years of age report at least one BADL limitation, while 25.2% report at least one IADL limitation (Gaertner et al., 2019). Thus, given the higher prevalence of IADL limitations in older adults, and high relevance for clinical practice (Orellano et al., 2012), this study focused only on IADL in relation to personality traits.
Personality and trajectory of personality change in old age
Personality traits have emerged as reliable predictors of different life outcomes, including health and life expectancy (Canada et al., 2021; Hampson & Friedman, 2008), with the magnitude of the effects being comparable to other well-known predictors of health (e.g. intelligence; Roberts et al., 2007). Of the Big Five (Goldberg, 1990), two trait domains, namely, neuroticism (i.e. tendency to experience frequent negative emotions) and conscientiousness (i.e. tendency to be responsible and capable of self-control) have most consistently shown associations with health-related measures (Murray & Booth, 2015). Extraversion (i.e. tendency to be outgoing and sociable), agreeableness (i.e. tendency to show friendliness) and openness (i.e. tendency to express curiosity) have produced more mixed findings in relation to health (Krueger et al., 2006; Murray & Booth, 2015; Wettstein et al., 2017).
Despite their relative stability, personality traits do change across the entire lifespan, from young adulthood to old age (Lucas & Donnellan, 2011). Compared to other age ranges, personality changes in old age are much less studied. The studies on personality change in old age suggest a decrease in rank-order stability (e.g. Lucas & Donnellan, 2011; Seifert et al., 2021; Specht et al., 2011) and mean-level increases in neuroticism (Graham et al., 2020; Kandler et al., 2015; Mõttus et al., 2012; Wortman et al., 2012) and decreases in extraversion, conscientiousness and openness (Allemand et al., 2007; Graham et al., 2020; Kandler et al., 2015; Lucas & Donnellan, 2011; Mõttus et al., 2012; Wortman et al., 2012). This suggests that after a phase of increasing personality stability and maturation during young and middle adulthood (e.g. Roberts et al., 2006; Roberts & DelVecchio, 2000), personality becomes more variable in old age and generally changes in the opposite direction.
Personality changes have been attributed to biological and psychosocial (context-related) processes (Bleidorn et al., 2020; Costa et al., 2019; McCrae et al., 2021). In old age, this refers to decline in health, sensory functioning and cognitive abilities, as well as losses of loved ones or social responsibilities (e.g. Mueller et al., 2017). More specifically, trait changes in older age might depict an adaptation to the declines and losses in old age as described in the model of selection, optimization and compensation (Baltes et al., 2007). Older adults disengage from goals that are no longer attainable, and adjust their daily experiences and behaviour to their physical condition (i.e. engagement in secondary control compensatory strategies; Heckhausen et al., 2010; Kandler et al., 2015; Wagner et al., 2016). For example, as illustrated by Mueller and colleagues (2017), increases in neuroticism could heighten older adults’ awareness of everyday dangers and prevent them from engaging in risky, or health damaging behaviours (e.g. carrying heavy objects). Thus, the above line of thought reveals that in addition to the predominant view of personality as antecedent of health and functional capacity (Murray & Booth, 2015), with increasing age, personality can also change as a consequence of declines in health (Jokela et al., 2014; Wagner et al., 2016). Thus, two perspectives on personality in relation to IADL emerge: Personality and personality change act (a) as a predictor or antecedent of experienced IADL limitations and (b) as a consequence of these limitations.
Personality and IADL in older adults
Personality as antecedent of IADL limitations
Several studies have shown that personality predicts inter-individual differences in health and functional capacities (e.g. IADL) in older adults (Canada et al., 2021; Murray & Booth, 2015; Suchy et al., 2010). Adler and Matthews (1994), and Smith (2006) provided initial conceptual models for the personality–health link, which have recently been integrated and extended by Turiano et al. (2021) in the Personality and Health Process model (PHP model). The PHP model acknowledges three mechanisms for the personality–health link: (1) physiological functioning, (2) health behaviours and (3) social relationships. Cross-sectional and longitudinal data support these notions, as conscientiousness, extraversion, agreeableness, openness and neuroticism are linked to distinct physiological profiles (e.g. cortisol reactivity, cardiovascular functioning; Luchetti et al., 2014; Sutin et al., 2010; Williams et al., 2009), participation in health-related behaviours (Canada et al., 2021), exposure to interpersonal stressors (Hill et al., 2014; Smith, 2006) or social support (see Turiano et al., 2021 for a review on these links). Furthermore, the direct association between personality and IADL has also been recently reported by Canada et al. (2021), Suchy et al. (2010) and Gogniat et al. (2020) showing that older adults with higher neuroticism and lower conscientiousness, extraversion, openness and agreeableness were more likely to report IADL limitations. The associations for conscientiousness and neuroticism were replicated across studies, whereas the effects were mixed for the other trait domains.
Personality change as a consequence of IADL limitations
The challenges characterizing old age, such as increasing IADL limitations, threaten individuals’ ability to maintain their previous acquired lifestyle and are therefore rightfully expected to affect their personality (Wagner et al., 2016). For example, one’s inability to perform IADL (such as shopping and handling money) and reduced independence might cause feelings of vulnerability and anxiety, favouring increases in neuroticism (Hayman et al., 2007; Mueller et al., 2017). Similarly, with decreases in physical health and increases in IADL limitations, it might be more difficult to maintain one’s previous levels of orderliness or discipline, resulting in decreases in conscientiousness (Chopik, 2016; Mõttus et al., 2012; Mueller et al., 2017). In line with notions of lifespan theory, this would mean that with increasing age and more pervasive health declines, the effectiveness of compensatory psychosocial resources for health is reduced (e.g. personality; Baltes et al., 2007; Löckenhoff et al., 2008; Mueller et al., 2018). Further applied to the current context, with increasing age, functional declines might be too strong to be compensated by psychosocial resources and might reduce personality stability (e.g. one has fewer opportunities to express behaviours related to conscientiousness). Past research has reported changes in personality traits in response to changes in health (e.g. Jokela et al., 2014; Kornadt et al., 2018; Stephan et al., 2016), thus supporting a predictive effect of health decline on personality change.
Evidence for a reciprocal link
Both, the PHP model (Turiano et al., 2021) and the framework of lifespan development (Mroczek et al., 2020), expect reciprocal associations for the health–personality traits link, which operate most likely through feedback loops and co-development. To illustrate, lower extraversion is considered to predict reduced health outcomes due to a lack of social support or involvement in social activities (Mund, et al., 2018; Turiano et al., 2021). In turn, reduced health, coupled with reduced social activity could lead to decreases in extraversion (Mueller et al., 2018). The reciprocal link for personality and health have been previously reported: Using a sample of older adults (aged 70 years and older), Mueller et al. (2018) reported reciprocal links between neuroticism, extraversion and performance-based measures of functionality (i.e. handgrip strength and visual acuity) and Wettstein et al., (2017) observed reciprocal links between neuroticism, agreeableness and IADL for sensory-impaired older adults (but not healthy adults), with the mentioned traits being the only ones assessed. Most recently, using multiple longitudinal studies combining younger samples (adults aged 15 and older), Luo et al. (2022) reported reciprocal links between neuroticism, extraversion, openness and conscientiousness and different indices of health (e.g. self-reported health and disease levels), but no effects for agreeableness.
Correlated change between personality and IADL limitations
In addition to personality affecting IADL limitations and vice versa, both can be simultaneously affected by change in a third variable, such as cognitive or physical decline. Previous studies have reported personality changes (e.g. increasing neuroticism, decreasing conscientiousness and decreasing extraversion) in response to increasing health problems (Kornadt et al., 2018), onset of chronic diseases (Jokela et al., 2014), decreasing physical functioning (i.e. performance-based measures of handgrip strength, visual acuity; Mueller et al., 2018) or frailty (Stephan et al., 2017) in older adults. Only a few studies have examined the effect of cognitive decline on personality change (e.g. Aschwanden et al., 2017; Wettstein et al., 2017), and found some significant correlated changes – although the majority of associations were insignificant. An age-related decline in health (e.g. onset of chronic diseases) and cognition might result in both an increase in IADL limitations and changes in personality, which can be identified as correlated change.
A distinction of between-person and within-person effects
There are two distinct levels of analysis for the personality-IADL association: the between-person and the within-person levels. With some exceptions (e.g. Mueller et al., 2018), the association between functional capacities and personality traits has predominately been examined at the between-person level. Between-person results indicate, for example, that compared to those less neurotic, more neurotic individuals are more likely to suffer from IADL limitations (Gogniat et al., 2020; Suchy et al., 2010). In contrast, a within-person analysis would denote that the association of the two constructs is evaluated with respect to how a person varies from his/her trait levels over time. It can show, for example, that intra-individual increases in neuroticism lead to increases in IADL limitations (Orth et al., 2021). The repeated assessment within individuals is also suited to investigate personality and IADL, which naturally show variations across time (Carmona-Torres et al., 2019; Lucas & Donnellan, 2011).
In addition, the design of interventions requires the study of within-person associations but is often based on the assumption that within-person relationships mirror the findings on between-person associations. This is not necessarily the case, as results do not always replicate (Keijsers, 2016; Kievit et al., 2013; Mueller et al., 2018; Voelkle et al., 2014). Knowing that more neurotic individuals are more likely to suffer from health limitations (compared to those less neurotic) could lead to planning interventions that focus on decreasing one’s neuroticism, without considering that this finding might not be supported on an intra-individual level (or without knowing that decreasing neuroticism over time would indeed lead to decreasing IADL limitations). As argued before (Hamaker et al., 2015; Mueller et al., 2018; Voelkle et al., 2014), if the aim of empirical findings is to create a foundation for clinical interventions, it should also be assessed if personality and health indices are related to each other in such a way that changes in one (e.g. increases in neuroticism) relate to changes in the other (e.g. increases in IADL limitations).
The limited research investigating the reciprocal links between personality and health in older adults have predominantly used the cross-lagged panel model as an analytical approach (e.g. Wettstein et al., 2017; 2018). This model represents one of the most frequently used analysis for investigating reciprocal associations within the field of psychology (Orth et al., 2021) and is a popular approach for studying reciprocal links between health and different forms of self-evaluations (e.g. loneliness, self-esteem; Cacioppo et al., 2010; Orth et al., 2016; Tsur et al., 2019). However, the traditional cross-lagged panel model was criticized for providing estimates with a mix of between-person and within-person variances (Hamaker et al., 2015; Mund & Nestler, 2019). The random-intercept cross-lagged panel model was proposed as an extension decomposing the variance in stable between-person associations and within-person dynamics (i.e. therefore allowing interpretation of reciprocal links as purely within-person; Hamaker et al., 2015). Still, the extent to which the mix of variance in the traditional cross-lagged model affects the interpretation of its estimates is still under debate (see Lüdtke & Robitzsch, 2021; Orth et al., 2021). As the traditional cross-lagged panel was previously used to investigate the reciprocal health–personality link in older adults (e.g. Wettstein et al., 2017; 2018), this research aimed to also compare the results of the cross-lagged model with its within-person extension (random-intercept cross-lagged model).
The present study
This study aims to investigate the reciprocal relationship between personality and IADL limitations using up to four waves of data, covering 12 years, from the Health and Retirement Study. The link between personality traits and IADL limitations was investigated both at within- and between-person levels, comparing the findings of the commonly used cross-lagged panel model (CLPM), to a random-intercept cross-lagged panel model (RI-CLPM; Hamaker et al., 2015). Based on existing literature investigating the link between personality and health or functional capacities (Canada et al., 2021; Gogniat et al., 2020; Luo et al., 2022; Mueller et al., 2018; Suchy et al., 2010), we expected the strongest cross-sectional and bidirectional associations between IADL and higher neuroticism (N), as well as lower conscientiousness (C), extraversion (E) and openness (O). In line with the existing literature, we did not expect to find associations for agreeableness (A). We focused on the following three research questions:
First, are personality traits and IADL limitations correlated in older adults? We expected that the personality traits are associated with IADL limitations in older adults, both in stable inter-individual differences (i.e. random-intercept correlations in the RI-CLPM), and with respect to change (i.e. correlated measurement occasion–specific residuals in the RI-CLPM).
Second, do personality traits predict more IADL limitations at a subsequent time point and vice versa (i.e. more IADL limitations predict changes in personality)? We expected that individuals with higher N and lower C, E and O (i.e. cross-lags in the CLPM) will show more IADL limitations at a subsequent time. Similarly, we expect individuals with more IADL limitations to show higher N and lower C, E and O at a subsequent time. We compared the effect sizes of these two pathways to compare the strength of these effects.
Third, do intra-individual changes in the personality traits lead to subsequent changes in IADL limitations, and vice versa (i.e. changes in IADL limitations predict changes in personality)? We expected that intra-individual increases in N and declines in C, E and O will predict increases in IADL limitations (i.e. cross-lags in the RI-CLPM), and in turn, increases in IADL limitations will predict subsequent increases in N and decreases in C, E and O. Again, we compared the strength of these effects.
Method
Sample
This project was based on data of the Health and Retirement Study (HRS; Juster & Suzman, 1995; Health and Retirement Study, (HRS core) public use dataset; 2006-2018), a national longitudinal ongoing panel study, initiated in 1992, that includes more than 37,000 American adults older than 51 years, followed up at 2-year intervals. Participants were interviewed in person or by telephone on major components of their lives (e.g. health, retirement and socioeconomic status), and their informed consent was obtained orally before each interview. New cohorts are added every 6 years. The HRS is sponsored by the National Institute on Aging (NIAU01AG009740) and conducted by the University of Michigan, with data publicly available at http://hrsonline.isr.umich.edu/.
Four waves of data were used for this study, from 2006, the first year personality traits were assessed, until 2018. As personality was assessed on only half of the sample at every 2 years, the same sample completed the personality assessment every 4 years. For this study data from 2006, 2010, 2014 and 2018 was analysed, as it allowed us to include four measurement waves of personality. The analysis was restricted to participants that were aged 65 years and older in 2006, or more specifically, participants who were born before 1941 if they joined at a later wave. We decided to restrict our sample to adults aged 65 years and above, given a higher prevalence of health limitations after this age (Okoro et al., 2018; Rönnlund et al., 2005). For this study, we only included participants with no missing data on the control variables (i.e. age, gender, education and at least one wave of cognition), at least two waves of self-reported data for each variable of interest (i.e. N, C, E, A, O and IADL limitations), and who were not already in nursing homes or disabled at their first assessment (i.e. still able and required to perform IADL in everyday life). These led to a total number of 3540 participants, 57% of them being female (age range 65–99, M = 73.25, SD = 6.31 years) and 86% participants reporting to be white/Caucasian. Participants reported to have on average 12.58 years of education (SD = 2.99). A flow diagram outlining the exclusion of participants can be found in the OSF supplement (Figure 1; https://osf.io/gj35x/). Out of the final sample, 661 adults had only two assessments and 1196 adults provided data for all four assessments.
Compared to those who provided only two assessments, participants that responded to all four assessments were younger (70.75 vs. 74.29 years; p < .001; d = −0.65), more educated (13.14 vs. 12.52 years; p < .001; d = 0.23), less neurotic (1.87 vs. 1.98; p < .001, d = −0.24), more conscientious (3.38 vs. 3.32; p < .001; d = 0.15), more agreeable (3.52 vs. 3.48; p = .020; d = 0.10), more extraverted (3.21 vs. 3.12; p < .001; d = 0.17), more open (2.91 vs. 2.80; p < .001; d = 0.22), reported fewer IADL limitations (0.04 vs. 0.08; p < .001; d = 0.45) and higher cognitive functioning at the first wave (1.87 vs. 1.24; p < .001; d = 1.64). Men had also more incomplete assessments than woman (5.76 for men vs. 5.44 for women; p = .04; d = 0.07). We used full information maximum likelihood (FIML) estimation in all models to account for missing data and included age, gender, education and (time-varying) cognition as covariates in our models to account for potential effects of these differences.
Measures
Instrumental activities of daily living (IADL)
Based on the Lawton IADL Scale (Lawton & Brody, 1969), IADL limitations were assessed using six items that required a yes/no response. Participants were asked whether they had ‘any difficulty’ with performing the following activities: grocery shopping, preparing meals, managing money, making phone calls, taking medication and using a map. Each item response was coded as 0 = no difficulty or 1 = any difficulty. For our analysis, we used the mean score of each participant at each measurement occasion, ranging from 0 to 1 (see Wahrendorf et al., 2013 for similar approach using HRS data). Composites score for IADL limitations was previously used in large scale research using the HRS data (Wahrendorf et al., 2013). Cronbach’s alpha coefficients for the measure ranged from .47 to .82 across the measurement occasions. However, these should be interpreted with caution, as IADL limitations reflect a formative construct (i.e. a composite of different limitations) rather than a reflective one (i.e. a latent disability factor), implying that items do not have to correlate (Stadler et al., 2021). For the same reason, longitudinal measurement invariance was not assessed for IADL limitations (see Analysis section).
Personality
Personality was assessed using the Midlife Development Inventory (MIDI; Lachman & Weaver, 1997). Participants were presented with a list of 26 items containing adjectives, to which they had to indicate how well each described them, on a scale from 1 (a lot) to 4 (not at all). Four items were used for assessing neuroticism (i.e. moody, worrying, nervous and calm), five to assess conscientiousness (i.e. organized, responsible, hardworking, careless and thorough), five for extraversion (i.e. outgoing, friendly, active, lively and talkative), five for agreeableness (i.e. helpful, warm, caring, softhearted, and sympathetic) and seven for openness (i.e. creative, imaginative, intelligent, curious, broad-minded, sophisticated and adventurous). Two items (i.e. calm and carless) were reverse-coded. Mean scores were calculated for all traits. Mean scores were reversed so that high scores indicate higher trait levels. Cronbach’s alpha values were rather low for neuroticism and conscientiousness ranging from 0.69 to 0.71 for neuroticism, from 0.52 to 0.59 for conscientiousness, from 0.74 to 0.76 for extraversion, from 0.77 to 0.79 for agreeableness and from 0.78 to 0.80 for openness. 1 Because the scales were rather short and included reverse-coded items, lower reliability coefficients were to be expected (Tavakol & Dennick, 2011).
Covariates
In addition to including age, gender and education as covariates in our analyses, we also used a time-varying measure for cognitive functioning, as this might influence personality as well as IADL limitations and their association. A composite (mean) score was created for each participant on objective measures of cognitive performance available for the study sample. This overall cognitive performance score was based on two tests for episodic memory (i.e. Immediate and Delayed word recall), counting backwards (i.e. Serial 7’s test), and the general mental status assessment comprising of date, object, president/vice president naming (general mental status adapted from Brandt et al., 1988 and Folstein et al., 1975). For a description of cognitive assessment in HRS, see Ofstedal et al., (2005). With the exception of gender, all covariates were z-standardized prior to inclusion in the model.
Analysis
All supplementary materials and analyses scripts used in this study are available in an OSF repository: https://osf.io/gj35x/. The analyses were not pre-registered. All analyses were performed using R and the R-packages psych v2.0.8 (Revelle, 2020) and lavaan v0.6-7 (Rosseel, 2012). All models were estimated using full information maximum likelihood (FIML) to account for missing data, and robust standard errors (1000-fold bootstrapping). As chi square is highly dependent on sample size (Bergh, 2015), model fit was assessed using three estimators: comparative fit index (CFI), root mean square error of approximation (RMSEA) and square root mean residual (SRMR). Values of CFI higher than .90 suggest acceptable fit and values higher than .95 show good fit. For RMSEA and SRMR, values lower than .08 suggest acceptable fit and values lower than .05 show good fit (Bentler, 1990; Bentler & Bonett, 1980; Byrne, 2013; Hu & Bentler, 1999).
Measurement invariance testing
We first tested for longitudinal measurement invariance across time for all five personality traits using a correlated factor model in which the personality trait factors loaded on all items at the corresponding measurement occasions and were allowed to correlate across time. The same items were also allowed to correlate across time by adding residual correlations. We evaluated measurement invariance by comparing model fit of four increasingly restrictive models: (1) a model without parameter constraints across time (i.e. configural invariance), (2) a model with equal factor loadings across time (i.e. metric invariance), (3) a model with additionally constrained item intercepts across time (i.e. scalar invariance) and 4) a model with additionally constrained residual variances across time (i.e. strict invariance). A decrease in the comparative fit index (CFI) between nested models beyond ΔCFI = −0.01 (Chen, 2007) would suggest that measurement invariance does not hold across time. For the current analysis of the covariance structure, metric invariance is sufficient.
Cross-lagged panel models
To investigate the between-person associations, as well as the dynamic relation between personality and IADL limitations, we used a cross-lagged panel model (CLPM, see Figure 1a) and a random intercept cross-lagged panel model (RI-CLPM, see Figure 1b; Mund & Nestler, 2019). We used the time-specific personality and IADL mean scores as indicators for the model. Models were estimated separately for each Big Five factor. For the CLPM, we specified autoregressive paths (i.e. path a/b: personality/IADL limitations predicted by the previous measurement occasions), cross-lagged paths (i.e. path c/d: personality/IADL limitations predicting IADL limitations/personality at a subsequent time point) and measurement occasion–specific correlations between the residuals of personality and IADL limitations (i.e. path e). Cross-Lagged Panel Model and the Random-Intercept Cross-Lagged Panel Model. Note: (a) represents the CLPM and (b) represents the RI-CLPM; P = personality traits (neuroticism, conscientiousness, extraversion, agreeableness and openness); IADL = instrumental activities of daily living; 06, 08, 10, 18 = assessment points (i.e. 2006, 2008, 2010 and 2018). Boxes represent scale scores at each measurement occasion and ellipses latent factors (i.e. the random intercept and measurement occasion-specific deviations). Parameter labels (a to e) indicate equality constraints across time. We controlled for age, education, gender and cognition (time-varying) in all models (not depicted).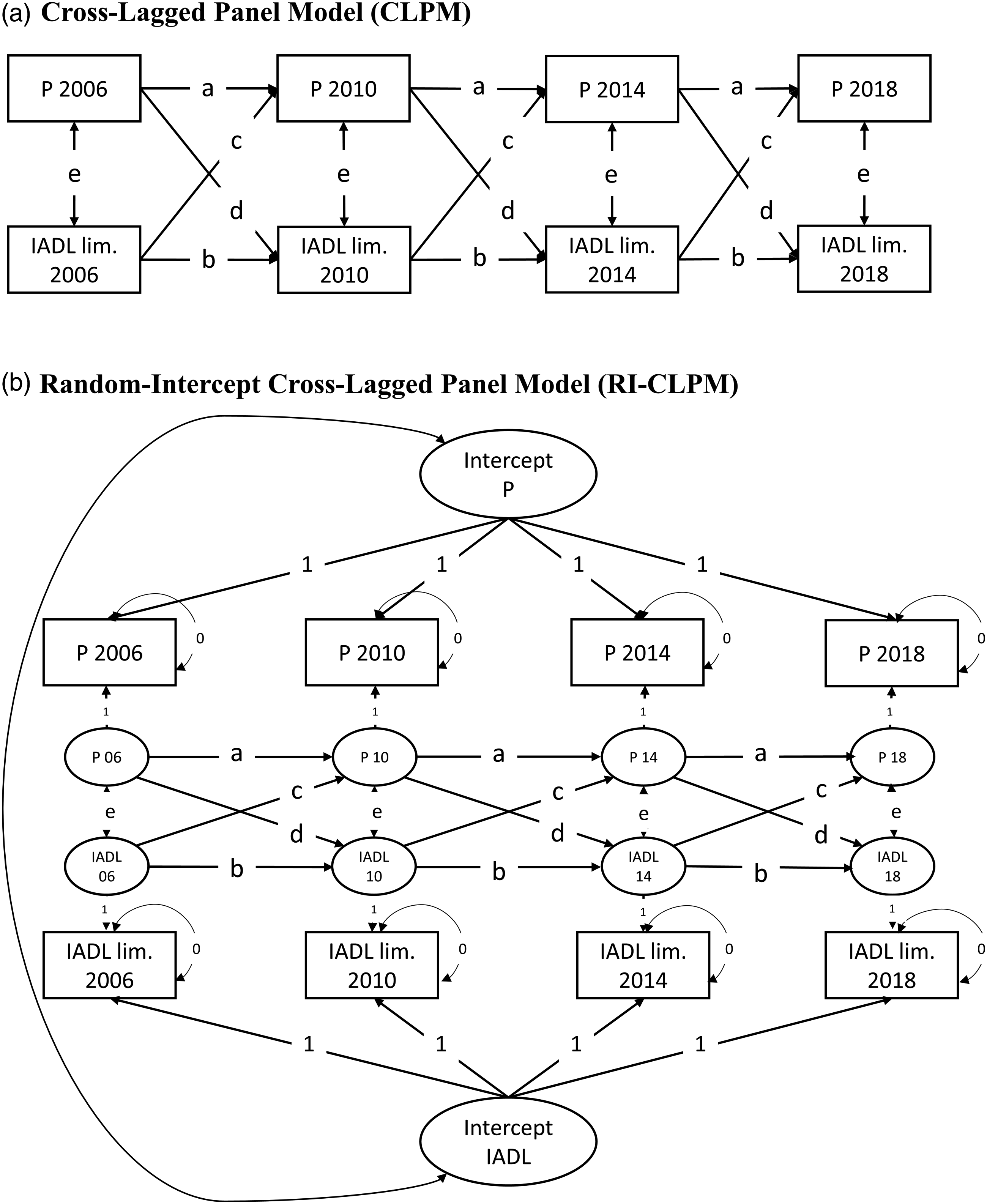
For the RI-CLPM, we specified a random intercept for each construct that loaded on all measurement occasions with a loading of λ = 1, representing the stable level across time. The random intercepts were allowed to correlate. Apart from the random intercept, the same paths were specified as for the CLPM. The extraction of the stable variance with the random intercept ensures that the paths a to e in the RI-CLPM represent associations between the intra-individual fluctuations around the stable intra-individual mean level. For the CLPM, the paths represent a blend of between-person and within-person associations. To test whether the paths can be constrained to equality across time, we compared the model fit of a model without equality constraints to a model in which each path was constrained to equality across time. We did so for both the CLPMs and RI-CLPMs (see OSF Table 2 for model fit indices). For all models, the BIC values were lower for the constrained models, suggesting that the paths could be set to equality across time. As such, we will use the constrained models for the subsequent analyses.
For the first research question, whether personality traits and IADL limitations are associated, we examined the correlations between the random intercepts (between-person) and occasion-specific residuals (within-person) in the RI-CLPM. While this is also reflected in the within-time correlations in the CLPM (parameter e in Figure 1a), stable (i.e. between-person) and measurement occasion–specific (i.e. within-person) associations are confounded in this model. With regard to the second research question, whether personality traits predict IADL limitations at a subsequent time point and vice versa, we examined the cross-lagged effects in the CLPM (paths c and d in Figure 1a; Hamaker et al., 2015; Mund & Nestler, 2019). Because the cross-lagged paths in the CLPM incorporate a mix of between- and within-person associations, we used the RI-CLPM to investigate our third research question, whether intra-individual changes in personality traits are associated with changes in IADL limitations at a subsequent time, and vice versa. More specifically, we examined the cross-lagged effects in the RI-CLPM (paths c and d in Figure 1b).
To examine whether the effect of personality on IADL limitations or the effect of experiencing more IADL limitations on personality change was stronger, we tested for significance between the magnitude of the cross-lags by estimating a difference parameter within the model and deriving standard errors and significance values with 1000-fold bootstrapping. Finally, all models controlled for age (numeric), gender (binary variable), education (number of education years) and (time-varying) cognition (numeric), as they have been suggested to impact older adults’ health and personality (Canada et al., 2021; Deary et al., 2010; Jaconelli et al., 2013; Mueller et al., 2018; Terracciano et al., 2017). In all models, we specified covariances between the control variables, such the entire sample was used for the models estimation (i.e. participants with only one assessment on cognition were not excluded).
Results
Descriptive results
Means, standard deviations and correlations.
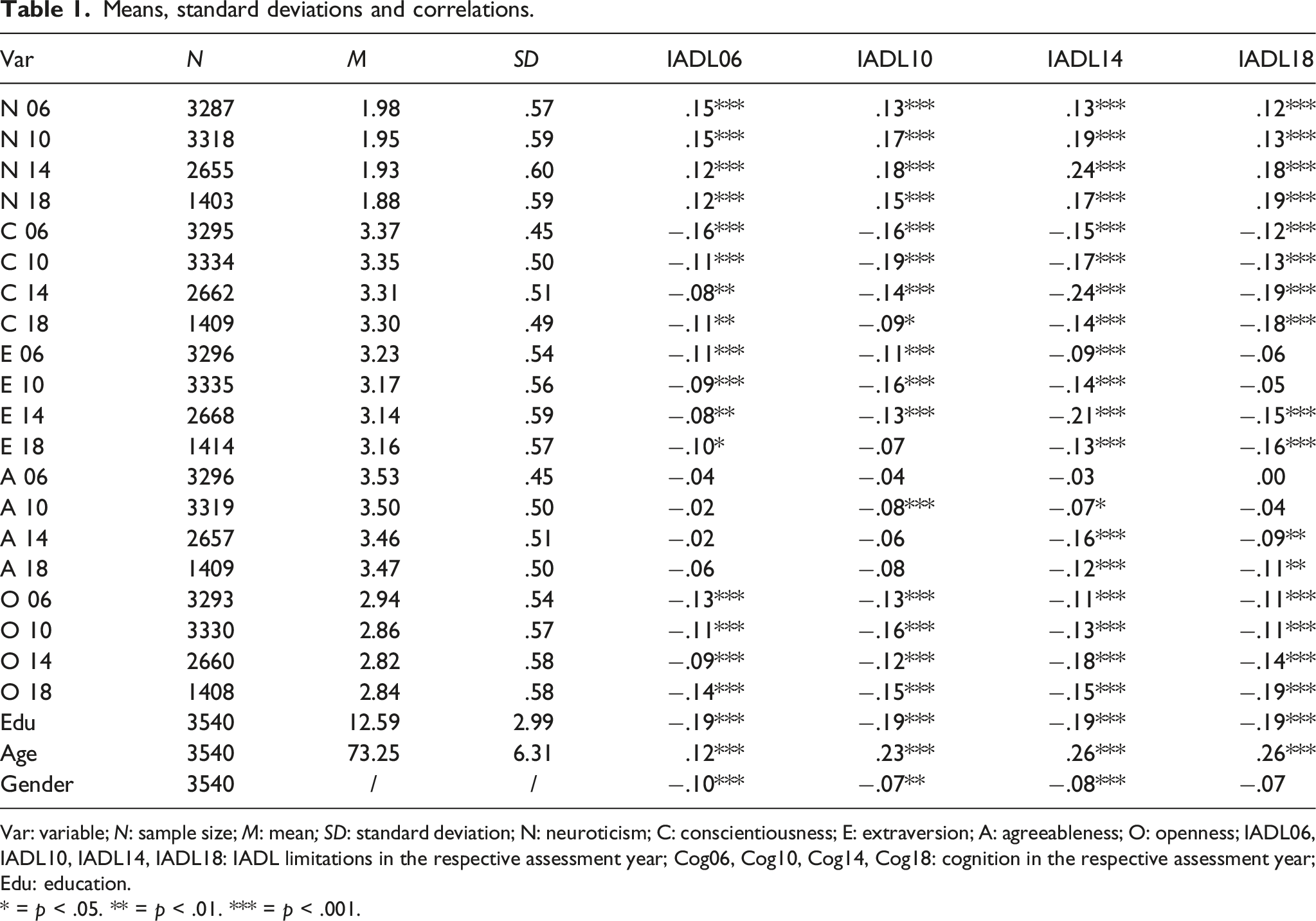
Var: variable; N: sample size; M: mean; SD: standard deviation; N: neuroticism; C: conscientiousness; E: extraversion; A: agreeableness; O: openness; IADL06, IADL10, IADL14, IADL18: IADL limitations in the respective assessment year; Cog06, Cog10, Cog14, Cog18: cognition in the respective assessment year; Edu: education.
* = p < .05. ** = p < .01. *** = p < .001.
Model fit and measurement invariance
Longitudinal measurement invariance models for traits.
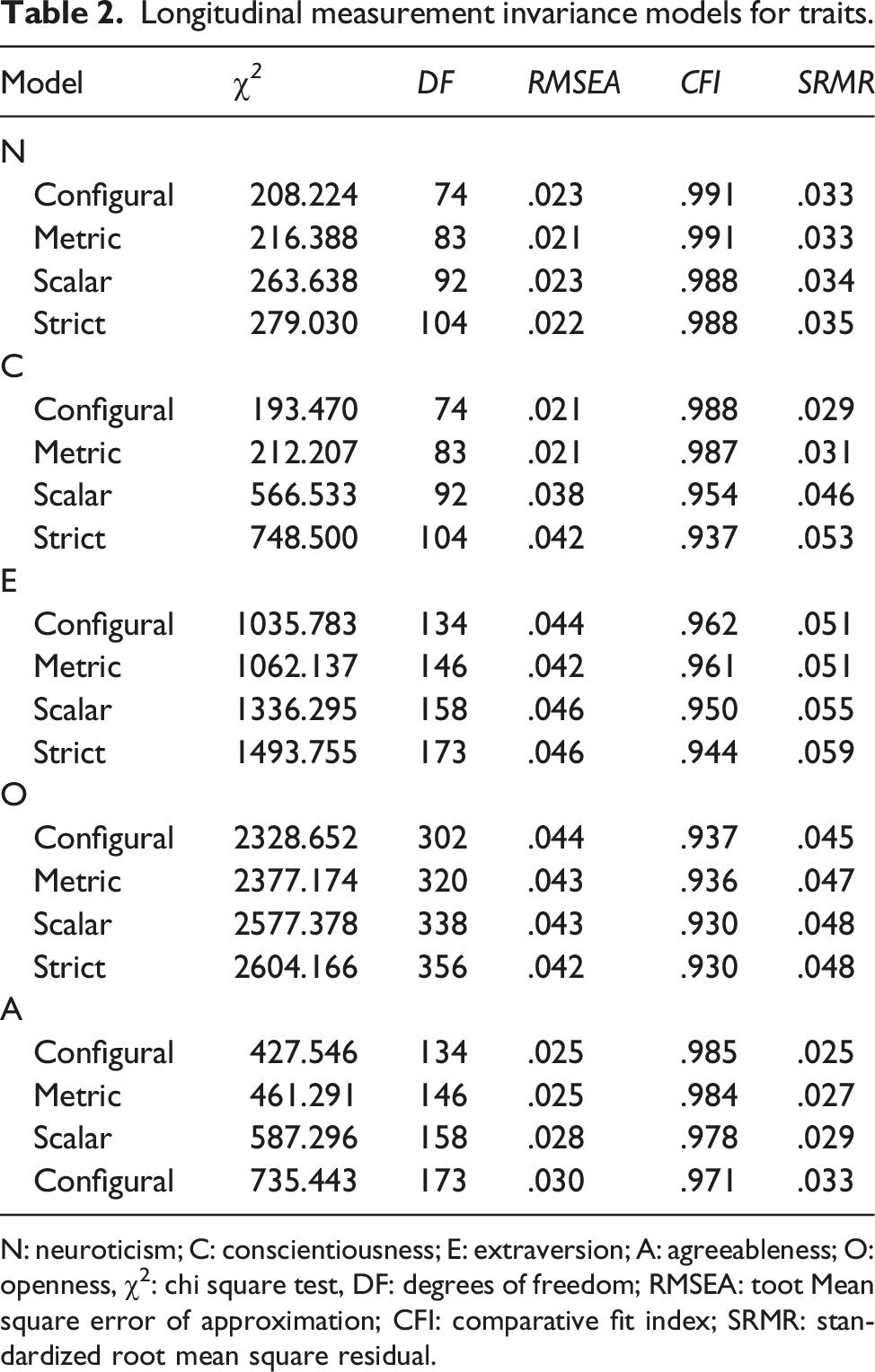
N: neuroticism; C: conscientiousness; E: extraversion; A: agreeableness; O: openness, χ2: chi square test, DF: degrees of freedom; RMSEA: toot Mean square error of approximation; CFI: comparative fit index; SRMR: standardized root mean square residual.
Model fit cross-lagged panel model and random-intercept cross-lagged panel model.
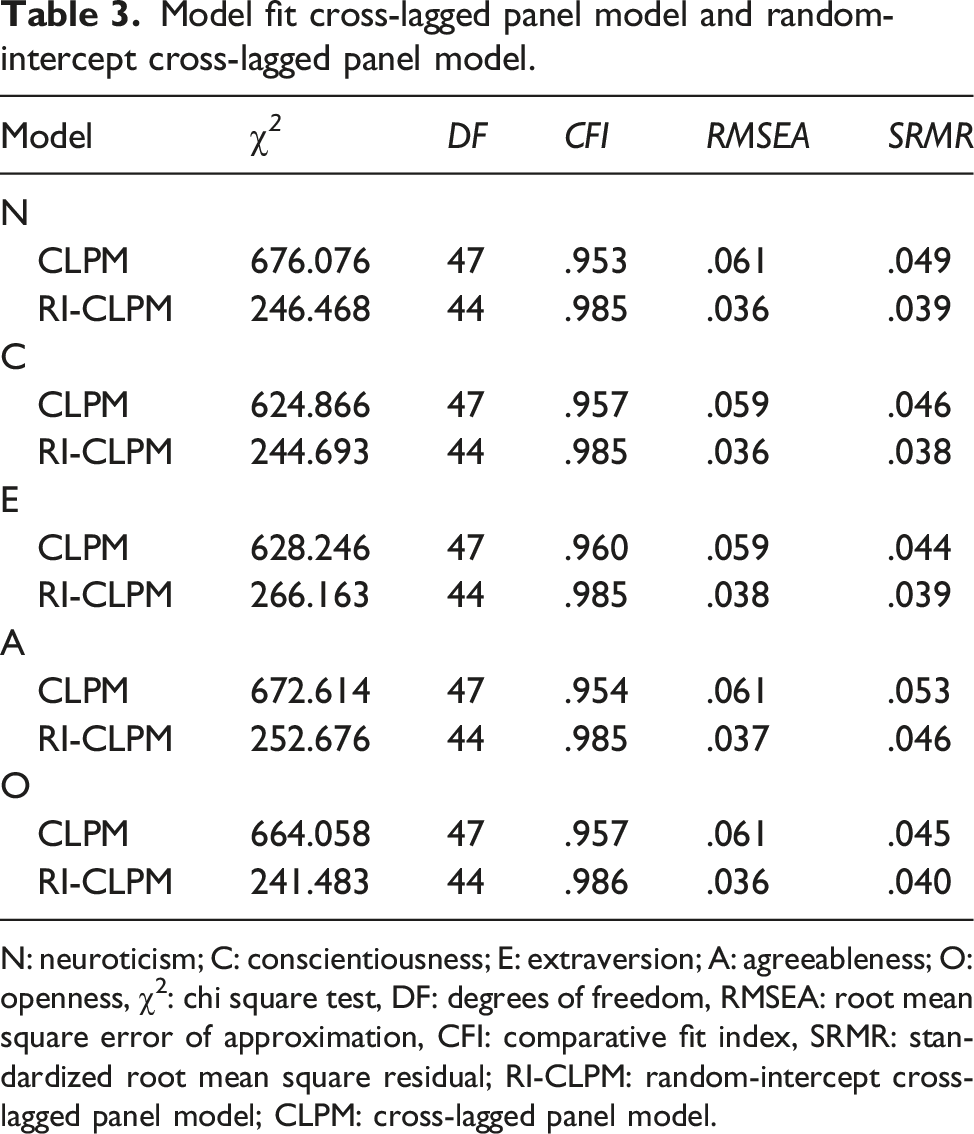
N: neuroticism; C: conscientiousness; E: extraversion; A: agreeableness; O: openness, χ2: chi square test, DF: degrees of freedom, RMSEA: root mean square error of approximation, CFI: comparative fit index, SRMR: standardized root mean square residual; RI-CLPM: random-intercept cross-lagged panel model; CLPM: cross-lagged panel model.
Correlations between personality traits and IADL limitations
Within waves, the number of reported IADL limitations correlated from r = .15 to .24 (ps < .001) with the N scores, from r = −.16 to −.24 (ps < .001) with the C scores (see Table 1), from r = −.07 to −.21 (ps < .05) with the E scores, and from r = −.09 to −.19 (ps < .001) with the O scores. The correlations with A were mixed (see Table 1). Parameter estimates for CLPM and RI-CLPM, can be found in Table 3. We found a moderate correlation between the random intercepts of N and IADL limitations (r = .20, p < .01), showing that in general, older adults who have higher levels of N tend to have more IADL limitations compared to older adults with lower N. Further, there was also a significant negative correlation between the random intercepts of C and IADL limitations (r = −.15, p = .018), showing that older adults who reported higher C levels also reported less IADL limitations compared to older adults with lower C. We found no significant correlations of the random intercepts for E, O and A.
Parameter estimates of the cross-lagged panel model and random-intercept cross-lagged panel model.
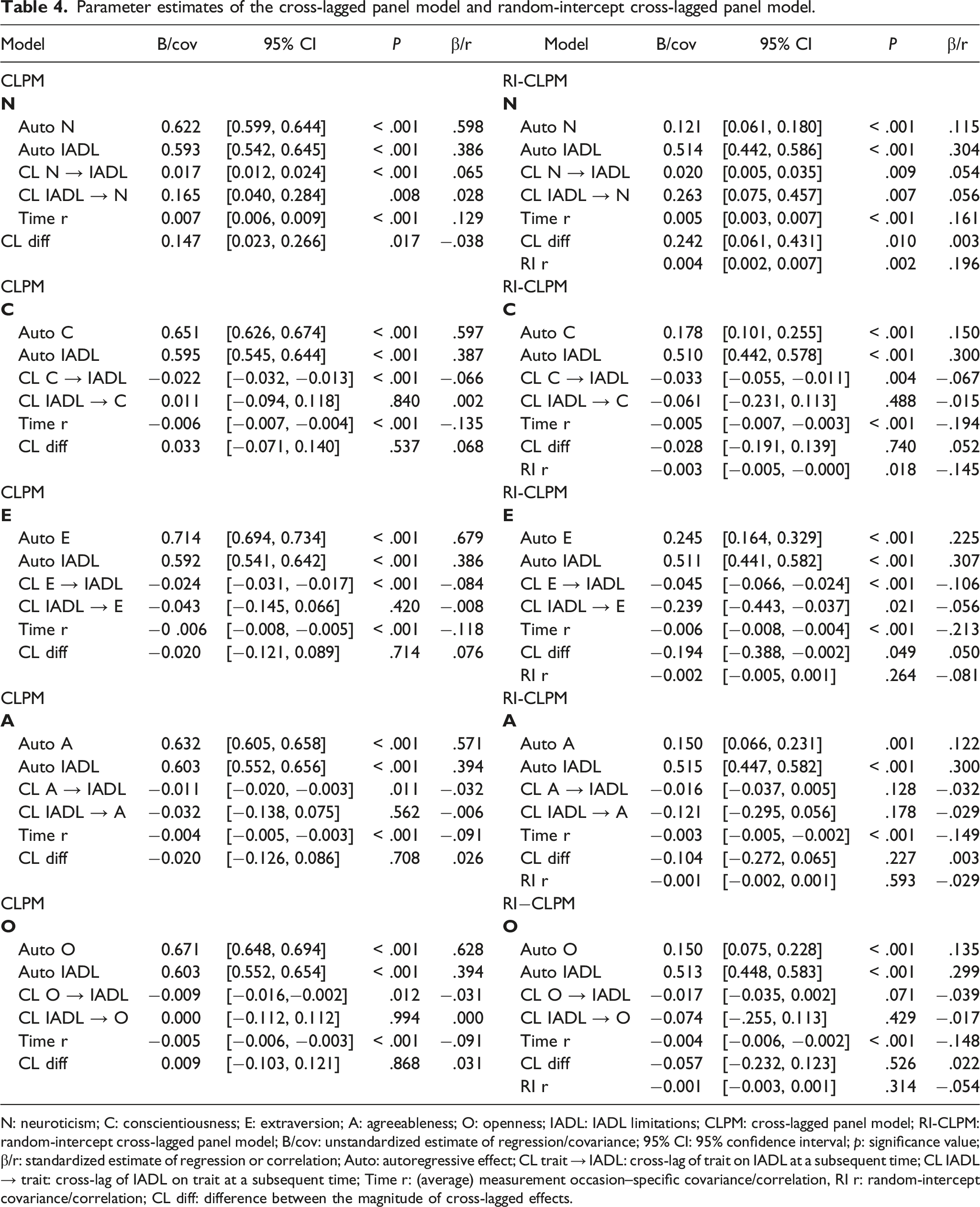
N: neuroticism; C: conscientiousness; E: extraversion; A: agreeableness; O: openness; IADL: IADL limitations; CLPM: cross-lagged panel model; RI-CLPM: random-intercept cross-lagged panel model; B/cov: unstandardized estimate of regression/covariance; 95% CI: 95% confidence interval; p: significance value; β/r: standardized estimate of regression or correlation; Auto: autoregressive effect; CL trait → IADL: cross-lag of trait on IADL at a subsequent time; CL IADL → trait: cross-lag of IADL on trait at a subsequent time; Time r: (average) measurement occasion–specific covariance/correlation, RI r: random-intercept covariance/correlation; CL diff: difference between the magnitude of cross-lagged effects.
Reciprocal effects based on CLPM
For our second research question, we examined whether older adults with higher N and lower C, E, and O levels reported more IADL limitations at a subsequent time point, and vice versa (path c and d in Figure 1a; for estimates see Table 4). In the CLPM, the cross-lagged coefficients showed that higher levels of N were predictive of more IADL limitations at a subsequent time (β = .065, p < .001) and more IADL limitations predicted higher levels of N at a subsequent time (β = .028, p = .008). The effect of N on IADL limitations was stronger than the reciprocal effect (Δβ = −.038; p = .017). An increase in IADL limitations was predicted by lower levels of C (β = −.066; p < .001), lower E (β = −.084; p < .001), lower A (β = −.032, p = .011) and lower O (β = −.031, p = .012), but a reverse effect of IADL limitations on these traits was not found.
Reciprocal effects based on RI-CLPM
With respect to our third research question, we expected intra-individual increases in N and decreases in C, E and O to predict increases in IADL limitations at a subsequent time point, and vice versa (paths c and d in Figure 1b; for estimates see Table 4). In the RI-CLPM, measurement occasion–specific increases in N predicted changes in IADL limitations (β = .054; p = .009), as well as the other way around (β = .056; p = .007). The effect of decreases in IADL limitations on increases in N was significantly stronger than the effect of increases in N on IADL limitations (Δβ = .003; p = .011) - albeit with a negligible difference. Decreases in C also predicted increases in IADL limitations (β = −.067; p = .004), but the reciprocal effect of IADL limitation on C was not significant (β = −.015; p = .488). Decreases in E lead to increases in IADL limitations (β = −.106, p < .001), and increases in IADL limitations predicted decreases in E (β = −.056, p = .021). However, it is not clear which direction of the effect was causally dominant (Δβ = .050, p = .049). No significant effects were observed for A and O, contrasting the significant effects from A and O on IADLs found with the CLPM.
In summary, increases in reported difficulties of performing IADL were preceded by increases in N, decreases in C and decreases in E. In contrast, reporting more IADL difficulties had an effect on increasing N and E at a subsequent time, but no effect on C, O and A.
Discussion
This study investigated the reciprocal association between personality and IADL limitations using four waves of data (covering 12 years) from the Health and Retirement Study (HRS). To do so, we used a random-intercept cross-lagged panel model and compared the findings to the more commonly used cross-lagged panel model. In line with previous research, we found the strongest associations between IADL limitations and the personality traits N and C. For these traits, we found cross-sectional associations, as well as effects of the traits on functional capacities, and for N, also the reciprocal effect. The findings for the other traits were less pronounced or differed by model used. In the following, we discuss the main findings in detail.
Correlations between personality and IADL limitations
Concurrently, higher N, lower C, E, A and O were associated with more IADL limitations, which replicates previous cross-sectional research on smaller samples of older adults (Gogniat et al., 2020; Suchy et al., 2010). When looking at the correlation between the random intercepts of RI-CLPM, reflecting between-person associations for personality traits with health (i.e. correlation of time-invariant traits with the time-invariant component of IADL), only higher N and lower C were associated with more reported IADL limitations. This denotes that individual differences in N and C are linked to individual differences in IADL limitations, such that older adults with a higher tendency towards distress and emotional instability (i.e. higher N) and a higher tendency to be disorganized and less dutiful (i.e. lower C) compared to others, report having also more IADL limitations (i.e. difficulties with performing tasks such as preparing meals and taking medication). This effect could result from a lifetime of poor health-related behaviours and dysfunctional psychological processes. For example, higher N and lower C and E were previously associated with less physical activity (Sutin et al., 2016), more depressive symptoms (Hakulinen et al., 2015) or less qualitative social relationships (e.g. Allemand et al., 2015; Parker et al., 2012), and in turn, these have been related to higher incidence of IADL limitations and other health impairments (e.g. Balzi et al., 2010; Canada et al., 2021; Holt-Lunstad et al., 2010; Turiano et al., 2021).
In terms of correlated change, or time-specific within-person correlations between deviations in traits with deviations in health, we found significant effects for all traits. This shows that the observed between-person associations (i.e. random-intercept correlations) were not always generalizable to within-person correlated change, a conclusion similar to the one reached by Luo et al. (2022). The within-person association may be driven by changes in a third, unmeasured variables (e.g. death of partner and transition periods) that determine changes both in personality and IADLs. Another possible explanation for this effect may be that increases in IADL limitations affected the traits or the self-perception of the participants negatively in a shorter time span then covered by the cross-lags, resulting in simultaneous increases in N self-ratings, and decreases in the ratings on the other traits.
The longitudinal dynamics of personality and IADL limitations
The observed predictive effects of personality on IADL using the CLPM are in line with recent findings of Canada et al. (2021), who showed that higher N and lower C, E and O at baseline were related to a higher risk of IADL limitations 3–12 years later, across eight longitudinal datasets. Canada and colleagues did not find a significant effect from A to IADL, while we observed a significant negative cross-lag of A on IADL. A similar non-finding for A was reported also by Wettstein et al., (2017), on a sample of adults older than 44 years of age. The discrepancy could possibly be explained by the sample used by Canada et al. (including middle-aged adults) and the use of only two assessments (baseline and follow-up).
At the intra-individual level (i.e. cross-lags in RI-CLPM), we found that increases in the tendency to show distress and emotional instability (increases in N), decreases in the tendency to be self-disciplined and organized (decreasing C) and decreases in the tendency to be outgoing and social (decreasing E) predicted increases in reported difficulties with performing IADL at a subsequent time. These findings are in line with research assessing personality and health also in younger samples (adults older than 15 years of age; Luo et al., 2022) and indicate that traits not only predict individual differences in functionality, but also within-person changes in health. As outlined by Turiano et al. (2021) within the PHP model, changes in traits could have an effect on health indices through psychological changes (i.e. increases in stress reactivity), changes in health behaviours, and changes in social relationships (e.g. social support). However, research investigating how changes in these mechanisms lead to changes in health is still limited. For example, so far, we know that decreases in C were associated with decreased self-perceived health through decreasing health preventive behaviours (Takahashi et al., 2013), and that increases in N predicted changes in mental health status (i.e. increases in depression; Chow, & Roberts, 2014), which was linked to physical functioning (Canada et al., 2021). Further, increases in N and E have been associated with increases in negative social support (e.g. being criticized; Hill et al., 2018), which could possibly determine changes in health outcomes (Jackson et al., 2017). However, more research is needed to investigate the potential influence of certain mechanisms (e.g. health behaviour and social support) for the link between personality and changes in IADL limitations, ideally investigated as time-varying factors.
When considering the reverse relationship (i.e. IADL predicting personality), within CLPM we found that older adults who have more limitations in performing IADL compared to others, are more likely to report higher N at a later time. This finding is in line with previous research on middle-aged and older adults, that, using also cross-lagged panel models (albeit on smaller samples), confirmed the effect of subjective and objective health on N (Wettstein et al., 2017; 2018). Thus, having more functional limitations (compared to others) likely implies having a higher tendency to show distress and irritability (i.e. higher N) at a later time. This predictive effect could be explained by lower mobility, less opportunities for social participation, self-discipline and higher loneliness of those with poor functional capacities (Jackson & Hill, 2019; Luo et al., 2012; von Soest et al., 2020), that in turn foster higher N (Mund & Neyer, 2016; Roberts & Wood, 2006).
While we found a predictive effect from IADL to N using the CLPM, we did not find effects for the other personality traits. This contrasts the findings of Wettstein et al., (2018) and Wettstein et al., (2017), reporting also a reversed link between N, C, A and different health indices (i.e. IADL, self-rated health and objective health). However, the conditions under which these effects were observed differed (e.g. reciprocal links between A and IADL are found only in sensory impaired older adults; or some effects fail to exist in the presence of covariates), highlighting the complex picture of the personality–health association.
The effect of IADL on N was confirmed also within-person (cross-lags in RI-CLPM), suggesting that increases in reported IADL limitations lead to increases in N. Interestingly, in contrast to the previous results, an additional effect emerged within the RI-CLPM, as increases in reported IADL limitations predicted decreases in E. These within-person observed effects align with past findings, showing increases in N and decreases in E in response to increasing health problems (Kornadt et al., 2018), decreasing physical functioning (Mueller et al., 2018) or frailty (Stephan et al., 2017) in older adults. From the perspective of Selection, Optimization and Compensation (SOC) model of Baltes and Baltes (1990), the negative ratio of gains to losses characterizing old age would favour older adults to invest their current resources differently in order to adapt to everyday challenges. This means, that with increasing IADL limitations, older adults would increase in N and decrease in E, as they become more aware of everyday dangers that could further damage their health (Kornadt et al., 2018; Mueller et al., 2017).
Contrary to our expectations, increases in IADL limitations did not predict decreases in C and O. This non-significant effect is surprising given some past research showing that decreasing self-rated health (Luo et al., 2022), onset of chronic disease (Jokela et al., 2014) or frailty (e.g. walking speed, fatigue; Stephan et al., 2017) predicted decreases in C and O. This unexpected finding could be explained by the health indices we used, as IADL describe more complex activities (e.g. handling money and cooking). In the sense of SOC (Baltes & Baltes, 1990), individuals reporting difficulties in performing such activities could try to maintain their C or O levels by focussing specifically on these activities or parts of these activities (i.e. Selection), as they are relevant for their independence and autonomy. They could also use C or O-related strategies (e.g. reorganizing dishes and food to be more easily accessible; finding strategies to keep track of money) to reduce the effects of physical and mental decline on the performance of such tasks (i.e. Compensation). Therefore, future research could examine whether more basic ADL (e.g. bathing and eating), have a more powerful effect on changes in C and O. A second possible explanation is that our study used self-reported data to measure IADL limitations, instead of objective measures of functionality (as previous studies mentioned in this paragraph). Future studies should try to include both performance-based and self-reported measures of functional capacities.
An alternative explanation for these non-findings pertains the time lag between assessments. Within HRS, the time lag is 4 years (i.e. personality assessed every 4 years on the same sample), which could attenuate some of the existing effects. For example, using a RI-CLPM, Luo et al. (2022) confirm reciprocal associations also between C, O, and self-reported health with a time lag of 1 year between observations (on a sample of adults aged 15 years and older). Thus, it could be that certain trait-health links are more sensitive to the time lag between assessments than others. For example, both our study and the paper of Luo et al. (2022) failed to capture a longitudinal link for A (despite different time lags), while the reciprocal links between N, E and health (IADL in this case) have been confirmed. More research is however needed to investigate the optimal time lag to investigate such relationships.
Interestingly, when comparing the size of the two lagged effects within CLPM, for N, the predictive effect of the trait on IADL limitations was significantly higher than the reverse predictive effect, but the difference was small (Δβ = −.038). Within RI-CLPM, a significant difference emerged in the opposite direction (effect of IADL is higher), but the effect was negligible (Δβ = .003). No other differences in the magnitude of the cross-lags were observed for the rest of the traits. Still, further replications are needed before giving conceptual explanations for a significant difference, but the reciprocal associations found for N, E and IADL highlight the complex picture of the personality–health association and ask for the inclusion of both directions of the effects (i.e. personality on health and vice versa) in future research.
Practical implications
When transferring the empirical findings to clinical practice, the two perspectives inform each other: It is valuable to know that someone who scores higher on N compared to other people will (likely) experience more IADL limitations at later timepoints (between-person approach), as this could allow practitioners to identify potential risk groups. However, in order to properly inform clinical interventions, it is necessary to check if changes in traits lead to later changes IADL limitations (within-person approach). As mentioned earlier, such effects were observed for N and E, in both predictive directions, and for the effect of C on reported IADL limitations. This observation emphasizes the importance of building interventions aimed at changing traits (Hudson & Fraley, 2015; Roberts et al., 2017; Stieger et al., 2021), and call for more interventions of personality change in samples of older adults specifically. Alternatively, intervention research that aims at compensating IADL limitation through assistive care could also investigate if increases in independence (i.e. IADL performance) foster personality change and the extent to which in the long term this change is desirable (e.g., increases in E could prompt more social support, but it might lead to exposure to other health risks).
Limitation and directions for future research
Some limitations of this research have to be taken into account when putting the current findings into perspective. In order to maximize sample size, we used data from participants that completed at least two assessment waves for each variable. This sample size was large enough to have sufficient power to detect small effects. For example, for detecting a small effect size expressed as a correlation of .1, power equals .96 for an alpha of .05 and a sample of 1400 participants, and the degrees of freedom for all of our tests (much) exceeded 1400. When comparing the two extreme groups of participants included in the analysis (those with only two waves vs. those with complete assessment), it was found that participants with only two assessments were older (70.75 vs. 74.29 years of age), and less educated (13.14 vs. 12.52 years of education). Further, men had also more incomplete assessments compared to women. Still, the only group difference that had a high effect in terms of effect size (Cohen’s d; Cohen, 1988) was age, but still with only a 6 years difference in the means of the two (extreme) groups. We included these demographic variables as control variables in the model to account for these differences.
It is important to keep in mind that both, personality traits and IADL were self-reported. As such, the found correlations between personality and IADL limitations may partly reflect shared self-perception processes, such as an over-reporting of limitations for more neurotic individuals, and potential under-reporting for individuals with higher conscientiousness levels (see Suchy et al., 2010). C had also a low reliability, most probably due to the reduced number of items (i.e. five) and a negatively keyed item. Further, in HRS, IADL limitations are assessed on a binary scale, and a composite score was obtained for this measure. Even if it is generally argued that this approach is appropriate to capture IADL disabilities (Chan et al., 2012), evaluating the association of personality with continuous and more objective measures of IADL limitations could offer a more complete understanding of the association of personality with functional capacities.
Further, this study aimed to capture if changes in one’s capacity to perform IADLs leads to changes in personality; hence, we restricted our study sample to older adults (65 years of age and older), who were living independently at the first assessment occasion, assuming that older adults living in nursing homes or adults disabled have less room to lose/gain in their capacities to perform IADLs. However, future studies should investigate if these assumptions hold and if our findings can be generalized to a larger population. In addition, the time between the assessment points was also large (i.e. 4 years). This led to an underrepresentation of adults older than 85 years in this sample (i.e. old-old adults). Therefore, we could not differentiate young-old from old-old adults in their cross-lagged associations between personality and IADL. A more fine-grained time scale (years, months) would offer the possibility to capture a more dynamic picture of the personality and IADL association and could also allow to include age as a moderator, ideally as a continuous variable (e.g. Olaru & Allemand, 2021). We would expect the protective effect of personality traits for health to lose importance with advancing age and a stronger physical and cognitive decline (Baltes et al., 2007; Mueller et al., 2018). In contrast, the impact of health decline on personality change might be more pronounced in very old age, as the functional decline might be too strong to be compensated by psychosocial resources (Baltes et al., 2007).
Conclusion
The current study advances our understanding of the association between personality and functional capacities in older age by investigating the reciprocal associations of the two constructs, using two analytical approaches often employed in the study of bidirectional associations: the traditional CLPM and its within-person extension, RI-CLPM. With the use of CLPM, we found that all personality traits predicted IADL limitations, and more self-reported IADL limitations predicted higher N at a subsequent time. These findings were partially replicated within the RI-CLPM, or at the intra-individual level, as changes in N, C and E predicted changes in reported IADL, but a reciprocal effect was found only for N and E. In summary, personality traits (at least N and E) and functional health seem to be both predictors and outcomes of each other, but the results differ depending on the chosen analytical approach. These findings highlight the co-development of personality and functional capacities in old age, while providing evidence for future interventions studies targeting personality traits to maintain high functioning in old age.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.