
Abstract
Purpose
To assess the differences in Human Immunodeficiency Virus (HIV) testing among women survivors of traumatic Childhood Sexual Abuse (CSA) by urban-rural residency status.
Design
Cross-sectional survey.
Setting
2022 Behavioral Risk Factor Surveillance System (BRFSS).
Sample
Adult women (N = 6616) with a history of CSA from 12 US states.
Measure
Outcome was HIV testing. Covariates included sociodemographic characteristics, health-risk behaviors, perceived health status, presence of any disability, and subjective cognitive decline.
Analysis
We conducted three multivariable logistic regression models for urban-only, rural-only, and both, summarizing associations between HIV testing and covariates using adjusted odds ratios (aORs) and survey-weighted estimates.
Results
Logistic regression analysis highlighted significant urban-rural differences in HIV testing among Women CSA (WCSA) survivors. Among urban women, those aged 45-55 (aOR = 4.96), Asians (aOR = 9.58), current smokers (aOR = 2.13), and those with subjective cognitive decline (aOR = 2.99) had higher odds of HIV testing compared to their counterparts. Among rural women, being Hispanic (aOR = 19.40) and a current smoker (aOR = 3.44) were associated with higher odds of HIV testing. All P-values < .05.
Conclusions
Findings highlight the need for future research on interventions including raising awareness on different testing strategies for rural WCSA survivors with lesser education to enhance HIV testing uptake.
Purpose
In the United States (US), approximately 25% of girls and 5% of boys experienced a lifetime childhood sexual abuse (CSA) involving non-consensual sexual acts with a minor. 1 CSA can be traumatizing, leading to long-term negative health impacts,2,3 engagement in risky health behaviors, and limited health service utilization. 4 As of 2022, approximately 1.2 million people in the US were living with HIV, with 31,800 new diagnoses annually, and a higher proportion lives in the rural areas.5,6 Research has identified a high prevalence of CSA history (31%) among people living with HIV (PLHIV). 7 However, studies examining HIV testing among CSA survivors remain limited, particularly in the context of urban-rural disparities. Furthermore, CSA survivors face unique challenges related to HIV testing including fear of disclosure, and limited health care access, with heightened stigma in rural areas. 8 This paper aims to add the existing literature by examining the relationship between HIV testing behaviors and covariates among US Women CSA (WCSA) survivors, a unique and HIV-susceptible group, with an emphasis on urban and rural settings.
Methods
Setting & Design
This cross-sectional study uses nationally representative data from the 2022 Behavioral Risk Factor Surveillance System (BRFSS), an annual telephone-based survey conducted by the Centers for Disease Control and Prevention (CDC) and state health departments across U.S. states and territories. The BRFSS employs a disproportionate stratified sampling design, with an overall median response rate of 44.1%.9,10
Sample
The present study analyzed 2022 BRFSS data on the US women aged 18 and older who experienced lifetime CSA (N = 6,616). CSA-related questions were included as a part of the Adverse Childhood Experiences module, which was administered in 12 US states.
Measures
The outcome variable was self-reported HIV testing, excluding tests conducted for blood donations. 11 The exposure variable was a history of CSA. 11 Covariates included socio-demographic characteristics: age groups (18-24, 25-34, 35-44, 45-55, 55-64, ≥65), race/ethnicity (i.e., non-Hispanic (NH) White, NH Black, NH Asian, American Indian/Alaska Native, Hispanic, and other), education level (< high school, high school graduate, 1-3 years college (some college or technical school), and college graduate (4 or more years or college graduate)), household income (< $15,000, $15,000 to < $50,000, ≥ $50,000), and being employed. 11 Moreover, we included HIV risk behaviors (i.e., substance use, multiple sexual partners, etc.,), smoking status, binge drinking, as well as the presence of any disability and subjective cognitive decline. 11
Analysis
Descriptive statistics and Pearson Chi-Square tests of independence were performed to assess associations between HIV testing and covariates. Three multivariable logistic regression models were applied: for urban, rural, and both cohorts to understand the effect of different covariates in each sample on HIV testing uptake. Survey weight was applied, and a P-value of .05 or less was considered statistically significant. All analyses were performed using Stata 18.0. 12
Results
Among WCSA, 53% (n = 2,935) had ever been tested for HIV. Approximately 93% (n = 5,529) and 7% (n = 1,087) of the full sample were urban and rural residents, respectively. The bivariate analysis results revealed significant differences across the groups. Lower percentages of HIV testing were observed among the following populations: women aged ≥65 (8%), Asian or American Indian or Alaska Native women (2%), those with an annual household income less than $15,000 (15%), those currently unemployed (44%), current smokers (24%), binge drinkers (37%), those engaging in HIV risk behaviors (14%), and those who reported subjective cognitive decline (6%).
Among rural WCSA survivors, lower HIV testing rates were observed in several groups: those aged ≥65 (10%), women identifying as races other than those listed (other; 6%), individuals with less than a high school education (5%), those with a household income under $15,000 (13%), former smokers (29%), and individuals without disabilities (41%).
Results From Multivariable Logistic Regression: HIV Testing Status Among WCSA Survivors by Urban and Rural Status.
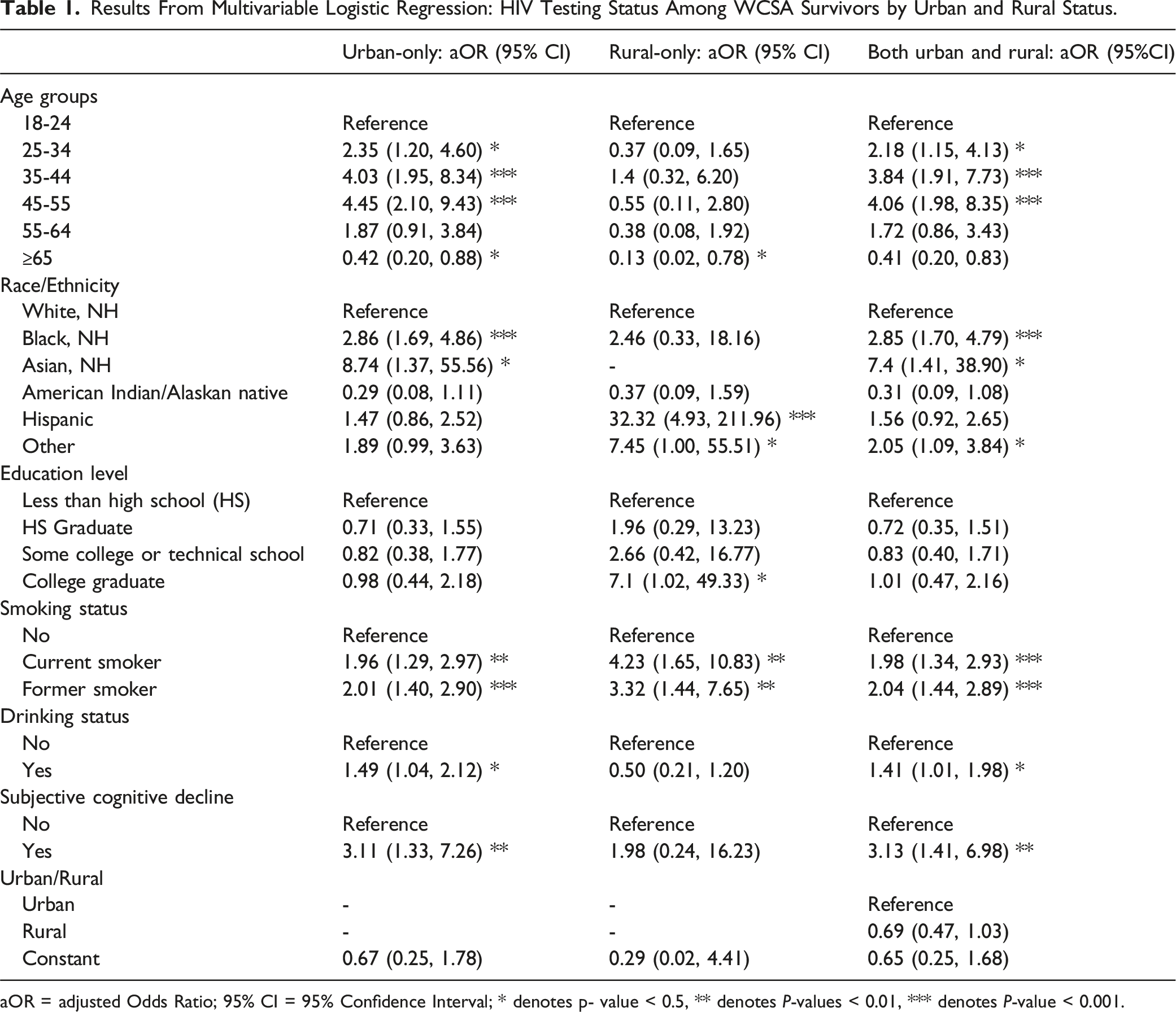
aOR = adjusted Odds Ratio; 95% CI = 95% Confidence Interval; * denotes p- value < 0.5, ** denotes P-values < 0.01, *** denotes P-value < 0.001.
Discussion
Summary
This study examined HIV testing patterns among U.S. WCSA across geographic location. While previous research among the non-WCSA women found lower HIV testing rates among younger women, our finding that middle-aged (25-55) urban WCSA survivors had a higher likelihood of HIV testing than younger survivors differs from these prior patterns. 13 While a prior study found that women who heavy or moderately drank were less likely to undergo HIV testing, 14 our findings indicate that the urban binge drinkers had higher odds of HIV testing than urban non-binge drinkers. Future research should explore HIV testing behaviors among urban non-binge drinkers and rural binge drinkers, where patterns were not clearly established in this study. Moreover, among WCSA survivors, smokers had higher odds of HIV testing than non-smokers, with increased likelihoods observed across both urban and rural residents. Additionally, the higher likelihood of HIV testing among individuals with cognitive decline may be driven by provider initiatives, as cognitive decline has been associated with HIV, 15 and early detection could facilitate timely treatment. These findings warrant further research.
The rural women with more education were more likely to get tested for HIV compared to those with less education attainment, aligned with previous research on the general adult population. 13 However, it is interesting that Hispanic WCSA survivors were more likely to undergo HIV testing, highlights the need for exploration of factors including motivations and health knowledge.
Critical Limitations
Our study has some limitations: Self-reported nature of BRFSS data may introduce social desirability bias. Also, caution must be taken to interpret temporal association between CSA and HIV testing uptake, due to the study’s cross-sectional design.
Significance
This study highlights factors influencing HIV testing uptake, emphasizing the role of geographic location, education, and co-morbidities, particularly among rural WCSA college graduates.
Conclusion
Although this study found no geographic disparities in HIV testing among WCSA survivors, it identified key factors influencing testing behaviors that differed between urban and rural populations. Given the high prevalence of CSA among PLHIV in prior research, our study’s findings warrant the need for future targeted interventions. This includes strategies such as raising awareness on available testing methods, particularly for rural WCSA survivors with lower educational attainment, to improve HIV testing uptake.
Recommendation
Further research is needed to better understand individuals with CSA, and their use of HIV testing to prevent a compounded burden on these vulnerable populations, particularly for rural WCSA survivors with lower educational attainment. Childhood sexual abuse (CSA) survivors often have limited access to health services or a decreased uptake of available health services. The present study uses 2022 BRFSS survey data to examine the association between HIV testing and multiple comorbidities specifically among Women CSA (WCSA) survivors, stratified by urban and rural residency status. The findings warrant future research focused on tailored health promotion and prevention strategies for both the general population as well as WCSA survivors, taking into account urban and rural residency status.So What?
What is already known on topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Author Contribution
WWM contributed to conceptualization, analysis, and writing the first draft, and revising the final version. QF & RA contributed to critical review and editing. BNM contributed to critical review, editing, and supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.