
Abstract
Keywords
In 2006, the Centers for Disease Control and Prevention (CDC) recommended offering human immunodeficiency virus (HIV) screening as part of routine medical care. 1 Since then, many states, including New York State, have created their own laws and regulations to reflect CDC’s recommendations. 2 When CDC first promulgated these recommendations, policy makers envisioned that emergency department HIV screening would be sustainable through reimbursement by public or private health insurance. 3 This view became even more tenable with the passage of the Affordable Care Act, which ensures coverage for many recommended clinical preventive services (including HIV screening). 4,5 Nevertheless, widespread sustained implementation of HIV screening has not taken hold in US emergency departments. 6 Because of the complexities of third-party billing, few hospitals report successfully recouping HIV screening costs from third-party insurers, 7 and even with the passage of the Affordable Care Act, many emergency department patients remain uninsured. 8,9 Consequently, because hospitals are expected to routinize emergency department HIV screening and not all patients have insurance that covers the HIV screening test, some patients might be surprised to receive a bill from the hospital for the HIV screening test.
This issue has raised the question (for example, at the AIDS Institute, New York State Department of Health) of whether patients should be alerted that they might be responsible for the cost of the HIV screening test when they are offered the test. To our knowledge, this question has not been addressed in published academic literature or public discussion. Although an alert would allow patients to consider cost when they make the decision to accept or refuse the test, such an alert could also dissuade patients from accepting the test and thereby frustrate policies intended to maximize HIV screening in emergency departments. In this brief commentary, we offer our views on the question of whether patients targeted for HIV screening in the emergency department should be alerted to the possibility that they could be billed for the cost of the test, and we suggest how New York State hospitals might address this issue.
To learn more about this question, we conducted a small survey at our medical center. From June 2013 through July 2014, we surveyed patients at Albany Medical Center on whether they might refuse an HIV test if they had to pay for it themselves. Albany Medical Center is a large urban medical center located in Albany, New York, and is a New York State Designated AIDS Center. 10 The emergency department serves approximately 70 000 patients annually and, at the time of the survey, had 1 full-time HIV testing counselor. For the survey, the counselor chose a convenience sample of patients aged 18 to 64 who were not known to be living with HIV infection. The first 334 respondents were surveyed and then offered a free HIV test; the next 251 respondents were first offered a free HIV test, and only those who accepted the HIV test were surveyed. To explore whether alerting patients to the costs of HIV testing would dissuade them from being tested, we asked the patients about their willingness to have an HIV test in the emergency department if the test were free or cost the patient $1, $10, $50, or $100. Patients participated in the survey anonymously. This project was approved by the Albany Medical Center Institutional Review Board.
Of the 585 patients who completed the survey, 391 (67%) were women; 265 (45%), non-Hispanic black; 188 (33%), non-Hispanic white; and 90 (15%), Hispanic. A total of 495 (85%) patients had health care insurance. Only 37 patients said that they would refuse a free HIV test, if offered. The proportion of patients who said that they would refuse an HIV test increased as the hypothetical cost increased (Figure). We found no differences in test refusal rates by age, race/ethnicity, sex, marital status, insurance status, or number of emergency department visits in the previous year. Despite the limitations of this convenience sample study, we concluded (1) that patients were less inclined to accept HIV screening if they had to pay for the test themselves than if the tests were free and (2) that notifying patients that they might be responsible for out-of-pocket costs for HIV testing might dissuade some from being tested.
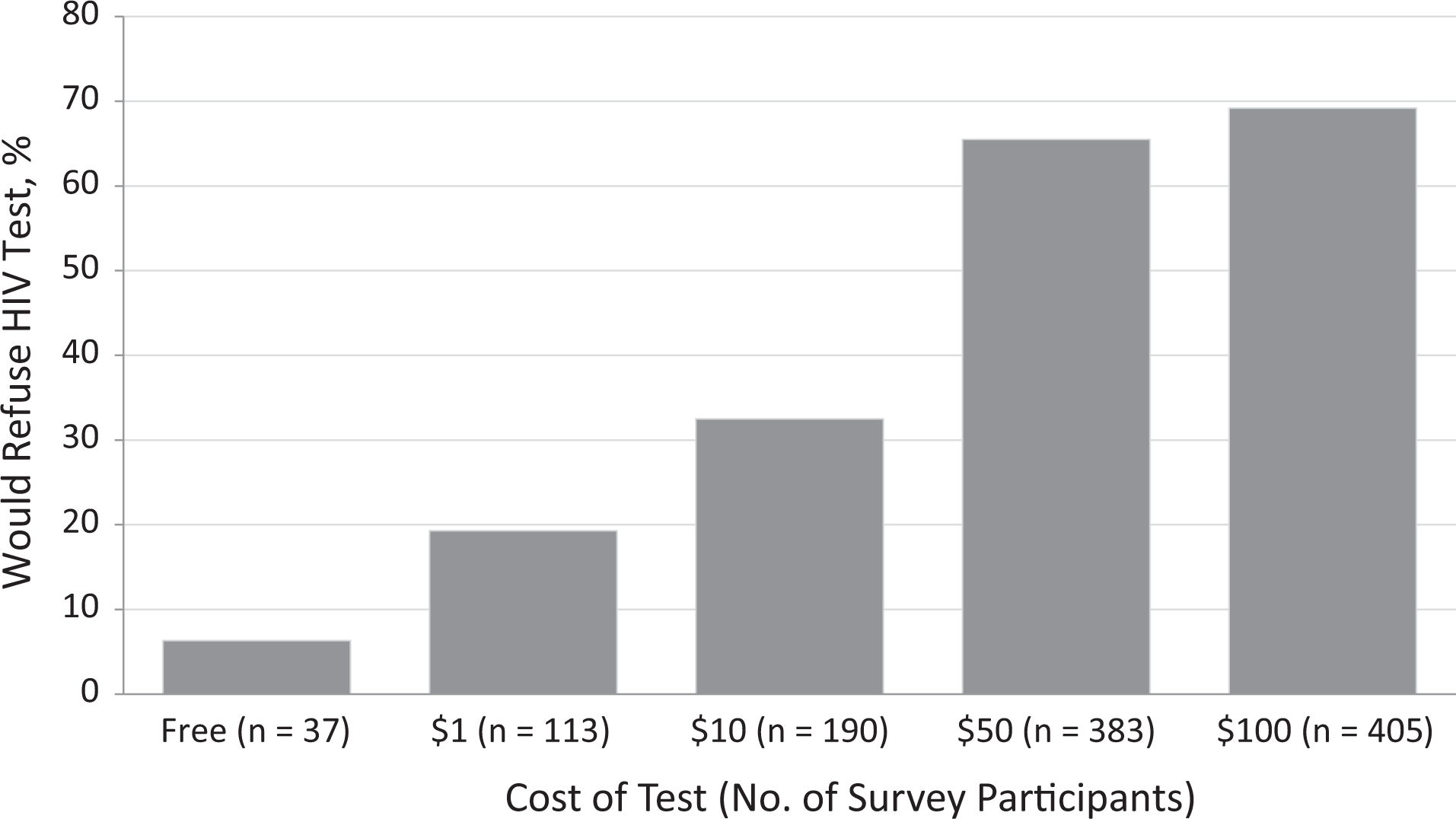
Proportion of patients who would refuse human immunodeficiency virus (HIV) testing if they had to pay for it, by cost of testing, in a survey of 585 patients conducted at Albany Medical Center, Albany, New York, 2013-2014.
Contemporaneously with the study, we convened an expert working group to provide recommendations on whether and how to alert patients of the possible costs of HIV screening in the emergency department. We chose 10 representatives from emergency medicine, HIV testing research, law, bioethics, and hospital administration. The group met for 1 day, hosted by the AIDS Institute, New York State Department of Health, on October 13, 2013.
The working group considered that, although CDC and New York State clearly consider HIV screening to be part of routine emergency department care, 1,2 some leaders in emergency medicine believe that routine preventive interventions should not be part of emergency care. 11 Accordingly, whether HIV screening (and the associated costs) lies outside routine emergency department care may still be debatable. In addition, the working group assumed that patients have the right, as consumers of health care, to be informed of the costs of their health care. Having considered these points, the working group also discussed that emergency department patients are not typically alerted of the costs of their emergency department care in a line-item fashion. Instead, they are typically informed that they will be responsible for all their emergency department costs through a routine written statement when they are signed in by the registration clerk. The working group recognized that alerting patients to the costs of HIV testing at the same time as offering the test might dissuade some from accepting the test, even in those cases when a patient’s insurance would cover the HIV screening test.
The working group came to a consensus on how New York State hospitals might approach this tricky issue. First, the working group recommended against specifically alerting patients of the costs of testing at the time that the test is offered (ie, “Would you like an HIV test? Your HIV test may not be covered by your insurance”). Second, the working group determined that it would be permissible for hospitals to alert patients to the costs of testing either implicitly or explicitly. It would be permissible to do this implicitly by simply allowing the cost of testing to remain as part of the general statement that all patients sign during the registration process, acknowledging that they bear financial responsibility for all their emergency department care. A patient always has the right to be informed of the cost of their health care in a line-item fashion. If a hospital felt that it was important to explicitly alert patients to potential additional costs of HIV screening, it would also be permissible to alert patients more explicitly by including language specific to extra procedures, such as HIV screening, during the registration process.
Footnotes
Acknowledgments
We acknowledge the contributions of all members of the working group not listed as authors: Jonothan Karmel, Franklin Laufer, and Lyn Stevens (AIDS Institute, New York State Department of Health, Albany, New York); Teresa Celada (Department of Philosophy, Wheaton College, Norton, Massachusetts); Frederick Heigel (Hospital Association of New York State, Rensselaer, New York); Lorraine Ryan (Greater New York Hospital Association, New York, New York); and Deborah Kaufman (Facilitator, Boston, Massachusetts).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.