
Abstract
Objective
This systematic review summarizes the effectiveness and the dose of walking interventions on specific cognition domains in older adults, including executive function, memory, attention, processing speed, and global cognition.
Data source
Published randomized controlled trials in PubMed, Embase, and Web of Science until 10 May 2023.
Study Inclusion and Exclusion Criteria
Studies include older adults without Alzheimer’s or related dementias, involving a walking intervention and performance-based neuropsychological assessments for executive function, memory, processing speed, attention, or global cognition.
Data Extraction
Two independent research assistants reviewed 8424 studies and included 17 studies.
Data Synthesis
Participant demographics, intervention features (type, intensity, time, frequency, duration, format, and context), cognitive assessment tools, and main findings.
Results
Nine studies found a favorable effect of walking interventions on at least one cognitive domain. Walking interventions improved executive function (n = 6) and memory (n = 3). These studies delivered the intervention individually (n = 3) for at least 40 minutes (n = 6) each time, three times per week (n = 8), between 6 to 26 weeks (n = 8), and walking at a moderate to vigorous intensity (n = 7).
Conclusion
Walking interventions may improve specific domains of cognitive function in older adults, particularly executive function and memory. More standardized reporting of intervention design and participant compliance based on published guidelines is needed to determine the dose-response association and the long-term effect of walking interventions on cognition.
Objective
Promoting healthy aging is critically important because, by 2050, approximately 22% of the population in the United States will be over the age of 65. 1 Age is a risk factor for Alzheimer’s disease and related dementias (ADRD), with no clear path for cure. Not only does ADRD affect individuals, but it also affects family members who provide care or help coordinate long-term care or nursing home placement. Thus, reducing the risk or delaying the onset of ADRD can potentially mitigate the public health burden.
One of the established risk factors for ADRD is physical inactivity, 2 making regular physical activity participation a preventative strategy. According to two meta-analyses, physically active older adults reported lower rates of cognitive decline and incidence of ADRD than their inactive counterparts.3,4 Similar results were found in more recent studies that used device-based measures for physical activity. For example, a systematic review found a positive association between global cognition and physical activity intensities (i.e., light and moderate- to vigorous-intensity physical activity [LPA and MVPA]). 5 Moreover, a meta-analysis found that exercise interventions, including aerobic exercise and multi-component exercise, improved cognitive function. 6 The current Physical Activity Guidelines for Americans report that physical activity promotes cognitive health, especially executive function, memory, processing speed, and attention domains, across all age groups. 7 However, only 18% of adults over 65 years old reported meeting the physical activity guidelines, 8 meaning the majority of older adults are not obtaining the full cognitive benefits from MVPA.
Older adults’ barriers to engaging in MVPA include, but are not limited to, physical health problems, frailty, fear of falling, and lack of knowledge of physical activity. 9 Walking can be a feasible solution to overcome these barriers. Unlike other aerobic exercises, walking has practical advantages because it is a lifestyle activity that requires minimum resources, equipment, and training and thus has few restrictions. 10 In addition to its feasibility, walking is an ideal type of activity for older adults because older adults require fewer steps per minute to reach a moderate-to-vigorous intensity. For older adults, 70 steps per minute is sufficient to reach moderate- to vigorous intensity, whereas other age groups may require 100 steps per minute or more. 11
One systematic review with meta-analysis, which included 44 randomized controlled trials (RCTs) with 4793 participants, reported that 60 minutes three times a week of walking at moderate intensity is required to improve cognition. 12 However, this meta-analysis focused on the effect of walking on global cognition and based its conclusions only on studies using the Mini-Mental State Examination (MMSE). Although MMSE is commonly used to assess overall cognitive function, including orientation, language, and memory, it does not emphasize other cognitive domains sensitive to age or mild cognitive impairment (MCI). 13 Executive function is also a crucial domain of cognition because it includes problem-solving skills that enable individuals to live independently. 14 Decreased executive function and memory loss are indicators of early-stage dementia and MCI. Additionally, executive function, memory, processing speed, and attention tend to decline with age, unlike vocabulary and language domains. 15 Therefore, investigating the domain-specific effect of exercise is important because each cognition domain may respond differently to walking or MVPA.
Moreover, the design features of walking interventions (e.g., dose of walking, duration of program, walking format, and walking context) may have different impacts on cognitive outcomes. For example, group- vs individual-based walking formats may result in different outcomes. One study found that group-based exercise intervention improved gait variability, which has been linked to better cognition, while individual-based exercise improved physical function. 16 In addition, one meta-analysis found that shorter session times and higher frequency of exercise, including both aerobic and anaerobic, showed the greatest cognitive improvements in older adults with cognitive impairment. 17 Lastly, active control groups may also impact study conclusions or the magnitude of the walking intervention effect observed.
Therefore, the primary purpose of the current systematic review was to synthesize the existing literature on randomized controlled trials (RCTs) regarding the effectiveness of walking interventions on specific cognitive domains in older adults. This review synthesized findings in five cognitive domains, including executive function, memory, processing speed, attention, and general or global cognition. In addition, the current review summarized findings about walking interventions based on key intervention features (i.e., walking type, intensity, time, frequency, duration, format, and context), the target population, measures for cognitions, and the control group.
Methods
This systematic review follows Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) protocols and PRISMA reporting guidelines. 18 This review is registered at PROSPERO (CRD42024539106).
Data Source
PubMed, Embase, and Web of Science databases were searched until 10 May 2023 with no limit on publication date. MeSH terms were identified based on the four key elements: walking, cognition, older adults, and RCT. MeSH terms for “walking” were Fitness Tracker[MeSH], Walking[MeSH], and Nordic Walking[MeSH]. Walking[MeSH] did not include lower hierarchy level MeSH terms (i.e., gait, stair climbing, dependent augmentation, and walking speed) to exclude concepts irrelevant to the research question. MeSH terms for “cognition” included Attention[MeSH]. Cognition[MeSH] did not include lower hierarchy level MeSH terms. MeSH terms for the “older adult” concept were Age[MeSH], Geriatrics[MeSH], Health Services for the Aged[MeSH], Homes for the Aged[MeSH], Housing for the Elderly[MeSH], Retirement[MeSH], and Pensions[MeSH]. MeSH terms for RCT were program evaluation[MeSH], randomized controlled trial [Publication type], and pilot project[MeSH]. In addition to MeSH terms, relevant keywords (e.g., walk, brain health, aging, and intervention) for each element were searched in PubMed Abstract/Title advanced search. The final search term for each electronic database is attached in the supplemental document. The same strategy was used to search for publications in Embase and Web of Science. In addition, we manually searched the reference list of previous systematic reviews about the effectiveness of walking on cognition to include additional articles not identified from the database search.
Study Inclusion and Exclusion Criteria
The Covidence systematic review platform was used to remove duplicate studies. We created a separate list for manually searched articles. Abstract, title, and full-text assessments were conducted based on the following inclusion/exclusion criteria. Inclusion criteria were (1) the target population is older adults or adults aged ≥65 with different levels of cognitive and physical health (e.g., MCI, at risk of dementia, frailty, or healthy); (2) intervention must include a walking component, therefore, interventions that included walking with another component such as a cognitive task or mindfulness practice were also included; (3) intervention outcomes include one or more of the following cognitive domains: executive function, memory, processing speed, attention, and global cognition; (4) experimental study design was RCT; and (5) article was written in English. There was no restriction on intervention duration. Exclusion criteria were (1) target population was older adults clinically diagnosed with ADRD based on the Diagnostic and Statistical Manual of Mental Disorders (DSM5-TR) 19 ; (2) cognitive outcomes were not measured by performance-based neuropsychological outcomes; (3) non-peer-reviewed studies; (4) studies that solely included neuroimaging (e.g., gray or white matter of the brain) or proxy measures of cognitive function (e.g., Brain-Derived Neurotrophic Factor); (5) studies that did not include a control group. Two reviewers, JL and JD, independently screened the title and abstract and conducted a full-text review for eligibility. The third reviewer, C-HY, resolved reviewers’ conflicts.
Data Extraction and Synthesis
The authors JL and JD independently screened searched studies based on the inclusion and exclusion criteria and extracted information on demographics, intervention features, measurements, and main findings (i.e., the walking intervention’s effect on cognition). The information extracted from each manuscript included participant demographics, the walking intervention’s type, intensity, frequency, duration, format, context, the measure used for each cognitive domain examined, and the types of the control group.
Cognitive Outcomes Examined
This study synthesized the effectiveness of walking on cognition based on performance-based neuropsychological tests that target executive function, memory, attention, processing speed, or global cognition. Executive function represents cognitive flexibility that enables goal-directed behavior. 20 Memory is the capacity to preserve information or recall past experiences. 21 Attention occurs when cognitive resources are selectively allocated in a particular environment, and the central nervous system is ready to respond to stimuli. 21 Processing speed is a time requirement to respond to and process information from external stimuli. 22 Global cognition reflects general mental status and can be used as a screening tool for potential cognitive decline and impairment. 23
Risk of Bias (RoB)
The authors JL and JD independently assessed the risk of bias based on the Cochrane Risk of Bias Tool for Randomized Controlled Trials. 24 Conflicts in agreement on RoB were resolved after a discussion between the two authors. The tool provides criteria to assess studies’ RoB based on five domains: random sequence generation, allocation concealment, other bias, blinding of participants and personnel, blinding of outcome assessment, and incomplete outcome data. The overall quality of the study was determined as good (low RoB ratings for all domains), fair (one high or two unclear RoB ratings, but reviewers determined the outcomes were unlikely to be biased), or poor quality (one high or two unclear RoB ratings and reviewers determined the outcomes most likely to be biased).
Results
As shown in Figure 1, 17 studies were included in the final synthesis. Among them, 15 studies were obtained from database searches, and two studies were from manual searches. Table 1 summarizes general information and participant demographics from included studies. PRISMA 2020 flow diagram.
18
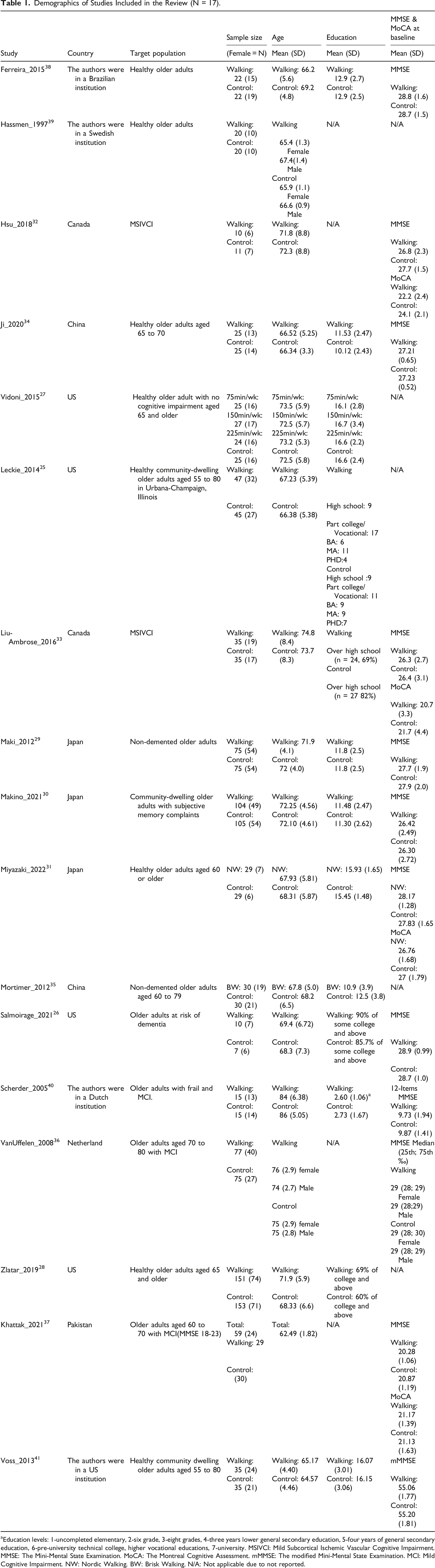
Demographics of Studies Included in the Review (N = 17). aEducation levels: 1-uncompleted elementary, 2-six grade, 3-eight grades, 4-three years lower general secondary education, 5-four years of general secondary education, 6-pre-university technical college, higher vocational educations, 7-university. MSIVCI: Mild Subcortical Ischemic Vascular Cognitive Impairment. MMSE: The Mini-Mental State Examination. MoCA: The Montreal Cognitive Assessment. mMMSE: The modified Mini-Mental State Examination. MCI: Mild Cognitive Impairment. NW: Nordic Walking. BW: Brisk Walking. N/A: Not applicable due to not reported.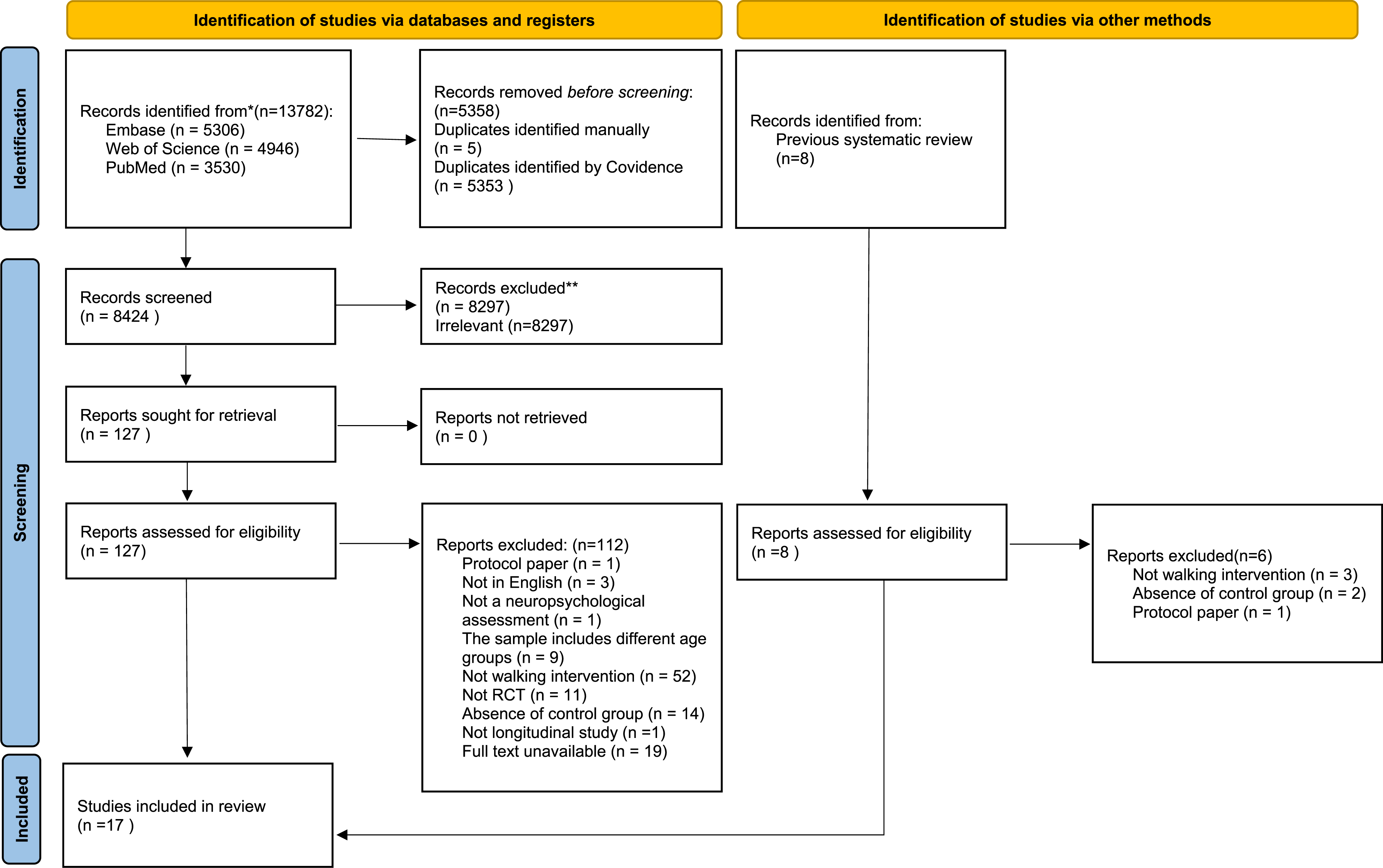
Study Sample Characteristics, Demographics, and RoB Quality Assessment
Studies were conducted in the United States,25-28 Japan,29-31 Canada,32,33 China,34,35 Netherlands, 36 and Pakistan. 37 Four studies did not explicitly mention the country of origin.38-41 The target population’s cognitive conditions mostly included older adults who were healthy,25-28,31,34,35,38,39,41 followed by those who experienced subjective cognitive impairment, 30 had MCI,36,37,40 had mild subcortical ischemic vascular cognitive impairment (MSIVCI),32,33 and were at risk of dementia. 26
This review included 1527 (female = 839 [55%]) older adults, with the study samples ranging from 21 (female = 13 [62%]) 32 to 304 (female = 145 [48%]). 28 The mean age of participants was 70.55 (±8.31) years, ranging from 62.49 (±1.82) 37 to 85 (±5.74) years. 40 Among the 8 studies that reported years of education,27,29-31,34,35,38,41 the mean education level was 13.03 (±3.42) years, ranging from 10.63 (±2.5) years 34 to 16.5 (±2.73) years. 27 Five studies reported education levels in categorical variables,25,26,28,33,40 and four studies did not report participants’ education levels.32,36,37,39 Only one study reported race and ethnicity, which consisted of 94% of White Americans and 2% of Latinos. 26
Summary Table for Intervention Features and Cognitive Outcomes With Assessment Tool by Domains.
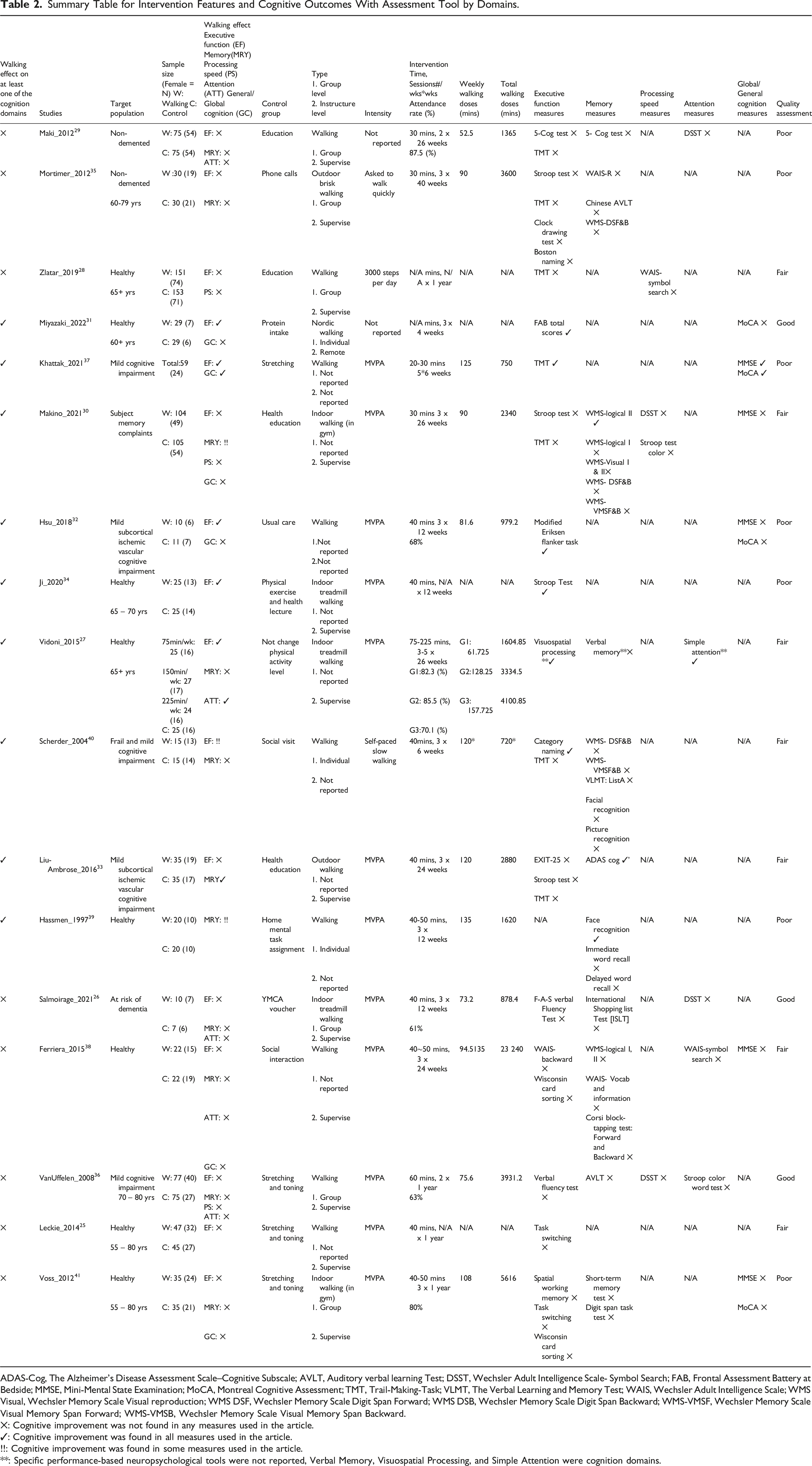
ADAS-Cog, The Alzheimer’s Disease Assessment Scale–Cognitive Subscale; AVLT, Auditory verbal learning Test; DSST, Wechsler Adult Intelligence Scale- Symbol Search; FAB, Frontal Assessment Battery at Bedside; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; TMT, Trail-Making-Task; VLMT, The Verbal Learning and Memory Test; WAIS, Wechsler Adult Intelligence Scale; WMS Visual, Wechsler Memory Scale Visual reproduction; WMS DSF, Wechsler Memory Scale Digit Span Forward; WMS DSB, Wechsler Memory Scale Digit Span Backward; WMS-VMSF, Wechsler Memory Scale Visual Memory Span Forward; WMS-VMSB, Wechsler Memory Scale Visual Memory Span Backward.
✕: Cognitive improvement was not found in any measures used in the article.
✓: Cognitive improvement was found in all measures used in the article.
!!: Cognitive improvement was found in some measures used in the article.
**: Specific performance-based neuropsychological tools were not reported, Verbal Memory, Visuospatial Processing, and Simple Attention were cognition domains.
Walking Features and Adherence
Table 2 presents intervention features, including walking type, intensity, time, frequency, duration, format, and context. Twelve studies focused on walking intensity at a moderate-to-vigorous intensity,25-27,30,32-34,36-39,41 one conducted slow-paced walking, 40 one asked participants to walk quickly, 35 one targeted achieving 3000 steps without a time limit, 28 and one did Nordic walking but did not report intensity. 31 The target range of percentage of Heart Rate Reserve (HRR) for included studies was 60% 34 to 80%, 38 and the Borg Rating of Perceived Exertion (RPE) was 13 to 14 out of 20.37,39 Besides two studies that performed walking for 60 minutes,28,36 walking time per session ranged from 30 minutes29-31,35,37,40 to 40-50 minutes,25,26,32-34,38,39,41 excluding warm-up and cool-down time. One study used goal setting to accomplish walking 75 to 225 minutes per week as an intervention. 27
Walking interventions ranged from a frequency of two29,30,36 to five27,37 sessions per week; two studies did not report walking frequency,25,28 and the most popular frequency was three sessions per week.26,27,31-34,38-41 Intervention duration ranged from four weeks 31 to one year.23,26,34,40 However, the duration for most studies was either 24 to 26 weeks,27,29,30,33,38 followed by 12 weeks.26,34,39 The walking format was mostly group-based,26,28,29,35,36,41 followed by individual-based.31,39,40 The walking context was mostly indoors,26,27,30,34,41 with fewer studies conducted outdoors.33,36 Eight studies did not report walking format,25,27,30,32-34,37,38 and ten studies did not report walking context.25,28,29,31,32,36-40 Only six studies reported walking session attendance rates,26,27,29,32,36,41 with a mean of 75% of sessions completed, ranging from 63% 36 to 87.5%. 29
Control groups varied across the included studies. Seven studies provided health education lectures during the intervention period,26,28-30,32-34 four studies provided a stretching and toning program,25,28,36,37 and two studies provided a social interaction program.38,40 Other miscellaneous control groups were home assignments (mental tasks), 39 protein consumption, 31 regular phone call check-ins from researchers, 35 and no changes in daily physical activity. 27
Outcome Measures of Cognitive Function
More than two studies used the Trail Making Test (TMT) A & B 45 (n = 5),28-30,33,40 Task-switching paradigm 46 (n = 2),25,41 Wisconsin card sorting 47 (n = 2),25,41 and Stroop task 48 (n = 4)30,33-35 to examine executive function. Wechsler memory scale logical 49 was used in two studies.30,38 The Symbol Search (DSST) subtest from the Wechsler Adult Intelligence Scale 50 was used to measure attention26,29 or processing speed.30,36 MMSE (n = 5)30,32,37,38,41 and MoCA (n = 4)31,32,37,41 were used to measure global cognition. See Table 2 for details.
Walking Intervention and Domain-Specific Cognitive Effects
Among the 17 studies, three studies examined only one cognitive domain,25,34,39 five studies examined two domains,28,31,33,35,40 four studies examined three domains,26,27,29,41 and three studies examined four domains.30,36,38 Nine studies (52.94%) found that walking improved at least one cognition domain compared to the control group.27,30-34,37,39,40
Global Cognition
Among the six studies that investigated global cognition,30-32,37,38,41 only one study found that the walking group significantly improved global cognition compared to the stretching group 37 ; see Table 2 for measures. This study recruited older adults with MCI and delivered walking at a moderate-to-vigorous intensity, for 20 to 30 minutes five times per week for six weeks. The walking format and context were not reported. Five studies did not find an effect of walking on global cognition compared to the control group (health education, 30 social interaction, 38 stretching and toning, 41 usual care for MSIVCI, 32 and protein intake 31 ). The walking format was either group-based 41 or individual-based. 31
Executive Functions
Sixteen studies investigated the effect of walking interventions on executive function.25-38,40,41 of these, six studies (37.50%) found that the walking groups significantly improved executive function compared to the control group (health education, 34 social interaction, 40 protein intake, 31 no changes in daily physical activity, 27 usual care for MSIVCI, 32 or stretching and toning 37 ). See Table 2 for measures. The targeted population in these studies was older adults who were generally healthy,27,31,34 with MCI37,40 or MSIVCI. 32 Walking interventions were provided at a moderate-to-vigorous intensity,27,32,34,37 self-determined slow pace, 40 or Nordic walking. 31 The walking time was 20 to 30 minutes,37,40 or 40 to 50 minutes each session.27,32,34 The walking frequency was three times,27,31,32,40 or five times 37 per week. The duration of the walking programs was four weeks, 31 six weeks,37,40 12 weeks,32,34 or 26 weeks. 27 The walking format was individual-based.31,40 The walking context was indoor27,34 or outdoor. 31 In some of these studies, the walking intensity, 31 time, 31 frequency, 34 format,27,32,34,37 or context32,37,40 was not reported.
Ten of the 16 studies (62.5%) did not find a significant effect of walking on executive function compared to control groups (i.e., health education,28-30,33 social interaction, 38 phone calls, 35 receiving a YMCA voucher, 26 stretching and toning25,36,41). The walking format was group-based.26,28,29,35,36,41
Memory
Eleven studies examined memory.26,27,29,30,33,35,36,38-41 Three of these studies (27.27%) reported that walking groups significantly improved memory compared to the control group (health education30,33 or home-based mental task assignment 39 ). See Table 2 for measures. The target population was older adults who were generally healthy, 39 experiencing subjective memory complaints, 30 or with an MSIVCI. 33 Walking was delivered at a moderate-to-vigorous intensity.30,33,39 The walking time was 30 minutes 30 or 40 to 50 minutes.33,39 The frequency of walking was three times per week.30,33,39 The duration of the walking program was 12 weeks, 39 24 weeks, 33 or 26 weeks. 30 The walking format was individual-based. 39 The walking context was either indoor 30 or outdoor. 33 Other studies did not report the walking format30,33 or context. 39
Eight studies did not find an effect of walking on memory compared to control groups (health education, 29 receiving phone calls, 35 social interaction,38,40 receiving a YMCA voucher, 26 no changes in daily physical activity, 27 stretching and toning36,41). The walking format was group-based26,29,35,36,41 or individual-based. 40
Processing Speed
Three studies investigated processing speed, but none found a statistically significant effect of walking on processing speed compared to the control group (i.e., health education,28,30 or stretching and toning 36 ). The walking format was group-based.28,36
Attention
Five studies investigated attention.26,27,30,36,38 One study (20%) found a significant improvement in attention (i.e., simple attention) in three walking groups with different walking doses (i.e., 75, 150, and 225 minutes of walking per week for 26 weeks) compared to the control group (no changes in daily physical activity), 27 despite no dose-response relationship between weekly walking time and processing speed. Four studies did not find a significant effect of walking on attention compared to the control group (social interaction, 38 health education, 29 receiving a YMCA voucher, 26 or stretching and toning 36 ). In these studies, the walking format was group-based.26,29,36
Discussion
The current review synthesized the existing evidence of walking interventions on different domains of cognitive function in older adults. Findings suggest that walking interventions may significantly improve older adults’ cognitive function, especially their executive function and memory. The effective walking interventions were performed for at least 40 minutes each time, at least three times a week, for 6 to 26 weeks, and at a moderate-to-vigorous intensity. These results are aligned with a recent meta-analysis showing that physical activity intervention with sessions lasting 30 minutes 3-4 times per week for 14 to 24 weeks at moderate-to-vigorous intensity demonstrated the largest effect size on executive function and global cognition improvement. 51 However, the domain-specific effects of walking remain unclear due to the heterogeneity of study measures. More consistent reporting of intervention features is required before drawing definitive conclusions.
Physiological mechanisms could potentially underlie the impact of walking on cognition. As walking is a type of physical activity, it is associated with brain structure and function, which are related to cognitive performance. Physical activity is associated with grey matter volume in the hippocampus and prefrontal cortex, 52 and neurons in the brain continue to generate in response to physical activity. 53 Brain molecules including brain-derived neurotrophic factor (BDNF) and insulin-like growth factor 1 (IGF-1) could induce cognition improvement.54,55
Although the findings from our review suggest at least 120 minutes of walking per week at a moderate-to-vigorous intensity confers cognitive benefits, relatively unhealthy older adults may still obtain benefits with less time or a lower walking intensity and volume. For example, older adults experiencing subjective memory complaints showed significant memory benefits (i.e., Wechsler memory scale-logical II) with 90 minutes of walking per week at a moderate-to-vigorous intensity for 26 weeks. 30 Frail older adults with MCI who were unable to walk independently may experience improvements in executive function after participating in slow-paced walking. 40
This review showed that walking interventions had mixed benefits for cognition as two of the four studies that included measures of both executive function and memory demonstrated improvements exclusively in memory,30,33 while the other two showed improvements exclusively in executive function.27,40 Although declining memory and executive functions are sensitive to aging, this result suggests that the impact of walking interventions on executive function and memory may not be equivalent. Previous studies support this; for example, aerobic exercise selectively improved cognitive domains, 56 and working memory improvement did not transfer to improvement in executive function, 57 although they were highly associated. 58 However, the differences in walking intervention features across those four studies and the small number of studies limit the ability to determine which cognition domains are most sensitive to walking.
The current review suggests that cognitive benefits in attention/processing speed may manifest at a lower dose than required for executive function or memory enhancement because 25 minutes of walking performed at a moderate-to-vigorous intensity three times per week demonstrated improvement. However, this interpretation should be taken cautiously because only one study in the current review showed the effect of walking intervention on attention or processing speed.
A previous meta-analysis reported the optimum intensity to be moderate (796–851 METs-min/week) for 60 minutes three times a week for walking interventions to increase global cognition. 12 In the current review, one study that delivered 30 minutes of walking five times per week found an improvement in global cognition. 37 However, the maximum walking dose of the rest of the studies included in this review was less than 60 minutes, three times a week, which means that higher doses may be required to produce global and general cognition benefits.
There are indications that physical activity interventions of 6 months to one year can increase gray matter volume in the hippocampus and prefrontal cortex 52 ; however, the current review does not support the conclusion that year-long physical activity interventions improve cognition when measured using performance-based cognitive assessments in RCTs. The lack of significant cognitive improvements with physical interventions in these RCTs may reflect the nature of the control groups selected for the studies. In some of these studies, active control groups received stretching and toning or social interaction activities. It is possible that stretching and toning may have increased the physical activity of the participants, and thus impacted cognition 59 ; the potential that even this low-physical activity could improve cognition is highlighted by the lack of data on participants’ baseline physical activity in most of the included studies. Thus, if both the physical activity intervention and the control group improve cognitive function, the trials would not demonstrate a comparative improvement for the experimental interventions.
In fact, one study included in this review found that the social interaction group outperformed the walking group on memory tests. 38 Social interaction has been shown to positively influence processing speed, memory binding, 60 and buffer general cognitive decline, 61 which makes it a questionable control group to isolate the cognitive benefits of a walking intervention. However, the benefit of group-based walking is unclear in the current review. This may suggest that simply applying a group-based intervention or walking program does not necessarily promote social interactions. Therefore, the walking sessions might incorporate an active social interaction component to benefit cognition. Nevertheless, a previous study showed that an individual-based intervention applying walking training with cognitive tasks was superior to a group-based walking intervention on self-reported cognitive well-being in older adults recovered from COVID-19. 62 For future walking interventions, the impact of delivery format (e.g., group or individual format) should be investigated because these factors may amplify or regulate the intervention effect.
When studying cognitive health in older adults, several risk factors are present, such as insufficient aerobic physical activity, cigarette smoking, excessive alcohol use, obesity, hypertension, diabetes, depression, and hearing loss, that may confound the intervention effect.63,64 However, only five studies in the current review considered these confounding risk factors in the analysis, including body composition, 31 walking speed, 35 activity level, 36 blood pressure, and physical performance. 28 Participants’ baseline activity level is critical to determining the cognitive benefit of walking interventions. It is possible that inactive older adults would experience greater cognitive benefits than active older adults. Unfortunately, this information was not included in the analysis of all reviewed studies. Future studies should incorporate measures of these risk factors to assess the effect of walking interventions on cognitive health rigorously.
Most studies (n = 11) did not report intervention attendance or adherence rates, making it unclear whether participants received a total intended dose of the planned walking interventions. We recommend that future studies implement and report standardized experimental protocols to allow clearer comparisons across physical activity and exercise intervention studies. For example, applying the Consolidated Standards of Reporting Trials (CONSORT) for behavioral medicine-specific guidelines could be beneficial. 65 These guidelines emphasize five key intervention components to be reported, including training and supervision of treatment providers, treatment allegiance or preference of both patients and providers, manner of testing, success of treatment delivery by the provider, and monitoring and reporting of treatment adherence.
Future studies should utilize device-based measures, such as accelerometers, to collect more accurate walking doses and ensure intervention fidelity. They should also consider real-time measurement techniques, such as ecological momentary assessment (EMA), to explore the time-sensitive associations between walking and cognitive function. 66 Studies in the current review measured cognitive outcomes cross-sectionally with sparse follow-up intervals. Given that cognitive function fluctuates on a momentary level, 67 measuring cognition sparsely may not capture the potential acute effect of walking. 68
Although the current review includes studies conducted worldwide, the racial and ethnic groups within the studies were mostly unreported. This information is particularly important in the US due to known disparities in dementia prevalence across different race/ethnicity groups. 69 Investigating the differential impact of walking on cognitive function by racial and ethnic groups may provide more nuanced insights for developing culturally tailored walking interventions.
Strengths and Limitations
Unlike previous reviews investigating the effect of aerobic exercise, which encompass various types of physical activities, the current review’s strength is its narrow concentration on walking interventions appropriate for most older adults. Further, our study examines specific cognitive domains, which may be more sensitive to walking interventions, rather than focusing on general cognition. This review also provides information on the comparison conditions and the intervention delivery settings to provide a more nuanced understanding of the potential impact of the intervention design features on the study results. While previous studies investigate the optimum weekly physical activity dose for improving cognition,12,70 this review contributes to the literature by investigating the total walking intervention duration. Additional research is required to establish recommendations for intervals longer than a week (e.g., monthly dose).
This study also had limitations. First, language bias may exist in the review as aging research has been rapidly growing globally. 71 Studies published in a language other than English were excluded and thus did not inform these conclusions. Second, we were unable to conduct the meta-analysis due to the heterogeneity of intervention designs, differences in measurement tools, and the lack of reported effect sizes in the included studies. For a similar reason, we were unable to conduct formal statistical analysis to study the relative impact of the walking intervention across cognitive domains. Thus, the clinical significance of the walking intervention could not be determined. Third, our review only included performance-based cognitive assessments and did not cover other neuroimaging measures that may reflect observed changes in cognitive function. While these direct measures of brain activity and structural changes are valuable objective measures of cognitive health, it remains challenging to disentangle which specific cognitive domains correspond to these structural or signal changes in the brain.72-74
Conclusion
This systematic review indicates that walking interventions of at least 40 minutes, performed at a moderate-to-vigorous intensity, three times per week for a duration of 6 to 26 weeks, may improve cognitive function, particularly in executive function and memory domains. Transparent reporting of walking interventions following standard guidelines will facilitate direct comparisons across studies going forward. Comprehensive assessment of cognitive domains in the future will help to further elucidate the domain-specific cognitive benefits of walking interventions in older adults. As walking is the most prevalent form of physical activity for older adults, findings in this area can inform the development of optimal walking programs to maintain cognitive health and reduce the risk of ADRD in aging populations. Physical activity at moderate to vigorous intensity can improve general cognitive functions in older adults. Walking can be a practical solution for common barriers to regular physical activity. However, the benefits of walking on more specific cognition domains sensitive to Alzheimer’s and related dementias were less understood. Walking interventions significantly enhance cognitive health in older adults, particularly in executive function or memory. Each cognitive domain was independently affected by the walking intervention. Some intervention features, such as group-based and a year-long intervention, may not guarantee cognition benefits, while others, such as frequency and intensity, do. Practitioners may consider to incorporate walking as a key intervention for executive function and memory health in older adults, but it should be delivered at least 40 minutes at moderate to vigorous intensity three times per week for 6 to 26 weeks. Future research should focus on standardized reporting of walking interventions.“So What?”
What is Already Known?
What Does This Article Add?
Implications for Health Promotion Practice and Research
Supplemental Material
Supplemental Material - Walking Interventions and Cognitive Health in Older Adults: A Systematic Review of Randomized Controlled Trials
Supplemental Material for Walking Interventions and Cognitive Health in Older Adults: A Systematic Review of Randomized Controlled Trials by Jongwon Lee, Delia West, Christine Pellegrini, Jingkai Wei, Sara Wilcox, Jean Neils-Strunjas, A. Caroline Rudisill, Daniela B. Friedman, David X. Marquez, Jenna Dzwierzynski, Joyce Balls-Berry, Rachelle Gajadhar and Chih-Hsiang Yang in American Journal of Health Promotion
Footnotes
Acknowledgments
The authors acknowledge all project staff and students from the research team for their ongoing time and effort in implementing this study. We also appreciate the help from the University of South Carolina librarian Amy Edwards and undergraduate research assistant Neha Biju in searching keywords and databases. We also appreciate the support from the Center for Disease and Control and Prevention (CDC) and the University of South Carolina’s Prevention Research Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by Cooperative Agreement Number U48DP006401 from the Centers for Disease Control and Prevention (CDC) of the U.S. Department of Health and Human Services (HHS) as part of a financial assistance award totaling $595,099 over two years, with 100% funded by CDC/HHS. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by CDC/HHS, or the U.S. Government.
Data availability statement
All data reported in this study are available upon request
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.