
Abstract
Purpose
To explore perspectives of participants in the WISEWOMAN program in Pennsylvania (PA-WISE) on challenges and facilitators of reducing cardiovascular disease risk as low-income and un-/under-insured middle-aged women.
Approach
Researchers conducted this 2 year qualitative data collection as one component of a broader, 5 year PA-WISE process and outcome evaluation.
Setting
Women from across Pennsylvania, primarily from rural communities.
Participants
Interviewees were low-income, un-/under-insured women aged 40-64 years who had recently participated in PA-WISE-facilitated health coaching and lifestyle programs (HC/LSPs).
Methods – data collection and analysis
Researchers conducted individual telephone interviews with 38 women from four discrete samples of PA-WISE participants at 4 time points. Three researchers used grounded theory, and an iterative process of line-by-line coding, data display, and reanalysis to identify emerging themes, sub-themes, and their relationships.
Results
Participants shared the important benefits of specific PA-WISE program traits. However, participants described significant financial constraints, difficult schedules, caregiving responsibilities, and insufficient social support as persistent challenges in their lives, making lifestyle changes in general, and program participation specifically, difficult.
Conclusion
The challenges that low-income and un-/under-insured women identified amplify the importance of having interventions that offer flexibility, options, and tailoring of supports and resources. The timeless challenges articulated by participants in this study completed just before the COVID-19 pandemic, remain relevant to be addressed through the pandemic and beyond.
Keywords
Purpose
This study was designed to explore perspectives of, and learn from, low-income, un-/under-insured middle-aged women on the challenges and facilitators of reducing cardiovascular disease (CVD) risk through participation in the WISEWOMAN program in Pennsylvania (PA-WISE). Researchers wanted to learn “What affects women’s ability to make lifestyle changes related to managing CVD risks and how does participation in PA-WISE affect this?” in order to inform program quality improvement. Heart disease is the leading cause of death for women in the United States. 1 However since hypertension, the ‘silent killer’, does not usually show symptoms until it causes a heart attack or stroke, women are often unaware of their risks for, and delayed in their diagnosis of, CVD. In 2019, over 300,000 American women died of heart disease, nearly 1 in every 5 female deaths. 1 Middle-aged women may not attend sufficiently to their own health, in particular when they are acting as caregivers (of children and elders) and decision-makers of other family members’ health.2-4 Women of lower socioeconomic status (SES) are more likely to have a high risk of CVD, compared to women of higher SES, due to constraints such as limited or no health insurance coverage, lower health literacy, and less access to health care providers and preventive services.5-9 These women also encounter environmental barriers, which can hinder their ability to adapt to or follow healthy behaviors, including transportation challenges; insufficient time (such as working multiple jobs, taking care of family’s needs before theirs, shift work); lack of access to safe and affordable physical activity programs or facilities; and lack of access to affordable healthy food.2,3,10,11
Approach
WISEWOMAN (Well-Integrated Screening and Evaluation for WOMen Across the Nation), administered through Centers for Disease Control and Prevention (CDC), aims to address low-income un-/underinsured women’s risk for heart disease and stroke by employing various strategies to improve delivery of CVD care and promoting healthy lifestyle changes.12,13 Most WISEWOMAN evaluation studies have been conducted using quantitative methods, thereby missing context and rich detail around “why” and “how” women experience the program.9,10,13-21 Additionally, to our knowledge, there has not been published research on WISEWOMAN participants’ perspectives, (although there has been research on program staff perspectives).22,23 This was a two-year qualitative component of a broader, 5 year PA-WISE process and outcome evaluation, led by the authors as contracted evaluators. The use of telephone interviews allowed us to engage English-speaking individuals from the Eastern half of the state in a time-efficient way, allowing findings to inform program quality improvement efforts. We anticipate that our findings on participant perspectives of engagement in this program may inform delivery of similarly focused interventions.
Setting
In Pennsylvania, as across the U.S.A., heart disease is the leading cause of death for women. From 2015-2019 this accounted for 78,256 women in Pennsylvania. 24 In an effort to reduce CVD risks among socially disadvantaged women, Pennsylvania Department of Health (PA-DOH) applied for and received funding for the WISEWOMAN program in 2008.12,13 The Pennsylvania WISEWOMAN program (PA-WISE) serves un- and under-insured women, aged 40-64 years, living below 250% of the federal poverty guideline by providing: (1) free access to CVD risk screenings and evaluation for CVD medications; (2) risk reduction and smoking cessation counseling; (3) opportunities for Health Coaching – A New Leaf (HC) and Lifestyle Programs (LSPs) designed to prevent, delay, or control CVD and other chronic diseases; and 4) referrals to other free or low-cost community resources.12-14,22 The PA-WISE strategies reflect many of those highlighted in the 2020 Surgeon General’s Call to Action to Control Hypertension, including increasing awareness of the health risks of uncontrolled hypertension, promoting the use of health care teams to manage hypertension, promoting links between clinical services and community programs, and eliminating disparities in the treatment and control of hypertension. 25
Participants
Sample of Characteristics of PA-WISE Clients. a

aData was captured January 2017. The figures in the table are rounded off. Percentages are based on the number of non-missing observations for each variable.
bClient readiness was determined according to the Stage of Change Model. 34
Intervention
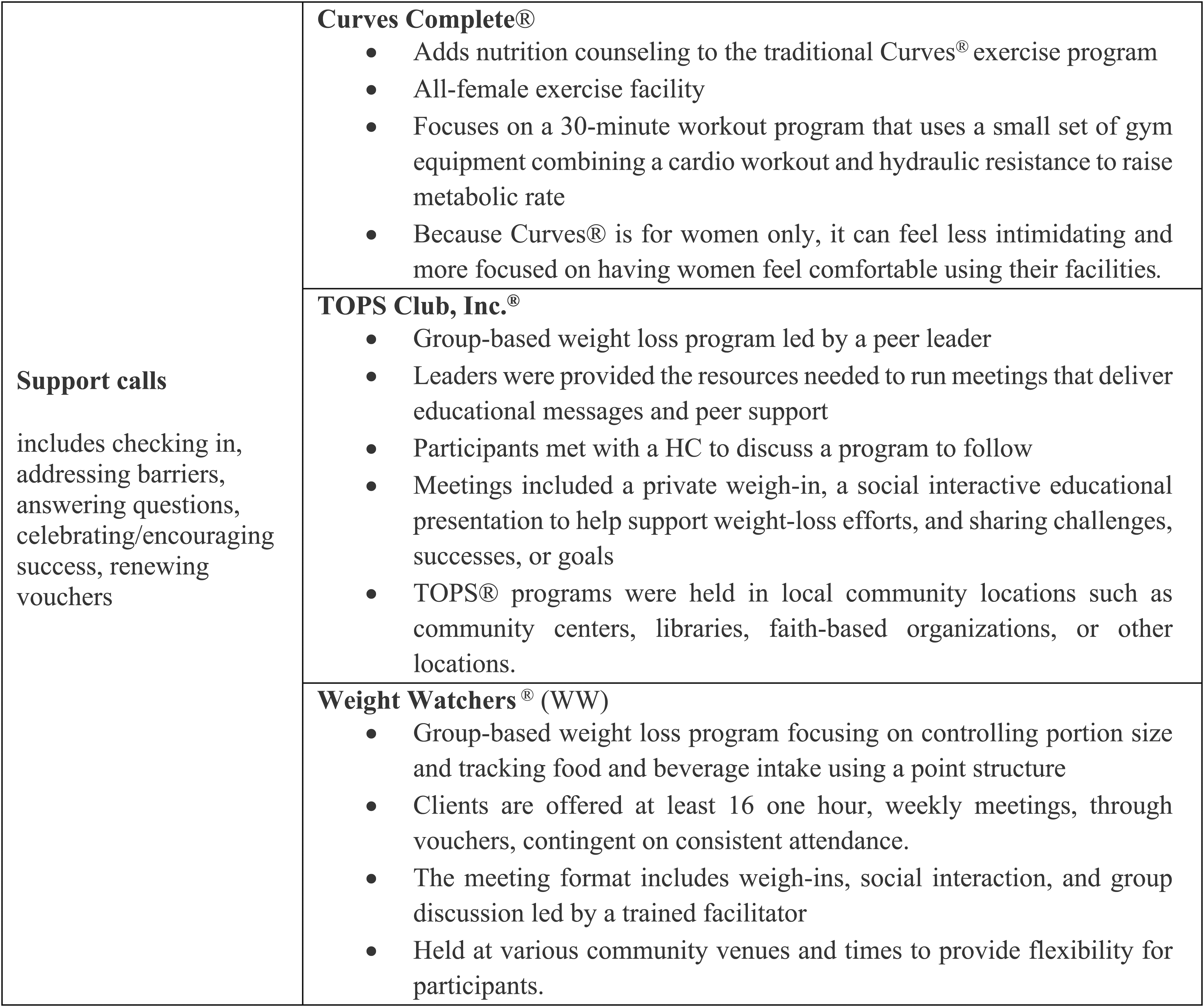
The WISEWOMAN program allowed women who had one or more abnormal results during the CVD risk screening to select a HC/LSP program that aligned with their goals and risk factors. Each clinic offered programs based on program availability and proximity to participants. Women were required by PA-WISE to engage in HC or support calls with health coaches to address their needs and challenges as participants, check in on their attendance and progress, and celebrate successes. Individual or group HC could be combined with a YMCA® membership, YMCA® National Self-Monitoring Blood Pressure, or other options (Figure 1). Support calls were offered with options of Curves Complete®, TOPS (Take Off Pounds Sensibly) Club, Inc®, or Weight Watchers® (Figure 2). Offering a choice of multiple LSPs with either HC or support calls was aimed at facilitating women’s participation by accommodating work and life challenges, transportation barriers, and personal preferences. PA-WISE encouraged participants to attend trial HC/LSP sessions to test the “fit” before committing. PA-WISE Lifestyle Support Program options with health coaching. PA-WISE Lifestyle Support Program (LSP) options with support calls.
The HC that was offered utilized motivational interviewing techniques to assist participants in setting SMART (specific, measurable, achievable, relevant, and time-bound) goals and helping them use problem-solving skills to overcome barriers. 15 HC provides personalized support for participants with limited resources and significant challenges, providing education on reducing CVD risks and living healthier. The LSPs are community-based, evidence-based programs to improve health behaviors associated with CVD risk factors (such as physical inactivity, poor diet, and smoking), with knowledge, skills, and practices.
Past research found WISEWOMAN participation to be associated with lower CVD risks, including controlling blood pressure levels, increasing health behaviors, and reductions in total cholesterol or blood glucose levels.15,17,18,26
Methods
Data Collection
PA-WISE Client Interviews by Recent Participation in LSP Type. a

aInterviewees spoke only of participation in these programs
bTwo clients indicated participation in both HC-YMCA® and Weight Watchers
Data Analysis
Three researchers used grounded theory, and a rigorous, iterative process of line-by-line and thematic coding, data display, and reanalysis to identify emerging themes, sub-themes, and their relationships.19-21 Initial coding was done in rotating pairs of researchers, and subsequent analysis was shared across all three. Participant feedback was shared in the aggregate with the Program at the conclusion of each wave of interviews and analysis to inform their continuous quality improvement efforts. The Institutional Review Board (IRB) at University of Pittsburgh reviewed the study and determined it met federal exemption criteria.
Representative quotes are included throughout this manuscript, as evidence of key findings and occasionally minority perspectives.
Results
Facilitators
PA-WISE participants indicated receiving a wide range of invaluable supports, including financial support to access HC/LSPs, individualized attention, social support, supportive attitudes of providers, flexibility of and diverse options for HC/LSPs, and educational aids from providers.
Financial Support to Access Lifestyle Programs
Participants shared the critical importance of financial support; many women indicated they never could afford to participate in HC/LSPs in the past and could not afford now without the PA-WISE resources. • “I’m very grateful to have come across the WISEWOMAN program… It’s really hard to fall into an insurance category because of my hours at my part-time work, even with two jobs – one doesn’t offer and the other I can’t afford.”
Women also appreciated being able to use vouchers anonymously, protecting their confidentiality, and avoiding the stigma of receiving subsidized admission. • “No one knew I was on a free ticket at the branch I went to.”
Individualized Attention and Social Support
Individualized and motivational support through health coaching or during support calls was beneficial for program participants. Individualized tips and recommendations also helped participants tailor activities to achieve their individual goals. • “She gives me ideas, a boost... She’s gone over my medicines when I’m taking it and how. She talks with me about stress and what affects me, things in my home, my grandchildren.” • “It’s better talking to someone and asking questions, getting into the stress. She is a good pep talk person, makes me feel good, helps get me back on track.”
Participants found social support and connections through group programs like HC-YMCA® and Weight Watchers ®, helping them to maintain their motivation in a community setting. • “There’s a real sense of community there.” • “Knowing that you weren’t the only one trying to achieve a goal.” • “When I walked in, I saw people that looked like me!”
Supportive Attitudes of Providers
All participants indicated feeling supported by clinic staff, expressing appreciation for the welcoming climate of clinics, time and attention, responsiveness, empathy, and non-judgmental approaches. • “Staff were encouraging, kind, and treated me with respect. They didn’t treat me like a charity case… …I was treated with kindness and overall compassion.”
Several women indicated that they were more likely to pursue HC/LSPs because providers spoke with them about their value. • “I probably would not have chosen to do it on my own. But because they put it out there, I did.”
Flexibility and Diversity of Health Coaching and Lifestyle Programs Options
Women shared the importance of the flexibility of the HC/LSPs, flexible times, and evening hours, given their busy and sometimes shifting schedules, in particular spoke of the YMCA® and HC. One participant said having childcare at the YMCA® was critical. • “[The health coach] was very flexible and if we missed a call, she would reschedule no problem.” • “That’s one of the things I love about the YMCA®, that you can go whenever you want and that they have childcare.”
Participating women discussed the importance and benefits of having access to diverse options for LSPs. Those who participated in HC – YMCA® consistently indicated that the range of options at the YMCA® was the best, specifically describing different classes, using workout spaces and equipment, as well as utilizing the services of personal trainers and on-site nutritionists. • “The YMCA
®
had everything. It had classes … a sauna, a pool, and machines. I met with a nutritionist/dietician six times and had three sessions with a personal trainer.” • “[I did] aerobics classes which I loved, a senior class twice a week, and swimming three times a week.”
Having multiple and diverse options was also important for women making the initial decision to participate in HC/LSPs, allowing women to choose one LSP over another depending on their preferences for more individually-focused LSPs or for more group settings, and their past experiences with LSPs. • “I feel better doing stuff on my own, I’m not real good as a group player. I kind of like, I want to be responsible for things myself, I’m not comfortable relaying personal information in a group.”
Educational Aids and Healthy Lifestyle Resources From Providers
Besides receiving intangible support, participants used a wide range of educational aids and resources such as recipes, tips on exercise, pedometers, spices, and salad keepers, to assist them in applying what they learned. • “The health coach has sent me different things like a pedometer, containers, tips on exercise – these are helpful even when I can’t attend Weight Watchers ®.”
Support From Family and Friends
Just over half of participants indicated having support from family, friends, or co-workers such as encouragement, sharing healthy food choices, working out together, and, in turn, sharing what they learned in PA-WISE with others (Table 3). • “Yes, I do, everyone is [supportive]. I’m raising my grandson - my daughter would help with him so I could exercise. My husband was excited about it too, willing to sacrifice time so I could go. Impact of Participation: Information Learned and Applied.

Impact of Participation: Information Learned and Applied
Women spoke about the many things they learned through participating in HC/LSPs including: how types of exercise and diet impact the body, reading food labels, understanding portion sizes, substituting spices for salt, and techniques for smoking cessation. Multiple women discussed changes in their behaviors and outcomes from participation – in particular improving diet and exercise, realizing weight loss, and sharing what they learned with others. Additionally, several women indicated that their increased awareness improved their ability to self-advocate (Table 3).
Challenges
Challenges – The things that made it Difficult to Participate in LSPs.

Women discussed a variety of additional challenges to their participation in HC/LSPs including discomfort with their own bodies, their own motivation, and stress. Some acknowledged giving up because of these challenges, while other women continued despite these challenges and framed their success in part as a matter of will.
Conclusions
This research highlights areas that are key to recruiting and retaining low-income middle-aged women in health improvement programs. Providing diverse HC/LSP options with flexible hours was critical given life’s challenges and preferences for either individual or group support. Unpredictable, full (six days a week) and long (10 hours a day) work schedules, availability of childcare, and caregiving responsibilities (of grandchildren, children, parents, and partners) were barriers to making adequate time for themselves. As in other studies, our findings show that time constraints were the most common and dominant barrier to physical activity for financially disadvantaged middle-aged women.2,3,11,16,27 After taking care of their responsibilities at work and home, many women have limited time and energy, which can impact their attention to healthy eating and exercise. PA-WISE not only helped women take time to care for themselves and learn how to adopt a healthier lifestyle even within challenging constraints but was able to do so in part due to providing options that busy women could access.
PA-WISE supported women in lifestyle change by providing both individual and group-oriented HC/LSP options. Individualized information, given by health coaching, allowed each woman to understand, focus, recall, and apply it in their lives. Our findings align with other studies that have found that tailoring information to individual women’s situations is both practical and more effective in supporting weight loss than general instruction.28,29 On the other hand, social support in a group setting such as Weight Watchers® or the YMCA®, has been shown to be protective and motivating for improving diet and physical activity among low-income overweight women in vulnerable communities. 30 Given that over a third of study participants indicated lacking any social support via friends or family, group-based HC-LSPs enabled women to find encouragement from and connect with others. Having HC-LSPs that were held in local community centers, libraries, and faith-based organizations provided added flexibility and opportunities to connect in familiar spaces. Some women indicated that despite appreciating free access to some LSP programs via PA-WISE, they preferred not to ‘share their business,’ and wanted to avoid ‘stigma,’ so having HC/LSPs that did not differentiate them from their peers who were not getting assistance was important. Offering diverse and flexible HC/LSP options appeared necessary to engaging these disadvantaged women.
Financial assistance was critical as women indicated that access to HC/LSPs was not feasible without financial support. Receiving educational aids and healthy lifestyle resources via PA-WISE also lightened women’s burden of cost for participating in HC/LSPs which may require specific products (such as measuring cups or blood pressure monitors) for participation. Educational aids and resources also directly benefitted participants, helping them act to improve and maintain healthy behaviors, such as using spices instead of salt, measuring blood pressure using a home monitor, bringing healthier food from home using a lunch box, and making lower cholesterol food using recipes. Furthermore, this ensures that women have these items to use after the HC/LSPs have concluded, thereby improving the sustainability of lifestyle changes.
PA−WISE incorporated a diverse range of options for women to receive support, education, and access to physical and dietary programming, as well as providing financial assistance to allow them to participate in that programming. Our findings indicate the importance of having flexible options that allow women to choose intervention approaches that are realistic given their busy lives and diverse needs. Women revealed that as they struggled with financial challenges in particular, PA−WISE allowed them to access supportive health programming they could not have otherwise, and therefore to begin making important lifestyle changes. Public health initiatives that address CVD in socially disadvantaged women could improve effectiveness by tailoring approaches to address women’s social contexts and concerns. 31
Providers’ attitudes and beliefs about women’s ability to change behavior have been identified as key influential factors in women’s changing their behaviors. 32 Our study showed that providers’ supportive and nonjudgmental attitudes were critical to women’s motivation, problem-solving, and lifestyle changes, and this may be especially true for women who lack social support elsewhere in their lives. Women indicated receiving substantial support from clinic staff and health coaches, support that was not available to them outside of PA-WISE.
However, women in the program could not avoid environmental and structural challenges impacting their efforts at lifestyle changes. In our study, financial constraints, challenging schedules, caregiving responsibilities, and transportation difficulties (cost, distance to food, and exercise options) were identified as presenting significant barriers to self-care. Many women were impacted by low-wage employment (which led to holding multiple jobs, fatigue, and time constraints), lack of affordable insurance (which impacted getting preventive care and available financial resources), and low-resourced communities without accessible healthy food and exercise options. These challenges have been consistently shown to be significant for low-income overweight women.2,3,10,11,28 PA-WISE has assisted low-income women with flexible and responsive programming that accommodates the complexity of their lives and acknowledges individual preferences. That many program participants opt out of a ‘readiness’ screening may reflect that these women do not see their own personal ‘readiness’ as a primary issue given their significant life challenges. Further work exploring this could be of value.
We acknowledge that there are limitations to this research. Selection bias for the study is presumed, as responses may have differed from women who opted not to be interviewed. The sampling method selected only women who spoke English and who had participated in at least two HC or LSP sessions but did not account for the fact that some women had participated in more sessions or more than one program. Since PA-WISE clinics were located largely in rural and suburban areas, findings do not necessarily reflect the perspectives of low-income women in more urban environments. We also learned that women did not distinguish differences between support calls and HC, so any distinctions between women’s experiences of these were not captured. Furthermore, the number of women interviewed was small and although their feedback was rich and detailed, for purposes of anonymity we were not able to capture details about their specific geographic location. We cannot know differences in responses by regions, where built resources and programming may differ significantly. However, the analysis was robust and thematic saturation was achieved in each subset of interviews, and we are confident that our findings overall reflect the diversity of participant perspectives.
Listening to their experiences reminds us how complex changing these women’s lifestyles is, as it is related to underlying multiple socioecological factors. Incorporating their perspectives can assist in the development of relevant and practical strategies to serve them.
In addition, materials demonstrating how to prioritize daily activities and self-care may help more women imagine how to adopt a healthier lifestyle even within challenging constraints.
The challenges identified by women in PA-WISE are timeless, and no less relevant because of the COVID-19 pandemic. Indeed, serving women eligible for PA-WISE is ever-important as we face novel threats to health and attendant accumulating health debt. The CDC recently updated the list of certain medical conditions that put people at higher risk of getting very sick from COVID-19 to include physical inactivity, common to women in PA-WISE.
33
Finally, some of the health infrastructures made common during the pandemic (eg telehealth) may further enhance providers’ ability to serve and offer support to these busy women. WISEWOMAN evaluation studies have largely utilized quantitative methods and focused on clinical outcomes. This qualitative study explores perspectives of low-income women on making healthy lifestyle changes while navigating significant, complex life challenges and engagement with PA-WISE. The complex challenges that low-income, middle-aged women face are both structural and personal: low wages; lack of time, transportation, and affordable insurance; insufficient access to healthy food; caregiving responsibilities; and fatigue. Providing flexible and no-cost lifestyle program options, as well as consistently supportive and nonjudgmental providers, may be of critical benefit to women’s program engagement and overall health improvement.So What? (Implications for Health Promotion Practitioners and Researchers)
What is already known on this topic?
What does this article add?
What are the implications for health promotion practice or research?
Footnotes
Acknowledgments
The authors would like to gratefully acknowledge all current and prior PADOH staff who worked on implementing the program since 2008 and contributed to data collection and conceptual evaluation discussions. For Program information contact Diane J. Ollivier. PA-WISE Program Director, PA Department of Health, 717.787.5900. The contents of this article reflect the views of the authors who are responsible for the findings presented herein. The contents do not necessarily reflect the official views or policies of the Commonwealth of Pennsylvania at the time of publication. This report does not constitute a standard, specification or regulation.
Author Contributions
Authors have read and followed the ICMJE guidelines on authorship. The authors would like to gratefully acknowledge and thank: (1) All of the women who shared invaluable insight into their lives and experiences that has helped shape the program’s future; (2) the current and former health coaches, clinical staff, and contractors for their time and dedication to program implementation and evaluation; (3) all of the LSP/HC providers who worked with PA-WISE women to take part in healthy lifestyle programs.
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Received funding for evaluation research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The creation of this article was made possible by cooperative agreement DP18-1816 from the Centers for Disease Control and Prevention/Division for Heart Disease and WISEWOMAN program. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the CDC.