
Abstract
Ischemic heart disease (IHD) is a major cause of death for women worldwide, and thus it is important to focus on lifestyle changes to reduce the impact of the disease on women’s everyday lives. Nine women were interviewed using an explorative approach to describe women’s lifestyle changes after being diagnosed with IHD. Three major themes emerged; ‘Heart disease: A life-changing event’, ‘Social life – both inhibiting and promoting lifestyle changes’ and ‘Maintaining changes: An ongoing challenge and a conscious choice’. Ischemic heart disease caused anxiety, and the women strived to find meaning in life after diagnosis. Family had a great impact on the lifestyle changes made and the social aspect of exercise was highlighted as important. Time since onset of disease affected the effort to make lifestyle changes, showing that changes were easier to make immediately after onset but difficult to maintain over time.
Background
Millions of people across the globe are diagnosed with ischemic heart disease (IHD) annually.1–3 For 11.2% of these people, IHD resulted in death in 2011. For those who survive, the impact of IHD increases mortality, anxiety, depression and reduces quality of life.4–8 Over the last decades, the prognosis has improved considerably, due to the introduction of new invasive and medical care, leading to an increasing number of people living with IHD.1–4,9 However, medical care alone is not enough to secure a desirable recovery. Ischemic heart disease is preventable through primary and secondary prevention, and, in people already diagnosed with IHD, tertiary prevention aims to prevent or minimise the consequences of the disease. 10
Ischemic heart disease is associated with lifestyle risk factors such as smoking, nutrition, physical activity, obesity and alcohol intake. These risk factors can be minimised by lifestyle changes. 11 The focus of this study was to explore what motivates women who are diagnosed with IHD to make lifestyle changes. Women are less likely to receive preventive interventions and recommendations, including lifestyle advice, and need to acknowledge the modifiable risk factors in order to follow healthy lifestyle practices and reduce the risk of a recurrence of the disease. 11 Studies indicate that women with IHD often do not make use of or fail to complete existing rehabilitation programmes. This seems to be due to logistical, financial or motivational reasons.12,13 A meta-analysis reported that approximately 40% of eligible patients with a heart disease are enrolled in cardiac rehabilitation (CR) but that generally there is a lower rate of CR utilisation among women than among men. 14 Consequently, women are often diagnosed with more advanced disease, and receive a poorer prognosis.15,16 Nevertheless, studies show that women who participate in and complete CR programmes reduce risk factors such as smoking, inactivity and unhealthy diet, compared to women who do not participate in a rehabilitation programme.17,18 Little is known of what motivates women to make lifestyle changes and their ability to maintain these changes over years. Thus, knowing the benefits of prevention, the aim of this study was to explore how women diagnosed with IHD make lifestyle changes.
Methods
An exploratory qualitative study design was chosen and the analysis was inspired by Malterud’s systematic text condensation. 19
Settings and participants
Nine women diagnosed with IHD participated in the study. Participants were purposively sampled 20 and recruited from an outpatient CR clinic and a department of cardiology at the same larger university hospital during October and November 2013. All participants had been diagnosed with IHD a minimum of one month previously, and were able to understand and speak Danish. The time since diagnosis served to ensure the women had considered or had made lifestyle changes. Palliative patients and patients with cognitive decline were excluded for ethical reasons and for the purpose of generating detailed knowledge.
Participants’ ages, diagnoses, time since onset of disease, attendance at cardiac rehabilitation (CR) and comorbidities.
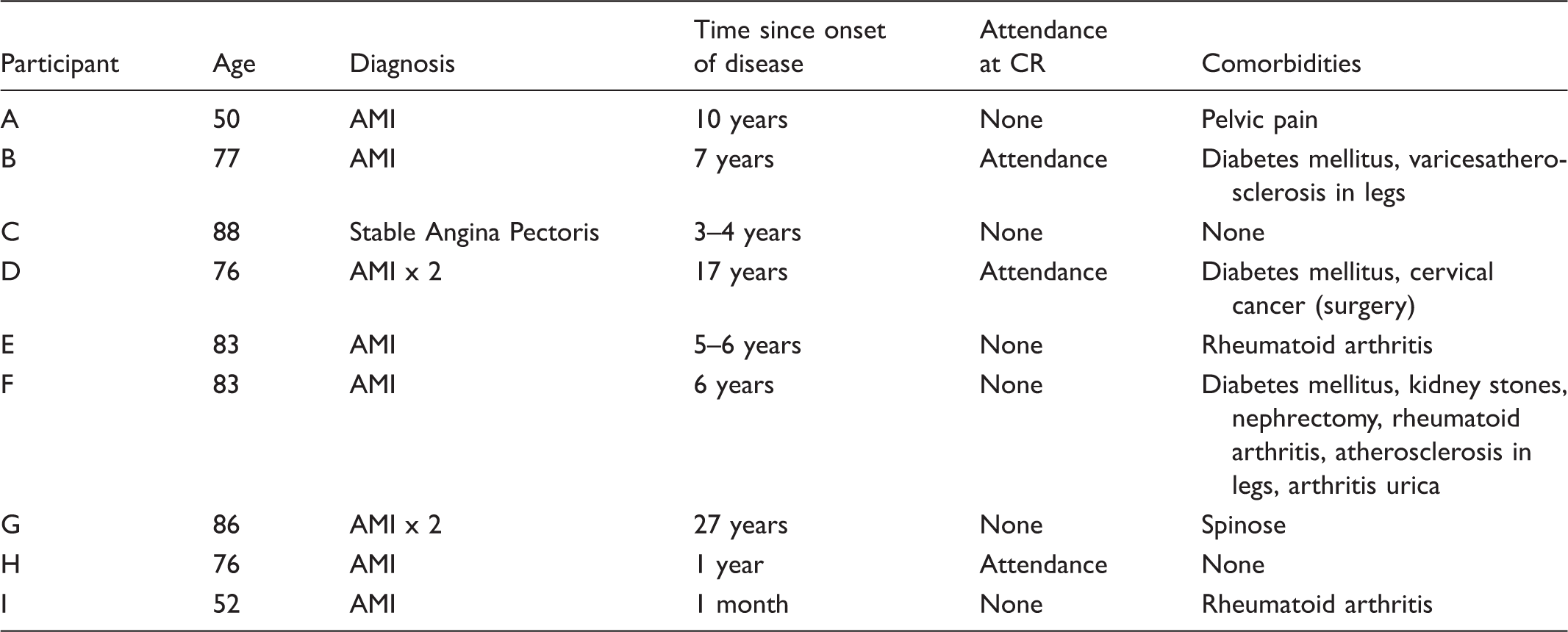
AMI = acute myocardial infarction.
Ethics
An interview study is not classified as biomedical research and thus, according to Danish law, does not need ethical approval. 21 The study followed ethical guidelines for nursing research and the principles outlined in the Declaration of Helsinki.21,22 Participants received both verbal and written information about the study and gave written consent. They were assured that participation was voluntary and that they could withdraw their consent at any time without further explanation. Participants were likewise informed that all data would be anonymised.
Data collection
Data were collected through semi-structured interviews. The interviews took place either in the women’s homes or at the hospital. The first author performed all interviews and an interview guide was used to ensure that all relevant aspects were covered.
The semi-structured interview makes it possible to pursue areas of interest revealed in the interview.19,23 It allows for clarifying questions about the participants’ statements with which data can be validated and data regarding the underlying causes and ideas can be generated. 23 This interview approach is therefore suitable for generating knowledge about the participants’ experiences of making lifestyle changes when living with IHD.
Each interview began with a short introduction, followed by questions relating to the participants’ experiences with lifestyle changes. An example of an opening prompt was: ‘Please tell me what lifestyle changes you have made related to your IHD?’ ‘What has helped you to make change(s) in the way you live your everyday life?’ All interviews were digitally recorded and transcribed verbatim. During the transcription, interviews were made anonymous. The interviews lasted from 17 to 58 minutes.
Data analysis
Data analysis guided by Malterud’s systematic text condensation entails four steps that enable the researcher to get an overview of the research material while keeping the research question in focus. 19 In the first step, the transcribed interviews were carefully read to get an overall sense of the data. At this stage preliminary themes were identified asking what was revealed about the women’s experiences of and motivation for making lifestyle changes. Based on this initial understanding, meaningful parts of the text were highlighted in the second step. We looked for meaning units where the women described their motivation to change lifestyle. The meaning units that revealed the most detailed experiences were systematised, and organised in themes. Malterud calls this step de-contextualisation and meaning units were organised and reorganised until a comprehensive understanding was reached. Then, in the third step of the analysis the themes were unfolded and described in sub-themes that captured all the aspects of the experience of making lifestyle changes following a heart disease revealed in the interviews. Finally, an analytical text for every theme was written and presented in the findings. 19 The first and the last author worked together in the analysis to ensure rigour, to challenge any pre-understanding, and to avoid essential findings being missed.
Findings
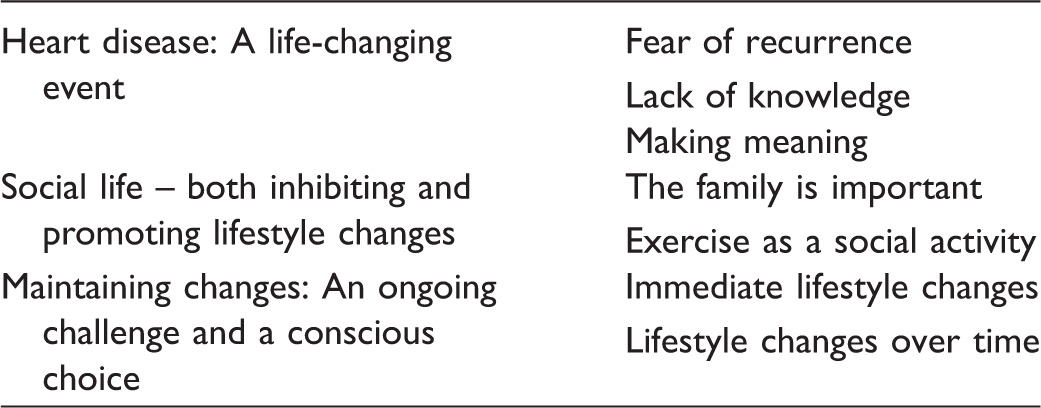
The themes and sub-themes found during analysis.
Heart disease: A life-changing event
Living with IHD had many aspects. In particular, the fear of recurrence was a major issue for the participants, but also the feeling of lacking knowledge about why they became unwell was expressed by participants, and this was closely connected to a profound wish to understand what had happened and why. Some of these aspects helped the women to make lifestyle changes, while others did not.
Fear of recurrence
Fear of relapse and fear of dying was a recurring theme expressed by the women. They expressed being frightened. This was particularly related to the unknown and not knowing whether something was wrong with the heart. … as soon as I feel ill, then the thoughts begin. All the time I have a little fear that there is something. It’s a bit like fearing that there must be something wrong again.… (A) I think more about not being stressed out than I do about eating healthy. It’s not so much that I want to be healthy, but more that I must prevent getting a new blood clot. (A)
Lack of knowledge
Closely related to the fear of relapse, uncertainty about what it meant being diagnosed with ischemic heart disease was evident. Not knowing why they developed the disease and how they should react to it had a negative impact on the lifestyle changes made, even if participants had the desire to change their lifestyle. One woman expressed her uncertainty like this: I wish I could just point at something and say, well, this is what you should do, but I can’t. (B) Overall I think it’s been a little frustrating that there was nothing I could do about it. It’s the feeling that you can do something – you actively do something to ensure that things do not come back.… a lot at times when I am stressed I start to get nervous that something will happen again. And it is not certain that it is caused by stress, but it’s the only thing I’ve been able to grasp. (A)
Making meaning
Several of the women expressed having found peace of mind, meaning and faith in religion or other forms of spirituality regarding their ischemic heart disease. One woman in particular who feared to die, stuck to a promise she had made to God the day she fell ill. To make changes and live a healthier life and 27 years later, she still held that promise. I said, ‘… dear Lord. If I am allowed to live, I will not smoke anymore’. And I did not. Once you have said it, well, then you cannot smoke [again].… I still keep that promise. (G) When I have mellow days, then I think, ‘Ma’am, you cannot just quit!’ I live near a forest. It’s so beautiful with the deer in the winter. They make trenches in my garden and eat my roses. But that’s okay. I also have four great-grandchildren, and indeed I have so much to live for. (F)
Social life – both inhibiting and promoting lifestyle changes
Social relations and the support they offer have a great impact on the ability to succeed in making lifestyle changes. Combining exercise with a social gathering thus promoted the wish to be active. The family in particular, however, had both a negative and positive impact on the women’s actions towards making lifestyle changes. The wish to stay healthy for the family was profound but at the same time a participant’s responsibilities towards the family and worrying about the family could cause her to push her own wellbeing into the background. The impact of social life is described in the following subthemes.
The family is important
Family and loved ones seemed generally to have a positive effect on lifestyle changes. The participants all expressed a wish to be there for the family, to take care of them and not leave them in the lurch. This wish influenced whether they managed to make lifestyle changes or not. One woman explained how the thought of not being there for her children helped her to maintain a healthy lifestyle: I will certainly be there for them. They do not have a father who can take care of them, so that should simply not happen to me. (A) When I need to buy cream cheese, then, without thinking about it, I’ll grab the low fat variant. It may well be that it’s something I’ve been thinking more about after that time. It is I who have chosen the products, and it’s ingrained in my husband too; when he goes shopping, he takes the lean beef because he knows that is what we normally do. (A) We have a son who is schizophrenic, and he was very ill at the time. It was a lot to handle while I was sick myself, so it has also meant that our life has been tough for the last two years. Both of us were worn out and then it becomes more difficult to get going again. (H)
Exercise as a social activity
In general, the women expressed a willingness and desire to begin exercising to improve their health. However, the majority of the women found it extremely difficult and, for some, even impossible to begin exercising, if there was no one they could exercise with: I feel that I needed someone to help me get started. You have to have someone along with you otherwise it will not happen. Of course I think… now you need to go for a walk and exercise a little. (B) It was actually very good to be part of, because it was like they expected that you would come, so you did. (H)
Maintaining changes: An ongoing challenge and a conscious choice
As time went by the women’s ability to make lifestyle changes was challenged. They described it as easiest to make changes immediately after the onset of the ischemic heart disease, whereas after some time it became more difficult to maintain or make additional lifestyle changes.
Immediate lifestyle changes
The immediate lifestyle changes made were to get rid of habits that evidently would endanger their health. They were generally initiated by the shock that most women felt when they unexpectedly found themselves with a heart disease. I stopped smoking the day I was admitted to hospital, and I have not touched a cigarette since. It was my revelation, I was simply afraid. I found it easy to quit, but I also think it was because I was afraid. Had I not been scared, I am convinced that I would have continued to smoke. When fear becomes greater than the need, then you should probably quit. I was not ready to die. I was afraid to die; I wanted to live. (B)
Lifestyle changes over time
Making lifestyle changes was experienced as very difficult. It was a conscious choice and took great effort. It was especially hard to change dietary habits. Several of the women tried for years to change their diet: I know very well what it takes. I have to force myself to do it and then get it going, but it’s not easy. I really do not get started. (B) It has to do with lifestyle and change of lifestyles, and it’s just a little difficult when you’re older. Gradually the character becomes a little frayed; you have to keep up with it and you have to go on. The onset of the disease helps to make immediate changes, but gradually, the old habits return. (D) I daresay that it is a little laziness; it’s easier to keep up the habits you’ve always had. Sometimes I really feel guilty and sometimes I say, you only live once and you’ll eat it anyway. (G)
The women were challenged in maintaining changes and often they returned to old habits. This was also the case for one participant who managed to lose weight at a course at Weight Watchers but slowly gained weight again afterwards.
Discussion
The purpose of this study was to gain insight into women’s experiences of making lifestyle changes after a diagnosis of IHD. Semi-structured interviews served to gain in-depth knowledge of what the participants experienced and learned in relation to making lifestyle changes. The interviews, however different in length, were generally detailed and contained descriptions of the efforts to make and maintain lifestyle changes, both immediately and in the long term. The shortest interview lasted only 17 minutes and was conducted with the participant who had only been diagnosed with IHD for a month. It was included as it was considered to contribute and supplement the variation of data. According to Kvale and Brinkmann, shorter focused interviews can also entail rich and detailed data. 23 The participants varied in age and time since diagnosis, thus reflecting variation. The participants were all recruited through the hospital, and thus may not be representative in a broader sense. However, by comparing and contrasting the findings from this study with other studies, the conclusions from this study seem to support the existing knowledge, adding details of both initial and long-term obstacles to making lifestyle changes following IHD and may be transferable to other comparable settings.
The use of Malterud’s systematic text condensation was considered a strength in this study as it can be applied without having a theoretical framework, thus allowing the researcher to be explorative. The stepwise approach provides a framework for a systematic analysis of data but at the same time can be a limitation if it interferes with the creative process. This issue was anticipated by having two authors working independently on the analysis and then discussing the findings together. 19
Issues of lifestyle changes in women with ischemic heart disease
The aim of this study was to explore how women diagnosed with IHD manage to make lifestyle changes and what motivates them to make and maintain changes. The findings revealed that both by inner psychological reactions and personal resources and other conditions, depending on family matters and the rehabilitation offered in the community, influence what changes are made, when they are made and to what extent they are maintained. Most striking was that the women remained insecure about what had happened and why. They continuously sought an explanation for why they developed IHD in the first place. When the occurrence of the disease could not be directly related to lifestyle it affected their motivation negatively.
For the majority of the women in this study, IHD triggered a crisis or slight shock reaction. One main theme was that the women were and still are afraid to die. The findings reveal how the fear that new symptoms will appear continued to be a worry in their everyday lives. The initial crisis helped the women maintain the energy to fight the threat to their future health, and in that sense, fear worked as a motivation for lifestyle changes. One distinct action was the decision to quit smoking immediately. Nevertheless, this might be explained by the fact that smoking is the most commonly known risk factor for developing cardiac diseases.10,24,25 The participants also expressed an overarching fear of recurring heart disease. The findings revealed an ongoing and ever-present fear that something could go wrong again, even several years after diagnosis. This fear served as a motivating factor for making and sustaining lifestyle changes. This is contrary to Moore et al., who found that women who had had a heart attack did not wonder or worry about the disease when they were asymptomatic. 26 The findings are, however, similar to those found by Sjöström-Strand et al. 7 They found that women continued to fear what the future would bring five years after an AMI. The women wanted to live, but at the same time they experienced an altered sensation and perception of themselves and their bodies. The women from the same study also experienced being worried about developing another case of AMI, which was experienced as very stressful. 7 The women in our study experienced anxiety as constantly present, even if they did not have any symptoms from the disease. This anxiety led several of them to try to maintain a healthy lifestyle, and they expressed a desire for additional lifestyle changes. In this way, fear became a motivating factor in making lifestyle changes. This finding is consistent with one of the themes presented by Moore et al., who also found fear of relapse to be a motivating factor. 26 In contrast to this, a Norwegian study from 2009 found that patients with AMI had higher levels of anxiety right after being diagnosed, but that after 3–18 months their level of anxiety was no higher than that of the Norwegian reference population. 27 This could explain why lifestyle changes for some of the women were easier at first, immediately after being diagnosed but demanded greater effort later on. Fear is a motivator to avoid having another AMI, but when the anxiety disappears, the motivational need for lifestyle changes disappears as well, and the women go back to living as they did before.
In conjunction with this anxiety, many women felt the need to find meaning. Astin et al. found that managing lifestyle changes to improve health was one small part of a changed health status and was not always a priority. 28 Instead attention was focussed on bigger life decisions such as working life and social life. 28 This also seemed to be the case for some of the women in the present study. They decided to focus on the positive aspects of life such as family, nature and, for some, religion. Faith and finding meaning after surviving a crisis contributed to the accomplishment of making lifestyle changes immediately after the heart disease. In particular, it was the main reason for a lasting and sudden decision to quit actions known to be potentially harmful. They experienced a situation in which worsening of their disease and, in the worst case, death, could be the final consequence and this was something which seemed to motivate lifestyle change.
Another important finding is support from the family. Support from the family after a heart attack is invaluable and necessary for successfully changing one’s lifestyle and discontinuing harmful actions. Other studies supported this finding, and found that support from family and friends is especially important if one is to change one’s lifestyle and maintain lifestyle changes that have already been made.29,30,31 Furthermore, support from professionals is necessary during the first year after AMI, and in some cases even longer.7,30 However, family can also have the opposite effect on the ability to make lifestyle changes. Other problems or considerations in the family often affect women to such an extent that they do not manage to keep the focus on themselves and their lifestyle. In our study, one woman was highly affected by the fact that her son was ill at the same time that she received the diagnosis of IHD, making it more difficult for her to change her lifestyle immediately. Wagner found that women often prioritise family responsibilities over their own health, and that women can feel a sense of guilt if they cannot live up to the roles set by others and themselves. 18 Other studies also found that recovery after heart disease can be problematic for women because they want to save others from trouble and preserve their role in the family.32–33
Not only does the family have a great role in supporting women in making lifestyle changes. Another important finding in this study is that socialising as part of exercising has a great impact on the likelihood of the women to exercise regularly. The women clearly expressed that sticking to a healthy lifestyle works best with others. It is particularly motivating to exercise with others, and it seems evident that the women benefit from participating in a rehabilitation programme with others. The need for fellowship in training is similar in the general population, in which more and more people attend fitness centres together. Wagner found the same positive results in their study. 18 Their findings also suggest that women who participate in a rehabilitation programme generally have more success in reducing risk factors than women who do not participate.
This study underlines the fact that the multifaceted reasons for developing IHD have an impact on women’s ability to make appropriate lifestyle changes. The fact that it is not possible for the individual woman to identify the exact reason for the occurrence of IHD, and thereby propose targeted preventive actions towards recurrence of the disease has an impact on her ability and motivation to act accordingly. It is important that healthcare professionals use this knowledge to individualise the information and guidance that are given. Based on the discussion it may be suggested that this information should be repeated over time. Likewise, it is suggested that healthcare professionals take a greater responsibility for finding appropriate rehabilitation programmes based on an individual assessment of the woman’s life circumstances, needs and wishes.
Conclusion
Our study illuminates how women diagnosed with IHD experience making lifestyle changes. Overall, the women feared falling ill again which motivated them to make and initially maintain lifestyle changes such as eating healthily, exercising and quitting smoking. Not knowing why they developed IHD or how to prevent a relapse affected their ability to act according to recommendations and left the women with uncertainty. The family played an important part and affected the women’s preventive behaviour both negatively and positively. Exercising with others was an important motivation highlighting the need for having group offers in cardiac rehabilitation. Time since the diagnosis turned out to be essential when making lifestyle changes. Initial changes being the easiest whereas maintaining changes in the long term turned out to be challenging.
This study has found several aspects and concerns that are important to address to improve the care of women after a diagnosis of IHD. The findings highlight many aspects of the motivation to change and maintain lifestyle changes. Women need individual guidance on how to make appropriate lifestyle changes such as healthy eating and support on how to live a more active life. Even more important, they need help maintaining these changes as it can be difficult not to pick up old habits.
Footnotes
Acknowledgments
The authors wish to thank the women who participated in the study and shared their life experience in relation to lifestyle changes after an IHD diagnosis.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.