
Abstract
Objective
This study aimed to systematically review and analyse intervention programs in a school context centred on the family, focused on increasing youths' physical activity.
Data source
The research was carried out in the PubMed, Scopus and Web of Science databases.
Study inclusion criteria
Studies were included if participants were children or adolescents, focusing on school-based intervention studies with parental involvement and physical activity, sedentary behaviour or physical fitness outcomes.
Data extraction
The search was performed according to the PRISMA protocol. A total of 416 articles were identified. After being considered for eligibility and duplicates, 22 studies were identified as relevant for inclusion.
Data synthesis
Sample and intervention characteristics, objective, the role of the family, outcomes measures, main findings regarding the outcomes and risk of bias.
Results
Ten studies reported improvements in physical activity, 6 in sedentary behaviour and 9 in the components of physical fitness and/or skills related to healthy behaviours and lifestyles. Most of the interventions adopted a multidisciplinary and multi-component approach.
Conclusions
Most interventions employed a school’s multidisciplinary/multi-component approach to promoting physical activity, nutrition, and general education for healthier lifestyle behaviours. The impact of school-based interventions involving families on youth’s physical activity levels is still a relatively emerging theme. Further research is needed given the diversity of the intervention’s characteristics and the disparity in the results’ efficacy.
Objective
Implementing health behaviours, such as physical activity, should be established as soon as possible in the life cycle. Thus, promoting physical activity should be consistent throughout childhood and adolescence. Due to the significant amount of time children and adolescents spend at school, this setting has been considered a key opportunity for nearly all school-aged children and adolescents to access health-enhancing physical activity.1,2 Although increasing evidence suggests that schools can play an important role in promoting active lifestyles, there is also evidence stating that the effects are generally short-lived.3-6 In fact, it is still unclear which factors influence the effectiveness of interventions for promoting medium- and long-term healthy behaviours, such as physical activity engagement.7,8 Thus, there is still a need to understand better what aspects of the social and built environment are associated with physical activity participation since these are critical but less explored factors to consider in designing successful physical activity programs in the school setting.
Family involvement may play a fundamental role in adopting and maintaining active lifestyles that cannot be ignored in the school setting when considering children and adolescents.9,10 Multidisciplinary interventions in the school setting involving the school community and students’ families have the potential to promote physical activity and healthy lifestyles among children, adolescents, and their relatives.11,12 Family support, encouragement, and the availability to monitor children’s physical activity are critical factors that influence children and adolescents attitude towards physical activity.13-15 Furthermore, some evidence suggests that physical activity interventions integrating the family lead to longer-lasting effects. Even within interventions incorporating the family, those where parents participate directly and regularly in the activities show better results when compared to interventions where parents participate indirectly.8,16-18
Despite the literature suggesting the beneficial effects of family involvement in school-based physical activity interventions, there is still no systematized evidence on how family interventions influence children and adolescents' physical activity levels. Thus, the objective of this study was to systematically review the effects of school-based interventions involving the family in promoting physical activity and/or reducing sedentary behaviour among children and adolescents to understand its effects better. Also, this systematic review will allow physical education and general education professionals to identify important factors to consider in developing and implementing physical activity interventions involving the family in the school context.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. 19
Search Strategy
The electronic databases considered in this systematic review were PubMed, Scopus, and Web of Science were searched for relevant records on the 30th of April 2021. The following terms were searched in the title: “physical activity” OR sport* OR exercise OR fitness OR sedentary OR “motor skill* AND school AND intervention* OR program* OR protocol* OR RCT OR “randomized controlled trial” OR experimental AND health*.
Study Selection
Primary source articles published in peer-reviewed scientific journals were considered eligible until the 30th of April 2021. Articles were included in the systematic review if they met the following criteria according to PICOS (participants, intervention, comparison, outcome, study design) guidelines: (1) participants were children, adolescents, and their relatives; (2) school-based intervention studies with parental involvement; (3) any comparison; (4) physical activity, sedentary behaviour, or physical fitness outcomes; and (5) RCT design studies. Duplicated records from the database search were removed. Afterward, the title and abstract were independently screened by 2 authors (FS, HS) for eligibility. A complete reading of the eligible records was carried out to consider inclusion in the systematic review. The same 2 authors reviewed potential studies, and the inclusion and exclusion decisions were made by consensus.
Data Extraction and Harmonization
Two authors (FS, HS) performed data extraction and harmonization using a standardized approach with a consensus. Relevant information extracted included: sample characteristics (number, age, and parents where the study was carried out), study features (duration, main characteristics of the intervention, and how the parents were involved), measures/instruments used (only those that mediate physical activity and/or sedentary behaviour were considered) and the main results.
Study Quality and Risk of Bias
The Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for
Quantitative studies were used to assess study quality. 20 This instrument has 6 components that consider selection bias, including study design, confounding factors, data collection methods/instruments, whether raters and participants were “blinded”, reports of withdrawals, and dropouts. According to the specific criteria, scores of weak, moderate, or strong were assigned to each category. Study quality was independently assessed by 2 authors (FS, HS). The discrepancies were discussed and decided by agreement.
Results
Study Selection
The flowchart of the study selection process is shown in Figure 1. Through the search carried out in the databases, 416 articles were identified. Of these, 202 were considered for eligibility after duplicates were removed (n=214). A total of 134 studies were eliminated in the title and abstract screening phase. Lastly, the full text of 68 studies was fully assessed, and 22 were elected as relevant for inclusion. Flowchart of the study selection.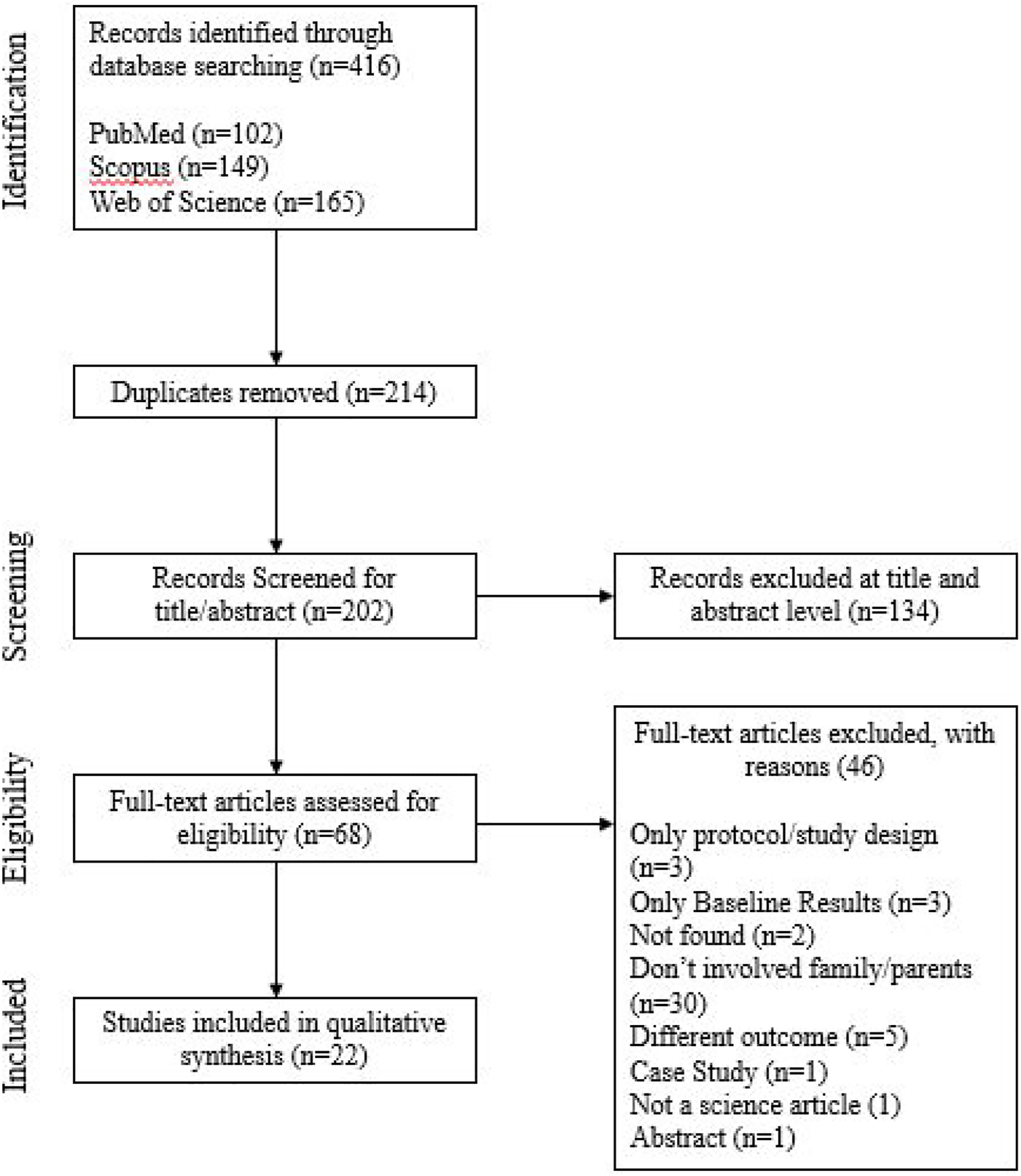
Study Quality and Risk of Bias
Studies Methodological Quality Assessment.

Abbreviation: R, rating of components; F, fair; G, good; P, poor/weak
Intervention Characteristics
Characteristics and Main Results of the Studies Included in The Systematic Review.

Abbreviation: CG, control group; CPAIQ, children PA Item questionnaire; EPAQ, eating and PA questionnaire; GOAL, Guys/Girls Opt for activities for life; healthy youth Places, HYP; HEELP, exercise, eating, and lifestyle; HR, heart rate; HRQol, health-related quality of life; IG, intervention group; LIPA, light physical activity; METs, metabolic equivalent; MVPA, moderate to vigorous physical activity; PA, physical activity; SB, sedentary behaviour; F/S, fitness/skills; PDPAR-24, previous Day PA Recall; PedsQL, Pediatric quality of life Inventory; VPA, vigorous physical activity
Most studies performed a multicomponent approach (n=20), intervening in nutrition education, physical activity, psychological variables, and/or re-education for healthier lifestyle behaviours. In the other 2 studies31,33 the intervention programs focused on promoting physical activity. Also, different forms of family involvement were employed. Half of the studies (n=11)21,23-25,28-30,34,37-39 involved the family through sessions/workshops, in which tools and knowledge about healthy lifestyles were provided. In 8 studies,22,27,32,33,35,40-42 parental involvement focused on carrying out/completing assessment instruments (ie, questionnaires) and/or on participating in some intervention processes (eg self-monitoring; family homework). The other 3 studies26,31,36 contemplated a direct parental involvement in physical activity, where parents performed physical activity with their children.
Main Results
The main results of each study are presented in Table 2. The outcomes considered in this systematic review were organized into 3 components: physical activity, sedentary behaviour, and fitness/skills. Most studies (n=19) showed a positive intervention effect in at least 1 of the outcomes of interest (physical activity, sedentary behaviour, fitness/skills), with only 3 studies22,23,28 not reporting post-intervention improvements. Ten studies reported improvements in physical activity behaviour.25,27,29,30,32,36,37,39,41,42 From those, 4 studies additionally revealed improvements in sedentary behaviour27,36,39,41 and 1 study presented further improvements in sedentary behaviour and fitness/skills. 42 Other 8 studies showed positive effects of the intervention only on fitness/skills.21,24,31,33-35,38,40 Lastly, only 1 study reported improvements solely in sedentary behaviour. 26
Some characteristics of the studies appeared to influence the main results. For example, all the 3 studies that included direct parental involvement in physical activity26,31,36 showed an improvement in 1 or more outcomes. Also, all studies encompassing more than 1 educational level showed a positive effect of the intervention on the outcomes of interest. On the other hand, all interventions targeting children aged 6 years or less22,23 showed no significant impact.
Discussion
This study systematically reviewed the effects of school-based interventions involving the family in promoting physical activity, reducing sedentary behaviour, and improving fitness/skills among children and adolescents. Of the 22 included studies, 19 showed a positive effect in at least 1 of the main outcomes of interest. Most interventions employed a multicomponent approach, integrating physical activity promotion, nutrition education, and general education for healthier lifestyle behaviours. Shorter intervention durations and greater family involvement appeared to be more effective.
Although there is some evidence on the effectiveness of interventions to promote physical activity in the school setting,25,39,41 it is necessary to understand further the factors that support the change and maintenance of healthy behaviours, such as physical activity, in the medium- and long term. In the reviewed studies, we found an association of other areas of intervention with the main purpose of promoting physical activity to enhance the acquisition of different behaviours and skills. Those areas mostly integrate nutrition and the motivational component.23,32,38,40 Multicomponent and multidisciplinary interventions that involve physical activity and combine nutritional education to promote behaviour changes and redefine parenting strategies are considered the main potential components for creating an intervention program.43,44 Psychological variables such as knowledge, motivation, mental well-being, and psychosocial aspects are also sometimes associated with this type of intervention. 45 However, the results are still very incipient, so further studies are needed to understand better the effectiveness and mechanisms of multidisciplinary interventions for physical activity promotion in school contexts involving the family. This is also relevant when sedentary behaviour and fitness/skills outcomes are considered.
Discussing the best way to involve the family in learning and acquiring skills in the school context is not a recent issue.46-49 There is some evidence that the lack of support from family reduces the likelihood that behaviours and skills acquired in the context of regular physical activity will persist over time.50,51 The importance of family involvement in interventions in health and maintenance of more active and healthier lifestyles is widely recognized. Even so, interventions centred on the family have different forms of structuring. While some choose to focus on parents as the sole agents of change, strengthening parents’ leadership skills,52,53 others promote parental support in changing the child’s behaviour, taking responsibility for creating a supportive environment, and empowering children to make informed choices.53,54 Ideally, from a public health perspective, interventions designed based on simultaneous participation and pursuit of goals by the family and children, making commitments to change behaviour together, are the most sustainable.55,56 However, only 3 studies in this review26,31,36 achieve more interactive and direct participation by the family concerning inclusion in the practice of physical activity, with consistent results. Factors such as labour issues, lack of time, or inflexibility of schedules, among others, may justify a certain inability to generate contexts and intervention programs that do not clash with the existing daily routine.50,57,58
In the revised literature, the inclusion of the family in a perspective of control and evaluation of the process, acquisition of skills and knowledge that regulate and encourage physical activity practice occurs mainly through sessions/workshops to transmit knowledge about healthy lifestyles and filling in questionnaires or reports. It appears to be the most used way to promote and generate interventions to increase physical activity levels, both in children and families. Although the literature indicates the importance of parental involvement and the creation of specific conditions in the family context as critical aspects for the success of the interventions,59,60 it has been common to find a high heterogeneity among existing studies, both in methodological terms in intervention strategies. These factors highly limit the results’ applicability and consequently do not provide sufficient evidence to obtain political relevance to support or improve this type of program.61,62
Another important variable to consider in the study’s design and structure is the age and/or school years for which the programs are designed. It seems evident that intervention programs are mainly focused on younger children. The nature of interactions between parents and their children’s school becomes more formal and less frequent after the first few years of schooling. 63 It is also important to realize that the younger the children’s ages, the greater the possibility that the programs will depend on families' involvement in aspects unrelated to the exercise itself, but related to other components such as evaluation processes, filling out questionnaires, and others. On the other hand, as children are getting older, there are many factors to consider, such as more difficulties in changing behaviours and lifestyles more significant number of affordances and behaviours different from those that the programs intended to promote. In addition, when compared to adolescents, younger children may be more flexible in their ability to change behaviours since it is at this stage that they begin to develop self-regulation skills for a healthy life. 64 How Parent and family support tends to peak at age,12,65 and there is a greater tendency for teenagers to become independent in their leisure time and follow influences from their peers. 66 Considering this, and since the results showed that children under 6 years old did not show significant effects in the interventions, it is believed that the ideal interval to develop this type of intervention program would be between the age of 6 years to adolescence.
Regarding the duration of interventions, most studies reviewed have fewer than 3 months (n=10) or are longer than 12 months (n=9). Concerning the motivation and adherence factors of the program’s interventions, short-term interventions have greater effectiveness in physical activity, physical fitness, and/or skills related to healthy behaviours and lifestyles than longer interventions duration. In sedentary behaviour, a similar number of studies showed positive results. The lowest rate of studies analysed lasted 3 to 6 months with manifestly reduced effects on study outcomes. These results can be important indicators of the difficulty of maintaining the positive impact of interventions for more extended periods. Strategies to strengthen the, especially in long-term interventions, are essential factors.
Limitations
The findings of the current systematic review should be interpreted considering some limitations. Although study quality was assessed, studies were not weighted or ranked, nor were any removed from the review. Therefore, studies with poorer quality were given no less importance than findings from studies with greater quality. Furthermore, the studies included presented a variety of instruments for assessing the outcomes. In addition, 1 study did not clarify the family’s role in the intervention programs. 24 It is important to note that only published articles were included in this systematic review. In this way, the publication bias may also be a limitation since there may have been unpublished studies not included due to not having achieved significant results. Finally, there was high heterogeneity among included studies, both in methodological terms and intervention strategies. All these factors lead to difficulties and caution in the comparisons presented. The impact of context constraints on the design of the intervention (eg, locals’ educational policies) and the multidisciplinary approach put a severe challenge to the precision of future intervention implementation (ie, repeatability and reproducibility).
Conclusion
School-based interventions involving the family seem to effectively promote physical activity behaviour, reduce sedentary behaviour, and improve fitness/skills. Successful intervention programs should include a multicomponent and multidisciplinary approach, integrating physical activity promotion, nutrition education, and general education for a healthier lifestyle. Family support increases the likelihood that behaviours and skills acquired in regular physical activity will persist over time. However, few interventions achieve more interactive and direct participation by the family concerning inclusion in physical activity practice. Future interventions should overcome this limitation by integrating participation and pursuit of goals by the family and children simultaneously, making commitments to change behaviour together. Due to the high heterogeneity among studies, both in methodological terms and intervention strategies, more studies are needed to understand better which factors impact the success of the physical activity, sedentary behaviour, and fitness/skills programs. Implications for Health promotion Practitioners and Research There is still no systematized evidence that reports the influence of School-based interventions involving the family on children and adolescents’ physical activity levels. This systematic review provides new information on how physical activity interventions centred on the family at the school can increase physical activity and reduce sedentary behaviour. We considered the level of physical activity, sedentary behaviour, and fitness/skills at the school context as the pillars of this research. Given this three-dimensional scenario, it was possible to identify standardised dynamics concerning how successful interventions should be structured. School-based interventions involving the family seem to effectively promote physical activity behaviour, reduce sedentary behaviour, and improve fitness/skills. This approach requires a multicomponent and multidisciplinary method, integrating physical activity, nutrition education, and general education for a healthier lifestyle. Also, interventions designed based on simultaneous participation and pursuit of goals by the family and children, making commitments to change behaviour together, are the most sustainable.So What?
What is already known on this topic?
What does this article add?
What are the implications for health promotion practise or research?
Footnotes
Author Contributions
Francisco Santos: Formal analysis, Investigation, Writing – Original Draft.
Honorato Sousa: Formal analysis, Investigation, Writing – Original Draft
Élvio Rúbio Gouveia: Conceptualization, Formal analysis, Project administration, Writing – Original Draft
Helder Lopes: Conceptualization, Project administration, Writing – Review and Editing
Miguel Peralta: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Writing – Review & Editing
João Martins: Conceptualization, Methodology, Writing – Review and Editing. Eugenia Murawska-Ciałowicz: Writing – Review and Editing. Grzegorz Żurek: Writing – Review and Editing. Adilson Marques: Conceptualization, Formal analysis, Funding acquisition, Project administration, Writing – Review and Editing
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Education, Audiovisual and Culture Executive Agency (622288-EPP-1-2020-1-PT-SPO-SCP).