
Abstract
The effects of child sexual abuse (CSA) have been found to surpass generations as maternal history of CSA is associated with increased difficulties in sexually abused children. However, little is known about the mechanisms underlying this association. The present study aimed to test maternal mental health symptoms including psychological distress, post-traumatic stress disorder (PTSD) symptoms, and dissociation as mediators of the relationship between maternal CSA and children’s internalizing, externalizing, and dissociation symptoms in a large sample of sexually abused children. A total of 997 sexually abused children aged 3-14 years old and their mothers were recruited at five specialized intervention centers offering services to sexually abused children and their families. The children were divided into two groups depending on their mothers’ self-reported history of CSA. Mothers completed a series of questionnaires assessing their mental health and children’s functioning. Maternal history of CSA was associated with increased maternal psychological distress, PTSD symptoms, and dissociation following children’s disclosure of CSA. In turn, maternal psychological distress and maternal dissociation were associated with increased child internalizing, externalizing, and dissociation symptoms. Maternal PTSD symptoms were associated with child internalizing symptoms. Maternal mental health difficulties mediated the association between maternal CSA and sexually abused children’s maladaptive outcomes. Clinicians should assess for possible history of CSA in mothers of sexually abused children and determine how best to support them to cope with the aftermaths of their child’s disclosure and with their own traumatic past.
Introduction
Child sexual abuse (CSA) is a global problem with worldwide estimates ranging from 8% to 31% for girls and 3% to 17% for boys (Barth et al., 2013). A large body of empirical research indicates that the widespread presence of CSA is concerning as it not only has immediate deleterious effects on the child (e.g., Lewis et al., 2016; Lindert et al., 2014), but it can have harmful far-reaching consequences in adulthood (e.g., Dworkin et al., 2017; Maniglio, 2010), as well as in the next generation of children (e.g., Borelli et al., 2019; Trickett et al., 2011). Previous studies showed that maternal history of CSA is associated with increased risk of sexual abuse in children (Baril & Tourigny, 2015). In addition, victims of CSA whose mothers present a history of CSA have more difficulties following disclosure than victims with nonabused mothers (Berthelot et al., 2012; Trickett et al., 2011). This study aimed to identify potential mechanisms underlying the associations between maternal history of CSA and sexually abused children’s difficulties using a large sample (N = 997) of preschool and school-aged children.
Intergenerational Continuity of CSA
Intergenerational findings demonstrate that mothers who were victims of CSA are more likely to have children who will also be sexually victimized (Baril & Tourigny, 2016; Testa et al., 2011). However, these findings do not suggest that the mother becomes perpetrator, but instead that the trauma experienced by the mother as a result of CSA produces negative outcomes, such as mental health difficulties, which unintentionally create familial environments conducive to violence, thereby increasing children’s risk of abuse (Baril & Tourigny, 2016; Noll et al., 2009; Testa et al., 2011). Consistent with the Complex Post-traumatic Stress model (CPTSD; Courtois & Ford, 2009), CSA is associated with long-term consequences for the victim in terms of psychological and interpersonal functioning (Trickett et al., 2011). Core difficulties include affect dysregulation—a transdiagnostic process involved in many psychopathologies (Aldao et al., 2010)—structural dissociation, somatic dysregulation, impaired self-development, and disorganized attachment patterns (Courtois & Ford, 2009). In line with this conceptual model, empirical findings show increased levels of dissociation (Hillberg et al., 2011), post-traumatic stress disorder (PTSD) symptoms (Dworkin et al., 2017), depression (Maniglio, 2010), substance use (Tonmyr & Shields, 2017), and anxiety (Maniglio, 2013) in adult survivors of CSA.
In addition, some studies have shown that mothers with a history of CSA display more psychological distress following their child’s disclosure of CSA when compared with mothers without a history of CSA (Hiebert-Murphy, 1998; Trickett et al., 2011). Findings from one of our recent studies are in line with this assumption, as we found that mothers affected by dual traumas were at heightened risk of presenting mental health difficulties (dissociation, psychological distress, PTSD symptoms) following their child’s disclosure (Langevin et al., 2020). Although disclosure of CSA from one’s child is distressing for the vast majority of parents, it could also trigger reexperiencing symptoms in mothers with a history of CSA. Unfortunately, the presence of PTSD symptoms and dissociation in CSA survivors have been shown to increase the likelihood of intergenerational continuity of CSA (Baril & Tourigny, 2016; Leifer et al., 2004; Trickett et al., 2011).
A potential explanation is that PTSD symptoms and dissociation, and more generally speaking psychological distress, can create additional challenges that interfere with parenting (i.e., decreased supervision), and can increase risk factors making the child vulnerable to CSA (Baril & Tourigny, 2015; Cort et al., 2011; Noll et al., 2009). For instance, DiLillo and Damashek (2003) indicated that survivors of CSA may be more permissive parents and inconsistently apply disciplinary measures. Collin-Vézina et al. (2005) found that the association between mothers' CSA and parental inconsistencies was mediated by maternal dissociation symptoms. Permissive or inconsistent parenting can result in failure to set appropriate limits and failure to protect (DiLillo & Damashek, 2003; Testa et al., 2011). While nonabusive mothers should not be considered responsible for their child’s victimization, as responsibility always lies with the perpetrators, understanding the maternal factors associated with an increased risk of CSA or worsening the consequences of CSA in the next generation has undeniable value for prevention initiatives.
Maternal CSA and Sexually Abused Children’s Outcomes
Berthelot et al. (2012) found that the mother’s own CSA history was associated with higher externalizing—but not internalizing—symptoms in 115 preschool children victims of CSA. Another study documented more overall behavior problems and poorer functioning in sexually abused children between the ages of 6 and 13 years when their mothers were also victims of CSA (Paredes et al., 2001). A recent study examined the associations between CSA exposure (both mothers’ and children’s) and children’s internalizing and externalizing symptoms in a sample of 111 school-age children (Borelli et al., 2019). Results indicated that in addition to sexually abused children, children with a sexually abused mother, no matter their own victimization status, were at greater risk of presenting internalizing and externalizing symptoms (Borelli et al., 2019). While previous results tend to indicate that a history of CSA in mothers is a risk factor for increased difficulties in sexually abused children, and even in nonabused children (see Bowers & Yehuda, 2016 for a review), the mechanisms behind this association have yet to be determined.
Consequences of CSA
One of the most documented short-term outcomes of CSA is behavior problems. Congruent evidence suggests that child victims of sexual abuse have significantly greater externalizing (i.e., delinquent and aggressive behavior) and internalizing symptoms (i.e., withdrawal, somatic complaints, and anxiety/depression) compared to nonabused children (e.g., Charest et al., 2019; Langevin et al., 2015; Maniglio, 2015). A recent study compared behavior problems in sexually abused youth and maltreated (physical and emotional abuse, and neglect) but nonsexually abused youth and results showed the increased vulnerability of sexually abused children to these difficulties (Lewis et al., 2016).
Another well documented outcome in sexually abused children is their increased dissociation symptoms compared to nonabused children (Bernier et al., 2013; Hébert et al., 2020). Dissociation was defined by Spiegel and Cardena (1991) as “a structured compartmentalization of mental processes (e.g., thoughts, emotions, conation, memory, and identity) that are typically integrated” and is known to have long lasting deleterious consequences on multiple domains of children’s functioning (e.g., school, interpersonal; Silberg, 2014). Consistent with the CPTSD model, other consequences have been documented in sexually abused children (e.g., emotional dysregulation, sleep problems, insecure attachment patterns, somatic complaints; e.g., Charest et al., 2019; Langevin et al., 2019) but given the centrality of behavior problems and dissociation and their deleterious impacts on developmental trajectories (e.g., Colman et al., 2007; Reef et al., 2010), these will be the focus of the current investigation. Notably, a literature review concluded that 10%-53% of sexually abused children do not present difficulties following the abuse (Domhardt et al., 2015). Therefore, it is imperative to understand what are the factors that can exacerbate common difficulties in sexually abused children or rather foster resilience.
To summarize, past results revealed that mothers’ CSA history is associated with maternal psychopathology, including dissociation, PTSD symptoms, and depression, as well increased risk of psychopathology and CSA for children. In addition, CSA has been associated with several short-term difficulties in children, some of the most documented and detrimental being dissociation, and internalizing and externalizing symptoms. While it has been documented that a maternal history of CSA is associated with increased difficulties in sexually abused children, the mechanisms underlying this association are still unknown. Further, a majority of studies have important limitations including small sample sizes (Trickett et al., 2011), and failure to include a comparison group (Seltmann & Wright, 2013). Many studies have focused on specific populations limiting the generalizability of findings such as clinical samples (e.g., Borelli et al., 2019) or narrow age ranges (e.g., Bernier et al., 2013). Other studies relied on child protective services reports to determine maltreatment status; however, these reports are known to greatly underestimate the prevalence of child maltreatment (Lewis et al., 2016). Finally, studies examining the intergenerational continuity of child maltreatment and its correlates often combine all forms of child maltreatment together, without consideration for the specificity of different maltreatment subtypes (Berzenski et al., 2014). Intergenerational cycles of CSA warrant independent examinations given the unique nature of this form of maltreatment, including the fact that perpetrator is not necessarily a caregiver and the unique traumagenic dynamics of sexualization, betrayal, stigmatization, and powerlessness involved (Finkelhor & Browne, 1985). Cycles of CSA, as compared to other forms of maltreatment, are understudied (Langevin et al., 2019). While our study does not allow to identify mechanisms of intergenerational continuity of CSA, it will fill some important gaps in the literature and further our understanding of the mechanisms involved in the associations between maternal history of CSA and sexually abused children’s outcomes.
The Present Study
The present study examined maternal psychological distress, maternal PTSD symptoms, and maternal dissociation as potential mediators of the relationship between maternal CSA and children’s internalizing, externalizing, and dissociation symptoms in a large sample of sexually abused children. Based on previous findings and theoretical models linking maternal CSA to later mental health difficulties and increased risks of maladaptation in sexually abused children (Baril & Tourigny, 2015; Cabecinha-Alati et al., 2020; Courtois & Ford, 2009), it was hypothesized that maternal history of CSA would be associated with increased maternal psychological distress, PTSD symptoms, and dissociation following children’s CSA, and that these increased mental health difficulties would in turn be associated with increased child internalizing, externalizing, and dissociation symptoms.
Method
Participants
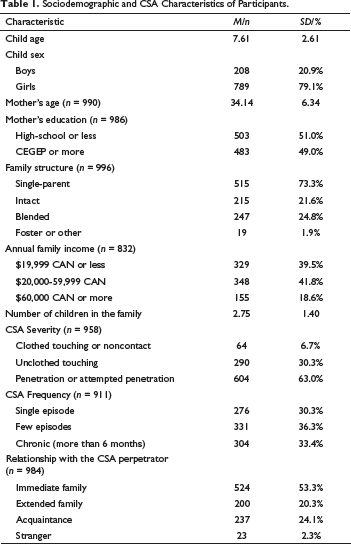
Sociodemographic and CSA Characteristics of Participants.
Measures
Background information. A sociodemographic questionnaire was used to compile background information as reported by the mother (e.g., mother and child age, levels of education, income). Mothers were also asked a question about their own histories of childhood sexual victimization: “During your childhood, have you ever been sexually abused?” (yes or no). Answers to this question were used to classify children in two groups depending on their mother’s histories of CSA. Studies have shown the validity of self-reported measures of CSA with adults, especially as it relates to psychopathology outcomes (Danese & Widom, 2020; Widom & Morris, 1997). CSA characteristics for children were coded using the clinical/medical files from the specialized intervention centers.
Maternal psychological distress. Mothers’ levels of psychological distress were assessed using the Psychiatric Symptom Index (PSI; Préville et al., 1992), a 14-item self-report measure used to assess symptoms of irritability, depression, anxiety, and cognitive difficulties in the last week. Mothers rated the intensity of their symptoms on a 4-point Likert-type scale (0 = never to 3 = very often). A total score for mothers’ psychological distress, ranging from 0 to 100, was calculated. Internal consistency for the total score was α = .92 in the current study.
Maternal PTSD symptoms. Mothers’ PTSD symptoms were self-reported using the Modified PTSD Symptom Scale—Self Report (MPSS-SR; Falsetti et al., 1993). The 17 items represent symptoms contained in the DSM-IV PTSD diagnosis. Mothers were asked to refer to their child’s disclosure of CSA while answering. The internal consistency for the total score in this study was α = .95. The PTSD symptoms scores were available for a subsample of 667 mothers (67% of the sample).
Maternal dissociation. The frequency of mothers’ current dissociative experiences was assessed using a 6-item version of The Dissociative Experiences Scale II (DES-II; Carlson & Putnam, 1993). Answers were provided on a continuum ranging from 0% to 100% of the time. Items were derived from the Absorption and Imaginative Involvement subscale (5) and the Amnestic Dissociation subscale (1). Item selection was made based on findings regarding their ability to differentiate victims of sexual abuse from nonvictim. The 6-item version was shown to have adequate internal consistency (α = .78) in the current study. The dissociation scores were available for a subsample of 673 mothers (68% of the sample).
Child dissociation. Mothers evaluated their children’s dissociation symptoms by completing the Child Dissociation Checklist (CDC; Putnam et al., 1993) comprising 20 items rated on a 3-point Likert-type scale (0 = not true to 2 = very true). The CDC assessed a wide range of dissociative behaviors, adaptive (e.g., child daydreams) to pathological reactions (e.g., child has two personalities). A total score ranging from 0 to 40 is calculated with a score of ≥ 12 being considered the clinical cut-off score (Putnam et al., 1993). The total score showed high internal consistency in the present sample (α = .82).
Child behavior problems. Mothers reported on their children’s behavior problems using the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2000, 2001). The preschool version was used for children aged 3-5 and the school-aged version with older children. Mothers indicated on a Likert-type scale the frequency of behaviors observed in the last two months (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true). T-scores were calculated for two subscales: internalizing symptoms (36 items in the preschool version; 32 items in school-age version) and externalizing symptoms (24 in the preschool version; 35 items in school-age version). Internal consistencies of the internalizing and externalizing behavior problems subscales are high (α = .91–.98).
Procedure
Children and their mothers were recruited during the intake interview at the specialized intervention centers. Mothers completed the questionnaires on site after giving informed written consent. Children old enough to understand the nature of this study gave their assent. Families were clearly informed that their participation in the study was voluntary and that declining participation would not alter service provision. Inclusion criteria were: (1) corroboration of CSA by CPS; or expert judgement—following in-depth assessment of children and their families by a multidisciplinary team in a hospital clinic specialized in CSA—deemed that the child was a victim of sexual abuse; (2) speaking French or English; (3) and not presenting cognitive limitations leading to an inability to consent to this study and/or to understand the questionnaires. The delay between the disclosure of CSA and the participation in this study vary greatly among the participants, but the majority (74.0%) of children were assessed within a year of the disclosure, and 90.1% within 2 years (data available for a subsample of 541 children). Ethic Committees of the Centre hospitalier universitaire Ste-Justine and Université du Québec à Montréal approved all research procedures.
Data Analyses
Means, Standard Deviations (SD), and Correlations for Study’s Variables.
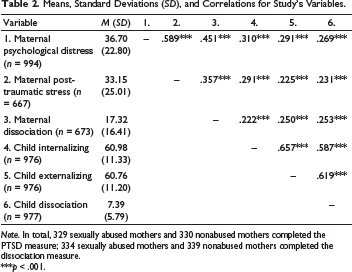
Note. In total, 329 sexually abused mothers and 330 nonabused mothers completed the PTSD measure; 334 sexually abused mothers and 339 nonabused mothers completed the dissociation measure.
***p < .001.
t-Tests Results for Group Differences in Outcome Variables.
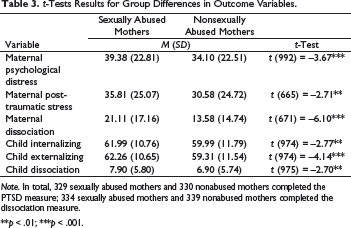
Note. In total, 329 sexually abused mothers and 330 nonabused mothers completed the PTSD measure; 334 sexually abused mothers and 339 nonabused mothers completed the dissociation measure.
**p < .01; ***p < .001.
Results
Preliminary Analyses
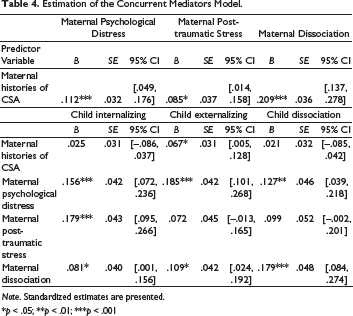
Estimation of the Concurrent Mediators Model.
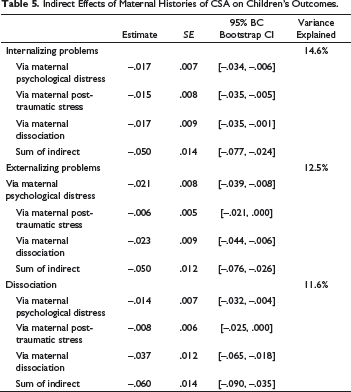
Indirect Effects of Maternal Histories of CSA on Children’s Outcomes.
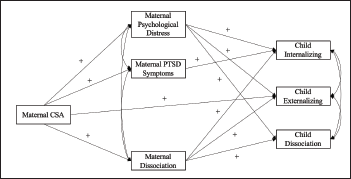
Note. In order to simplify the figure, nonsignificant paths are not represented here even though they were estimated. Also, not represented here, maternal education used as a control variable for all the outcome variables and child age used as a control variable for the child’s outcome measures.
The t-tests showed significant mean differences in the scores of sexually abused and nonabused mothers for psychological distress, dissociation, and PTSD (see Table 3 for detailed results). Abused mothers had higher scores on all these variables. Children of abused and nonabused mothers also differed in their levels of dissociation and internalizing and externalizing symptoms. Children of mothers with a history of CSA presented more symptoms.
Concurrent Mediation Model
The results from the main mediation analysis are presented in Table 4 and 5. A visual representation is also available in Figure 1.
Fit indices were satisfactory: RMSEA = .059, CFI = .994, and SRMR = .015. Maternal history of CSA was directly associated with maternal psychological distress, PTSD symptoms, and dissociation. Abused mothers reported higher levels of difficulties than nonabused mothers. Maternal victimization was also directly associated with externalizing symptoms in abused children. Maternal psychological distress and dissociation were positively associated with all three child outcomes. On the other hand, maternal PTSD symptoms were only associated with internalizing problems when all other variables were considered.
Indirect effects analyses revealed that maternal psychological distress, PTSD symptoms, and dissociation mediated the association between maternal history of CSA and sexually abused children’s internalizing symptoms. For externalizing symptoms and child dissociation, maternal psychological distress and dissociation came out as significant mediators. PTSD symptoms did not mediate the associations between maternal history of CSA and abused children’s externalizing and dissociative symptoms. The total effects of maternal histories of CSA on children’s outcomes were significant as reflected by the Sums of Indirect effects reported in Table 5.
Maternal education, used as a covariate, was only significantly associated with externalizing symptoms in children: mothers with higher levels of education had children presenting fewer of them. Child age was positively associated with internalizing and externalizing symptoms, but negatively associated with dissociation symptoms. The final mediation model explained 14.6% of the variance of internalizing symptoms, 12.5% of the variance of externalizing symptoms, and 11.6% of the variance of child dissociation.
Discussion
The aim of this study was to further our understanding of the mechanisms underlying the associations between maternal history of CSA and sexually abused children’s outcomes by examining maternal psychological distress, PTSD symptoms, and dissociation as potential mediators in the associations between maternal history of CSA and maternal reports of children’s internalizing, externalizing, and dissociation symptoms. Results were generally in line with our hypotheses and reflected the roles of maternal psychological distress and dissociation in the association between maternal CSA and all three child outcomes. However, mothers’ level of PTSD symptoms was a mediator only for child internalizing symptoms.
Our results are consistent with previous studies showing that mothers with a history of CSA show higher levels of mental health distress following their child’s disclosure than mothers with no history of CSA (Hiebert-Murphy, 1998; Langevin et al., 2020; Timmons-Mitchell et al., 1996; Trickett et al., 2011). Given the long-term consequences of CSA on survivors, mothers with a history of CSA might be more vulnerable from the get-go (Hillberg et al., 2011). Consistent with the CPTSD model, they are at increased risk of impairment (Courtois & Ford, 2009). For these vulnerable mothers, learning about their child’s sexual abuse could overwhelm their adaptive capacities and represent a major trigger of difficult memories and symptoms, leading to suboptimal coping mechanisms such as dissociation (Cyr et al., 2013).
Unfortunately, these increased mental health difficulties in sexually abused mothers appear to be associated with maladaptive outcomes in their sexually abused children. More specifically, increased maternal psychological distress and dissociation were associated with more internalizing, externalizing, and dissociation symptoms in children as reported by the mothers. Mothers with higher levels of distress and dissociation could be less emotionally available to support their child following the CSA. Given that maternal support is a major protective factor fostering child recovery (Wamser-Nanney, 2017; Zajac et al., 2015), this could in turn increase children’s difficulties (Dubowitz et al., 2001; Grunsfeld, 2018). Vicarious learning processes could also be at play, with abused children reproducing the reactions observed in their mothers by showing increased anxiety, depression symptoms, withdrawal, somatic complaints, aggressive behaviors, and dissociation in response to their trauma (Bandura, 1965; Thompson, 2013). Further, genetic studies can provide clues for increased vulnerability to psychopathology. A study including 6,924 mothers and their children found a significant increase in offspring PTSD symptoms in a dose–response relationship with maternal PTSD symptoms (Roth et al., 2014). A possible candidate contributing to the heritability of PTSD is the S’ allele of the 5-HTTLPR polymorphic region. It has been associated with increased risk and severity of PTSD (Wang et al., 2011). As such, children of PTSD survivors with this genetic predisposition may be at an increased risk of experiencing similar symptomology if stressed. Finally, it is also possible that mothers with mental health difficulties overestimated the difficulties presented by their children (Najman et al., 2000).
Interestingly, increased PTSD symptoms in mothers were only associated with internalizing symptoms in children. The bulk of the measured PTSD symptoms in this study could be considered internalizing: reexperiencing, avoidance, cognitive distortions (e.g., self-blame), and overregulation of affect (e.g., detachment, emotional avoidance). This could explain this finding, but since externalizing symptoms and dissociative reactions can be part of post-traumatic reactions too, future studies are needed to better understand the lack of associations between maternal PTSD symptoms and children’s externalizing and dissociation symptoms in this study.
While this study is the first, to our knowledge, to investigate the very important topic of the associations between maternal CSA, maternal mental health, and sexually abused children’s outcomes, and has numerous methodological strengths (large sample size, robust statistical analyses, validated measures), some limitations are to be acknowledged. This study used cross-sectional data, which prevents from drawing conclusions about causality and temporality of observed associations. Additionally, this study only relies on maternal reports, which could lead to informant bias and inflated effect sizes given shared method variance. Finally, given that this study used secondary analysis of data collected over almost two decades as part of multiple research projects with sexually abused children, there were some missing data on ethnicity and maternal PTSD symptoms and dissociation. FIML was used to account for the missing data on maternal symptoms. However, the high percentage of missing data on ethnicity limits our ability to draw conclusions about the generalizability of the findings to non-Canadians which composed 84% of the sample with data on this variable. Another limitation associated with the use of data collected over a long period of time is that diagnostic and treatment changes could have impacted the findings in a way that is not possible to document. Future studies should replicate these findings with longitudinal designs, cross-informant assessments, and individuals with diverse ethnic backgrounds. Other relevant variables could be integrated into the models such as cumulative trauma and revictimization (Brenner & Ben-Amitay, 2015), emotional dysregulation (Smith et al., 2014), attachment (Kwako et al., 2010), and maternal and social support (Zajac et al., 2015). Replicating these findings with nonoffending fathers of child victims of sexual abuse could also be of interest given that fathers may play a complimentary role in sustaining coping and recovery in CSA victims (Guelzow et al., 2002; Hébert et al., 2018).
Implications and Conclusions
It is crucial to emphasize that while this study examined maternal factors associated with outcomes in sexually abused children, mothers should not be blamed for their child’s abuse and difficulties following the abuse. On the contrary, this study was designed to provide valuable information on the needs of mothers in the context of their child’s victimization and to underscore the specific and heightened challenges that mothers with a history of CSA might face. Our findings show that specialized teams working with sexually abused children and their families need to document maternal histories of CSA and determine if, in addition to the child, the mother might need professional support for mental health difficulties. Such professional support should be routinely offered in order to not only help the mothers cope with their own distress and process their trauma, but also to strengthen their ability to support their child in this sensitive period following disclosure of CSA. Making sure that the mothers of sexually abused children are the best support they can be for their child will most definitely foster children’s recovery and trauma processing and help abused children resume to a healthy developmental trajectory.
Footnotes
Acknowledgments
We would like to thank the families who participated in this project.
Declaration of Conflicting Interests
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to acknowledge the several grants awarded to Martine Hébert by the Conseil québécois de la recherche sociale (RS-3282, 1999), Social Sciences and Humanities Research Council of Canada (#410-2001-0931, 2001; #410-2006-2292, 2006; #410- 2010-2424, 2011), the Fonds de Recherche du Québec—Société et Culture (SR-4648, 2002), and the Canadian Institutes of Health Research (#77614, 2006; #110945, 2011) that supported this project. These funding sources had no role in study design, in the collection, analysis and interpretation of data, in the writing of the report, and in the decision to submit the article for publication.