
Abstract
We investigated the prevalence of contact child sexual abuse (CSA) victimization in the US by comparing perpetration types in two adult cohorts. Participants included a nationally representative sample of adults aged 18–22 (n = 3,174) and 32–36 (n = 3,237). We used weighted proportions to obtain prevalences, Rao-Scott χ2 tests to assess for differences between cohorts. Analyses were also stratified by gender. The overall prevalence was 21.7% and similar between the two cohorts; 9.7% reported abuse by adults and 16.9% by youth under age 18. Most said that offenses were perpetrated by people known to them. CSA perpetration by youth was greater in the younger cohort than in the older cohort (18.8% vs. 15.1%). Among women, intrafamilial abuse by adults and youth declined from the older to the younger cohort. This study highlights emerging trends in CSA victimization by age of people who offend, by relationship to survivors, and by survivor gender.
Introduction
Child sexual abuse (CSA) is a global public health problem (Letourneau et al., 2014; Mercy, 1999; Veenema et al., 2015). Including its online forms, CSA is reported by up to 32% of women and 11% of men in the US (Finkelhor et al., 2024). Children who survive sexual abuse often experience substantial physical and mental health ramifications, as well as health risk behaviors (Guiney et al., 2024; Nagtegaal & Boonmann, 2022; Noll, 2021). Moreover, a significant national economic burden is associated with CSA (Letourneau et al., 2018). While substantial population-based evidence exists regarding prevalence, little research has examined what groups should be targeted for prevention services—critical information, as perpetration-prevention interventions must also be prioritized (Assini-Meytin et al., 2020). In this study, we focused on elucidating (1) the age of people who perpetrate contact CSA (i.e., children/adolescents versus adults) and (2) the relationship of individuals who perpetrate contact CSA to the people they harm by surveying victimization experiences of two age cohorts (ages 18–22 years and 32–36 years).
Child sexual abuse involves sexual acts experienced before age 18 that are inflicted by any adult or child in a position of power over the victim (e.g., physical, emotional, psychological, cognitive, economic) to obtain sexual gratification, when the child either does not have capacity to provide consent, or has capacity but does not provide consent (Mathews & Collin-Vézina, 2019). Sexual acts that constitute CSA are varied and can be broadly classified as contact and noncontact abuse. The prevalence of contact CSA, specifically, across the globe is estimated at 9.5% for girls and 5.5% for boys (Piolanti et al., 2025). In those analyses, prevalence rate for lifetime attempted and/or completed forced intercourse ranged from <0.5% to 18.2% among girls and from 0.4% to 9.4% among boys across the countries analyzed (Piolanti et al., 2025). In another global analysis of contact CSA, the prevalence identified was higher and estimated at 18.9% for girls and 14.8% for boys (Cagney, 2025). Variation in findings across studies stems from differences in the definition of CSA, operationalization of CSA, and data collection methodology (Letourneau & Assini-Meytin, 2025). As it pertains to the latter, online or other types of self-administered surveys tend to result in accurate capture of CSA prevalence (Meinck et al., 2016). The accuracy might be explained by fewer social desirability biases, greater perceived response anonymity, and greater comfort in disclosing victimization experiences (Meinck et al., 2016).
Variations in definition and operationalization of CSA can pertain to the child’s age, the age of the person who perpetrated harm, elements of sexual gratification, behaviors that constitute CSA (including behaviors in online environments), and consent (Mathews & Collin-Vézina, 2019). For example, in the US, the most recent CSA prevalence study disaggregated a generic measure of contact CSA (adult contact abuse, including forced sexual intercourse, and victimization by children or adolescents) from online CSA (Finkelhor et al., 2024). The study identified a prevalence of 19.8% for CSA among women and 6.2% among men; when the authors included online abuse, the CSA prevalence increased to 31.6% among women and 10.8% among men, representing increases of 59.6% and 74.2%, respectively (Finkelhor et al., 2024).
A limited body of research has examined the prevalence of CSA based on the relationship between the individual perpetrating CSA and the survivor. US-based research indicates that most children (i.e., 86% of boys and 93% of girls who were survivors of CSA) experienced CSA by someone they knew (Gewirtz-Meydan & Finkelhor, 2019). A recent comprehensive study on CSA perpetration type in Australia found that CSA was committed by a diverse array of individuals. For example, 7.8% reported CSA perpetrated by a parent or adult caregiver in the home (Mathews et al., 2024). That study also reported that, relative to women, men were significantly less likely to report CSA by a parent or adult caregiver in the home (Mathews et al., 2024). In a study with a non-probabilistic sample of 1,071 adults in Spain, most CSA was committed by adult acquaintances and adults not known to the child (Ferragut et al., 2021).
Child sexual abuse by adults in organizations was also a focus of prevalence studies. In a comprehensive scoping review of child maltreatment in youth-serving organizations, Finkelhor et al. (2025) documented a wide range of CSA in places such as daycare, healthcare, and sports organizations. In the US, the past-year prevalence of CSA in youth-serving organizations was found to be relatively low. Out of the 0.4% who experienced any type of maltreatment, 6.4% experienced CSA (Shattuck et al., 2016). The lifetime prevalence of CSA by adults in youth-serving organizations in the US was reported at 3.75%, which includes cases of noncontact abuse (Assini-Meytin et al., 2025). In Australia, 2.0% of participants aged >16 years reported having experienced CSA by adults in a youth-serving organization, with men reporting higher rates than women (2.7% vs. 1.3%, respectively) (Mathews et al., 2024). Similarly, in a French study, 1.28% of men had experienced contact CSA by a member of the Catholic clergy, compared with 0.34% of women (Bajos et al., 2023).
Although adult-perpetrated CSA remains a major societal challenge, epidemiological data suggest that most CSA survivors report abuse perpetrated by adolescents (Gewirtz-Meydan & Finkelhor, 2019). In the Australian Child Maltreatment Study, 10.0% of participants reported experiencing CSA perpetrated by an adolescent acquaintance with whom they were not romantically involved—representing the largest perpetration group (Mathews et al., 2024). Contexts in which CSA victimization by adolescents occur include youth engaging younger family members in sexual behaviors, sexual assaults by a dating partner, exploitation of inebriated youth at parties, and bullying episodes with a sexual focus.
The scope of youth-perpetrated CSA is often minimized in the literature and in practice. Reasons for this minimization include varying definitions of CSA between systems and countries (Mathews & Collin-Vézina, 2019), researchers using different language for adolescents versus adults in efforts to reduce stigma for children and adolescents convicted of sexual offenses (Shawler et al., 2020; Taquette & Monteiro, 2019), and distinct protections for youth in juvenile courts (Jacobs, 2024). Of note, we acknowledge the pertinent distinctions between problem sexual behavior engaged in by youth and CSA perpetrated by adults. The distinction recognizes that children are still developing, and it helps to avoid stigmatizing labels for children who engage in problem sexual behaviors (Swisher et al., 2008). However, we have chosen to retain the term CSA victimization because we assessed the survivor experience and not the prevalence of perpetration behaviors. Although we retained the term CSA victimization for consistency in this study, we acknowledge the important survivor-centered language use.
Emerging research also suggests that the risk of experiencing CSA may vary between age cohorts in the US, given that substantiated CSA cases reported to child protective services are declining over time (Finkelhor et al., 2023). It remains less clear whether this decline applies to all age and relationship dyads. The trends related to the prevalence of different types of perpetrator–survivor relationships in the general population, including the different types of intrafamilial abuse, is critically relevant to identifying gains and areas that need concentrated efforts. For example, data from Australia indicate that CSA perpetrated by adults in familial and institutional contexts has declined over time and abuse by adult strangers has remained stable, whereas sexual victimization perpetrated by adolescents has increased among girls (Mathews et al., 2024). Still, it is important to consider that different policies and prevention efforts have been utilized in the US and Australia; therefore, whether a similar trend is emerging in the US remains unknown. This study represents one the first efforts in the US to disaggregate CSA victimization by age of the person who offended and the relationship between the person who offended and their victim. Findings from our research are crucial for identifying key groups for targeted perpetration-prevention efforts. Data were collected across two birth cohorts using a nationally representative sample. Specifically, the purpose of this study was to identify the prevalence of contact CSA victimization in the US, variations by perpetration type, and trends across two adult representative sample cohorts over time.
Methods
Study Design and Data Source
In this study, we used a retrospective cross-sectional cohort design and included data from a nationally representative sample of US adults (N = 6,411). We included two participant groups: one aged 18–22 years (n = 3,174) and another aged 32–36 years (n = 3,237). Data originated from the Boundary Violation and Sexual Victimization Survey—a study aimed to assess the change in prevalence of CSA in youth-serving organizations in the US that included measures of CSA perpetrated by anyone, not solely those in organizational settings (Assini-Meytin et al., 2025). We designed the study with two age cohorts to identify prevalence differences between these groups while minimizing overlap in childhood years and recall biases. Participant ages differed between cohort members by a minimum of 10 years to a maximum of 18 years. The two groups represent (1) young adults who are recently passed the legal threshold of childhood/adolescence and therefore proximate to contemporary reporting periods (18–22 years) and (2) adults who experienced childhood less than a generation earlier (32–36 years). Our design enabled us to examine potential shifts across developmental cohorts, as well as changes in institutional and societal contexts over time.
Data were collected by Ipsos from July to August 2022, which represents the summer months in the US. Our survey company partner reports low seasonal effects on survey responding in general. For this survey, the field period lasted 27 days, a slightly extended period designed to overcome potential reduction in participation owing to people being on vacation. The final sample included panelists from their KnowledgePanel (35.4%), supplemented with panelists recruited from partnering companies (64.6%). Specifically, 17.6% of panelists in the younger cohort and 52.9% of panelists in the older cohort were recruited from KnowledgePanel; 82.4% of panelists in the younger cohort and 47.1% of panelists in the older cohort were recruited from partnering companies. Survey response rates for KnowledgePanel and partnering companies were 49.6% and 17.6%, respectively. Per Ipsos internal records, the survey response rate is within the expected response rates for KnowledgePanel (50%) and partnering companies (5% to 20%). KnowledgePanel is a probability-based sample, whereas the partnering companies’ samples, though non-probability-based, are designed to be representative of the US population. Ipsos’ weighting methodology ensures that the blended samples better represent the final target population. The following demographics were used in the weighting process: age by gender (man, woman, non-binary/prefer to self-describe/refused); race and Hispanic ethnicity (Non-Hispanic White, Non-Hispanic Black, Non-Hispanic two or more races, Hispanic, Other Non-Hispanic); education (less than high school, high school, some college, bachelor’s degree and higher); census region (Northeast, Midwest, South, West); metropolitan area (yes, no); and household income (<$25,000, $25,000-$49,999, $50,000-$74,999, $75,000-$99,999, ≥$100,000). In addition to the listed demographics, the following variables were also included in the weighting of panelists from partnering companies: TV use (<3 hours/day, ≥3 hours/day); Internet for personal use (<10 hours/week, ≥10 hours/week); expression of political/community opinions online (less than once a month or more often, not at all); and frequency that participants try new products (not at all/somewhat, a lot/completely).
The Institutional Review Board of Bloomberg School of Public Health at the Johns Hopkins University approved the study. Participants could opt out and skip any survey item. All participants were provided with a list of annotated psychological support resources at the end of the survey. Of note, data for this study were collected by a third-party company that adheres to participant treatment protocols outlined by the federal Office of Management and Budget, follows guidelines from the Belmont Report, and is compliant with the Health Insurance Portability and Accountability Act. Per contractual agreement, the survey company deleted the link between survey responses and panelists’ personally identifiable information once the dataset was delivered to the research team.
Measures
Demographic Characteristics
Participant demographic characteristics were assessed as gender identity (men, women, non-binary/other), race and ethnicity (as described above), educational attainment (as described above), and highest educational attainment of the participants’ mothers (less than high school, high school graduate, some college, college graduate/some graduate school, graduate school, don’t know).
Any Contact CSA
In the current analysis, CSA victimization was assessed by using three items adapted from the Juvenile Victimization Questionnaire (JVQ)-R2: Adapted Version (Australian Child Maltreatment Study) (Mathews et al., 2021). The Australian Child Maltreatment Study CSA items were closely modeled on and substantively similar to the US-based JVQ-R2 items on CSA (Finkelhor et al., 2015) and validated after an extensive testing process (Mathews et al., 2023). These three items were adapted to assess CSA by (1) adults and youth unrelated to organizations (in the family, other known adults and youth, and adults and youth who were strangers to the participant); (2) adults in organizations (e.g., organizations for recreation and culture, sports, religion, music and arts, K-12 education); and (3) youth in organizations. For each of these contexts, the three items asked whether an individual (1) “touched your private parts when they shouldn’t have, or made you touch their private parts;” (2) “tried to force you to have sex, even if it didn’t happen;” and (3) “forced you to have sex.” Of note, for the purpose of the current analysis, we conceptualized CSA as abuse involving physical contact only. This definition generated a conservative estimate of prevalence and avoided any possibility of overinclusion of noncontact exposure experiences in younger participants enabled by recent technological advances (e.g., through online flashing), especially given that this survey did not include separate items about online sexual victimization. These three contact CSA items are congruent with a robust conceptual model of CSA that delineates the key CSA defining characteristics (Mathews & Collin-Vézina, 2019). Response options were: 1 = Yes, 2 = No, and 3 = Not sure. The nine CSA items were combined into a single measure coded as 0 = Never, 1 = Ever, and 2 = Not sure, where “Ever” indicates at least one instance of contact CSA before age 18. Out of 1,572 participants coded as “Ever” experiencing CSA, 901 experienced more than one instance of CSA across the nine items. Among the remaining participants, at least one instance of “Not sure” was coded in such category (n = 365).
Perpetrator Age
Adult Perpetration
Contact CSA victimization by adults was assessed with a composite measure based on three items that specified perpetration by adults in organizations and ten items that specified abuse by adults in the family (eight items), other known adults (one item), and unknown adults (one item). Items were combined into a single measure as 0 = Never and 1 = Ever, where “Ever” indicates at least one instance of contact CSA by adults before age 18.
Youth Perpetration
Contact CSA victimization by youth was assessed with a composite measure based on the three items that specified perpetration by youth in organizations and by four items that specified abuse by youth in the family (brother, sister, cousin, foster sibling; one item); current or former romantic partner (one item), other known youth (one item), and unknown youth (one item). These items were combined into a single measure coded as 0 = Never and 1 = Ever, where “Ever” indicates at least one instance of contact CSA before age 18 by children or adolescents.
Perpetrator Types
Adults in the Family
Contact CSA victimization by adults was assessed with eight items that specified perpetration by a family adult member. We further subdivided the items to conduct an analysis of subtypes of perpetration in the family by male caregivers (father, step-father), female caregivers (mother, step-mother), non-live-in boyfriend/girlfriend, other relatives (uncle, aunts, grandparents), and foster parents.
Adults in Organizations
Contact CSA victimization by adults in organizations was assessed with a composite measure based on the three items specifying contact CSA by adult staff and volunteers in organizations for recreation and culture, sports, religion, music and arts, and K-12 education.
Other Known Adults
Contact CSA victimization by known adults was assessed with a single item that specified perpetration by a known adult, excluding those affiliated with an organization and family members.
Unknown Adults
Contact CSA victimization by adult strangers was assessed with a single item that specified perpetration by an adult who was a stranger to the participant.
Youth in the Family
Contact CSA victimization by siblings and cousins was assessed with a single item that specified perpetration by a participant’s brother, sister, or some other child who lived with the participant (e.g., cousin, foster sibling).
Current or Former Romantic Partner
Contact CSA victimization by a participant’s current or former romantic partner was assessed with a single item that specified perpetration by a participant’s boyfriend/girlfriend or former boyfriend/girlfriend.
Other Known Youth
Contact CSA perpetrated by a youth known to the participant was assessed with a composite measure based on the three items describing contact CSA perpetrated by children/youth in organizations and by the one item that specified contact CSA perpetration by a youth known to the participant but unrelated to an organization.
Unknown Youth
Contact CSA victimization by an unknown youth was a single item that specified CSA perpetration by a child/youth who was a stranger to the participant.
Statistical Analyses
Analyses comprised two main steps. First, to correct demographic imbalances, we used weighted proportions to obtain prevalences and corresponding 95% confidence intervals (CIs) of contact CSA victimization overall and by perpetration types. We used Rao-Scott χ2 tests for survey data to assess for statistically significant differences between contact CSA prevalences by cohort. We compared cohort differences between the two categories (0 = No vs. 1 = Yes) and excluded 2 = “Not sure” responses in the cohort comparison given the small proportion of participants in that category. Statistical significance for differences between cohorts was set at p < .05. Analyses were conducted for the full sample and then again stratified by gender. The small number of participants who identified with diverse gender identities (n = 155), particularly in the older cohort (n = 35), precluded subanalyses with this group. Missing data comprised <1% of the sample and were excluded from the analyses. All analyses were conducted in Stata/SE 18.0.
Sensitivity Analysis
We conducted a sensitivity analysis on the “Not sure” responses within the “any contact child sexual abuse” measure. To account for the possibility of ambiguous yet positive CSA cases being excluded from the analysis, we classified the 365 “Not sure” responses as “Yes.” Conversely, to address the potential that “Not sure” responses did not reflect cases of contact CSA abuse, we also classified the same 365 “Not sure” responses as “No.” We conducted Rao-Scott χ2 tests for survey data to assess statistically significant differences in contact CSA prevalence by cohort for both scenarios.
Results
Sample Demographic Characteristics With Weighted Percentages by Cohort
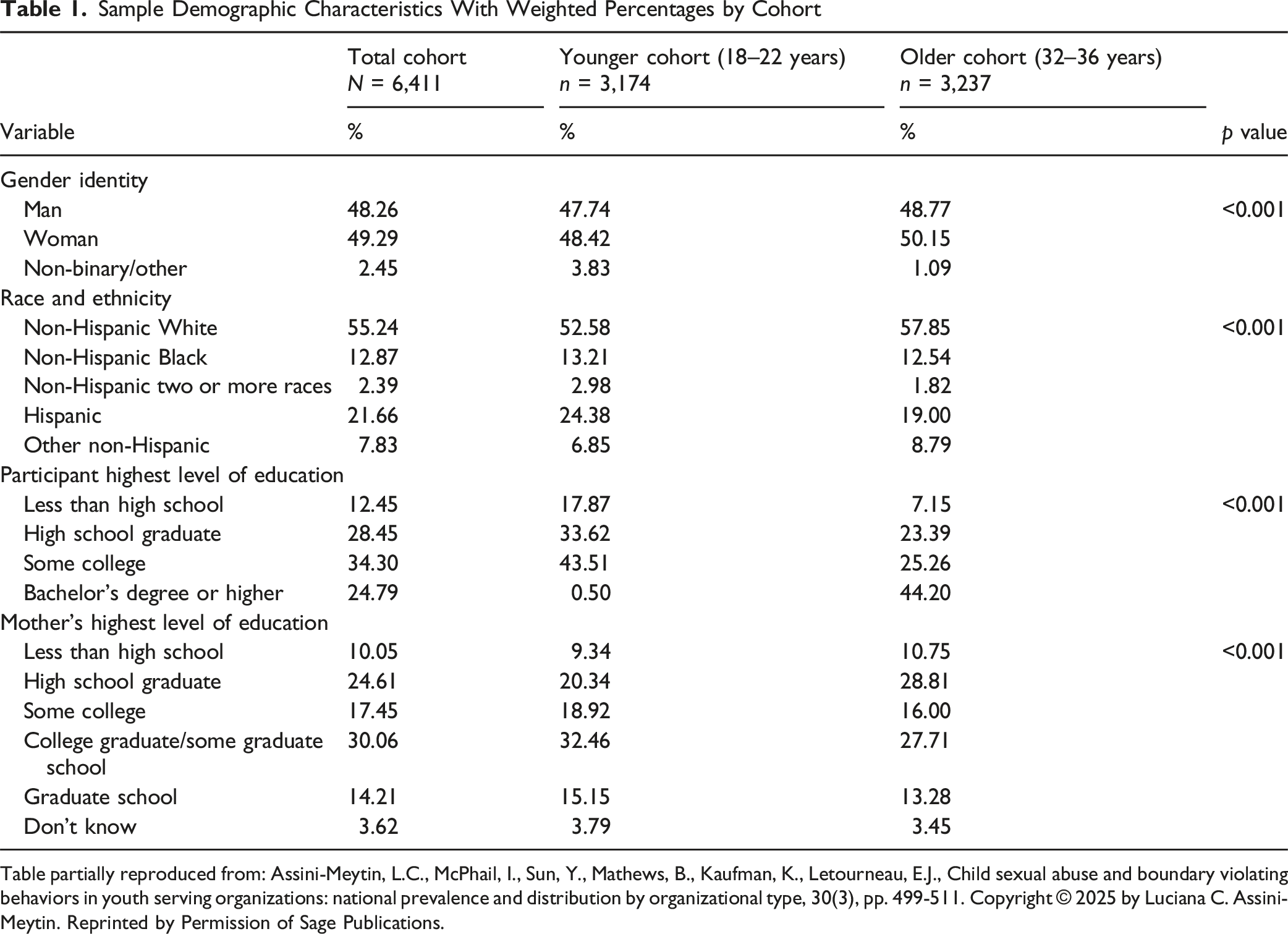
Table partially reproduced from: Assini-Meytin, L.C., McPhail, I., Sun, Y., Mathews, B., Kaufman, K., Letourneau, E.J., Child sexual abuse and boundary violating behaviors in youth serving organizations: national prevalence and distribution by organizational type, 30(3), pp. 499-511. Copyright © 2025 by Luciana C. Assini-Meytin. Reprinted by Permission of Sage Publications.
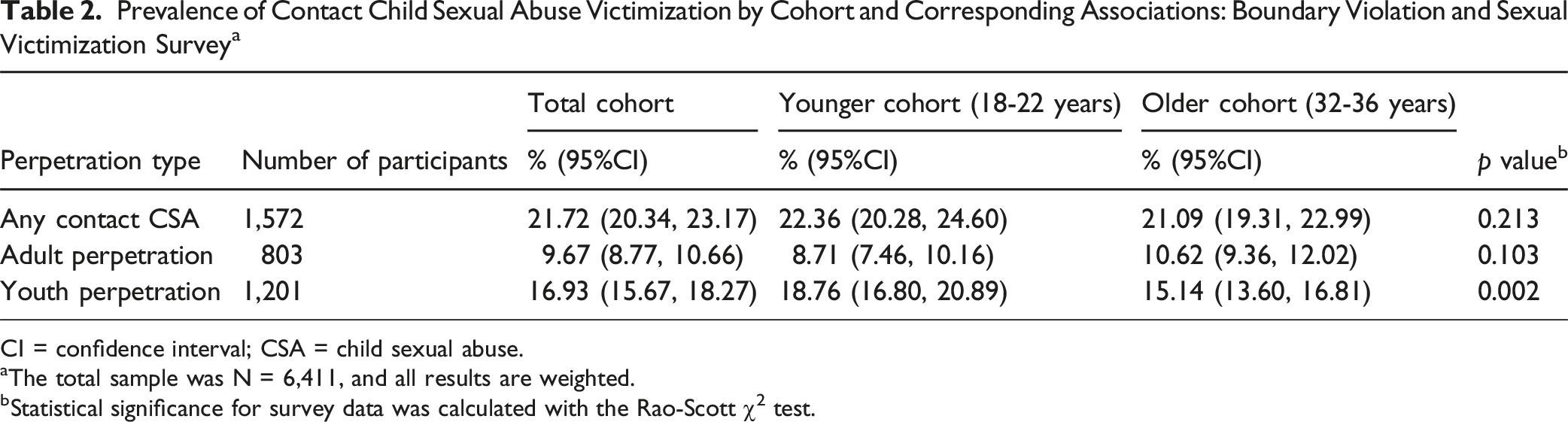
Prevalence of Contact Child Sexual Abuse Victimization by Cohort and Corresponding Associations: Boundary Violation and Sexual Victimization Survey a
CI = confidence interval; CSA = child sexual abuse.
aThe total sample was N = 6,411, and all results are weighted.
bStatistical significance for survey data was calculated with the Rao-Scott χ2 test.
As shown in Table 2, 9.67% (95% CI 8.77, 10.66) of participants experienced contact CSA perpetrated by an adult, and 16.93% (95% CI 15.67, 18.27) experienced contact CSA by a youth. Participants in the younger cohort reported a higher prevalence of contact abuse by youth than did the older cohort (18.76% vs. 15.14%; χ2 = 18.15, p = .002).
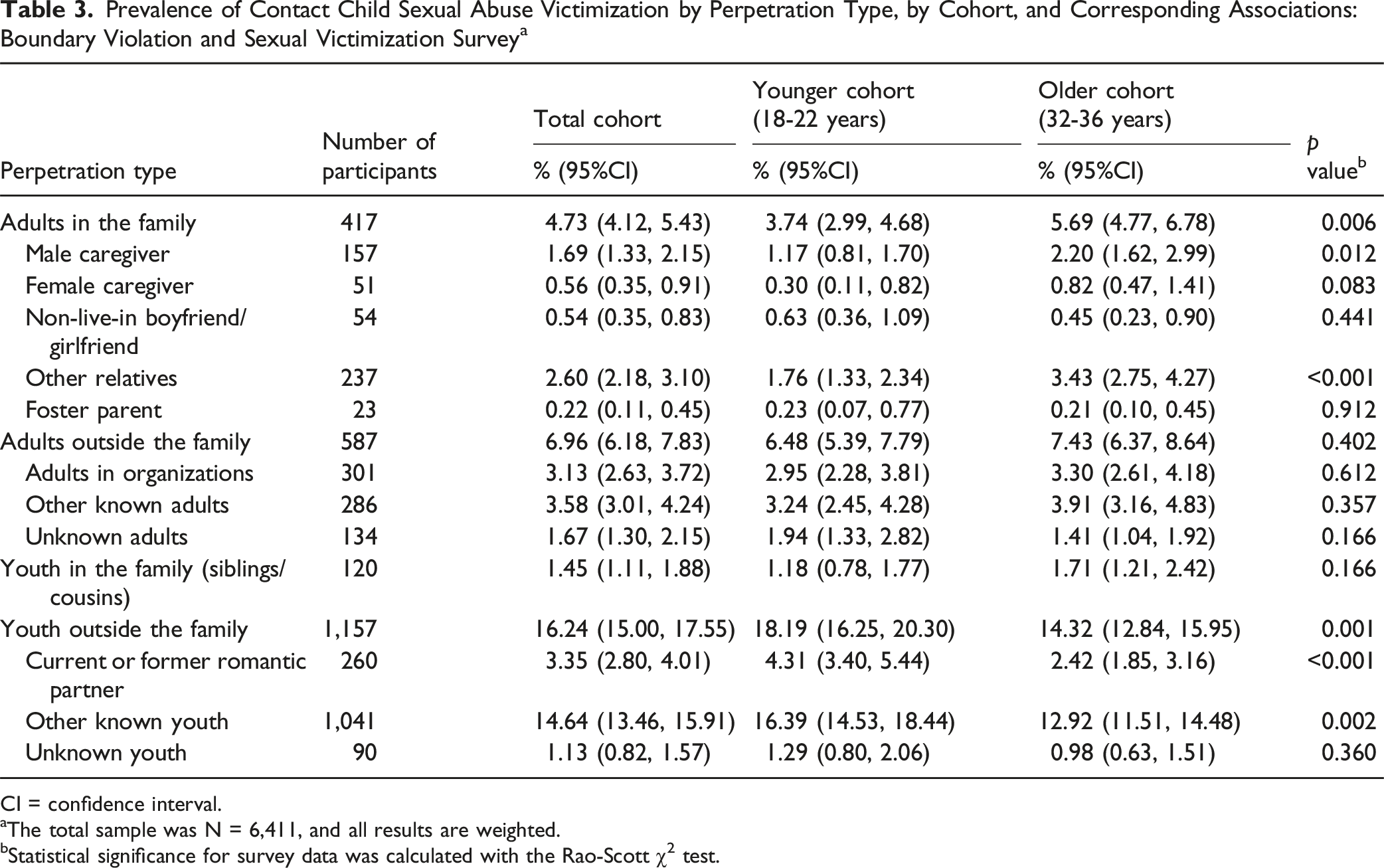
Prevalence of Contact Child Sexual Abuse Victimization by Perpetration Type, by Cohort, and Corresponding Associations: Boundary Violation and Sexual Victimization Survey a
CI = confidence interval.
aThe total sample was N = 6,411, and all results are weighted.
bStatistical significance for survey data was calculated with the Rao-Scott χ2 test.
Compared with those in the older cohort, participants in the younger cohort reported a lower proportion of abuse by adults in their families (3.74% vs. 5.69%; χ2 = 11.99, p = .006). Specifically, the prevalence rates of contact CSA in the younger cohort were approximately half that in the older cohort for male caregivers: 1.17% vs. 2.20% (χ2 = 9.47, p = .012) and other relatives 1.76% vs. 3.43% (χ2 = 16.28, p < .001). However, a greater proportion of participants in the younger cohort reported abuse by current or former romantic partners (4.31% vs. 2.42%; χ2 = 19.14, p < .001) and other known youth (16.39% vs. 12.92%; χ2 = 18.48, p = .002) compared with those in the older cohort reported.
CSA Victimization Among Women
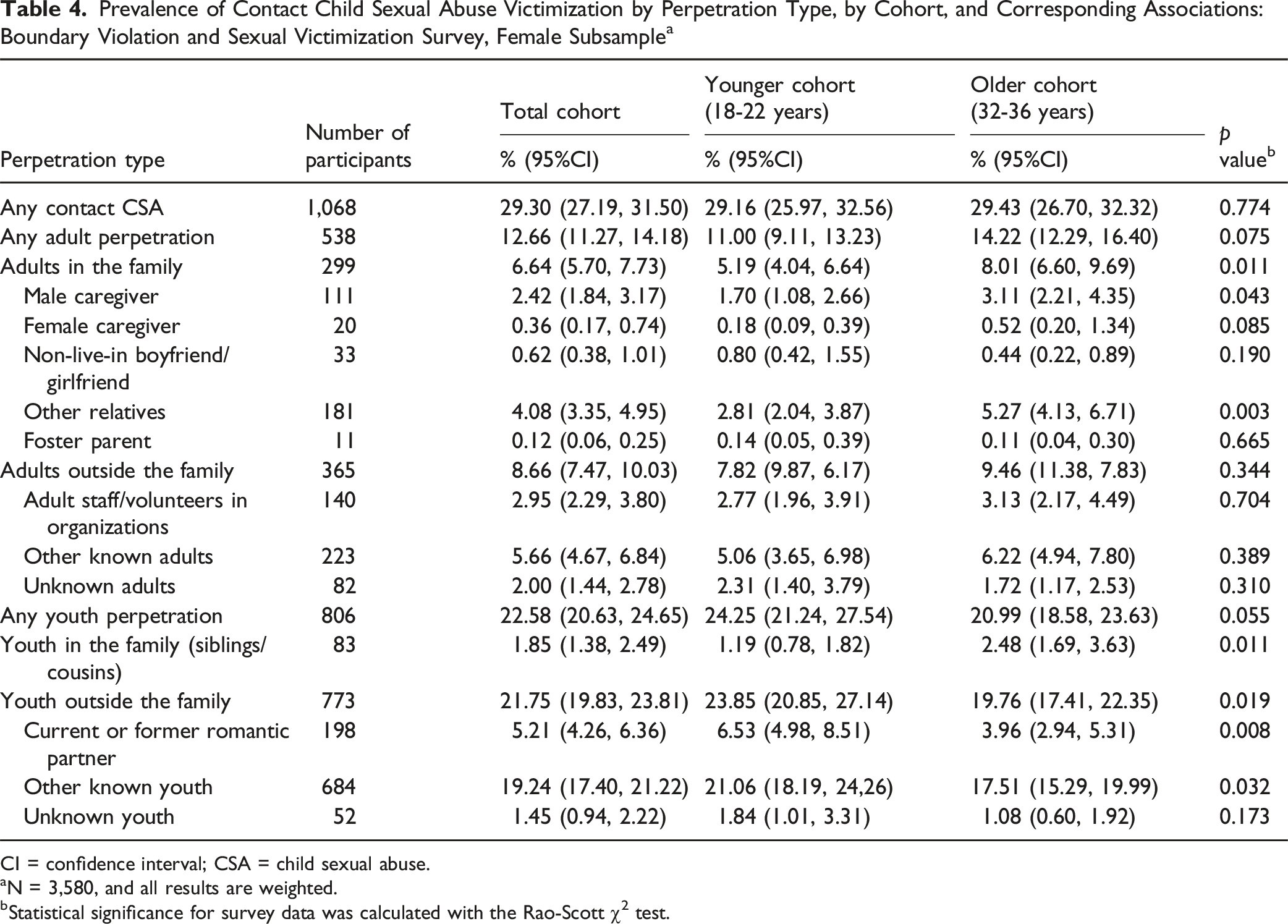
Prevalence of Contact Child Sexual Abuse Victimization by Perpetration Type, by Cohort, and Corresponding Associations: Boundary Violation and Sexual Victimization Survey, Female Subsample a
CI = confidence interval; CSA = child sexual abuse.
aN = 3,580, and all results are weighted.
bStatistical significance for survey data was calculated with the Rao-Scott χ2 test.
Results indicated a marginally statistically significant lower prevalence of any adult perpetration among the younger cohort compared with the older cohort (11.00% vs. 14.22; χ2 = 5.74, p = .075). Specifically, women in the younger cohort reported a lower proportion of intrafamilial abuse by adults than did the older cohort (5.19% vs. 8.01%; χ2 = 9.80, p = 0.011). Women in the younger cohort reported a greater prevalence of contact CSA perpetrated by youth than did the older cohort (24.25% vs. 20.99%; χ2 = 7.80, p = .055). Specifically, women in the younger cohort reported a higher proportion of contact CSA by current or former romantic partners (6.53% vs. 3.96%; χ2 = 13.52, p = .008) and by non-romantically involved youth (21.06% vs. 17.51%; χ2 = 9.86, p = .032). Notably, similar to adult perpetration, women in the younger cohort reported a lower proportion of abuse by youth in the family (siblings and cousins) relative to the older cohort (1.19% vs. 2.48%; χ2 = 7.98, p = .011).
CSA Victimization Among Men
Prevalence of Contact Child Sexual Abuse Victimization by Perpetration Type, by Cohort, and Corresponding Associations: Boundary Violation and Sexual Victimization Survey, Male Subsample a
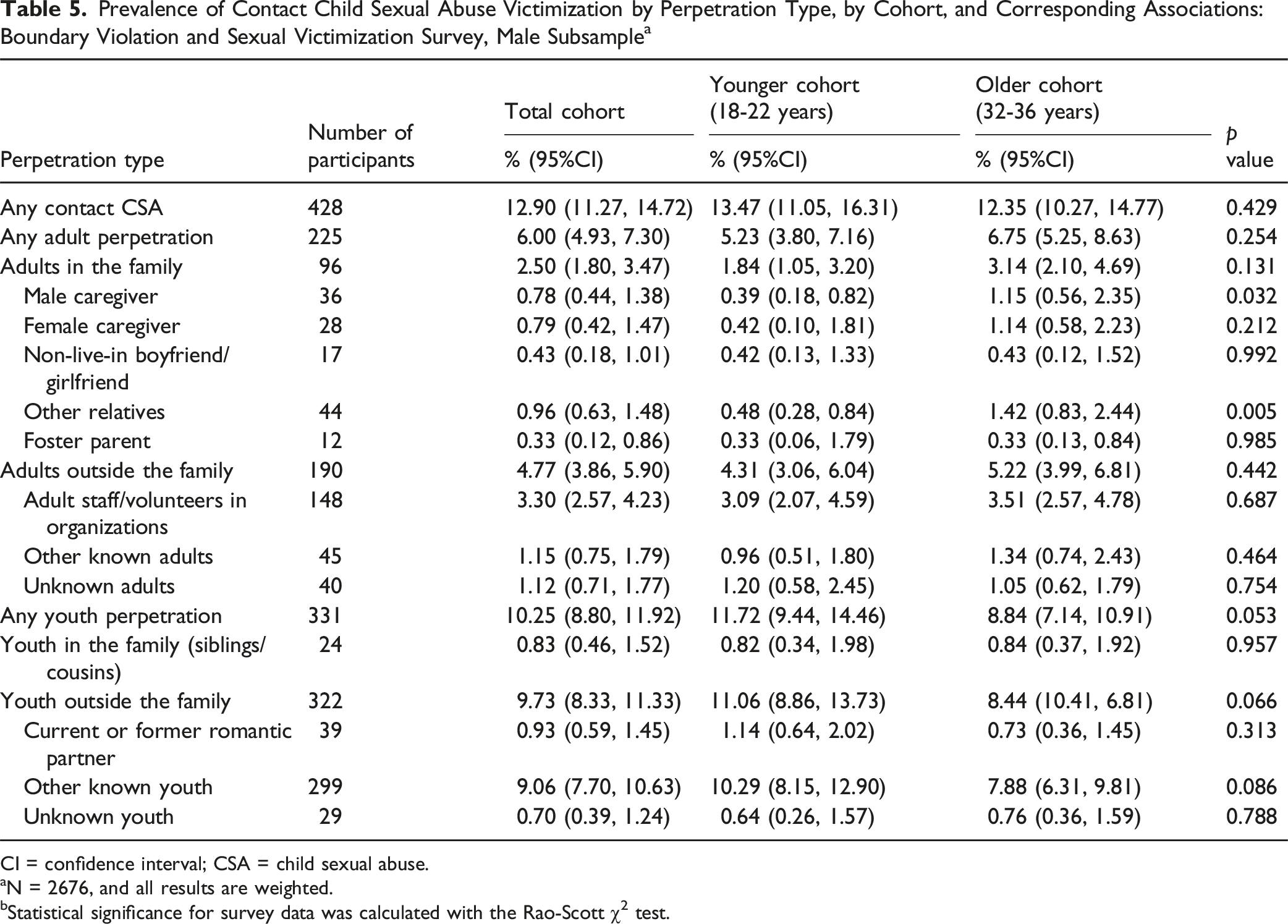
CI = confidence interval; CSA = child sexual abuse.
aN = 2676, and all results are weighted.
bStatistical significance for survey data was calculated with the Rao-Scott χ2 test.
Men in the younger cohort, relative to those in the older cohort, reported less contact CSA by male caregivers: 0.39% vs. 1.15% (χ2 = 4.926, p = .032) and other relatives: 0.48% vs. 1.42% (χ2 = 6.015, p = .005). They also reported a greater prevalence of contact CSA by youth: 11.72% vs. 8.84% (χ2 = 6.638, p = .053).
Discussion
Our findings reveal that one in five children, including one in three girls (29.3%) and one in eight boys (12.9%), experienced contact CSA in the US across two young adult cohorts who were ages 18 to 22 and 32 to 36 in 2022, when data were collected. For all participants combined, the prevalence of any contact CSA was 21.7%. Our sensitivity analysis showed that when we classified “Not sure” responses as experiences of contact CSA, the prevalence rate increased to 26.6%. Notably, when we did so, the younger cohort had a higher contact CSA prevalence than did the older cohort. It is possible that, compared with individuals ages 18 to 22, those who are in their 30s have had more time to reflect on their experiences and realize that ambiguous situations were indeed experiences of CSA.
Our findings closely mirror results from a recent prevalence study in Australia, which used similar assessment items (Mathews, Pacella, et al., 2023). We identified a higher prevalence rate of contact CSA than did other studies that used retrospective US adult reports (namely, 19.8% among women and 6.2% among men ages 18 to 28) when excluding online abuse (Finkelhor et al., 2024). The higher contact CSA prevalence rate that we identified might be explained by differences in CSA measurement. Finkelhor et al. (2024) measured CSA by adults with a single item adapted from the JVQ CSA items and only by adults the participant knew (Finkelhor et al., 2024). Our study also resulted in a higher CSA prevalence rate than a study of a nationally representative sample of children <18 years (i.e., 22.8% for girls and 10.3% for boys ages 14 to 17; last-year victimization; (Finkelhor et al., 2013). Our study’s higher rates may be explained by the fact that we assessed lifetime prevalence and our participants were ≥18 and were no longer at risk of accruing new CSA victimizations. Studies involving children miss future CSA victimizations, particularly the substantial proportion of CSA that occurs in mid-to-late adolescence (Gewirtz-Meydan & Finkelhor, 2020).
Our data showed that girls are at a higher risk than boys for contact CSA within families. It may be that children in families disproportionately live with heterosexual men, who may have a greater proclivity for abusing girls and much less proclivity for abusing boys. Although the prevalence of CSA in organizational settings was similar for men and women (2.95% vs. 3.30%, respectively), adults in organizations represented the highest proportion of perpetration by adults outside of the family among the male subsample. In certain types of organizations with a high presence of male youth and male adults (e.g., Catholic institutions), men who perpetrate CSA are more likely to have access to boys than girls and to be inclined to abuse boys rather than girls (Hunt et al., 2024; Mathews et al., 2024).
Study findings also revealed that youth were more often responsible for perpetrating contact CSA than adults were (16.9% vs. 9.7%). This result is consistent with other findings in the literature (Gewirtz-Meydan & Finkelhor, 2020). Further, and perhaps more important, we also identified higher rates of victimization by youth in the younger cohort relative to the older cohort (18.8% vs. 15.1%). In the stratified analysis, for both female and male participants and relative to the older cohort, perpetration by extrafamilial youth was higher in the younger cohort. These findings are mirrored by those reported in the Australian Child Maltreatment Study (Mathews et al., 2024). Potential explanations for the observed increase might include younger participants identifying more nuanced forms of coerced sexual interactions compared with their older counterparts, particularly following the #MeToo movement (Mathews et al., 2024). Another possible explanation is youths’ increased access to pornography, especially violent or nonconsensual content, which has been associated (though not causally linked) with higher self-reported violent behavior among boys and girls (Ybarra et al., 2011, 2024). However, our study showed that among women, perpetration by intrafamilial youth was lower, signaling a decline in intrafamilial offending by youth against girls. The decline in intrafamilial offending by youth may reflect overall decline in CSA by adults in families, stronger parental supervision, and enhanced social norms against incest.
These findings underscore the need for more emphasis on extrafamilial youth perpetration when discussing and addressing sexual abuse. The CSA problem should not be typified as only involving adults as potential perpetrators. For instance, inferences from child protection services data should be presented alongside a reminder that most youth CSA perpetration is not encompassed in these data. Strategies like background record reviews and increased legal system penalties need to be recognized as largely irrelevant for the youth perpetration segment (Bosetti & Fix, 2024; Letourneau & Caldwell, 2013).
Several productive strategies are available to foster the prevention of youth-perpetrated CSA. For example, pediatricians and counselors should provide parents and youth with healthy child and adolescent sexual development information and resources, as well as discuss the importance of children and youth learning to respect appropriate sexual boundaries. Such education should also discourage bullying, especially bullying involving sexual derogation and harassment. It should also emphasize the responsibility that older youth have to not engage younger children in sexual activity (Letourneau et al., 2022; Ruzicka et al., 2021). Evidence shows that 27.5% of abuse perpetrated by youth is against younger children ages 0–9 years (Gewirtz-Meydan & Finkelhor, 2020).
In addition, our findings highlight the critical need for strong school-based education and policies addressing normative and problem sexual behavior. As children age into adolescence and begin to engage in sexual behaviors with others, they are vulnerable to poor decision making, in large part because of limited knowledge and a lack of clear rules about appropriate sexual behaviors, contexts, and partners (Letourneau et al., 2017). These factors are exacerbated by the failure of caregivers, educators, and other trusted adults to teach pubescent children about consent and that younger children (including friends, family members, and neighbors) are inappropriate sexual targets (Letourneau et al., 2017; Mendelson & Letourneau, 2015).
Universal prevention approaches could foster an earlier understanding of appropriate behaviors and prevent the onset of problem sexual behaviors involving peers and younger children. In a meta-analysis of 20 randomized clinical trials that evaluated programs aimed at preventing sexual violence among adolescents, the authors found a significant association between these prevention programs and a reduction in the perpetration of sexual harm (Piolanti et al., 2022). Policymakers, educators, and preventionists should more actively promote the dissemination and adoption of school-based programs that prevent problematic sexual behaviors among young adolescents. Examples of such programs include Responsible Behavior with Youth and Children (Letourneau et al., 2022; Ruzicka et al., 2021), Safe Dates (Foshee et al., 2004), and Shifting Boundaries (Taylor et al., 2015).
Our study findings also revealed declining rates of intrafamilial abuse. The identified decline is consistent with overall declines in substantiated CSA reported to child protective services in the US (Finkelhor et al., 2023) and declines identified in a nationally representative sample in Australia (Mathews et al., 2024). Importantly, our data also showed a decline in intrafamilial abuse among girls perpetrated by youth (e.g., siblings and cousins). Although no research has provided causal explanations for such declines, they might be explained by a few factors, such as increased family vigilance about CSA, more active legal and social intervention for domestic sexual violence, and advancements in behavioral health treatment and pharmacology that may undercut depression and other family dynamics that underly the perpetration of intrafamilial CSA (Jones et al., 2001). Further, the increase in dissemination of CSA prevention programs may also explain CSA declines in families (Kenny et al., 2025; Noll et al., 2025). Future research is needed to ascertain what strategies prevent intrafamilial offending that could be harnessed to further advance observed declines in perpetration by adults and youth. The reduction in intrafamilial CSA is of special relevance, as this type of perpetration is particularly damaging for the health, psychological, and interpersonal well-being of survivors and contributes to the disruption of family systems (Noll, 2021). It is important to note that the statistically significant and non-significant contextual percentage declines each represent highly relevant declines in raw numbers of survivors at the population level (Mathews et al., 2024; Shattuck et al., 2016).
A number of study limitations merit discussion. First, we used retrospective reports. Although recall bias is expected in a retrospective design, it is unlikely in more severe cases of abuse (Hardt & Rutter, 2004; Widom & Morris, 1997). The reliance on participant retrospective reports may also have excluded life events that happened in the early childhood years before the formation of lasting memories. However, our mode of data collection as an online, self-administered survey, is a reliable form of obtaining accurate self-report data on childhood experiences, including sexual abuse (Meinck et al., 2016). Another limitation is that the two cohorts had some overlap in childhood years, which may limit interpretation of cohort differences in contact CSA trends.
Another important consideration in cohort comparison is that the recruitment of the younger cohort strongly relied on a non-probabilistic quota sample from Ipsos partnering companies. Because the samples within the two age cohorts were not fully based on a probabilistic panel, comparisons between the two age groups may partly reflect differences in recruitment methodology. Changes in prevalence between the two cohorts may also reflect cohort-specific patterns of disclosure, perceptions and interpretations of events involving sexual harm, and recall biases. Although Ipsos applied a weighting process to correct for demographic imbalances, the sampling structure and composition should be taken into account when generalizing the results to the broader US population within these age cohorts.
Although our findings are specific to contact CSA, survey items may not have captured all forms of contact abuse. Further, our findings exclude an assessment of online abuse and noncontact abuse. The lack of inclusion of online abuse may underestimate the CSA prevalence, particularly in the younger cohort.
Conclusion and Future Directions
This study identified important trends in CSA prevalence in the US, including by gender, and as inflicted by different individuals. Encouragingly, we identified a decline in some types of CSA, especially intrafamilial CSA, and particularly for girls. Future research should continue to monitor this trend and should further explore the factors that influence this important advance. In addition, future studies should incorporate intermediate cohort limits to examine generational trends and differences over time. Of more concern, however, is the higher contemporary prevalence of adolescent-inflicted CSA, which should be made an urgent priority. This trend warrants further research, including consideration of influential social and environmental factors. Similarly, research to consider the effectiveness of current prevention programs in mitigating CSA across this and other types of perpetration risks can shed light on the efficacy of existing programs and may illuminate which types of targeted prevention are now most urgently needed. Future studies should also consider trends across all gender types and in noncontact abuse, including abuse types facilitated by technology.
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this manuscript was fully supported by the CDC’s National Center for Injury Prevention and Control, through an award to the Johns Hopkins Center for Injury Research & Policy (R49 CE003090; Project 2; PI, Letourneau).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement by, the CDC/HHS, or the US Government.