
Abstract
Relational Cultural Theory (RCT) offers a feminist, relationally-centered approach to therapy and social work practice, which is focused on the unique developmental experiences of girls, women, and individuals from traditionally underrepresented or marginalized groups. Much of the theoretical and intervention research on this model has focused on adult women, with less attention devoted to RCT's application with adolescent girls. This integrative literature review synthesizes qualitative, quantitative, mixed methods, and case study research on RCT to assess: 1) how RCT theoretical tenets have been translated into intervention strategies with adolescent girls, and 2) the degree to which RCT intervention research includes experiences of girls from diverse and underrepresented groups. Five electronic databases were searched through August 2023. Following deduplication and screening for inclusion/exclusion, 12 studies were retained for inclusion in this review. Analysis revealed four core RCT concepts that were linked with therapeutic intervention components across all included studies: mutual empathy, authenticity, empowerment, and the overall strengthening and deepening of relational connections. Over half of included studies reported samples that were over 50% girls of color, and/or having an expressed study purpose focused on girls from a diverse or underrepresented group. Practice implications for work with adolescent girls are discussed.
Keywords
Introduction
Research on Relational Cultural Theory (RCT) as a counseling framework has emphasized the conceptual principles that undergird this model of human development (Comstock & Qin, 2005; Frey, 2013; Jordan, 2017). Less is known about how these principles have been translated into social work treatment interventions with adolescent girls across diverse practice contexts. As relational health gains increasing traction as a key component of well-being among adolescents exposed to adversity (Li & Julian, 2012; Yu & Deutsch, 2020), there is a need to synthesize research findings on theoretically-based interventions that promote relational health in this population. Furthermore, while RCT's theoretical origins emphasize the model's applicability to diverse and underrepresented women, much of RCT's early empirical research was drawn from majority White, college-based samples (Frey et al., 2005; Frey et al., 2006; Liang et al., 2002). This integrative literature review seeks to address these gaps by offering an examination of findings on the clinical application of RCT with adolescent girls, including a synthesis of research on RCT interventions, therapeutic practice strategies, and application to therapeutic work with girls from diverse and underrepresented groups.
Relational Cultural Theory: Overview and Key Concepts
RCT is a model of human development that prioritizes mutually empathic and empowering relationships as the foundation for healthy development. With origins in feminist psychology, RCT asserts that meaningful connection to others is central to one's capacity for intellectual and personal growth, strength in the face of adversity, and capacity to enact individual and collective change (Hartling, 2008; West, 2005). While traditional theories of human development have emphasized separation-individuation from others as paramount to healthy development, feminist critics have pointed out that such models are based primarily on the experiences of Western, White, heterosexual, cisgender men, and thus do not account for the developmental experiences of women, minority populations, non-Western cultures, and individuals from other underrepresented groups (Gilligan, 1987; Jordan, 2017). RCT offers an alternative framework that attends to the unique differences in socialization and relational growth that may accompany diverse social identities.
Growth-fostering connections are at the heart of RCT, and are defined by relationships that are mutually engaging, authentic, and empowering. Mutual empathy requires that relational participants: 1) feel heard by the other, and 2) feel that they impact the other (Comstock & Qin, 2005). When both parties feel equally seen and heard by the other, power differentials are dismantled and a mutual sense of safety is nurtured in the relationship. Authenticity is present when both participants are comfortable expressing their true selves with the other (Frey, 2013). Authenticity permits freedom in self-expression, as individuals recognize that they are unconditionally accepted by the other. Lastly, growth-fostering connections promote relational empowerment where one feels confident to take action (Jordan, 2017). This may manifest as exercising the right to say “no,” communicating decisions about what one will do or share in a relationship, or setting limits in a relationship (Comstock & Qin, 2005; Lenz, 2016).
Developmental Focus: Adolescent Girls
Adolescence is a developmental period marked by the transition from childhood into emerging adulthood, with three phases including early adolescence (ages 11–13 years), middle adolescence (ages 14–16 years), and later adolescence/emerging adulthood (ages 17–21 years; Barrett, 1996). Across these stages, girls and young women contend with sexual decision-making (Lara & Abdo, 2016), self-esteem and body image (Burnette et al., 2017), sexual identity and romantic attraction (Everett et al., 2019; Stewart et al., 2019), puberty (Teitelman, 2004), and friendships and peer group belonging (Huntley & Owens, 2013; Newman et al., 2007). For girls who do not fit into the “dominant majority”–-including Black, Indigenous, and People (girls) of Color (BIPOC), those who identify as sexual and/or gender minorities, and girls belonging to other marginalized groups–-developmental experiences can be complicated by discrimination and institutional oppression (Mereish et al., 2022; Benner et al., 2018). During a developmental period where “fitting in” is paramount, feeling as if one does not fit a society-prescribed mold can present challenges. For girls belonging to marginalized groups, their experiences with discrimination and racial trauma have been linked with health risk behaviors, lower academic engagement, mental health problems, suicidal ideation, and lower life satisfaction (Daley et al., 2018; Leath et al., 2019; Pachter et al., 2018; Sutter & Perrin, 2016).
Yet, connections to positive adults have demonstrated a protective effects for girls in general (Hamilton et al., 2016), and for BIPOC girls and those belonging to other marginalized groups in particular (Clonan-Roy et al., 2016). Girls’ growth-fostering connections with adults can be transformative and promote the three C's of girls’ resilient development: 1)
Current Study: RCT as a Practice Framework for Adolescent Girls
The centrality of relational connections in the social-emotional development of adolescent girls makes this an ideal developmental stage for the application of RCT practice approaches. Furthermore, it is an ethical imperative in social work to attend to the unique therapeutic needs of girls from culturally diverse backgrounds, and RCT has been suggested as a practice framework that answers this call (Haskins & Appling, 2017; Kress et al., 2018). While there is a substantial body of theoretical research on RCT, the field lacks a developmentally-specific synthesis of RCT empirical studies related to direct practice with adolescent girls. Lenz's (2016) systematic review offers an important overview of RCT measurement studies and interventions across the lifespan; however, the review's lack of developmental, gender, and cultural specificity challenges its utility for social workers seeking specific strategies for adolescent girls. Practitioners and scholars seeking theoretically- and empirically-grounded strategies for building relational health into their work with girls may benefit from an integrative picture of RCT's capacity to advance such relational therapeutic goals. Thus, this integrative review seeks to summarize and synthesize empirical research on the RCT intervention models and strategies implemented in therapeutic and/or clinical practice settings. The following research questions will be addressed:
Methods
Methods implemented for this review were informed by Torraco's (2016) and Whittemore and Knafl's (2005) guidelines for an integrative literature review, which are further described below: articulation of the search strategy, specification of inclusion/exclusion criteria, and evaluation and analysis of data.
Search Strategy and Inclusion/Exclusion Criteria
Five electronic databases were searched for articles: CINAHL, ERIC, Medline, PsycINFO, and Social Science Citation Index. Key search terms include the following: (“relational cultural theory” OR “relational-cultural theory” OR “relational cultural” OR “relational-cultural”) AND (adolescen* OR “young adult” OR “emerging adult” OR “teen*” OR “preteen*” OR “youth”) AND (“practice” OR “intervention” OR “therapy” OR “therapeutic” OR “treatment” OR “counseling” OR “social work”). Citations were exported to the bibliographic citation management software Zotero.
After deduplication, the following inclusion criteria were applied for screening of article titles and abstracts: 1) peer-reviewed published articles with full-text accessible, 2) English language, 3) RCT used as guiding theoretical framework, 4) target population is girls spanning any phase of adolescence (ages 11–21 years), 5) implementation of an RCT-based intervention in social work and/or other therapeutic or clinical practice settings, and 6) attention to some developmental outcome(s) salient to girls’ well-being, such as self-esteem, prosocial skills, health risk behaviors, relationship skills, or mental health. In an effort to reduce publication bias, dissertations were included. Both authors screened and coded all articles, and a third doctoral-level researcher reconciled any coding discrepancies. Articles retained from the title and abstract screening underwent full-text review for inclusion.
Data Evaluation and Analysis
Data Evaluation: Focused Inclusion of Diverse Sample
Each included study was evaluated for whether it included a sample with focused inclusion of girls from a diverse and/or underrepresented group (yes/no), including BIPOC, girls who identify as a sexual and/or gender minority, girls with disabilities, and/or any other minoritized status. “Focused inclusion” was indicated by at least 50% of the sample being composed of girls from diverse and/or underrepresented groups.
Data Analysis
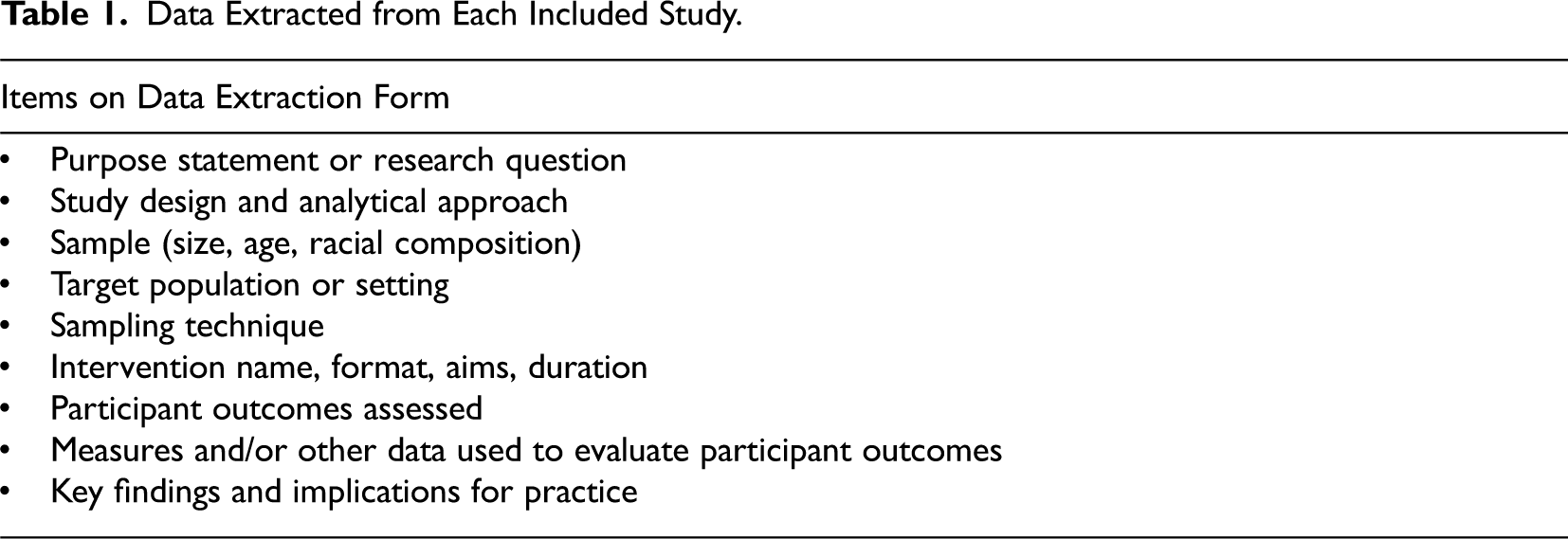
Data analysis involved three steps drawn from Whittemore and Kanfl's (2005) constant comparison method for integrative review analysis: data reduction, data display, and data comparison. First, data reduction involved classifying articles into four subgroups––qualitative studies, quantitative studies, mixed methods studies, and case studies. A summary sheet of extracted data points (See Table 1) was compiled for each included primary source. Second, ATLAS.ti qualitative analysis software (version 9) was used to examine patterns and themes between articles. Summary sheets were organized into document groups based on study type (quantitative, qualitative, mixed method, case study); open codes were then used to highlight central concepts and themes in each study. Lastly, data comparison involved identification of patterns that linked RCT with practice approaches and interventions with adolescent girls.
Data Extracted from Each Included Study.
Results
Systematic searching of the five electronic databases yielded 716 initial citations. Manual deduplication resulted in 457 remaining citations for screening. Overall, 65 citations met criteria for full-text review. Two articles were not available in full-text, resulting in full-text review of 63 articles for eligibility, and 12 studies meeting inclusion criteria (See Figure 1).
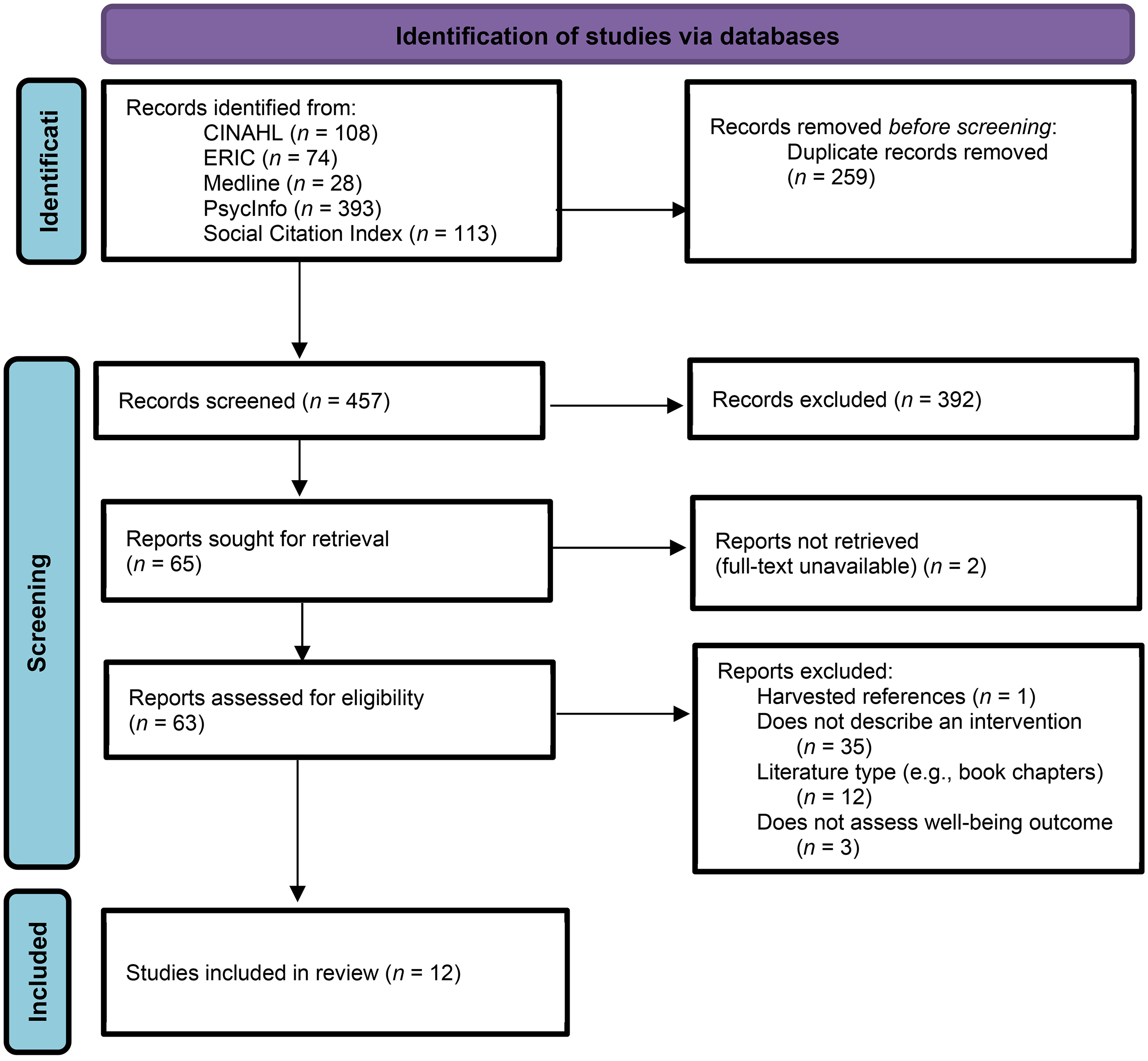
PRISMA flow chart (Page et al., 2021) of study screening and inclusion/exclusion.
Characteristics of Included Studies
Studies spanned 13 years of publication, from 2004 (Sillitti, 2004) to 2017 (Haskins & Appling, 2017). Half of the included articles (n = 6) were case studies (Haskins & Appling, 2017; Lazzari et al., 2005; Melles & Frey, 2014; Ruiz, 2012; Sassen et al., 2005; Sillitti, 2004). three were mixed methods (Allen, 2011; Foley, 2008; Kappus, 2008), one was an A-B single case design (Lenz et al., 2012), one was a qualitative study (Cannon et al., 2012), and one was a descriptive quantitative study (Steese et al., 2006). One-third of included studies (n = 4) were dissertations (Allen, 2011; Foley, 2008; Kappus, 2008; Sillitti, 2004), and the remaining were peer-reviewed articles (See Table 2).
Summary of Included Studies with RCT-Based Interventions for Adolescent Girls (N = 12).
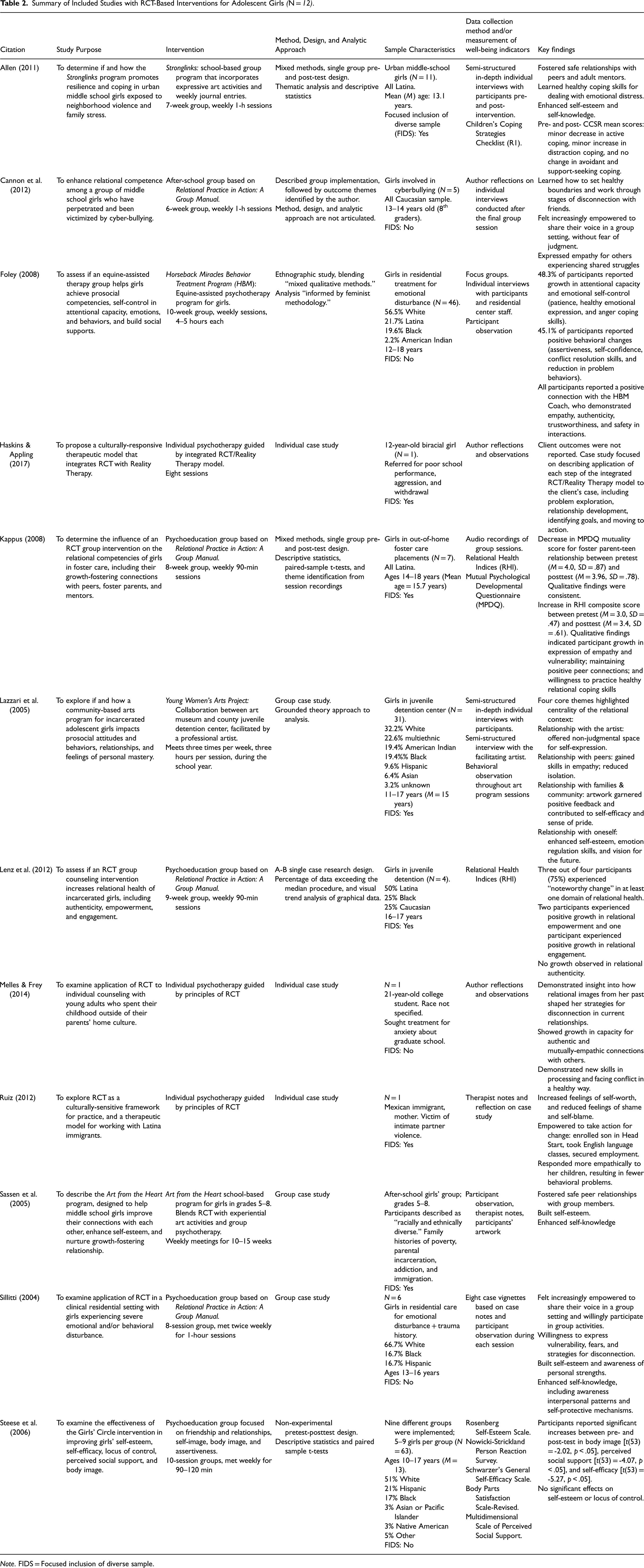
Note. FIDS = Focused inclusion of diverse sample.
Interventions
Seven different therapeutic interventions were described across the twelve included studies, including Stronglinks after-school program (Allen, 2011), Horseback Miracles Treatment Program (HBM; Foley, 2008), the Young Women's Arts Project (Lazzari et al., 2005), Art from the Heart after-school program (Sassen et al., 2005), Girls’ Circle (Steese et al., 2006), individual psychotherapy (Haskins & Appling, 2017; Melles & Frey, 2014; Ruiz, 2012), and psychoeducational expressive therapy groups based on Jordan and Dooley's (2001) Relational Practice in Action: A Group Manual (Cannon et al., 2012; Kappus, 2008; Lenz et al., 2012; Sillitti, 2004). The majority of studies (75%, n = 9) implemented small-group interventions in settings such as schools, clinical residential programs, and juvenile detention centers. Intervention length ranged from six weekly sessions (Cannon et al., 2012) to three times/week for the length of a school year (Lazzari et al., 2005), with the majority of interventions lasting 8 to 10 weeks.
Study Sample Characteristics
The target populations included adolescents exposed to a trauma such as neighborhood and/or family violence, girls with clinically significant emotional-behavioral difficulties, girls in foster care, girls in juvenile detention centers, and girls identifying as “third culture” (children raised outside of their parents’ home culture, such as expatriate or missionary families). Sample age range across studies was 11–18 years of age, with the majority of girls being 15–17 years old. Sample sizes were small, ranging from single-client case studies (Haskins & Appling, 2017; Melles & Frey, 2014; Ruiz, 2012) to a two-year ethnographic study of the Horseback Miracles Behavior Treatment Program (N = 46; Foley, 2008).
RQ 1: Translation of RCT Concepts to Intervention Components
Analysis revealed four core RCT concepts that were linked with practice strategies across all twelve studies: mutual empathy, authenticity, empowerment, and the overall strengthening and deepening of relational connections. For each of these core RCT concepts, a brief description of practice strategies implemented across included studies is described below.
Mutual Empathy
The most common practice strategy for promoting empathy was providing opportunities for supported vulnerability, which was reported by 75% (n = 9) of studies (Allen, 2011; Cannon et al., 2012; Kappus, 2008; Lazzari et al., 2005; Lenz et al., 2012; Ruiz, 2012; Sassen et al., 2005; Sillitti, 2004; Steese et al., 2006). This included activities in which participants discussed shared challenges or adversities without fear of judgment or ridicule. Kappus’ (2008) group for girls in foster care offered numerous examples, noting that participants bonded through sharing their trauma histories, and demonstrated remarkable growth in their expressions of empathy, understanding, and sensitivity toward peers.
Half of included studies (n = 6) highlighted facilitator role modeling as a key practice strategy for fostering empathy (Foley, 2008; Haskins & Appling, 2017; Kappus, 2008; Lazzari et al., 2005; Ruiz, 2012; Sassen et al., 2005). Sassen et al. (2005) indicated that their Art from the Heart group provided real-time role modeling of empathy when facilitators observed participants saying hurtful comments about other girls. The group leaders used these incidents as an opportunity to express concern for what the victim might be feeling, and help the girls engage in perspective-taking to understand how their choices can affect those around them.
Some studies (n = 3; 25%) promoted empathy through therapeutic discussions focused on girls’ gender or culture (Kappus, 2008; Ruiz, 2012; Sillitti, 2004). In a group for Latina girls (Kappus, 2008), participants empathized with their shared experiences with cultural beliefs and gender influencing their positions in the family, and their sense of power and voice. Similarly, girls in Sillitti's (2004) residential treatment group practiced empathy in group discussions about gender-specific issues such as the sexual double standard and the traumas of sex work.
Authenticity
All twelve included studies used authenticity exercises focused on self-discovery as a key practice strategy. Programs such as Stronglinks (Allen, 2011) were developed with an emphasis on self-discovery, with three of the program's four themes centered around identity. Other studies described activities focused on self-exploration and identity, such as a “self banner” in which girls created a banner that depicts both the external self they share with the world, and their “true” inner true self (Sillitti, 2004).
Over half of the nine group interventions (n = 5; 56%) used artistic or creative activities as a practice strategy to facilitate self-expression (Allen, 2011; Lazzari et al., 2005; Sassen et al., 2005; Sillitti, 2004; Steese et al., 2006). The Young Women's Art Project (Lazzari et al., 2005) provided an especially strong example of art as a therapeutic vehicle for authenticity. Through collaboration with a major metropolitan art museum, the artist facilitator helped girls explore their histories, feelings, and experiences through painting, sculpture, and photography.
Empowerment
Over half of included studies (n = 6) focused on empowering girls and building confidence by learning a new skill or developing a creative product through painting, sculpting, writing, drawing, or other forms of creative expression (Allen, 2011; Foley, 2008; Lazzari et al., 2005; Melles & Frey, 2014; Ruiz, 2012; Sassen et al., 2005; Steese et al., 2006). Such activities instilled a sense of mastery, competence, and pride in participants, which empowered them to take agency in other domains of their lives. For example, an empowerment practice strategy in the HBM equine therapy program (Foley, 2008) was horse care and training, with girls demonstrating improvements in self-confidence, communication skills, and assertiveness. Similarly, participants reported that emotion regulation strategies gave them a sense of self-control that felt empowering (Foley, 2008).
In 75% of studies (n = 9), therapeutic discussions about marginalization, stereotypes, oppression, and/or power were highlighted as an empowerment practice strategy (Cannon et al., 2012; Haskins & Appling, 2017; Kappus, 2008; Lenz et al., 2012; Melles & Frey, 2014; Ruiz, 2012; Sassen et al., 2005; Sillitti, 2004; Steese et al., 2006). Discussion that focused on experiences of marginalization gave participants insight into the structural forces that shape society's views of gender, race, and class, and subsequently inform girls’ perceptions of themselves. Authors noted the collective sense of empowerment girls experienced when drawing connections between harmful societal messaging about race and gender and their own struggles with self-acceptance.
Strengthening and Deepening Relational Connections
Nearly half of included studies (n = 5) indicated that forming a positive relationship with the group facilitator was a key practice strategy for helping participants deepen their capacity for growth-fostering connections (Allen, 2011; Foley, 2008; Lazzari et al., 2005; Ruiz, 2012; Steese et al., 2006). By demonstrating trustworthiness, compassion, and non-judgment, mentors modeled a healthy relational template and provided participants with a safe space to explore all dimensions of themselves. In Foley's (2008) equine therapy study, participants explained that the Coach's respect, care, and compassion showed them what a healthy and supportive relationship looks like, and led them to expect these standards in other relationships in their lives.
Psychoeducation about RCT's connection-disconnection cycle was a practice strategy used in several interventions (n = 6; 50%) to help participants understand the ways they use disconnection strategies—social withdrawal, aggression, or hostility—as a means of self-protection (Cannon et al., 2012; Lenz et al., 2012; Ruiz, 2012; Sassen et al., 2005; Sillitti, 2004; Haskins & Appling, 2017). Such psychoeducational exercises explored how previous relational experiences with abandonment and trauma led participants to use disconnection strategies as a defense against vulnerability and authenticity in relationships (Sillitti, 2004). Across studies, exploration of the connection-disconnection cycle allowed participants to understand how and why they use disconnection to create distance in relationships, and identify adaptive replacement strategies that permit more authentic and meaningful connections.
Facilitating experiential activities to connect with peers was a key practice strategy in seven studies (Allen, 2011; Foley, 2008; Kappus, 2008; Lenz et al., 2012; Sassen et al., 2005; Sillitti, 2004; Steese et al., 2006). Artwork, horse care and riding, hiking, and writing were used as creative mechanisms to promote bonding and connection among participants. Allen (2011) noted in her work with the Stronglinks program that it was through the experiential group activities that participants became comfortable expressing appreciation for each other, admiration for their peers’ strengths and talents, and disclosing about their personal struggles.
RQ 2: Focused Inclusion of Girls from Diverse and Underrepresented Groups
Over half of included studies (n = 7, 58%) reported samples that were over 50% individuals from diverse or underrepresented racial or ethnic groups (Allen, 2011; Haskins & Appling, 2017; Kappus, 2008; Lazzari et al., 2005; Lenz et al., 2012; Ruiz, 2012; Sassen et al., 2005). Diversity on metrics of sexual or gender minority status, religious background, disability, or other minoritized identities were not addressed in any studies. The most commonly-represented group were girls identifying as Latina and/or Hispanic (Allen, 2011; Kappus, 2008; Lenz et al., 2012; Ruiz, 2012). Kappus (2008) took particular note of how Latina girls in her group for foster youth bonded over their shared Hispanic heritage and cultural issues related to power, gender, and race. Although the Young Women's Art Project (Lazzari et al., 2005) and Art from the Heart (Sassen et al., 2005) both reported focused inclusion of girls from underrepresented groups, study results were reported as aggregate qualitative findings across all participants, and not separated by race and/or ethnicity.
Lastly, Ruiz's (2012) psychotherapy case study with Mexican immigrant “Claudia,” placed significant emphasis on the sociocultural factors that impacted Claudia's experiences of victimization and oppression, including her family's cultural beliefs about gender and power. Therapeutic sessions drew attention to issues faced by Claudia which are common to Latina immigrant women, including language barriers, discrimination, undocumented status, and intimate partner violence (Ruiz, 2012). The author observed that jointly exploring the impact of these sociocultural factors on Claudia's circumstances helped reduce her feelings of self-blame and shame, and promote a sense of agency and empowerment over her life and choices.
Discussion
This review revealed that RCT intervention research with adolescent girls has focused on clinical practice strategies that promote the core building blocks of growth-fostering connections: mutual empathy, authenticity, and empowerment. These core concepts–all of which contribute to the fourth theme of deepening and strengthening relational connections–were consistent across studies with diverse populations, practice settings, and group and individual therapeutic contexts. This has important implications for participants’ relational images, or their perception of how they see themselves in relationships and what they can expect from others in relationships (Jordan, 2010). Exposure to chronic trauma and violence–as experienced by many of the samples included in this review–can increase one's risk of developing negative relational images, or the perception that disconnection, inconsistency, lack of trust, and/or rejection are expected parts of human relationships (Frey, 2013; Comstock & Qin, 2005). Therapeutic interventions that facilitate growth-fostering connections have the potential to serve as a corrective experience for participants, permitting them to develop more positive relational images that emphasize mutuality, trust, and authentic connection. For example, Avent-Harris and colleagues’ (2021) work with RCT highlights the power of corrective relational images in their therapeutic work with religious Black women, and Rhodes and colleagues (2006) have similarly found it in decades of work with youth mentoring programs. These findings align with many of the qualitative results reported by studies included in this review, several of which revealed a renewed sense of hope, trust, and relational safety experienced by participants through their connections with intervention facilitators, therapists, and/or fellow group members.
While there was consistency across studies regarding the translation of core RCT concepts into therapeutic practice strategies, the age of this body of literature suggests there is room for modernization on this topic. 83% (n = 10) of included studies were published ten or more years ago, and 33% (n = 4) of studies used Jordan and Dooley's (2001) RCT intervention manual, published over two decades ago. Jordan and Dooley's (2001) group manual is a seminal text in RCT intervention work and has provided the foundation for RCT practice with groups. Yet, there is also potential for innovation and adaptation of this model based on modern research on the impact of trauma on neurobiology and relational capacities (Zaleski et al., 2016), and the ways that systematic oppression can impact the unique relational needs and experiences of girls from underrepresented groups (Bryant-Davis & Moore-Lobban, 2019). For example, Zelenski and colleagues (2016) argue that treatment interventions that support relational connection in the aftermath of trauma must begin by addressing clients’ neurobiological trauma response, including the effects of a chronically activated sympathetic nervous system. That is, before engaging in practice strategies focused on building relational connection, we must help clients develop the tools to downregulate the trauma symptoms of hyperarousal and vigilance, which can inhibit feelings of safety and trust in relationships.
Diversity was fairly well attended to in this body of literature, with over half of included studies having samples where the majority of participants were from diverse or underrepresented racial/ethnic groups. The relational focus of RCT interventions may be particularly salient for girls who are raised in diverse cultures that emphasize the centrality of relationships and connection. Although we cannot ignore heterogeneity and diversity within cultures, research has broadly found that warm, emotionally positive social interactions and close extended family bonds are interpersonal priorities that are embedded in Latine cultural values (Campos et al., 2008), which was the most frequently represented group across included studies. In alignment with these values, the relationally-focused interventions included in this review seek to elevate relational connections as a strategy for promoting resilience and thriving.
Less attention was focused on girls from other underrepresented groups, with no studies reporting a sample majority of girls identifying as Black/African-American, Asian, Native American, sexual or gender minority, or girls with a disability, among others. Yet, recent qualitative research with African-American (Goodkind et al., 2020) and Native American (Banyard et al., 2022) girls has found that relational and collective intervention strategies can have meaningful effects on girls’ confidence, relational health, and overall resilience. Among lesbian, gay, bisexual, transgender, and queer (LGBTQ+) youth, relational connections through LGBTQ+ community centers has been found to promote many qualities similar or identical to those defining RCT's growth-fostering connections: authenticity, engagement, and empowerment (Gamarel et al., 2014). The alignment of these studies with RCT core concepts suggests the potential for RCT-based intervention as a theoretically-grounded approach to healing and treatment for multiple diverse populations. Additional research is needed to pilot and explore these possibilities.
Limitations
Several study limitations warrant consideration. First, the exclusion of books and book chapters limits our integrated understanding of this topic to the more narrow body of academic literature contained in peer-reviewed articles and dissertations. Second, all of the studies included in this review were written in the English language and used U.S.-based samples, thus limiting our knowledge of RCT interventions to those developed from a Western perspective. Third, some studies about RCT interventions were excluded because they did not meet the inclusion criteria for this study, but could still add insight and perspective to this topic. Lastly, there is room for growth in the methodological rigor in this body of research. Limited details were provided about each study's analytic approach, and many qualitative studies reported that “themes were identified,” without describing analytical steps, coding approach, or steps taken to establish trustworthiness–an important element of rigor in qualitative studies (Lietz et al., 2006). This limitation exacerbated the inherent challenges in synthesizing studies with such diverse methodologies (e.g., quantitative, qualitative, single case study design).
Implications for Future Research and Practice
Several areas for growth in RCT intervention research were identified in this study, including enhanced methodological rigor and measurement of intervention effects and participant outcomes, expansion of diverse focal populations, and incorporation of modern research on interpersonal neurobiology, bias, and oppression in adolescence. Future RCT intervention research would benefit from focused implementation with adolescent girls from a broader variety of underrepresented groups, and integration of a more explicit anti-oppressive lens, as illustrated in Joe et al.'s (2020) RCT-based work with BIPOC adult women survivors of domestic violence. RCT was developed as a culturally-responsive feminist model of practice, and findings from this review revealed that participants felt empowered by RCT practice strategies that involved sharing cultural- and gender-specific experiences with their intervention groups. However, none of the included interventions were explicitly informed by an anti-oppressive lens, which could more directly attend to participants’ intersectional identities, experiences with privilege and oppression, and the healing power of collective action.
From a practice perspective, RCT offers a culturally-sensitive, gender-responsive, and relationally-centered approach to therapeutic work with adolescent girls. Practitioners seeking to translate the principles of RCT into social work practice strategies may use this review as an inventory of therapeutic strategies, as well as a catalog of RCT interventions that have been piloted with adolescent girls. Additionally, this review may serve as a springboard for practitioners and researchers seeking to develop and pilot new RCT interventions, based on the identified areas for future research and intervention work.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.