
Abstract
Many women experiencing homelessness and intimate partner violence (IPV) often do not use formal support services due to barriers such as finances, inaccessibility, controlling partners, and stigma. The current literature lacks studies that examine the formal service experiences of women who have undergone both homelessness and IPV. Therefore, the current study used a qualitative-dominant design and explored the formal service needs of these women, barriers and facilitating factors associated with accessing services, and how the women's identities affected their experiences with formal services. Interviews with 10 women were conducted, and a reflexive thematic analysis was conducted using a critical feminist and intersectionality lens. The most common factors that led to homelessness were conflict and precarious circumstances leading to housing instability. Common barriers were systemic, psychological, dismissal, minimization, and financial barriers. The most common needs were health, finances, and basic necessities. The most common facilitating factors were support networks and resilience, growth, and proactivity. The social positionings most commonly affecting their experiences were class and race/ethnicity. These findings highlighted the voices of marginalized women and can be used to implement positive change in formal services that cater to this subgroup of women.
Introduction
In Canada, more than 235,000 individuals experience homelessness within a given year (Gaetz et al., 2016). This group faces a multitude of adversities such as mental health disorders, chronic health diseases, lack of basic needs, unemployment, and financial struggles (e.g., Daiski, 2007; Rodriguez-Moreno et al., 2020). Compared to the general population of homeless individuals, women are more vulnerable to experiencing these hardships and less prone to using formal services due to the number of barriers they face. Formal support services refer to assistance from a trained professional and are available to the general public (Shiba et al., 2016). Specific barriers for this population include difficulty getting information, a lack of finances, insufficient availability of services, cultural barriers (e.g., language), and stigma (Campbell et al., 2015; Narendorf, 2017; Ponce et al., 2014). Relatedly, homeless individuals experienced increased risks during the COVID-19 pandemic, such as higher exposure to the virus, medical comorbidities, and lack of access to care and treatment (Baral et al., 2021).
Intimate Partner Violence Barriers
Although numerous factors can contribute to a woman becoming homeless, it is well-known that one of the leading causes is intimate partner violence (IPV; Sullivan et al., 2019). IPV is defined as, “behaviour by an intimate partner or ex-partner that causes physical, sexual or psychological harm, including physical aggression, sexual coercion, psychological abuse and controlling behaviours” (World Health Organization, n.d.). Barriers to accessing formal services are especially prevalent for women who experience IPV (Barrett & St. Pierre, 2011; Rodriguez et al., 2009). For example, women enduring IPV often experience high rates of mental health disorders, physical health problems, and a lack of shelter if they flee their abusive relationship (Ponce et al., 2014; Vijayaraghavan et al., 2012). Despite the need for help and safety, these women often experience barriers such as being controlled by their partner or feeling embarrassed about being an IPV survivor (Ponce et al., 2014; Wilson et al., 2007). These women often do not seek services for their needs because of these barriers (Ponce et al., 2014; Wilson et al., 2007). In addition, the COVID-19 pandemic undoubtedly impacted the frequency of IPV and the barriers to services. The stay-at-home orders and the pandemic, in general, led to an increased risk of experiencing IPV due to being isolated with an abusive partner for extended periods of time (Nnawulezi & Hacskaylo, 2022). It was also more difficult for survivors to access resources like transportation, food, and employment (Nnawulezi & Hacskaylo, 2022).
Many studies have been conducted with women experiencing homelessness and women who have endured IPV; however, studies examining both homelessness and IPV in conjunction with women's experiences with formal support services are less numerous. Therefore, the purpose of this study was to explore the experiences of women who endured both of these adversities while examining the barriers and facilitating factors to accessing formal support services. Furthermore, it was important to consider the impact of the COVID-19 pandemic on women's experiences with formal support services due to the study being completed following the pandemic restrictions.
Feminist Theories
Feminist theories, in the context of IPV, view behaviors related to IPV in terms of larger societal structures and the general sociocultural context rather than studying pathology on an individual level (Lawson, 2012). Although different waves of feminism view IPV differently, generally, radical feminism views IPV through the lens of gender, stating that gender plays the most central role in these acts of IPV, followed by variables of power and dominance (Dobash & Dobash, 1979). Specifically, the inequality between the socially constructed genders is often cited by many feminist theorists as a leading factor in the occurrence of IPV (Chesworth, 2018).
Taken together, a fundamental view is how gender has been socially constructed. Society has sorted specific behaviors and paired them with a particular gender, leading to what constitutes “male” as being superior (Chesworth, 2018). These sociological theories further examine IPV by dissecting sociocultural factors (Chesworth, 2018). More notably, radical feminism stands on the notion that violence toward women occurs in order for men to have power and control over women; this is the byproduct of a patriarchal society (Dobash & Dobash, 1979). However, it is important to note that not all violence is perpetrated by men toward women. Nonetheless, feminism is still important to consider in this context.
Homelessness can also be viewed as a feminist issue (O’Brien, 2023). Previous definitions of homelessness have not taken into consideration the gendered and lived experiences of women and those who identify as anything other than male (Wendt & Moulding, 2016). Feminist theories often view homelessness as directly related to gendered violence, such as unequal gender and power relations within society (e.g., unequal pay and domestic violence) (O’Brien, 2023; Wendt & Moulding, 2016). Overall, feminist theories provide us with an understanding of some of the root causes and potential reasons why women experience IPV and homelessness today.
Intersectionality Theory
The literature discussing barriers to formal services explores the relationship of identity and social positioning with experiences of oppression, systems of power, and social inequities (Atewologun, 2018; Chavis & Hill, 2008; Kelly, 2011). The theory of intersectionality is a critical framework that posits that we should be examining the impact of social categories together and consider how they converge to influence individual experiences, as well as investigating the relationship between these categories and structural systems of privilege and oppression (e.g., racism and sexism) (Atewologun, 2018; Crenshaw, 1991).
In terms of IPV and formal service use, the additive effects of all social categories that are part of a woman's identity result in each person having their own distinctive experience (Chavis & Hill, 2008). As we know from previous literature, the intersection of gender and socioeconomic status (SES) can affect service usage, such that women with lower SES are more likely to experience mental health concerns and less likely to seek formal help due to barriers like finances (Narendorf, 2017). An increase in the number of marginalized identities one identifies with often leads to an increase in the level of oppression experienced by the individual (Weldon, 2008). Overall, an individual's social categories can affect the barriers they face in accessing formal services and influence how structural systems affect their experiences (Chavis & Hill, 2008). This study aimed to fully consider the participants’ intersecting identities and how they relate to and affect their experiences.
The Current Study
The following study aimed to understand the service experiences of women who endured homelessness and IPV. We also examined the formal service needs for this subgroup of women, the barriers and facilitating factors to accessing formal services, and how the women's social positionings affected their experiences with these services. Due to the exploratory nature of the study and the qualitative-dominant methodology, there were no proposed hypotheses. Qualitative methods were chosen for this study because they allow us to get a deeper understanding of an individual's perspective and personal experiences. Further, qualitative methods are able to capture the complexity of the real world (Braun & Clarke, 2013). This study explored four research questions:
What are the formal service needs of homeless women experiencing IPV? What are the barriers to accessing formal services for homeless women experiencing IPV? What facilitates successful help-seeking for homeless women experiencing IPV from formal service providers? How do the social positionings and standpoints of homeless women who are IPV survivors shape their service needs and experiences when accessing formal services?
Method
Recruitment
Ten women who resided in Windsor, Ontario, Canada, were recruited through convenience sampling from the Welcome Center Shelter (WCS), a homeless shelter for women and their families. The organization granted access to the primary investigator (PI) to visit the site and recruit participants. The researchers visited the organization once a week, for three months, at the center's drop-in sessions to recruit participants. Grant money from the PI's supervisor was used to fund this project and compensate the participants.
Criteria for participation included being homeless or in an unstable housing situation and having experienced IPV with a past or current romantic partner, ranging from minor to severe. The WCS does not specifically serve women who have experienced IPV, but the staff indicated that the IPV rates of the women using their services are high. Therefore, it was feasible to recruit from this location. The participants also had to have functional skills in reading, writing, and speaking in English, and they had to be 18 or older.
Measures
A qualitative-dominant design was used for this study while incorporating three brief surveys, including demographics, The Experience of Domestic Violence Scale, and the Intimate Partner Violence Strategies Index (IPV-SI). Analyses included calculating percentages and mean scores. The demographic survey asked about the participants’ age, race and ethnicity, gender, sexual identity, living situation, education level, relationship status, current employment status, disability status, number of children, and the country in which they were born.
The Experience of Domestic Violence Scale measured the levels of IPV experienced in a current or past romantic relationship (Fujiwara et al., 2010). For this measure, Cronbach's alpha is .86, which demonstrates good reliability (Fujiwara et al., 2010). IPV-SI measured the strategies used to access safety when experiencing IPV (Goodman et al., 2003). The authors of this scale concluded that the IPV-SI has good interrater reliability, face, and convergent validity (Goodman et al., 2003).
Interviews
The interviews were planned for 60–90 min and ranged from 14 to 85 min (M = 40.4). They were semistructured and audiorecorded, and the PI and one volunteer researcher conducted the interviews. The following topics were discussed: living situation, formal support needs relating to homelessness and IPV, barriers and facilitating factors for accessing formal support services, how their social positionings may have affected experiences with formal support services, and the effect of the COVID-19 pandemic on service experiences.
Procedure
The project received clearance from the University Research Ethics Board. Before data collection, the PI and the second interviewer watched a webinar that provided them with a general discussion of IPV. The participants were then invited to sign up for the study at the WCS. The shelter residents were told they could sign up under a time slot by providing their first names. All other forms with data (consent form, surveys, and transcripts) used ID numbers. Interviews were conducted at the WCS in private rooms. The participants provided informed consent verbally. During the study completion process, the researchers were present to assist with clarifications or help with reading. The participants were also allowed a support person in the room.
Questionnaires were completed first, followed by trauma-informed interviews (Lalonde et al., 2020). A trauma-informed approach involves incorporating strategies into interactions with participants who have endured trauma that create a physically and emotionally safe environment for them to share their stories. For example, this included asking participants if they wanted a support person in the room, taking frequent breaks, providing water and snacks, and conducting the interview in a familiar environment (for more information on trauma-informed approaches, see Lalonde et al., 2020). Participants were informed that mentions of child abuse or other duty-to-report instances might need to be reported. There was also ongoing consent to ensure that they wanted to continue. Upon conclusion of the interview, participants were given a letter of information with resources for mental health, domestic violence, and shelter services, and a $25 gift card.
Analyses
The interviews were transcribed and deidentified, and a reflexive thematic analysis (RTA) was used to analyze the interviews to explore individuals’ experiences and how they make sense of them (Braun & Clarke, 2021). The RTA followed Braun and Clarke's six steps and involved identifying codes within the dataset that were conceptually similar and turning them into themes that can be revised throughout the analytic process (Braun & Clarke, 2021). The RTA was approached from a feminist standpoint. This theory recognizes that knowledge and experiences are socially situated; therefore, strong reflexivity is essential, where the researcher acknowledges and interrogates their positionality and subjectivity (Wigginton & Lafrance, 2019). This approach also aims to highlight the voices of marginalized individuals (Wigginton & Lafrance, 2019).
Critical feminist and intersectionality interpretive lenses were also used to inform the decisions made by the researchers. Questions were asked around power relations, and reflection occurred on how questions were being asked (Lafrance & Wigginton, 2019). This lens was also used to analyze the experiences of oppressed social groups and how their positions lead to inequality in accessing resources (Chavis & Hill, 2008; Kelly, 2011). Overall, these lenses helped inform the research process, data analysis, and write-up.
Trustworthiness and Positionality
To establish trustworthiness, a volunteer researcher helped with the RTA coding process. This researcher coded 7/10 interviews, while the PI coded all 10. The PI and research assistant also used reflexive journals (Nowell et al., 2017). In these journals, the researchers kept track of their analytical and methodological decisions, thought processes, assumptions, and reflections on the study's processes (Nowell et al., 2017).
Positionality is also important in qualitative research for the readers to understand how the researcher's background can shape the research (Braun & Clarke, 2019). I, the PI, am a 25-year-old woman. I have never experienced homelessness or IPV. However, I have experienced barriers to accessing formal services. I have been put on waitlists, struggled with paying for services, and have been doubted by service providers. These experiences have made me hesitant to access further services when I need them. Part of the reason I chose to do this research was because of past obstacles I encountered and wanting to make a change for those who are vulnerable to more barriers than I have faced. These personal experiences can and have affected how I view some formal services, such as medical professionals and the healthcare system, so it was important to be reflexive throughout the project to ensure these experiences did not distort how I interpreted the findings and interacted with the participants.
The other researcher identified as a cisgender woman and has had the security of stable housing throughout her life. She attributed the experiences she gained as a residential youth worker as formative in her research interest development. The treatment program where she was employed offered support to a resilient population with complex traumatic histories and experiences of dating violence. This exposure shaped her understanding of the social world and gave rise to her interest in bridging the research–practice gap, which, in turn, was something she regularly reflected upon throughout her involvement in this study.
Results
Demographics
The mean age of the sample was 44 years old (range = 28–70), all participants identified as female, and all were born in Canada. The length of time being homeless for the sample varied from 3 weeks to 3.9 years (M = 30.8 weeks). The average number of times being homeless was three. See Appendix A, Table 1, for the remaining demographic statistics.
Quantitative Findings
All participants scored above zero on the Experience of Domestic Violence Scale, where scores can range from 0 to 12. Sixty percent of participants’ results demonstrated the maximum score on the scale (M = 11.1). This indicated high rates of domestic violence in the sample.
IPV Strategies Index
The most endorsed strategies on the IPV-SI were Resistance and Placating. In the placating category, 90% of the women tried to avoid an argument with their partner. In the resistance category, 90% of the women fought back physically and verbally and left their homes to escape their partners. The calculated percentages for the average number of strategies used on each subscale were as follows: 38% for Formal Network, 40% for Legal, 42% for Safety Planning, 57.2% for Informal Network, 82% for Placating, and 83% for Resistance. The scores for the helpfulness levels were not calculated because of excessive missing data.
Qualitative Findings
Five domains were created in the RTA process: Factors Leading to Homelessness, Needs of Women Experiencing IPV and Homelessness, Barriers to Accessing Services, Facilitating Factors, and Social Positionings’ Effect on Homeless Experiences and Access to Barriers.
Factors Leading to Homelessness
The main factor leading to homelessness was Conflict and Precarious Circumstances Leading to Housing Instability. All the women in the study became homeless due to conflict or precarious, unstable situations. The types of conflict consisted of human trafficking, IPV, landlord, and/or familial conflict. Multiple participants became homeless due to fleeing an abusive romantic partner. Trafficking was perpetuated by a wide range of individuals. Women reported being trafficked by individuals, known and trusted by survivors, such as service providers and financial supports. Landlord issues were discussed, including not paying rent on time, being forced out of their unit for no legitimate reasons, or not having the correct paperwork.
These precarious circumstances continued to be a pattern in many women's lives as they continually attempted to find housing. A few women described conflict between roommates and other women at the shelter, disputes and dissatisfaction with the other women they roomed with, and difficulty finding housing with roommates. For example, one participant said, “They give you heat, shelter. I can't say anything wrong about this place. The only thing is thieving. Stealing and stuff like—we all have to live together. We all have nothing. Come together like, you know what I mean?” Overall, precarious situations were the most prevalent factor leading to homelessness, which continued for some while the women were trying to get back on their feet. This theme demonstrated both the internal and external circumstances of the system and being housed with others who were likely to cause or heighten conflict.
Needs of Women Experiencing IPV and Homelessness
Three subthemes were generated regarding the participants’ needs: The Foundation to Survive, Health and Wellbeing, and Employment and Financial Assistance.
The Foundation to Survive. All 10 women described the need to have shelter. This was either expressed in the difficulty in finding housing or in describing the importance of housing for meeting other needs (e.g., employment). One participant discussed the importance of having a place to live, “Well, I’m a firm believer that you need a home first in order for everything to fall into place. Because you need a place.” Another participant described needing shelter first, followed by essentials like food and clothing. Some women mentioned a strong interest in transitional living. Other desired basic needs: access to food banks, identification mechanisms, and clothing.
Health and Well-being. All participants described some form of health need, whether it was a physical or mental health need. Professionals such as counselors, therapists, and social workers were the most common need. Not every woman recognized this need for themselves, but other supports in their life did. One participant also expressed needing self-esteem building in relation to mental health, despite not stating a need for individual therapy or counseling.
Physical health needs involved surgeries, medications, consultations with a primary healthcare provider, as well as gym/fitness needs. For example, one participant experienced extensive injuries due to IPV and expressed her need for medical care for “broken bones and seizures.” A need for medication was also expressed as well as referrals to healthcare practitioners.
Employment and Financial Assistance. The final subtheme was employment and financial needs. Women mentioned the need for financial assistance and employment and desiring help with finding employment opportunities. One participant expressed the difficulties of finding employment when you do not have your basic needs met: “—but it's hard to have a job when you have no place to wash clothes or wash yourself, never mind clothes.” Participants also expressed not having enough money to access certain environments and being looked down upon for their lack of money. Others expressed wanting assistance with finding part-time jobs to slowly transition back into work. Further, one participant also expressed the need for skills-building workshops and training to prepare herself for the workforce.
Barriers to Accessing Services
There were four subthemes concerning barriers to accessing formal services for homelessness and IPV: Strained and Flawed systems, Psychological Barriers, Experiences of Dismissal and Minimization, and Financial Obstacles.
Strained and Flawed Systems. The most common theme surrounding barriers to accessing formal services was related to flawed systems. The women often expressed being put on waitlists, insufficient availability of beds and providers, a lack of rooms accommodating specific needs (e.g., dog friendly), or a lack of availability for needed services. This is demonstrated by a participant's long wait time for mental health treatment, “I was on their waiting list for posttraumatic stress for 5 years.” The waitlist barrier was magnified during the COVID-19 pandemic, such that participants expressed how shelters had insufficient bed space and experienced longer waitlists compared to prepandemic times.
Multiple participants expressed difficulties with getting into a shelter due to insufficient space. This barrier also occurred for human trafficking services and sober living services. One participant noted that this obstacle could contribute to “life or death”: There's 10 beds in (city), um, for women who want to live sober … by the time somebody gets up on the list, they've either tried to kill themselves, or are in the psych ward, or they're out homeless, using drugs and are probably in psychosis, and have no idea what to do with themselves … When you're on a waitlist for a treatment center, or for sober living, or for (the nonprofit mental health organization), or for a family doctor, that's life or death for addicts especially, and people who are already homeless.
Another issue the participants described, specifically at the shelter, was a lack of pet-friendly rooms and other restrictive requirements for staying in particular rooms. Two participants described their experience of dog ownership while homeless and reported that they were unable to keep the dogs at the shelter. This led to distress for these women, as they considered their pets to be a part of their family. Another participant had difficulty with getting a particular room at the shelter due to requirements for family and single rooms, as she could only stay if she had a child with her. To conclude, many of the described barriers related to how systems have been structured, leading to waitlists and insufficient space.
Psychological Barriers. Another barrier revolved around women's emotions, perceptions, and mental health. One participant said, “I was scared” when talking about barriers to accessing services, and another stated that “the emotional part” years ago got in the way of help-seeking. It was also scary for another participant, as she said, “Violence is to tell … To tell somebody or to tell.” Emotions, such as pride, further impeded participants’ ability to seek help.
There were also expressions of not being ready for help. One participant specifically expressed that her mental health state affected her ability to reach out for help: I would say number one reason would be my anxiety, depression … It holds me back from doing a lot of things … and it's almost like it started with like PTSD through the domestic violence—And kind of grew from there …
These findings demonstrate the impact that emotions and individual perceptions of readiness have on participants’ ability to seek out help and formal support services.
Experiences of Dismissal and Minimization. Participants reported instances of not being taken seriously by service providers, including police officers, doctors, shelters, and services for human trafficking. Participants stated that they “always get turned down” or that “they (the service providers) didn’t care.” Three participants described instances with police officers who were dismissive, disrespectful, lacked empathy, or did not attempt to help them. Comments were made about police officers in relation to power and how women reported feeling that the police officers desired to maintain dominance over them while also lacking care during their interactions. All these experiences demonstrate the common occurrence of being dismissed and belittled by providers, leading to services not being utilized by those in need.
Financial Obstacles. A few women expressed financial obstacles when attempting to access services (e.g., transportation and medical services), or how in general, life as a homeless individual is unaffordable. For example, one participant pointed out that, “Homelessness is not cheap, by the way. It is not. It's very expensive to be homeless. Let me tell you that.” Others discussed the difficulty of trying to pay for services such as medical care such as surgery. Due to delays in accessing services, participants endured pain for years. Two participants noted difficulties in relation to getting or paying for transportation. One talked about the frustration and financial strain of paying for her child's transportation between the school and the shelter, “… $120 for 2 days of school … $60.00 a day.” Overall, financial barriers further impeded participants’ ability to access the services they needed.
Facilitating Factors
There were two subthemes that became evident in relation to facilitating factors for accessing formal support services: Supportive Networks and Resilience, Proactivity, and Growth.
Supportive Networks. The most prevalent facilitating factor was social support. The nature of this social network varied and consisted of family, friends, other women at the shelter, staff, or the providers of services. The women talked about feeling supported by others in their lives who encouraged them to get help and provided help when they were in need. Some noted that the providers they saw showed support by pushing them to do better and displaying transparency and honesty. This was reflected by a participant's statement when talking about her counselor, “I think ‘cause she's real. She doesn't beat around the bush, she’ll tell me exactly how it is.” Others talked about how “amazing” and “helpful” service providers have been for them, other than just providing the required services.
Some women noted that they receive a lot of support from their family members, who often encourage them to get help and leave their precarious circumstances. Supportive networks also came from those at the shelter, both the other residents and the staff. Some women were able to make connections with other residents, reported being treated nicely, and did not feel judged by those around them. A participant reflected on the support and connections made with other women at the shelter: I think the other thing too is support among people and not necessarily professionals, but sisters among sisters women among women. Even men among women. Like sharing experiences because you do, you do pick up people that you bond with here and like for instance, (name of other resident) and the baby. I laid eyes on that baby. I laid eyes on (name of other resident) and within minutes I knew she could be my friend. She is—We could be connected and we were and we became friends.
Similarly, other participants discussed how well they were treated at the shelter. Overall, the women described receiving social, emotional, and instrumental support from many individuals in their lives that facilitated their ability to seeki support services.
Resilience, Proactivity, and Growth. Some women's stories demonstrated that their resilience, proactivity, and growth as a person were facilitating factors in their journey of seeking support services. Participants talked about being proud of themselves and being able to open up more. Others reflected on putting in their own effort and being proactive, leading to them getting help. Similar sentiments were shared by other participants about finally putting in the effort to take care of themselves and showing self-love; this was exhibited by the following quote: “I got to take care of me. It's time … I did it for me, not for anybody else, so I've learned different things that work for me.”
One other participant also emphasized being proactive, and how this helped her get the services she needed. She discussed doing her own research and finding information for services on her own. Others emphasized being strong-willed and standing up for themselves when they did not get treated well. Another participant discussed the difficulty of being on disability, and how she must be strong because of it, “When you're on disability, and like you know, you've got all these three strikes against you, it's harder. And if you don't have a voice, you gotta have a backbone.” Overall, these women demonstrated resilience, strength, and being proactive as facilitators in moving forward with getting help and assisting themselves.
Social Positionings’ Effect on Homeless Experiences and Access to Barriers
Although most participants did not believe that their identity or social positioning affected their homeless experiences or ability to access services, there were two subthemes that were generated from the interviews: class and race/ethnicity.
Class Social Positioning. Some women expressed the effect of their class, or SES, on their experiences with homelessness and with formal support services. Being currently homeless and part of the lower class resulted in others treating them differently, including lack of respect and being looked down upon, taken advantage of, and stigmatized. One participant described being spoken to inappropriately due to her class. This was also emphasized in the following quote from a participant who originally came from a well-off family: … I was raised in a very, very well, well-off family. I chose to be on my own. And it's like … I can go with my family somewhere and get anything I wanna in society, but when I walk into a store myself, I'm labeled. Why am I labeled? Like, I have $6,000 in my pocket I'm going to buy something. But I—you're following me around the store.
Two participants described that the intersection of health and class led to difficulties for them during their homeless experiences and when trying to access services, leading to oppression and a harder time gaining employment. One participant shared an experience that also included gender, being a woman, in this intersection, “You got disability, you got gender you got income. All three. That is so hard to get through to people that, you know, and keeping us oppressed in this country is all part of their strategy too.” Overall, this theme demonstrates how the effect of one's social class and its intersection with one's health identity leads to negative experiences and stigmatization by the greater community.
Race/Ethnic Social Positioning. Two of the three non-White participants touched on experiences with race and ethnicity and described the effect of their identity as significant to their experiences. Both participants described how their ethnicity/race made it much more difficult for them to access services, led to them being denied services or not taken seriously, or led others to think that they did not deserve what they had due to their identity. While one of these participants did not consent to the use of anonymous quotations, she described in great detail her experiences with systemic racism and how racism impacted her experiences being homeless and trying to access formal support services. Her identity as a woman of color exposed her to racial slurs and assumptions of her worthiness for financial support, which contributed to her experiences with violence and homelessness. This further affected her experiences with finding housing after becoming homeless, as some landlords expressed racist behavior and did not want someone of her identity in their unit. Finally, she expressed that she felt others looked down on her and saw her as “less than” due to her identity.
The other participants expressed similar experiences. She faced racism in health services, the bank, and other services. She mentioned experiencing racism when trying to get approved for a mortgage: I couldn't even—I had money in the bank to have—to get a mortgage. The bank(er) that I dealt with did everything in her power, this manager, to make sure I couldn't get a house. A mortgage. She called everywhere and told them, ‘don't give her a mortgage. Don't give her a mortgage. ‘Aboriginal.’
Both participants expressed experiencing racism, and this impacted their ability to access formal services. This demonstrates the intersectional relationship between identity and structural systems of both privilege and oppression.
Discussion
The purpose of this article was to explore the formal service experiences of women enduring homelessness and IPV. The quantitative questionnaires revealed high levels of IPV in the study sample. The measures also showed that the most common types of strategies for getting help for IPV involved resistance and placating. These findings are noteworthy because using both strategies can imply that survivors are starting with one strategy and moving on to the other when it becomes ineffective. Researchers should examine the directionality of these strategies to understand what external factors contribute to a woman's decision to switch strategies.
Qualitative Findings
The thematic analysis showed three important needs for the group of women in this study: health, basic necessities, and employment and finances. The latter finding is consistent with previous studies that emphasize financial support as a need for those experiencing homelessness and those fleeing from partner violence (e.g., Campbell et al., 2015; Chiaramonte et al., 2022). Past studies also support the findings that mental and physical health needs are important for this subgroup of women (e.g., Daiski, 2007; Guenzel et al., 2020).
The most common reason for experiencing homelessness in this study was conflict and precarious circumstances that led to continuous housing instability. Conflict, especially partner violence, is a leading cause of homelessness, so it was no surprise that this was the most common factor leading to homelessness for this sample (Daoud et al., 2016). These findings provide insight into the cyclical relationship between IPV, homelessness, and reoccurring conflict. This relationship shows an enduring obstacle for these women—violent circumstances—that affect their ability to find stable housing. This is helpful to know from an intervention standpoint to inform government services and agencies aimed at assisting women who face these circumstances.
The most common barriers for women accessing formal support services were Strained and Flawed Systems, Psychological Barriers, Experiences of Dismissal and Minimization, and Financial Obstacles. The findings support previous research that has demonstrated the barriers to services related to a lack of finances, overwhelmed medical systems (e.g., waitlists), and interpersonal feelings for women experiencing IPV or homelessness (e.g., Campbell et al., 2015; Fugate et al., 2005). These findings provide us with a new understanding of obstacles that are prevalent for this subgroup of women in the Windsor community and potentially other communities within North America. Overall, formal services must better serve the identified needs of women taking into consideration their unique circumstances.
Two factors facilitating access to formal support services were discovered in the findings: Support Networks and Resiliency, Growth, and Proactivity. These results are consistent with previous studies that point out how supportive networks help women become both more resilient and more likely to seek out help, while also acting as a safety strategy (Chiaramonte et al., 2022). Other studies have found that resilience, empowerment, and confidence are factors that assist women dealing with IPV, homelessness, and attempts to access support services (Livingstone & Herman, 2017). Researchers should inform service providers to expand their services and offer women resources such as workshops, courses, and support that promote resiliency, empowerment, and proactivity to aid in help-seeking.
Regarding social positioning, two themes were uncovered in the data: class and race and ethnicity. It was found that women's social class explicitly affected their experiences with being homeless and accessing services. Two of the participants’ race and ethnicity heavily influenced their service experiences. It is not a new finding that race and ethnicity affect access to services, as a review completed by Waller et al. (2022) examining the intersection of African-American women and their help-seeking experiences found that women of color often have poorer interactions with formal service providers compared to other populations.
The effect of social positioning on women's experiences can also be explained by the theory of intersectionality. Intersectionality examines how women's identities (e.g., age and (dis)ability) impact and influence their experiences and the association between these social positionings and structural systems of oppression (Atewologun, 2018). In this study, it was demonstrated that class, status, and race led to oppression, racism, and discrimination, making it more difficult for the women in this study to obtain services. Overall, the findings confirmed that identity can lead to disadvantages based on these systems of power that cause some identities to have privilege and others not.
These findings can also be applied to the field of social work. The study highlights the importance of networking and being part of a multidisciplinary team. Many women felt dismissed by providers, especially women of color, and they also discussed the importance of having a strong support network. Social workers should aim to help women communicate with other agencies, acting as personal advocates in situations where women are feeling unheard or dismissed. Being a part of a multidisciplinary team can aid in easier referrals and connections to other areas of need for clients. It is also important for social workers to take a trauma-informed approach during interactions with clients and attend trauma-informed training. For this study, the trauma-informed lens assisted with making participants feel comfortable and allowed the researchers to understand how trauma impacted these women's lives and interactions. Social workers can use this approach while working with women who have experienced violence and homelessness by being aware of how they respond to these traumas and by putting emotional and physical safety strategies in place (e.g., education on trauma associated with IPV and homelessness, considering locations, discussion of triggers, providing support person, using a diverse team, etc.; Lalonde et al., 2020).
Limitations
The following study had a few limitations. The sample was comprised mainly of Caucasian women. Therefore, the findings from the sample cannot be generalized to more diverse populations. This also limited the information that could be gathered on the impact of race and ethnicity on experiences with services. Despite this limitation, important implications of race and ethnicity did emerge from the two minority women present in the sample. The sample size of the study was also a potential limitation. The original aim was to gather 15 participants, but due to time, availability, and willingness, only 10 were attained. Qualitative research can be done on smaller sample sizes (Braun & Clarke, 2019), but a larger sample could have added richer findings. Regardless, the findings can still be used to help communities with extrapolation for the needs of non-White women. Finally, the study population consisted of women from Windsor, Ontario, which limits the findings’ generalizability. Nevertheless, the findings can aid and guide service providers in other communities that aim to improve their services or conduct research on barriers and facilitating factors to accessing their services.
Implications and Future Directions
There are multiple implications that resulted from this study. This project used a group that is not often studied in relation to barriers and facilitating factors for formal services—women who have endured IPV and are also experiencing homelessness. Therefore, the study adds to the literature that examines women who have or are experiencing both adversities. Future research can attempt to replicate these findings and examine more diverse groups in Canada.
The findings of this study will also be used to create a report for the WCS and other services in the wide-ranging community. This will allow the findings to be used to implement changes in protocol, procedures, and programs that are offered for the local shelter populations. Participants in this study did provide suggestions for the shelter that will be included in the report that could be used to further improve services (e.g., more nutritious and culturally diverse food). These suggestions can be used to implement immediate changes to the current shelter services and other formal support services at large. Service providers in Windsor and the broader community (i.e., North America) can also consider the larger barriers regarding systemic issues to inform change by working toward adding additional services, expanding the current capacity of their services, changing policy, and training their employees in empathy.
The findings point to a few avenues for future directions of study. The study consisted of mostly heterosexual women, with few who had differing sexual identities. Future studies could aim to access populations from more varied backgrounds and attempt to include a sample of more diverse sexual identities. This would allow for a better understanding of the intersection between sexual identity and women's experiences with accessing formal services for needs related to homelessness and IPV. Finally, this study was conducted with a qualitative-dominant methodology. Mixed method designs are capable of leading to a greater understanding of the phenomenon being studied (Ponterotto et al., 2013). Quantitative components can be used to gain larger samples, and qualitative components (e.g., focus groups) can provide rich narratives that are more detailed. Overall, using mixed-methods approaches in future studies can help us further enhance our understanding of the experiences of women and IPV, homelessness, and formal service use.
Conclusion
To conclude, this study explored the experiences of women enduring homelessness and IPV and the factors affecting their access to formal support services. First, the findings highlight barriers related to overwhelmed systems, dismissal and minimization of women's issues, as well as psychological barriers, and financial concerns. Second, findings emphasized the factors that aid this group of women to seek help, such as having supportive networks and being resilient, proactive, and finding ways to enable personal growth. Third, this study demonstrated that social positionings such as race and class can lead to discrimination and oppression within structural systems when women try to access services. Finally, the study identified the common needs of this population, including health, finances, and needs related to basic necessities (e.g., housing and food). In summary, the current study provided rich information about barriers and facilitating factors to accessing formal services for women experiencing IPV and homelessness and can be used to implement change in many communities that provide services for these populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research and/or authorship of this article: Associate Dean Research Grant (Grant No. 820855).
Author Biographies
Appendix A: Demographics
Demographic Characteristics of Sample.
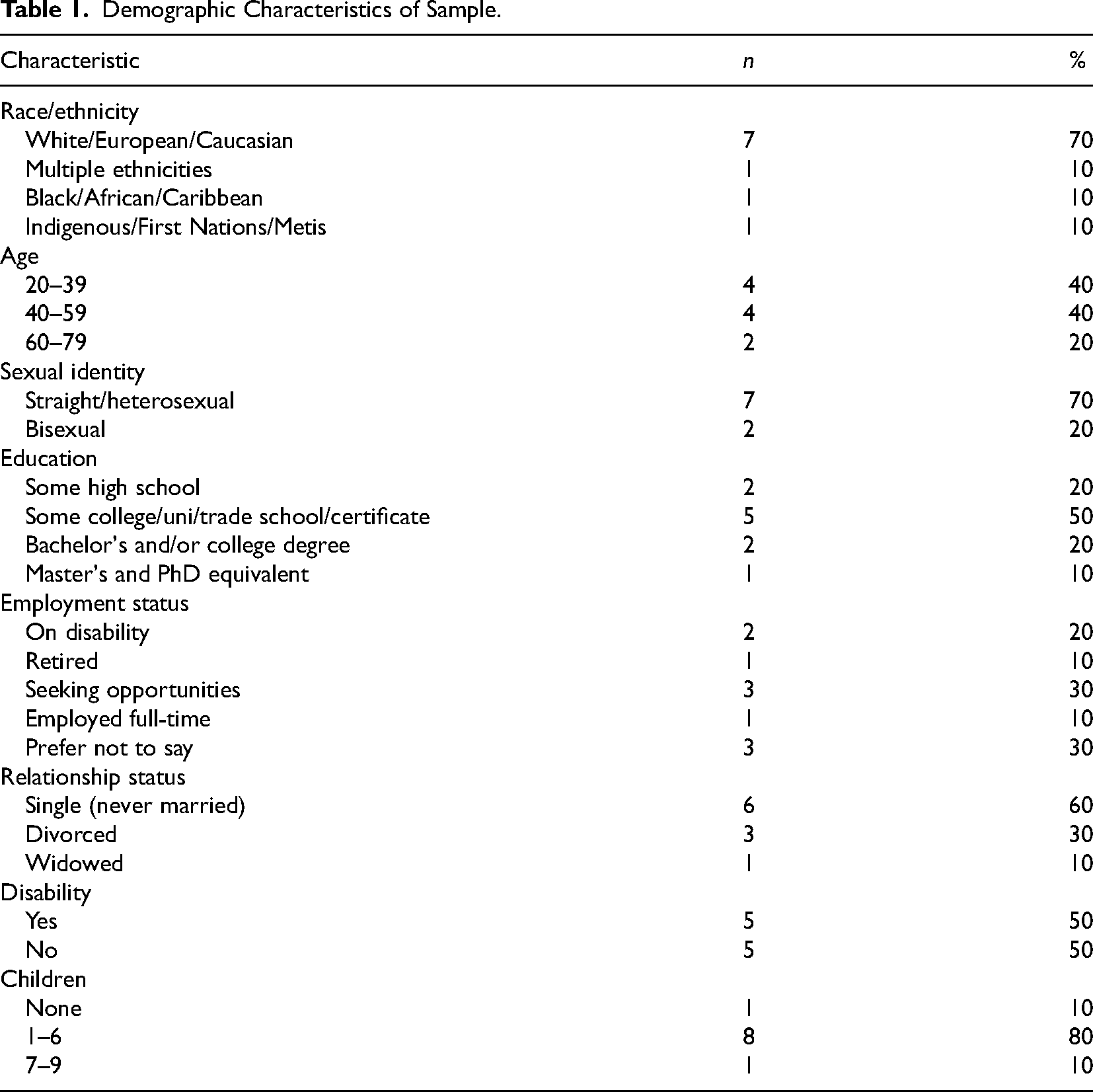
| Characteristic | n | % |
|---|---|---|
| Race/ethnicity | ||
| White/European/Caucasian | 7 | 70 |
| Multiple ethnicities | 1 | 10 |
| Black/African/Caribbean | 1 | 10 |
| Indigenous/First Nations/Metis | 1 | 10 |
| Age | ||
| 20–39 | 4 | 40 |
| 40–59 | 4 | 40 |
| 60–79 | 2 | 20 |
| Sexual identity | ||
| Straight/heterosexual | 7 | 70 |
| Bisexual | 2 | 20 |
| Education | ||
| Some high school | 2 | 20 |
| Some college/uni/trade school/certificate | 5 | 50 |
| Bachelor's and/or college degree | 2 | 20 |
| Master's and PhD equivalent | 1 | 10 |
| Employment status | ||
| On disability | 2 | 20 |
| Retired | 1 | 10 |
| Seeking opportunities | 3 | 30 |
| Employed full-time | 1 | 10 |
| Prefer not to say | 3 | 30 |
| Relationship status | ||
| Single (never married) | 6 | 60 |
| Divorced | 3 | 30 |
| Widowed | 1 | 10 |
| Disability | ||
| Yes | 5 | 50 |
| No | 5 | 50 |
| Children | ||
| None | 1 | 10 |
| 1–6 | 8 | 80 |
| 7–9 | 1 | 10 |