
Abstract
Taking a feminist and intersectional approach, this article conducts a socio-political analysis of the traditional paradigms of disability through an ethnographic study of the life histories of women with functional diversity (FD). In Spain, the term “people with functional diversity” has emerged as a preferred denomination for many, if not all, people and entities working in this field because it emphasizes the contribution of people with FD to society. Based on interviews with six study participants, the analysis examines these women's discourses and the different ways that they deconstruct traditional models of disability and ableism and the patriarchal and capitalist social categories that constrain them in positions of inequality and oppression. In particular, the analysis centers on the different ways of “being” a woman with FD and the transformative capacity of agency in overturning traditional representations in favor of plurality and inclusiveness. By challenging marginalized social categories, the women claim ownership of their bodies and sexuality and also open routes to social resources. Nevertheless, the research also shows that these resistances often took place at an individual rather than a collective level. Hence, while emphasizing the agentive capacity of the participants, the study shows how each of their biographies is framed within a socio-political context. This research makes an important contribution to the theory and practice of social work as it questions the traditional categories of FD and brings us closer to the lived experiences and practices of the study participants.
Introduction
Although the term “people with disabilities” is accepted by many of the most important international organizations such as the World Health Organization (2001) and the United Nations (2006), in Spain, the denomination “people with functional diversity” is preferred by many people who have disabilities and the entities that support them. Nevertheless, it is important to point out that it is yet to be fully accepted in the fields of research and service provision. As a woman with functional diversity (FD), as a researcher, and as an experienced social worker, I believe that the use of this term signals an important transformation in meaning from a homogenous view of limitations and exclusion to a productive view of diversity as a contribution of subjects to contemporary society. As this study examines the subjectivities of Spanish women with FD, I use the term to better reflect how this community represents itself and this new paradigm. Nevertheless, when referencing the work of other authors, I employ the terminology used in the original text.
Since the 1970s, research on people with FD in the fields of social sciences, specifically anthropology, has increased. This interest first arose within the North American cultural perspective and the materialist tradition of British sociology, which became the birthplace of the new field of Disability Studies. Studies by theorists and activists such as Michael Oliver (1990, 1998) and Jenny Morris (1991), amongst others, helped to formulate the theory of oppression and the social model of paradigm of disability.
Feminist Disability Studies arose from this context in the 1990s. One of the leaders of this movement was Jenny Morris, an activist and journalist highly committed to the defense of the rights of people with FD. Morris (1997) put forward the need to articulate gender and FD, and called for the feminist movement to highlight the experiences of women with disabilities. She argued that there is no abstract concept of women, only women in different contexts, occupying different positions of subordination or hegemony within identitarian systems.
Feminist theory provides Disability Studies not only with a gender-based approach but also with a socio-political critique that reveals the relationships of subordination resulting from the categories attributed to bodies. In this respect, feminism is a theoretical perspective that examines the discourses and categories that govern bodies and the intimately close relationship between subordination and patriarchal culture (Garland-Thomson, 1997, p. 21). On the other hand, feminist anthropology analyses the relationships of inequality stemming from the socio-sexual order. It critiques, analyses and explains the dominant relationship of men over women. In the 1990s, it primarily gave rise to conceptual frameworks that analyzed and established the myriad ways of being a woman, thereby expanding the initial focus of the discipline on the hierarchical relationship between the sexes (Méndez, 1995). This approach is guided by feminist intersectionality and helps explain how the axes of powergenerate different forms of discrimination. As a result, the articulation of the axes of patriarchy and FD can be analyzed along with the social markers of class, ethnicity, age or social preference, in order to examine the discrimination experienced by women with FD (Crenshaw, 1989). Social actors, both women and men, are placed in many different social positions, which determine the organization of the primary relationships or structures of power. These in turn cause a differentiation in the distribution of symbolic and material resources while producing and reproducing different forms of oppression and exploitation, thereby generating the identities and discourses that promote participation in and the transformation of the social order (Crenshaw, 1989; Hill Collins, 2017; Sales, 2018).
In this study, special attention is paid to the different models or paradigms of FD and how ableist interpretations influence the discourses and representations in the study participants’ life histories. These models provide us with alternative viewpoints on social understandings of FD. The individualist model, for example, represents a traditional and biologist view that focuses on the person and configures FD as a personal tragedy. This perspective ignores social factors and reinforces the traditional categories that disregard autonomy and focus intervention on medical rehabilitation. In opposition, one of the major contributions of the social model is to emphasize the role of the social milieu and to argue that FD is a particular social construction that does not take the needs or characteristics of people with FD into account. This line of work, originating in a sociological perspective, provides new conceptual frameworks (social and functional diversity) that make it possible to develop alternative representations that consider the influence of social values external to people with FD and the importance of dignity and diversity (Casado, 1991; Oliver, 1998; Palacios & Romañach, 2006; Puig de la Bellacasa, 1987; Toboso-Martín, 2018).
The concept of ableism, born in recent years in the field of Disability Studies and studied by English-speaking and Spanish authors, reflects on the intersection of ability and disability or dis-ability. Through its critique of individualist approaches (Sanmiquel-Molinero, 2020), ableism shows how those who do not fit the established norm of ability are discriminated against and identifies the mechanisms that cause an imbalance of power, as seen in access to resources and social and romantic relationships (Liddiard, 2017). From this perspective, we can question the idea that the medical and social approaches are fully in opposition. While the social approach considers disability to be a social construction, it does not interpret ability in the same way. Toboso-Martín (2018) points out that “we are ignoring the fact that our abilities are equally conditioned by the state of our bodies and by the characteristics and requirements of our social context” (p. 789, author's translation). In this respect, both approaches, the individualist and social perspectives, share the common objectives of ableing people with a disability or rather, dis-disabling them in order that they assimilate into society (Toboso-Martín, 2018). In other words, they share an ableist bias: while medical intervention is taken on the basis of their bodies, the social perspective focuses on the characteristics of the social settings.
For her part, the activist Park-Milbern (2019), self-identified as queer, uses Talia Lewis's definition of ableism, which goes beyond FD, and applies it to all oppressed social groups: [ableism is a] system that places values of people's bodies and minds based on societally constructed ideas of normalcy, intelligence and excellence. These constructed ideas of normalcy, intelligence and excellence are deeply rooted in anti-blackness, eugenics and capitalism. This form of systematic oppression leads people and society determining who is valuable and worthy based on people's appearances and/or their ability to satisfactory produce, excel and ‘behave.’ Importantly, you do not have to be disabled to experience ableism (p. 1).
As a central factor in the production of intersectional discrimination, I understand normalism to be a set of discourses and practices that discriminate against people with FD (Cozár Gutiérrez, 2011). These conceptual understandings provide us with a framework to understand negative representations of women with FD, particularly the influential category of “victim,” which underscores the traditional medical-rehabilitation model (Morris, 1991). In contrast, the category of “heroine” is associated with women who make enormous efforts, exceeding in the fields of sport, competition or professional or public activities. Their achievements make them “icons” of normality, but also obscure and invalidate the needs and day-to-day realities of discrimination experienced by people with FD and, therefore, in some ways reinforce ableism (Murphy, 1990).
Both categories, victim and heroine, present a naturalized objectified model which prevents us from questioning whether there are different ways to be a woman with FD. It becomes necessary to deconstruct the categories resulting from these hegemonic discourses in order to draw up others based on the ordinary experiences and identities of women with FD. The gaze of feminist anthropology provides us with an epistemological and methodological approach that permits us to analyze and critique these constructions, while identifying the more widespread discrimination and inequality caused by the axes of patriarchy and FD.
On the basis of this theoretical framework, the research set out to examine constructions of FD through the analysis of the life stories of six women with FD. The specific aim was to test these broad categories of victim and heroine and to analyze the processes of resistance and (re)negotiation used to subvert the norms constraining dissident bodies. In this respect, the research was particularly interested in the agentive capacity of the study participants. However, the aim was not to deny the influence of structural factors on inequality and discrimination of women with FD, but to examine how their representations and discourses challenge and respond to such factors and ultimately demand social change. As such, the study also seeks to make visible the constant struggle that these women face in their private and public lives as they attempt to defend their dignity and fight against discrimination. This study is particularly relevant to the field of social work because it contributes to efforts to move discourse beyond monolithic constructions and dominant social categories by exploring the multiple ways of being a woman with FD. Taking a rights-based and inclusive perspective, which supports independent living and full community involvement, it challenges social policy and service provision to see women with FD as autonomous subjects rather than objects of intervention. In this respect, it provides a basis for dignity and social justice through the development of individualized support and personal relationships.
Materials and Methods
Research Design
The research design is based on a qualitative interpretative paradigm and ethnographic methods, which involved interviews and participant observation. The development of the methodological design included establishing objectives, undertaking a literature review and making contact with organizations and women in the FD sector for the purpose of constructing a profile of the study population and potential sample. This article focuses on data from the interviews, which included two types of interaction with study participants: (a) three tape-recorded life-history interviews and (b) three interviews in the oral ethnographic tradition conducted during participant observation, which were not voice recorded but based on written field notes (Vansina, 1968). On the one hand, the life-history interviews, which were conducted in one session, allowed participants to construct a single narrative account of their lives and experiences. On the other, the oral ethnographic interviews were conducted over an extended period of time and based on various encounters and interactions. This approach permitted not just the gathering of narrative accounts of the participants’ lives but also allowed them to talk about the life issues and events that were important to them at particular times, such as work, family life and healthcare. Together, these two methods, contained within a broader project of participant observation, provided balance to the data, complementing each other and providing rich and personal accounts of the social experience and life histories (Pujadas, 2002) of women with FD. Although no direct data from other participant observations is reported in this article, it does provide important context to the study and informs the analysis and interpretation. This included interviews with experts, health professionals and support associations and charities; observations at meetings, social events, protest rallies, social service providers and medical-rehabilitation centers; and gathering of field materials and documentation, etc.
As a woman with FD, and with a background in social work and social anthropology, it is important to acknowledge that I came to this research from the privileged perspective of an insider, which was particularly beneficial in terms of recruitment and establishing trust with the study participants, as well as considering participant safety and the power dynamics that can influence qualitative fieldwork (Lucena Fernández, 2013). The study was not presented to an ethics board because, at the time the research was carried out, the University of Seville only required an ethics review for medical studies involving clinical trials and was therefore not possible to acquire. During the recruitment process, the participants were provided with transparent information on the nature of the study. It was made clear that their identities would be protected through anonymization and, in the case of the life-history interviews, written and signed informed consent to record the interviews prior to participating was acquired. Because the participants were all people with a physical FD, arrangements were made to interview them in spaces close to where they lived or that they frequently visited in order to avoid excess travel or accessibility problems.
Sampling and Recruitment
The study used a purposive sampling technique with two key criteria. Firstly, women with poliomyelitis, particularly those that were affected by the pandemic in the second half of the twentieth century in Spain, were prioritized because they are sub-group of FD that is typically underrepresented and experience significant socio-political invisibility. Secondly, the research centered on women whose biographical narratives revealed a history and continuity of resistance against assimilation by established social categories. These women were active in influencing social change, such as through involvement in FD support organizations, although not in any management capacity. They were of interest because their discourses often reproduced practices and terminologies implicated in transformations and ruptures with traditional paradigms. The research also prioritized older participants in order to observe historical changes in relation to the different stages of women's lives and also in Spanish society.
In total, six interviews were conducted. Firstly, three life-history interviews (recorded), of which one was recruited through an FD support organization, onethrough my work as a social worker and the other through a medical-rehabilitation center. Secondly, three ethnographic field interviews (based on field notes), of which one was recruited through an FD support organization and the other two during participant observation in the field.
As per the aims of the study, five of the study participants were aged over 50 and only one was under 40, at the time of the research. Four of the women's FD was a result of poliomyelitis, one woman had cerebral palsy and one had a congenital disease. All six participants identified as heterosexual women. See Table 1 for more details of the sample.
Fieldwork and Interviewing
The fieldwork for the study took place in intermittent periods between 2012 and 2018. As such, the three interviews conducted in the oral ethnographic tradition (not recorded, but based on field notes) were carried out during participant observation and involved various encounters with each study participant during this period (Manuela, Carolina and Esperanza). These interviews took place in public spaces, such as cafés, parks and other recreational spaces. The three life-history interviews (Rosa, Lola and Sira) were conducted between 2012 and 2013 1 and took place in locations chosen by the study participants, which included a café, a park and a participant's home.
The interviewing process for the three life-history interviews was unstructured. Following introductions and formalities, the study participants were asked to talk about the parts of their biography that they felt were most relevant to them. In this respect, the interviewer made very few interventions during the interview, except when the participants made explicit verbal or non-verbal requests for interaction. Complementary material related to each participant's life was also collected to provide context for the analysis. This included background information on the participants, such as their socio-economic context and where they grew up, details related to their housing (personal or institutional), employment and workplaces and involvement in non-profit organizations and activism.
Data Preparation and Analysis
Following the three life history interviews, the recordings were transcribed verbatim. The procedure for the qualitative analysis was based on Glaser and Straus's Grounded Theory (Glaser & Strauss, 1967) and was conducted with the Atlas.ti software program. This involved the fragmentation of the interview transcripts into quotations and coding them on the basis of the primary themes or life events that emerged in the interviews, as well as preparing analytic memos. The primary codes related to: age and time when the illness was contracted, medical treatments and institutionalization, schooling and other education, occupation and working life, symbolic representation of the FD, sexuality and reproduction and social participation.
Findings
The findings are structured in two parts. Firstly, the analysis considers how the study participants contextualize their own biographies and position in society, while the second part examines the specific socio-political content of their narratives.
On the Women and Their Backgrounds
All the study participants lived in the Andalusia region of southern Spain. The timeline of their accounts runs from the last half of the twentieth century to the present. All of the study participants’ families were working-class—their parents’ educations ranged from primary to secondary and their income levels varied on the basis of their occupations, which were mostly in waged employment, although one family had a small business. All the participants had some form of physical FD, either since birth or from an early age.
To start, the participants’ experiences and accounts of their different life trajectories highlight the fallacy of social constructs and the objectification of women with FD. Their experiences, accounts and knowledge revealed a group of women whose personal and social situations were multifaceted. They were committed to their personal and social development and routinely subverted the values attached to their bodies. In this sense, their narratives represented a break with the mold and the usual categories found in individualist and traditional models.
Rosa, for example, was born with cerebral palsy, which caused speech difficulties and greatly reduced her mobility. The profound limitations in expressing herself and in her mobility did not hinder her interest in an active life. She tried to study, work, love, and be loved; while she loved, she found being loved more difficult. Her story recounts how she has claimed her dissident body's right to pleasure. When her sisters and brother moved out of the family home she continued to live there until she was forced to move to a residence because of her parents’ advanced age, her functional limitations and lack of resources. Rosa explained: And then, well I realized I could not live with …, that is why I left home before my parents were no longer around, I have been in two residences, … now I have to go to another; in the end I have to change where I live, but I don't want to continue where I am because I don't have support.
Institutionalization deprived her of her vitality and happiness as she became immersed in feelings of sadness and isolation, telling me: “I have done everything I could … but I want to stress that everything I have done I have done myself, as I have had little help, from family or society.”
Lola's FD was caused by poliomyelitis, which she contracted as an infant. While still a young child, her family decided she would receive better rehabilitation if she moved to live in a socio-educational center that was over 200 km from the family home. She remembered well the first time they took her there: It was a Sunday and they checked me in, they came to check me in and my father said: “I’ll be right back, don't worry, I’ll be right back” and through the little window of the hospital I could see my father through the bars, he was wiping his tears and I was staying there. Now, you can imagine how I felt at six years old, now that I am a mother of two, can't you?
There she underwent numerous operations and continuous rehabilitation exercises to reform her dissident body: I had many operations and the rehabilitation work wasn't like when my mother did it. Of course, there were so many of us in the institution and so few staff, I don't know, I saw that as … my mother did not want San Juan de Dios [the name of the institution] under any circumstance, she did not, did not, did not … she saw she could, that she … that she would have done a better job with my rehabilitation but of course her life took a turn and mine … and mine with it.
Lola spent much of her childhood and adolescence in that institution. As a young person she maintained a connection to the center, where they offered her a job and she met her partner and future husband. They had two children together.
Sira's FD was also caused by the poliomyelitis she suffered when she was two years old, although her mobility was only partially affected. She received her early education in a socio-educational center and later moved to the same school as her siblings. She continued her studies in a secondary school and eventually graduated from university with a law degree. I really enjoyed that change because I have never felt comfortable in that … in San Juan de Dios, I don't know why, I don't … I liked playing with the children and San Juan de Dios was perhaps stricter than school … that's normal, I was very happy at my school, I was very … I had lots of friends, boys and girls. At Christmas they dressed me up as the Virgin Mary, I don't know, I sang, did my homework, I was just another … what I have always wanted to be.
She worked as a beautician until she studied for civil service exams and got a job as an administrative assistant in a public institution, where she has worked ever since. She has a son and daughter and has been married and separated twice.
Like Lola and Sira, Manuela also contracted poliomyelitis in childhood. She went to state school until she finished primary education and then married young—her husband does not have FD. Encouraged by her mother she took over the housework as well as being the main contributor to the family economy through her work as a lottery ticket seller. Later, she opened a small shop which created employment and income for the family.
Carolina's FD was caused by a congenital illness. She completed primary education, but not secondary. A variety of personal and family reasons prompted her decision to move to a residence, where she felt she would have greater opportunities for her personal and social development. At the time of the research, she continued to live in a residence, she was looking for a job, and a house adapted to her reduced mobility needs and she was trying to get personal assistance which would allow her to live independently. She had also decided to develop her romantic life. Finding herself in an abusive relationship with another resident, she felt the weight of social censure from other residents and those running the center when she received no support.
Finally, Esperanza, who also contracted poliomyelitis as a child, never attended school but received a basic education from a teacher at home. She had spent her whole life in the small coastal town where she was born and had never had a family of her own, although she took care of and provided some financial support to a large extended family. As an adult she was in a serious romantic relationship with a man in her town, however, if people asked him if he was her boyfriend, he would answer: “no, all I can feel for that woman is pity.”
These accounts of dissident bodies reveal a diversity of histories and ways of living and being a woman with FD which are far from the polarized social categories that constrain them. These accounts break the axis around which women with FD are structured as “victims”—child-like, infertile, sad, helpless, ugly, passive and bored—or “heroines” who are so “super” at everything that their individual needs associated with the different types of FD are denied. These discourses of diversity demand a (re)negotiation of the right to the everyday, to not be victims or heroines but just women with FD who want to write the script of their own lives.
On the Socio-Politics of FD
Based on the biographical portrayals, the second part of the analysis examines political factors and processes in the private sphere and the intersectionality of gender, FD, class and age. By examining accounts of sexuality, social mobility and violence the discourses and representations permit a deeper exploration of alternate ways of being women with FD and their capacity to challenge the oppressions that constrain them.
Sexuality
In the women's accounts of their lives, the social constructs of sex and FD are based on bodily differences that are redefined in terms of a pattern of hierarchized relationships between the sexes and ability/disability, which leads to relationships of inequality, as observed by other authors (Garland-Thomson, 1997; Morris, 1997).
Foucault's (1977) concept of biopower is a social mechanism that acts to suppress subjects’ bodies, such that, in the context of capitalist production, discourses and practices attempt to dominate and shape the sexual and dissident body in order to make it productive. However, we have seen that the oppression and subjugation experienced by the study participants did not impede them from generating strategies of resistance that question the social imaginary that defines them as asexual, infantilized, passive, sad and victims. The submission of dissident bodies and their resistance is present throughout the accounts. As Rosa states: In romantic terms, when … when I was younger my mother would tell me I could get pregnant and she warned me not to go near men, sort of to try to scare me as if something could happen to me.
These women's corporality is a highly important factor in their social interactions and participation. Bodies that do not reproduce the institutionalized model of beauty are invalidated and excluded from both the reproductive and productive systems. Sira spoke of the invalidating discourses she experienced in the town where she worked as a civil servant: ‘This girl is so pretty’. They said things I found funny, sometimes they would say: ‘you see her sitting there and she looks like a doll and if she didn't get up you wouldn't notice anything …’ ‘Well, and what's to notice?’ ‘No, woman, your little defect.’ And I just took it as fun.
Aesthetic evaluation, one of the main forms of social empowerment and validation in the construction of female social identity, is denied to them. Therefore, we do not find women like our study participants in fashion magazines, advertising or other fields where aesthetics is a primary factor. The non-existent social value of dissident bodies and their non-identification with beauty canons condemns women with FD to the silence and invisibility of illness, where they remain, hoping to attain the impossible ideal of a thin and healthy body. According to Sira: I was never … sexy enough, pretty enough, or anything enough, I always got … ‘you’re very fat’ … I have even been at a Christmas get-together with all his [her husband's] sisters, none of my sisters-in-law finished school, (…) they had trouble expressing themselves and it seems that I can express myself well, I am quite the extrovert (…) and when we left his parents’ house, I was told: ‘you’re definitely the fattest of all’.
From the perspective of Goffman's symbolic interactionism, the husband's gaze only sees Sira in negative terms and made no distinction regarding physical FD. He categorizes her as fat, not corresponding to the established model of thinness and therefore ignoring all her other attributes. The capacity for resistance and subversion is seen in the representation of the stigmatized protagonist, even if some time had to go by until Sira felt empowered: You can see I am overweight; I am aware of that. But I also have green eyes and I am charming and have nice hands. See, a person is an accumulation of everything, not just being overweight; and that made me very, very self-conscious …
Denied fertility and the ability to seduce and be the object of desire, women with dissident bodies redefine new beauty canons that are more plural than the singular institutional models. These are dissident models of beauty which take us back to the disorder of forms, asymmetry, plurality and the different ways of seeing beauty. Thus, women with FD have begun processes which allow them to deconstruct the standard and accepted beauty canon and to appropriate more heterogeneous models. This is how I interpret the gender-distribution of models in a recent exhibition on the effects of polio and post-polio from a medical perspective, which showed the effects of this illness on the bodies of 14 women and three men. The higher number of women may suggest increased empowerment of women and confidence in displaying the effects of polio on their bodies, leading to different aesthetic models. 2
We witness the critical and transformative capacity of agency which encourages us to move away from interpretations based on rigid social and cultural determinism and to move closer to interpretations based on dialectic relationships between hegemonic powers and the transformative capacity of agency (Pizza, 2005). As social actors, these women oppose processes of appropriation of their bodies and emerge as political subjects that rebel against the colonization of their corporeality by patriarchal power. In doing so, they become agents for transformation and rupture from the patriarchal culture, which in the case of Rosa, ties in with FD and when she became an adult: Later, I reached a point when I was at an age when I wanted to lose my virginity because I felt it was necessary to be a normal person. So, I found someone who wanted to sleep with me and that was it, I went to a hotel and slept with him, I had a more or less okay time, and I was no longer a virgin, which is what I wanted. He wanted to continue to see me but I didn't want him for anything else, but just because that happened and that's it, everything ended well.
Accounts such as this make demands for desire and pleasure explicit and confront the construction of sexless and childish women put forward by traditional models. The social and diversity models promote sexual diversity that is specific to the functional characteristics and sexual preferences of each individual. In keeping with this, the “Yes, we funk” movement, which asserts the right to sexual diversity in the political sphere, has been promoted as part of the Foro de Vida Independiente y Diversidad (The Forum for Independent Living and Diversity).
Medical practices overreach in their power over the bodies of women with FD, colonizing them through medical interventions which are reinforced by the clinical and social protocols of health, social and education professionals. Under the medical-rehabilitation model, dissident bodies cannot access the established aesthetic ideal and justify interventions through discourses that speak of improved health, quality of life and mobility. Interventions within this model are framed by aesthetic ideals, but from within a paradigm that maintains political and patriarchal control over the bodies of women with FD. Lola's account highlights the reparative action of medicine: “My mother did not want them to operate on me so much; she saw it wasn't good, that it would be good for education but not recovery.”
The traditional paradigms have inspired a practice which homogenizes or denies the corporeality of women with FD through, for instance, sexual practices, care during pregnancies and unauthorized sterilization in the case of women with intellectual FD. Unlike the medical-rehabilitative model, under the social and diversity paradigms, medical interventions also focus on the prevention of the illnesses which can affect an individual, along with the treatment of specific aspects of FD, if applicable.
Education, Work and Housing
As regards the educational history of the participants, their life stories show great diversity in educational backgrounds and attainment. These range from home-based education through a teacher/support association to attendance at socio-educational centers (special or non-inclusive education) and brief periods of regular attendance at state schools. The educational level of the study participants was heterogeneous, including women with no formal education, primary level, secondary level and higher-level education. Rosa recalls: I started doing things more or less on my own, like studying what I could … with an association that taught in the homes, I went to class and finished my compulsory school education. After this I started going to Instituto Bécquer, studying night classes, I did up to third year university entrance exams.
For her part, Sira says: I did the university entrance process for students over 25 and of course, as I had a good knowledge of French from the year I was in Paris, I got top marks, the rest was sort of average … I started studying in January and in May I passed the university entrance exam, (…) so that was it, I started studying first year Law, I was over the moon, over the moon, I could have called the Municipal Band to accompany me. I was the happiest woman in the world for the five years I was in university.
A comparison of data on the educational levels of men and women with FD shows a higher percentage of women with no studies and a higher percentage of men with at least a primary education. However, more women than men complete secondary school and third-level education (Instituto Nacional de Estadística, 2008). Although the accounts provide no specific information on access to educational resources or the possible difficulties or opportunities encountered by the study participants during their periods of education, the higher prevalence of basic levels of education and persistent material and psychological obstacles to accessing inclusive education highlight the disadvantages faced by persons with FD, specifically women.
Corresponding to the different levels of education and training we find different relationships to professional and occupational activity. The working lives of participants are also diverse, including unemployment, unemployed job seeker, employment in the public and private sector (selling coupons, administration, and telephony), as well as a small business owner. These occupational trajectories represent various survival strategies to generate income and employment for the participants and their families. These experiences both correspond with and diverge from the broader population. National data shows that while people with FD have lower levels of participation in the labor market in general, women with FD suffer significantly more inequality in access to employment than men with FD and when they are employed, they experience greater disadvantages (Instituto Nacional de Estadística, 2008). Social policies to promote increased participation of people with FD in the labor market have not been greatly successful, especially for women. In general, people with FD continue to be employed predominantly in public administration, protected employment, support organizations and self-employment, with significant exclusion from the private sector (Instituto Nacional de Estadística, 2017).
Lola's account of experiences in the labor market helps us to understand how the axes of patriarchal oppression and FD combine with the ableist imperative to hinder women with FD when they try to access the workforce: My father always said ‘well, you will have to be a seamstress because of the wheelchair …’ and I said that I would do anything except be a seamstress (…) but I told him that it was up to me to choose, that they shouldn't assume I was to be a seamstress because …. because I’m in this situation. Anything they said to me because I was in the wheelchair, because I was disabled, I didn't like. I wanted to be able to choose, like anyone else. So of course, when they said taxi cab company operator, considering how I like to chat and how good I am at it, it was a matter of learning to find the ideal job for me (…) At work we all had a disability, you know? Sometimes it also bothered me, because it was a job that gave me great satisfaction, showing my family I had a job which seemed ideal for me and that I was not going to be a lottery ticket vendor, I don't mean it to sound disparaging (…) or a seamstress, which is what was marked out for me, well, this was really satisfying, being able to take control of my life.
Institutional life is a deeply rooted social practice. Theoretical contributions warn of the social dehabilitation this can cause to residents (Goffman, 1961/2012). The United Nations Convention on the Rights of Persons with Disabilities (United Nations, 2006) and General Comment number 5 on living independently (United Nations, 2017) recognize the right of people with FD to choose the way of life they want to lead and recommends the mobilization of social resources to provide community facilities. However, this has not led to a reduction in institutionalization in Spain, which lacks the social policies that would ensure the personalization of services and measures to guarantee people with FD personal autonomy and the right to choose. This affects women especially as they are more likely to live in residential centers than men.
As mentioned earlier, Carolina chose to move to a residence because her expectations for greater personal and social development were not being met in her parent's home. However, when she wished to leave the residence and live in the community, she found herself trapped for various reasons, including financial resources, limited availability of personal living assistance and the shortage of accessible housing. Both Carolina and Rosa lived in a residence, but were not happy with the type of life it permitted and felt deprived of the right to make their own life decisions, in accordance with their rights (United Nations, 2006). Rosa described the limitations of life in the institution: Because your timetable is very limiting you cannot go to cultural events, you cannot go to things that clash with the set times for going to bed and waking up, for getting support … and things like that. I would be able to join associations, go to demonstrations, like when I was at home … Things like that, things I can't do now because I have to stick to a timetable in the residence where they are rather strict and not too accommodating. If, for instance, you arrive after midnight, you’re left in the street all night, and that is not right, things like that.
Many of these women have been overprotected in the home and family environment, which is underscored by traditional conceptualizations of appropriate social interactions. Frequently, this contributed to the reclusion of women with FD in the domestic setting or in institutions, as mentioned earlier. They have been denied the ability to start their own families, but have also been carers for all the members of their extended family, as we can see with Esperanza. In this regard, Angelino (2014), provides a new view of care relationships: “to review the idea that there are carers and people who only require care, but cannot give it. Disabled people are not only susceptible to finding themselves in a situation of reciprocal care” (p. 175, author's translation, in Pié Balaguer & García-Santesmases, 2015).
Feminist contributions question the informal and unpaid system of care maintained by women. They criticize the devastating effect of capitalist globalization and call for care to be the vertebral axis of social order (Carrasco et al., 2019; Pérez Orozco, 2006). A dignified care system must also provide a voice to those being cared for to prevent the care relationships from turning into hierarchical relationships of power. Not attending to the women with FD's demands for their rights to receive support impedes them from developing and controlling their lives (Keith & Morris, 1996). In this regard, the social model produces a strong critique of institutionalization and promotes the need for self-managed personal services (personal assistance) that make it possible for people with FD to live in the community. For its part, the FD model continues along this line of facilitating the support that is required for people with FD to live a dignified life and to manage their own affairs. Both models view personal assistance as a necessity for independent living and propose guidelines for the (re)negotiation of a new care system to dignify care work and the position that those being cared for must occupy as active subjects.
In the biographies, such as those of Rosa and Carolina, we can observe descriptions of life stories that have been placed on hold due to the limitations of living in institutions or family homes, the most common form of housing for people with FD. While Esperanza found herself in a liminal situation, Lola, Sira and Manuela had broken through the traditional barriers to independence and established social interactions and resources that had made it possible to start, organize and maintain their own families. In this respect, these three women's lives correlated with the plurality of possibilities that the social model and diversity model promote and which favor the rights of women to choose the type of life they wish to build.
Violence
The narratives also show how intersectional discrimination means that women with FD are often subject to different types of violence due to symbolic, structural and institutional action or inaction (Bourdieu, 1999). An example of institutional violence perpetrated through the practices of residential centers (Goffman, 2012) is evident in Lola's account of how her mother was not allowed to stay with her after surgical operations even though she was only a young child. In Rosa's case, it was being left in the street all night, or the threat thereof, if she did not manage to return to the residence before curfew. The institutional violence that occurs in hospitals and residential centers mostly remains hidden because of internment, lack of reporting mechanisms and absence of support for those who experience it. We can also consider that Rosa and Carolina experienced institutional violence due to constraints imposed by the model that does not provide sufficient social support to permit them to live full dignified lives in the community. Carolina experienced physical violence from a fellow resident, which led to rejection by her peers and those running the center. The multiple forms of violence in the narratives shows how its prevalence against women with FD is more frequent and broader in scope and that there are fewer resources to tackle it. This can be put in a wider perspective by considering that the results from a survey by the Spanish government on violence against women found that 40.4% of women with a disability have suffered some type of violence from their partner, compared to 31.9% of women without a disability (Ministerio de Igualdad, 2019). In this respect, violence is often perpetrated by those that are also providing care (partners, relatives or carers). There was symbolic violence on the part of Esperanza's lover when, in public, he made emphatic denials that her body could be an object of desire, able to produce and receive pleasure, and in the way that Sira's husband insults her appearance and casts doubt on her desirability. And, there is persistent verbal abuse through derogatory comments, such as that recalled by Rosa: “One day I went to buy the bread for my mother and I said: ‘the bread is that much?’ and the guy in the bakery said: ‘ooh, how funny, she knows how to count’.”
Outside the domestic and institutional sphere, violence manifests itself in subtle ways, due to the naturalization produced by the ascription of violence to cultural norms. Thus, the invisibilization or absence of people with FD in certain work or social environments is not perceived as a type of institutional violence.
Conclusions and Discussion
By constructing these accounts of life and functional diversity through the analysis of the study participant's discourses, the study seeks to provide an alternative to research that focuses on external discourses that construct subjects without taking into account lived experiences and subjectivities. Within their constructions, the women with FD in this study recount being subjected to interventions but not having rights, how they were limited to domestic or institutional settings and condemned to low levels of education and income, which was often from social benefits or sometimes precarious employment. These women become the “Cinderellas of the house,” not considered capable of starting their own families but perfectly able to look after other members of the family. They provide more care than they receive and their sexual and romantic relationships are hidden or denied, as is their right to motherhood. However, throughout the analysis I have paid special attention to the agential capacity of the participants while situating it firmly within the socio-political context of their life stories. It is clear that these women's discourses and practices can be framed and understood within the ideas of pioneering feminist activist-theorists (Garland-Thomson, 1997; Iglesias, 1998; Morris, 1997), participatory movements that led to key political initiatives, such as the IV Beijing Conference 1995 and the CRPD 2006, the concepts of the Independent Living Movement, along with local activism and legislative initiatives in Spain, which started in the late 1990s and early 2000s (Viñuela, 2009). More recent influences include contributions from post-structuralist feminism and new technologies (López-Rodrigán, 2019), not dealt with in this paper due to lack of space. All of these have contributed to a redefinition of FD from a strictly individual issue to a social concern (Turner, 1994), providing the socio-political context for agency and resistance to traditional models. The ability of the study participants to put strategies in place to achieve their desires and ambitions leads us to reflect on the fact that “people with functional diversity are not unhappy because of their diversity, but because of the social obstacles they encounter that prevent them from being so” (Palacios and Romañach, 2006, p. 7).
Thus, on the one hand, the strength of patriarchal and capitalist oppression, the enduring force of traditional paradigms and ableist requirements still immerse the women with FD in this study in intersectional discrimination that is manifested in the different aspects of their biographies and life histories. Their stories reveal the ravages of institutionalization, violence and denial of identity and the strategies they put in place to deal with this, manage their lives and make them meaningful at the periphery of the social order. On the other, while this helps us to understand the depth of the inequality and marginalization that they have experienced, it also frames their agential actions in bringing about transformations in their own lives and that of their social milieu (developing access to resources and claiming ownership of their bodies and their sexuality). So, although the participants are not strongly active in a political sense, the permeation of the sociopolitical frame (in traditional and social and FD models) is expressed in dual influences of constraint and agency. The possibilities afforded by autonomy are well expressed by Lola when she says: “I believe that looking back on my life now, at 53 years old, I believe that I have made good use of the talents that I was given.” As such, these women's representations steer us away from the persistent objectified image of women with FD which only encapsulates representations and practices of exclusion and intervention.
As a social worker and woman with FD, I believe that change is necessary in both social policy and service provision if the rights of women—and other people—with FD (United Nations, 2006) are to be respected and met. This study is highly relevant to both feminist disability studies and social work because it contributes to a more complex understanding of the social reality of women with FD. By breaking with the objectified and dichotomous images of women with FD, it asks social workers to recognize the plurality of life trajectories and these women's capacity for agency and autonomy. Too often, social policy and social work have viewed women with FD as vulnerable and one dimensional; the objects of intervention rather than fully agentive social actors. In adopting the rights-based approach that the social and diversity models promote, social work can contribute to the transformation of exclusion by shifting the focus from medical-rehabilitation and institutionalization to the provision of resources and support that permit independent living and full integration into the community. This starts with human relationships, listening to and getting to know the people that we serve. In recognizing diversity and autonomy, we are better placed to provide the support and resources women with FD really want.
Characteristics of the Study Participants and Data Collection Technique.
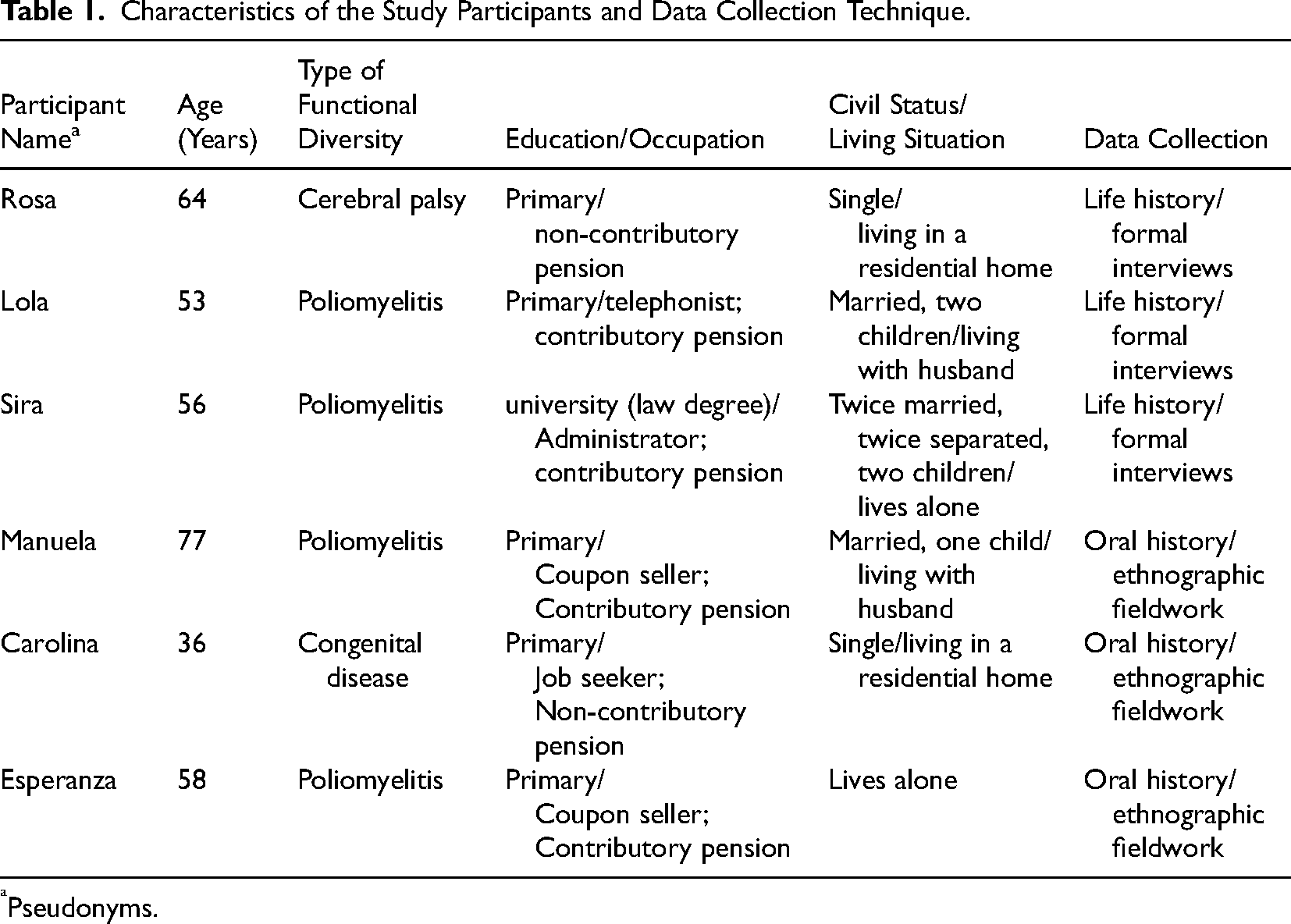
Pseudonyms.
Footnotes
Acknowledgments
I am very grateful to the study participants and Dr. Carmen Mozo González (Professor of Social Anthropology, University of Seville).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.