
Abstract
Although it is well established that women experience significant gendered oppressions when accessing mental health services, research exploring the impacts of involuntary mental health services is frequently conducted without attending specifically to gender. This article reports on a qualitative study that explored women's experiences of compulsory mental health treatment in Australia. In-depth interviews revealed substantial gendered harms experienced by women within involuntary mental health treatment settings. Themes identified were: involuntary treatment replicates the dynamics and tactics of gendered violence; treatment involves profound deprivation and losses, with potential implications across the lifecourse; mental health services disrupt and undermine mothering; and recovery is found outside of coercive mental health systems. The study reveals the heightened harms experienced by women within involuntary mental health contexts, as well as women's strategic resistances to psychiatric oppression. It demonstrates the relevance of a conceptual lens that is attuned to gender, in order to develop a deeper understanding of women's experiences of intersecting oppressions within involuntary mental health settings. Implications include the need for alliance-building across feminist and critical mental health movements, and the need for a much more robust engagement by the social work profession in challenging the widespread acceptance of involuntary mental health treatment.
Keywords
We are living in an age where the most dominant paradigm for understanding mental distress is offered by a reductionist biomedical model, which situates distress as a dysfunction within individuals, caused by biological processes in the brain (Read & Harper, 2020). Despite its prominence, the biomedical paradigm has been critiqued for concealing the links between adversity and distress, for overstating the role of biological processes in experiences of distress, and for constructing artificial boundaries between psychological “normality” and “abnormality” (Allsopp et al., 2019). Biomedical and diagnostic understandings also lead to very narrow interventions – primarily medication, and therapy focused upon individual behavioural changes – thus foreclosing opportunities to address the social drivers of emotional suffering (Morley & Stenhouse, 2021). In this paper, we follow other critical mental health theorists who use the term “distress” rather than “mental illness,” as a way of questioning a narrow and oppressive framing of emotional suffering as merely a biological process.
There are many theorists who have provided robust critiques of biomedical understandings of distress using an intersectional feminist lens. The deleterious effects of biomedical understandings of distress are often heightened for women, due to the gendered framing of women's distress within psychiatric settings (Fullagar et al., 2019). Gender biases are evident in psychiatric categories that are overwhelmingly assigned to women, such as borderline personality disorder, a diagnosis that leads to highly discriminatory responses by mental health professionals (Ussher, 2011). Further, the dominance of a diagnostic approach within mainstream mental health services has been critiqued for allowing a range of gendered stressors and inequalities, including gendered violence, to continue unchecked (Moulding, 2015). There is substantial evidence that women frequently experience mental health interventions as harmful, disempowering, and dehumanising, even if some benefits are also reported (Tseris, 2017; Fullagar et al., 2019; Ussher, 2011). However, there has been limited gender differentiated research into involuntary mental health treatment, leading to gaps in knowledge relating to the gendered dimensions of women's experiences within involuntary mental health settings (Ross, 2018).
This article reports on the findings from a qualitative study conducted in New South Wales (NSW), Australia, which explored women's first-person accounts of involuntary mental health treatment. Through centring women's voices, the study aimed to counter the unjust suppression and dismissal of the knowledges of people who have received a psychiatric diagnosis, due to sanist assumptions that position people deemed to be “mentally ill” as less legitimate knowers (LeBlanc & Kinsella, 2016). We draw upon critical mental health theory, which utilises “critical thinking on the practices, priorities and knowledge base on which psychiatric and related professionals lay claims to expertise” (Cohen, 2017, p. 1), which includes but is not limited to the contributions of Mad Studies and anti-psychiatry theories. We use the term “survivors” to describe women with experiences of involuntary mental health treatment. In our view, terms including mental health “consumers” and “service users” do not fully convey a politicised analysis of how mental health services are shaped by oppressive power relations and structural inequalities (Rose, 2021), although we recognise that some people who access mental health services find these terms helpful.
Literature Review
In involuntary mental health contexts, the power differentials between mental health professionals and people diagnosed with psychiatric disorders are substantial. Distinct from every other healthcare context, involuntary mental health treatment is characterised by forced treatment, detention in locked wards, seclusion and restraint (McKeown et al., 2019). Such coercive interventions are underpinned by mental health legislation, for example, the Mental Health Act in NSW, Australia, which states that a person may be detained involuntarily in a mental health facility if an authorised medical officer is of the opinion that “(a) the person is a mentally ill person or a mentally disordered person, and (b) no other care of a less restrictive kind, that is consistent with safe and effective care, is appropriate and reasonably available to the person” (NSW Government, 2021). In Australia during 2018–19, over half of patient days in acute mental health units were for people with an involuntary legal status, specifically, 51.9% of acute patient days for females and 60.6% of acute patient days for males (AIHW, 2022). Although this article focuses on involuntary mental health treatment within acute hospital settings, it should be noted that involuntary treatment extends far beyond this context, for example, treatment occurring in non-acute units and community treatment orders, which mandate medication in the community. It is also important to acknowledge that people may experience significant coercion within mental health settings, and pressure to comply with the views of mental health professionals, even if they are not being treated under the Mental Health Act. As social workers are employed within both inpatient and community mental health settings, and routinely refer people experiencing distress to mental health services, the social work profession both participates in, and witnesses the effects of, involuntary treatment.
Research on the Impacts of Involuntary Treatment
Involuntary mental health treatment is commonly perceived through a narrative of “violence as benevolence” (Lee-Evoy, 2019, p. 286), whereby actions that would in other contexts be understood as violent and unacceptable are justified because they are perceived to provide necessary forms of “care” and “treatment” to people experiencing mental distress (Mental Health Act, 2007). In addition, assumptions about the “presumed prudence” of mental health professionals in enacting coercive practices only as a last resort, combined with strongly held views about the connections between mental distress and dangerousness, reinforce rigid ideas that there are “no alternatives” to treatment without consent as a response to people deemed to be experiencing “severe mental illness” (van Daalen-Smith et al., 2014).
Despite a widespread acceptance of the perceived need for involuntary treatment, research into the experiences of compulsory mental health treatment has challenged the assumption that such responses are always enacted in the best interests of people experiencing distress, or the community more broadly. The extant literature demonstrates the dominance of a medical-custodial approach within hospital settings, which frequently exacerbates rather than alleviates distress, for example, through the trauma and humiliation of having belongings confiscated and being strip-searched (Prytherch et al., 2021). Whitaker et al. (2021) note that it is common for people with psychiatric diagnoses to be subjected to an ongoing cycle of involuntary admissions, which can be spirit-breaking. A recent report released by the World Health Organization (2021) cites similar concerns that people subjected to coercive practices “report feelings of dehumanization, disempowerment, being disrespected and disengaged from decisions on issues affecting them … leading people to avoid seeking care and support.” Ross (2018) questions the legal sanctioning of treatment without consent, given that people with psychiatric diagnoses are no more dangerous than the general population, and that interventions such as seclusion involve extreme deprivations of liberty that cause harm for the majority of people and lead to re-traumatisation for people who have previously experienced violence. In fact, psychiatric coercion appears to increase the risk of suicide attempts, disrupting the idea that involuntary treatment is justifiable on the basis that it reduces the risks posed by mental distress (Jordan & McNiel, 2019).
Social Work Perspectives on Involuntary Treatment
Concerningly, social work has largely demonstrated implicit support for involuntary treatment, by seeking to improve social work practice within involuntary settings rather than to outright challenge or contest it (Maylea, 2017). At the same time, a growing social work critique of biological and diagnostic understandings of mental distress, alongside social work scholarship demonstrating the incompatibility of involuntary treatment with recovery or mental wellbeing, means that social work is well-positioned to engage in more radical and robust critiques of involuntary treatment, as well as contributing to alternatives (Whitaker et al., 2021). Although involuntary treatment is often justified on the basis that the alternative would be to neglect people experiencing significant distress (Maylea, 2017), ceasing a reliance on force and coercion opens up an array of opportunities for providing support and new responses to distress that are focused upon social justice, agency, human rights, recovery and meaning-making, as a replacement for medicalised understandings of distress based on notions of individual pathology and narrow risk discourses (Watson et al., 2014). Such alternatives include investing in resources and supports to address the social determinants of distress, including violence, homelessness, poverty, discrimination and isolation, thus reducing the likelihood that mental distress will arise in the first place (Karban, 2017). Peer support approaches, which are led by people who have themselves been labelled with a psychiatric disorder, offer further opportunities for alternative understandings and responses and a collective reclaiming of the experiences and rights of people experiencing mental distress, beyond the constraints of mental health discourses or services (Probert, 2021).
The Relevance of a Gender Lens in Understanding Involuntary Treatment
Involuntary mental health treatment has been shown to have adverse effects for people of all genders (Watson et al., 2014). Nevertheless, emerging research indicates the importance of understanding the gendered dimensions of harm experienced by women. For example, it is now well recognised that separating mothers and infants in the context of perinatal distress has detrimental impacts, which has led to increased investment in currently under-funded mother and baby inpatient units (Stephenson et al., 2018). Mothers understandably fear custody loss and child protection involvement, which is often instigated during a psychiatric admission (Wright et al., 2018). Other research into the gendered dimensions of involuntary treatment has found that although men are secluded more than women, among repeatedly secluded patients, women are in the majority (Knutzen, 2007). Further, women who have experienced coercive psychiatric practices are more critical of coercive practices than men (Soininen et al., 2013), indicating that women experience these practices differently. Importantly, the trauma of compulsory mental health service provision is often compounded by women's previous exposure to sexual violence (Soros, 2021), which is particularly pertinent given the higher rates of sexual violence experienced by women with a psychiatric diagnosis in comparison to non-psychiatrised women. Women who have experienced gendered violence have described psychiatric coercion, including detention, and forced treatment, as re-traumatising due to their powerlessness and humiliation within such contexts, thus highlighting the relevance of a gender lens in understanding the impacts of involuntary treatment (Prytherch et al., 2021). Alarmingly, women detained within psychiatric units are also at high risk of experiencing sexual violence within these settings by male patients, male staff or partners/ex-partners (McGarry, 2019). To address these risks, women have described the need for changes to the built environment, gender segregation, staffing changes and survivor-led advocacy (Watson et al., 2020).
It is striking that women's exposure to such significant safety concerns in involuntary treatment settings occurs in the context of decades of attempted reforms in mental health, notably, recovery-oriented and trauma-informed policies. However, such policies have been constrained by a lack of a gendered approach (Women's Health Victoria, 2019). Overall, there has been scant research and attention on the gendered dimensions of women's experiences and needs during involuntary treatment (Archer et al., 2016). In this present study, interviews were conducted with women with first-hand experiences of involuntary mental health treatment. The research questions that guided the study were: How do women survivors describe their experiences of, and responses to, involuntary mental health treatment? How did mental health services respond to women's experiences of distress, and how does this compare to women's own understandings and suggested responses?
Methodology
Semi-structured, in-depth interviews were facilitated with 21 self-identified women over 18 years of age, with an experience of involuntary mental health treatment in Australia. The interviews were situated in the context of a larger research project, exploring the perceptions and experiences of involuntary treatment from multiple perspectives (survivors, family and friends and mental health workers). In addition, women were invited to contribute creative pieces and five participants chose to contribute art, poetry, and written reflections. These contributions will be reported on in a future publication, combined with further creative responses that will be produced in the next action research phase of the project.
The study was underpinned by the conceptual frameworks of intersectional feminism and critical mental health theories. It aimed to consider a range of power relations that intersect with both psychiatric oppression and gender inequality, and to draw upon a diverse range of women's experiences and perspectives (Quiros & Berger, 2015). Through centring the voices of women survivors of involuntary treatment, attending to power relations and making space for alternative understandings beyond the constraints of the biomedical paradigm, the project was “devoted to the critique and transcendence of psy-centred ways of thinking, behaving, relating, and being” (LeFrançois et al., 2013). Our research team included a researcher without direct experience of involuntary treatment (ET) and two survivor researchers (EBH and SF) brought experiential knowledge to the study, stemming from their direct experiences of involuntary mental health treatment, in addition to their research expertise. Consequently, survivor knowledges were embedded in both the project's interviewing approach and analytical processes, as outlined below.
Ethical Considerations and Recruitment
Ethics approval was obtained for the study via the University Human Ethics Committee. Supported decision-making principles informed a pre-interview discussion, which included opportunities to fully discuss the aims and processes of the interviews and to answer any questions (Gooding, 2013). This approach replaced a pre-research screening process that was initially recommended by the ethics committee, which the research team deemed paternalistic, and imbued with sanist assumptions about the reduced decision-making capacities of people who have been labelled with psychiatric diagnoses. All participants provided written consent. The interviews were recorded, and the audio files were transcribed.
Participants were recruited through a range of avenues, including online newsletters, community centres, “word of mouth,” and snowball recruitment. Participants were given a $75 gift voucher to acknowledge their time and participation in the project.
Interviews
The majority of interviews (18) were co-facilitated by the first author and a survivor researcher (second or third author). The role of the survivor researchers in co-facilitating the majority of interviews was valuable in building trust and safety, and in framing rich and relevant interview questions and responses to participants that drew upon their experiential expertise (Faulkner, 2017). Interviews were guided by an interview schedule; however, a broad scope was given to participants to explore issues of importance to them. Interview questions included: Could you describe (only in as much detail as you would like to share) your experiences of involuntary mental health services? What are your understandings of the experiences of involuntary mental health services for women in particular? Due to a lockdown as a result of Covid-19, the majority of interviews were conducted online.
In line with both feminist and critical mental health frameworks, the interviews aimed to allow participants to tell their stories in their own words, and to be guided by participants’ worldviews on their experiences (Ackerly & True, 2020), thus offering an alternative approach to the hierarchical power relations involved in psychiatric assessment processes. Interview questions did not use diagnostic language; however, some participants used diagnostic categories to describe their experiences, and the language that participants drew upon was respected. In addition to the harms of psychiatric and gendered oppressions, a focus of the interviews was exploring participants’ resistances to injustices, in order to identify the complex strategies used by women to resist and negotiate oppression (Lafrance, 2007).
Participants were offered the chance to debrief with the researchers following the interviews. Rather than imposing generalised “self-care” strategies onto participants, this process was participant-led, and most participants described existing supports and strategies that they would draw upon following the interviews. Despite the often-harrowing experiences that were shared in the interviews, nearly all participants described the interview as a positive experience that offered them the chance to contribute their perspectives in a safe and de-identified way and to receive affirming and validating responses from the researchers, which offered a strong contrast to their previous experiences of psychiatric assessment interviews. Most participants were enthusiastic about participating in the next planned action research phase of the project, describing the benefits that would be gained from connecting with other survivors and contributing to further research and social change.
Analysis
Data analysis was an ongoing and iterative process, often commencing within interviews, where researchers reflected on key concepts within survivors’ stories and checked their emerging understandings with participants. Researchers took notes during and after the interviews, engaged in journaling processes, and discussed reflections together in order to build a collaborative analysis. The transcripts were coded and analysed, using reflexive thematic analysis strategies (Braun et al., 2022) and tentative themes were discussed among the team as the analytical process progressed. Potential themes were assessed according to the extent to which they reflected salient concepts that were present across multiple interviews, which multiple team members had identified as significant. Potential themes were discarded if they were too wide-ranging, too similar to other themes, or if they did not closely address the research questions (Braun & Clarke, 2012).
In our analytical processes, we recognised that approaching the transcripts with some pre-formed social categories is both inevitable and valuable (Rose, 2021). In line with an intersectional feminist lens, the analysis aimed not only to centre an analysis of power and gender, but also to explore intersecting contexts and social forces, including race, age, rurality, income and housing (Ackerly & True, 2020). In addition, we emphasised the need to identify and value participants’ survivorship and resistance to psychiatric oppression. Further, rather than uncritically privileging objectivity and distance, we took the position that our personal reactions were valuable within the analysis (Faulkner, 2017). Critical reflexivity, assisted by memos and journalling, was therefore vital in recognising how our own experiences and perspectives were informing the analytical approach (Ackerly & True, 2020), while also ensuring that we were making space for diverse understandings among both the research team and the participants.
Findings
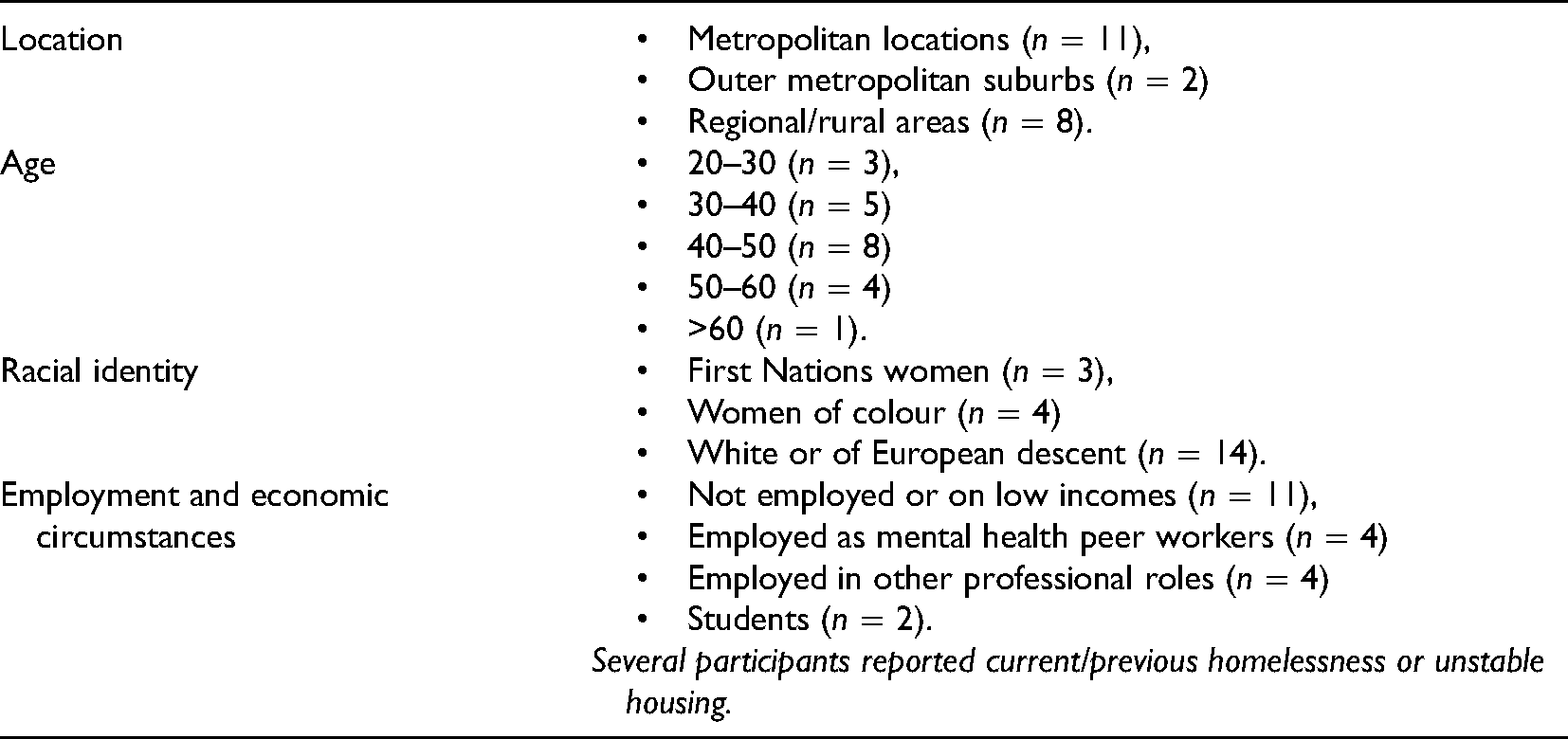
Twenty-one participants took part in an interview (see Table 1 for demographic information). Participants described diverse experiences at the time of receiving involuntary treatment, including suicidal thoughts and behaviours, significant distress, grief, hearing voices and/or experiencing unusual beliefs, altered states, exhaustion and depletion. Most participants had experienced at least one involuntary hospital admission, although three described involuntary transport to hospital by police and treatment occurring in the emergency department only. Many participants described multiple involuntary admissions, and the majority of participants described ongoing mental health system involvement. However, several participants described active strategies that they were now engaged in to attempt to reduce the level of mental health system involvement in their lives.
Participant Demographic Information.
All participants described involuntary mental health treatment as a profoundly negative and traumatic experience. The interviews revealed the multiple and ongoing implications of involuntary treatment: Involuntary treatment has greatly shaped the course of my narrative, of myself, of my life…. There’s all these relationships that have changed because of involuntary treatment…. I had to drop out of university at times because of involuntary treatment, which meant that I didn’t go down certain career paths. So the reason I’m doing this study is because … [it] could lead to some recommendations where we reduce coercive treatment such that it means that people have more choice over their life.
Participants discussed the ways in which their experiences of gendered oppression and violence were amplified rather than alleviated by mental health system involvement: I first came into contact with the mental health system in 1996. And yes, looking back, I think my life would be very different if I hadn’t come into contact with it. And I do say now that most of the issues I live with now are due to trauma within the system, rather than the stuff that brought me into contact with the system in the first place … I’ve experienced seclusion, I’ve experienced mechanical restraint, and yes, it’s just caused a lot of issues … yes, massive harm.
Many participants took part in the research in order to contribute towards change and as a way to “speak back” to a mental health system that has caused harm to women and not been held accountable: The reason I wanted to participate in this interview is because I want to effect change for women, particularly women who’ve experienced trauma and have intersected with the mental health system…. That makes me feel angry, that I’ve gone somewhere to get help and I continue to be oppressed and not heard.
Four major themes were identified in the analytical process: treatment replicates the dynamics and tactics of gendered violence; treatment involves deprivation and multiple losses; treatment disrupts and undermines mothering; and recovery is found outside of the coercive mental health system.
Treatment Replicates the Dynamics and Tactics of Gendered Violence
Several women described experiences of gendered violence as key drivers of their mental distress, which were rarely considered important by mental health professionals: [Gendered violence] was the whole reason why I became unwell. I know that that had everything to do with it…. If you were getting treated like that, of course things are going to happen…. I said once [while hearing a voice], “Who is it?” and [the voice] said, “Well, it’s B here,” that was [an abusive partner’s] name.
Even when mental health workers attempted to ask about gendered violence, the screening occurred in ways that caused further harm, because it did not lead to a different response outside of the narrow medical paradigm: It was actually re-traumatising for me to disclose because I was aware that it was just a probing, it was just adding to my case note history.
Interviewer: Did you have a sense that it shaped any of what they did?
I don't ever think the trauma was responded to, ever by the psychiatric system.
Several participants described feeling scared and unsafe on the ward, due to the presence of intimidating male patients, and experiences of sexual harassment and assaults that were not taken seriously by staff: He watched me on the bike each morning…. I just felt really uncomfortable … the nurses said, “oh, yeah, he makes us feel uncomfortable too, but we don’t have any history of any sexual assaults or anything like that, so don’t worry”…. He was just extremely creepy. Extremely creepy. And I think when he came into the room when I was on my own, I just felt - I felt quite threatened…. There was another guy who was kind of following me around a lot, and commenting on my looks … I just felt really uncomfortable being on the mixed ward.
The lack of safe spaces for women was a particularly significant issue for women with previous experiences of gendered violence: In all three admissions, men tried to come into my room … when I was 19, a man known to me raped me, and I think that’s one of the triggers that led to me being in psychosis. And I was very clear, right from the first admission, that I did not want to be around men, I didn’t feel safe … there should be gender-streamed areas, there should be better staff supervision … you take women … who usually have a history of trauma, and you put them in a re-traumatising, actively harmful, unsafe environment and call it treatment.
In addition to male patients, survivors also described being terrified by some male staff, especially security guards, who used excessive force, in ways that directly paralleled the power relations and violence of sexual assault: As a person that has experienced sexual abuse…. A petite, 19-year old girl, being held down by three large, male, security guards whilst my clothes were removed so they could inject a sedative into my rump…. I was of the belief that I was being taken into a room to be raped. The situation had scarily escalated, I cannot really recall how it ended up being so violent … the trauma from that incident is something I have had to work with ever since.
Survivors discussed their incredulity about the power imbalances involved in forced treatment and one participant described how such experiences led to a political awakening: Being put in seclusion radicalised me. It didn’t calm me, it radicalised me.… Three or four males trying to overpower a woman. I mean, it’s ridiculous.
Mental health services responded in harsh and cruel ways to women’s emotional expression and despair, utilising seclusion as a response to tears, and refusing to provide attention or compassion around intense suffering: A lot of shaming around my level of distress … what I needed at that point was for someone to sit beside me while I cried and cried and cried, but instead I got locked alone in a room to cry and cry and cry. And so, yes, a lot of that attitude of that I was too dependant and too needy and so they shouldn’t give me attention because that was just encouraging it.
Survivors described the relentless pathologisation of women’s lives by psychiatry, including gendered assessments of sexuality and assertiveness, as described by a young woman: A lot of my admissions, like the “manic” related ones were related to their perception of me as being overly confident and also hypersexual … they made all these comments about my skirt being too short…. And I was just thinking, why are you looking - why is that so important? … I didn’t think I was being overly sexual, whatever that means. I’m not sure what that means … there are times that people do feel more sexually aroused or whatever than other times.
Participants described responding strategically to psychiatric practices, for example, changing their behaviours in order to protect themselves from further gendered diagnoses: I knew I was skating a fine line between asserting myself and then ending up with a personality [disorder] as well. So I was kind of constantly monitoring the whole time, “How’s this going to be perceived?” Yeah, everything’s pathologised in there.
Survivors described the betrayal of a mental health system that did not acknowledge or take responsibility for the harms that it inflicted on women: There hasn’t been a proper look at women’s experiences of involuntary treatment…. Of course it doesn’t hold a mirror up to itself and actually reflect and look at the coercive practices that happen.
Many participants described the humiliation and fear in having their rights taken away, leading to an exacerbation of their distress. For First Nations women, the involvement of police as first responders and in transport to hospital was particularly harmful: I’ve always been involuntary admitted to a psychiatric hospital and always in the back of a paddy wagon in handcuffs … all those experiences have been so traumatising and that. And just sitting there and having so many police surround you … it’s horrific, that level of not treating you as a human being, because I’m not a white girl.
Poverty was another intersecting social location that precluded some survivors from being able to access private health insurance in order to avoid further involuntary mental health admissions. Several participants described undertaking significant financial sacrifices to safeguard themselves against further harm related to psychiatric coercion: Three burly people came and picked me up and put me in a secluded room, and then IV’d me…. So those experiences have really - oh my God, they’re just such significant experiences in my life, in terms of how terrible the mental health system can be for people…. The last thing I’ll ever do is to go in a public hospital. I’m on a pension, and I pay … for health insurance so I can go to a private hospital … in a public hospital you’re not, in many ways, you’re not regarded as a person.
Treatment Involves Deprivation and Multiple Losses
Survivors described that involuntary mental health treatment involved multiple layers of deprivations and losses, which sometimes had ripple effects over many years. Firstly, treatment involved replacing women's stories with a diminished psychiatric identity, which invited discrimination and punitive responses: I was experiencing massive overwhelming grief. And that’s what I needed support with. But it was very much pathologised … I got labelled with borderline personality disorder, and it was pretty much all downhill from there…. I have very big issues with the term manipulative. Like I’ve been told I’m manipulative about a thousand trillion times, and yes I refer to it as desperate help seeking behaviour.
The adverse effects of an over-reliance on medication, in the absence of alternative supports or choices, had particularly gendered impacts for women. For example, women described how fatigue impacted upon their caring responsibilities. The significant weight gain caused by psychotropic medications led to difficulties within heterosexual partnerships and unwelcome surveillance of their bodies against patriarchal standards: I had four men, all in the professional workplaces I was in asking if I was pregnant. And you know, they’re not really asking you if you’re pregnant. They’re just putting you in your place. They’re just saying you’re fat.
Alongside coercion, survivors were dismayed that involuntary treatment provided very few if any resources to address the main drivers of their distress, which nearly all participants described as social rather than biological. A lack of attention to social and economic contexts, in favour of a medication-focused response, meant that upon discharge women often returned to adverse circumstances, including violence and housing precarity, with no additional supports. In this way, participants described the ways in which forced treatment coincided with neglect: I’ve actually had a [psychiatrist] say to me, “We don’t know what you want us to do. We don’t know what you want from us. We don’t know why you keep doing this [expressing suicidality]. There’s nothing we can do, you’re discharged,” kind of thing. That’s actually been said to me. And with no particular discharge plan at all, just goodbye. And that’s after I tried to kill myself the night before.
Participants described a sense of hopelessness and despair that stemmed from being in a dehumanising, carceral environment where little was offered other than medication: Hospital makes you sometimes more unwell, I think…. There’s also a feeling that it’s a prison. It is to be honest. It is, you’re locked in there. And there’s very little I feel that they do to help you recover, apart from just giving you medication which they could give you in the community. There’s just a sense that you’re being contained.
As a response to the neglect and deprivation, some women sought connections with each other in order to access supports and opportunities to make meaning of their experiences: The one thing about being in hospital, there was zero counselling. So I didn’t talk about anything like that. I saw some of the consumers or patients would make quite tight friendships with each other and you’d see them counselling each other.
In addition to failing to address the social determinants of distress, participants described the ongoing impacts of diagnosis and treatment, which remained long after discharge, for example, a diminished sense of self and a significant loss of confidence: It was disgusting. I don’t know how to put it in words. They didn’t harm me physically, but they were very harmful emotionally, spiritually and mentally…. I wasn’t valued in any way, shape or form. My opinion, my person, what I was going through … I didn’t feel valid as a human being … my voice was taken away.
Many participants described how involuntary treatment disrupted their hopes and dreams for the future, with psychiatric treatment having multiple long-term effects across the lifecourse: I wanted to get married and have children. I’m 40 now. I’m getting a divorce. I have no children … I had an entry level job in 2015 which they pushed me out of because I was very affected by the Olanzapine and Mirtazapine. It was very obvious…. I fell asleep one day…. I have had to rebuild my life again since [the admission]. And I feel like it has put me back years and years and years.
Survivors described further losses post-discharge, including discrimination following a new, stigmatised identity as a “mentally ill” woman. A participant described the detailed strategies she had adopted to guard herself against the ongoing deleterious impacts of diagnosis: So I found when I disclosed this diagnosis of “bipolar” to people … if I was tired, if I was annoyed … people would say things to me like “have you taken your medication?” … It’s also a risk for me if I go into the hospital system so I have to be really careful … because I don’t have my health records altogether, they don’t know that once upon a time I had a diagnosis of bipolar disorder. If they did, they would treat me differently … I have to be vigilant around all sorts of systems.
Treatment Undermines and Disrupts Mothering
Five participants in the study were mothers, and one participant was pregnant with her first child. Each of the participants who were mothers described in detail the complex and stressful intersections between mental health system involvement and mothering. In addition, several participants who did not have children described the ways in which mental health treatment had delayed or entirely thwarted their hopes and plans relating to motherhood.
Participants described the intense grief, fear and uncertainty caused by the separation from their children during hospital admissions, which was often not well recognised by mental health staff. Women were often not provided with options or supports to maintain their mothering identity and responsibilities: My husband came once and I invited him and the kids in … then the nurses come rushing over and they’re like, “Children are not allowed in here” … Being separated from my children for a whole weekend … that was really hard…. It was horrendous [breast] pumping [for breastmilk], questioning my decision, like am I doing the right thing? … Or do I dry my milk up so I don’t have to go through this agonising pain?
The fear experienced by mothers in the context of an involuntary mental health admission was compounded by child protection system involvement. Two participants’ children were removed from their care following involuntary mental health treatment. Participants described the sanist assumptions that were made by child protection workers that mental distress is automatically connected to unfit or “risky” mothering: It’s been horrific, losing the children…. Just give ladies a chance with their children…. Just because you’ve got a mental illness doesn’t mean you can’t have your children…. I think that’s a bit unfair … I didn’t get a chance at all.
Child protection involvement following an involuntary admission could be protracted, and cause ongoing stress and crisis in women's lives: I am so crazy busy. Like it’s crazy, especially with one son coming back and I’m still going through court and it’s not a nice process. And you’ve got visits. I work one weekend, I go to [suburb] the next to see my son. This is just dragging on.
Two participants described their strategic decisions to downplay their distress, in order to avoid an admission. Although this left them without any support, they preferred this outcome to the consequences of child protection involvement: That’s not an option for me…. My kids would have to go into care… Like yes, [an admission is] going to keep me safe there and then, but it’s not going to help in the long run, and that’s what I need…. I just lied…. Just said what they wanted to hear kind of thing … “I’m fine, just – yeah, had a bad day” … Yeah. I’m not dumb.
Participants described the increased gender inequality that can arise in the context of mothering, and the unbearable weight of social expectations on mothers, as core drivers of their distress, but such contexts were rarely taken into account by mental health workers. This led to further despair for women, who were provided with a pathologising diagnosis and a lack of meaningful support. In addition, participants described the significant impacts of gendered violence on their wellbeing as mothers, which was frequently overlooked by mental health services that focused narrowly on biological explanations of distress: My relationship broke up and my ex-partner went to jail for trying to kill me, and then I was really, really struggling at home with my kids … trying to get help.
For some participants who did not have children, involuntary treatment delayed and undermined their dreams of motherhood. For example, women were denied essential information about the implications of psychotropic medications on fertility and pregnancy, or were provided with paternalistic messages about the inappropriateness of pregnancy and mothering in the context of a psychiatric diagnosis. A participant described her rejection of such significant attempts to control her life by mental health professionals: The message I got was, you shouldn’t be trying to have kids … [Laughs] I keep wanting to bump into my old psych … see me with my big [pregnant] belly now.
Recovery Is Found Outside of Coercive Mental Health Systems
It is important to note that mental health recovery is a highly contested term, which has been critiqued by many survivors as a concept that reinforces professional knowledges about the importance of symptom elimination (Moulding, 2015). Participants in this study, however, spoke about recovery as a broad and self-defined concept, most often found outside of the carceral mental health system, and often in the context of a community rather than as an individual experience. Many survivors described accessing alternative mental health supports following involuntary treatment, which offered space to explore social justice issues and to value rather than pathologise emotions, although finding this support was often based on a combination of luck and financial resources, as women usually paid private fees: What I’ve done in therapy, it’s really been about how do you survive in unjust circumstances, so that you can live a meaningful, rich life that you value, and continue? That’s really been what it’s been about.
One participant described an outright rejection of psychiatric understandings and mental health system involvement altogether in order to reclaim her life on her terms, while acknowledging the social privileges and resources that allowed her to do this: If I didn’t get out of the mental health system I would have suicided, that’s what I was heading for in that system because it made my life so dark and black … I’m well aware that where I was born, the colour of my skin ... has helped me to find my way out and I know others can’t … in that way it is really unfair.
Survivors described how coercive mental health responses led women to stop seeking help, and the importance of creating alternative forms of support for women to address this gap. A participant living in a rural context described the crucial need to address the isolation that can be experienced when avoiding mainstream supports: The system needs to be somehow a lot better than what it is. People are just trying not to go to hospital these days now and just trying to stay home but that’s not good for them either, like they need to help otherwise.
Additionally, a First Nations woman discussed the need for an anti-carceral approach to supports and resources for people experiencing distress: I’m not “anti” having a place for people to have peace and quiet. But they shouldn’t be run like a detention centre or a prison.
Participants spent time in the interviews imagining alternative supports and resources for women outside the constraints of the medical model. A number of participants described the need to create safe spaces for women, as noted by a participant living in inadequate housing: A women’s space…. A room of your own, that’s Virginia Woolf…. She’s a classic.
In addition to safe spaces and deep listening with women, survivors described the importance of practical supports to alleviate stressors, for example, the gendered demands of mothering: There’s so many mums out there with mental illness, or whatever, struggling deep – like they don’t need you to tell them what to do…. Let her go have a shower. Let her go to the toilet. Go wash some bottles. Do something.
Finally, many participants reported that they had ultimately experienced recovery, from both distress and from the harms of psychiatric system interventions, outside the bounds of professional mental health services, for example, the importance of connecting with Country and culture within First Nations worldviews: I love the feel of the red sand between my feet and all of my friends are here…. And to feel so loved and so wanted and so important and a part of the community has also been really healing.
A young woman with multiple disruptive admissions during her 20s described the role of creativity in resisting psychiatric oppression: There’s a sense like if I have that control and knowledge of who I am then I will always be free regardless of whether I’m physically free. That’s sort of where the poetry I guess came into it.
Discussion
This study reveals the ways in which women's experiences of involuntary mental health services are shaped by interconnected psychiatric and gender oppressions. The role of involuntary mental health services in pathologising women's lives and compounding their experiences of gendered violence is therefore an urgent priority for feminist mental health workers, activists and researchers. The findings elucidate key implications for social work, including both immediate changes to practice, as well as the need for social workers and researchers to contribute to the larger projects of mental health system reform and developing anti-carceral alternatives to involuntary mental health treatment.
Use Intersectional Feminism to Understand the Impact of Psychiatric Coercion on Women
This study mirrors other research that has reported on the significant harms, disempowerment and deprivations experienced by survivors of involuntary treatment (Watson et al., 2014; Whitaker et al., 2021), however through the use of a gender lens, the heightened and specific harms experienced by women have been made visible. For example, participants described gendered impacts of medication, the disruption and undermining of women's roles and identities as mothers, the refusal to provide pregnancy and fertility information, the pathologisation of women's emotions and sexuality, and the use of diagnostic language to conceal the experiences and impacts of gendered violence. An intersectional feminist lens makes visible the impacts of additional forms of oppression, including racism and poverty, on women's experiences of psychiatric coercion, for example, humiliating interactions with police experienced by First Nations women, and a lack of access to alternative forms of support for women without financial means.
Address the Detrimental Effects of the Medicalisation of Women's Distress
Involuntary treatment obscured the relationship between women's experiences of social inequalities and their emotional suffering, through a rigid medical model that positioned women's distress as evidence of dysfunction that required “treatment.” Survivors described the often devastating impacts of being contained and medicated in a carceral environment, with little or no support being provided to address the social determinants of their distress, meaning that upon discharge, they returned to situations including gendered violence and poverty, with the added stressor of navigating a new, stigmatised identity as a woman deemed to be “mentally ill,” which often led to ongoing negative consequences across the lifecourse. In addition, although this study concurs with other research that has described the harms experienced by mothers in psychiatric settings due to separation from their children (Stephenson et al., 2018), our findings demonstrate that a mere expansion of mother and baby psychiatric inpatient units will be insufficient in addressing the oppression experienced by mothers. Rather, broader transformations in care are required, in order to ensure genuine steps towards liberatory practices, including challenging the relentless medicalisation of women's lives in the context of gender inequality, disrupting the conflation of maternal distress with parenting capacity, and addressing the failure of psychiatric services to respond holistically to the social drivers of maternal distress, including gendered violence.
Update “Trauma-Informed” Guidelines to Acknowledge and Address Iatrogenic Harms
In addition to a failure to address the impacts of gendered violence on women's lives, mental health units were themselves often terrifying places for women, due to their lack of safety from men who perpetrated sexual harassment, assault, and intimidation. Thus, women were placed in an environment that intensified their distress. Survivors expressed anger and incredulity that they had been placed in such unsafe settings as a strategy that was supposedly intended to reduce their distress. In addition, for many participants, involuntary treatment itself replicated the dynamics and tactics of gendered violence, through the use of excessive masculine force, locked seclusion rooms, restraint, the carceral environment, and diagnostic processes that covered over women's stories with stigmatising labels. Given that such practices were experienced by survivors during recent admissions, the inadequacy of trauma-informed policies in addressing intersecting gendered and psychiatric harms for women in acute mental health settings is evident – in particular, the failure of mainstream trauma discourses to adopt a gendered lens to comprehensively engage with women's experiences in acute mental health settings (Women's Health Victoria, 2019), and the failure of trauma discourses to meaningfully challenge the iatrogenic harms that are inherent to involuntary treatment. Therefore, in addition to the crucial step of ensuring sexual safety in mental health units (Watson et al., 2020), this study elucidates the need for much more far-reaching paradigm shifts in how women's distress is understood and responded to, beyond the constraints of carceral logics and medical frameworks (World Health Organization, 2021).
Centre Survivor Knowledges in Mental Health System Reform
Despite the profound impacts of involuntary treatment, women demonstrated creative strategies to actively resist and survive psychiatric oppression, including adjusting their behaviour to avoid further diagnoses, downplaying their distress in order to protect their children from the adverse impacts of an admission, refusing to comply with directions to delay motherhood, and connecting with and gaining support from other survivors. For some participants, taking part in this research study was a further form of resistance. Participants also described their attempts to move away from psychiatric understandings of their distress, through strategies that included accessing less pathologising forms of mental health support in the community, imagining improved forms of care that could better support women, finding recovery on their own terms outside of the purview of professional mental health services, or moving away from psychiatric labels and the mental health system altogether. Survivors’ understandings of alternative responses to women's distress challenged the simplistic idea that rejecting involuntary treatment involves neglect and an absence of support (Maylea, 2017). Instead, participants imagined possibilities for providing care to women without coercion and beyond the constraints of psy-knowledges.
Develop Alternatives to Involuntary Mental Health Treatment
Given the intersecting oppressions experienced by women survivors of involuntary treatment, this study demonstrates the value of building solidarity and stronger alliances between feminist and critical mental health movements. The feminist aim of eliminating violence against women must extend to the violence experienced by women within psychiatric settings, and critical mental health activism will be strengthened by an increased awareness of the gendered dimensions of women's experiences of psychiatric coercion. Social work as a profession must move beyond a tacit acceptance of involuntary mental health treatment, and instead engage in much more concerted actions to disrupt the reliance on compulsory treatment as a response to mental distress. Given the profession's espoused social justice values, social work has a responsibility to work towards anti-carceral responses to distress that are based on human rights and survivor knowledges (Daley et al., 2019).
Limitations
The study is limited by its relatively small sample size, and as such we do not make claims about the generalisability of the findings at a population level. Barriers including a lack of time, access to technology, or privacy may have precluded some women with relevant experiences from being able to participate. The use of snowball sampling has been critiqued for its reliance on the existing networks of “hidden” populations. As some participants found out about the study from a newsletter sent by a “consumer” organisation, their analysis may have been informed by their connections to advocacy in the mental health sector, which not all survivors have accessed. The use of Zoom technology to conduct most of the interviews is likely to have hindered rapport-building in some instances. The extended lockdown also reduced opportunities to use creative methods in addition to interviews; it is hoped that the next phase of the study will generate further opportunities to use creative methodologies. Despite these limitations, the urgent need to question the assumptions of mental health service provision, and to transform how women's distress is understood and responded to, has been strongly demonstrated by the study.
Conclusion
Apart from some notable exceptions (Beaupert & Brosnan, 2021; Burstow, 2006; Daley et al., 2019), mental health treatment is rarely characterised as a form of violence against women. This study has demonstrated that psychiatric treatment is both complicit in and amplifies gender oppression, through multiple layers of force, violence, humiliation, neglect and disempowerment. Through centreing the voices of survivors, this study has demonstrated the astute analysis of women with direct experiences of psychiatric coercion, as well as their resistances. It seems fitting to end with the words of a survivor: “To me, it's something about returning the shame to where it belongs … take that shame that we feel and put it back on the systems and practitioners or hospitals that have let us down, because it’s they who should be ashamed.”
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Australian Research Council (grant number DE210100391).