
Abstract
This article, reporting on a Canadian-based research project, tells the stories of three first- and second-generation, racialized, young women from immigrant families in order to illuminate their unique realities of intergenerational care and to better understand the role of gender, racialization, and migration in shaping their lived experiences of care. Using a feminist-informed adaption to the intersectional life-course approach, we explore the life-course challenges experienced by these women and their perspectives on agency, resilience, and resistance in light of personal, relational, and structural barriers faced by both themselves and their parents and grandparents for whom they provide care. Findings related to meanings attributed to care and family, developmental and relational disruptions and their impact, hybridized subjectivity, and responses to discrimination and social isolation are explored through the telling of women’s caring stories across time. The article concludes with recommendations for social work intervention and service provision in order to better recognize and support racialized young first- and second-generation adult women carers across sectors.
Research has begun to address the unique perspectives, experiences, and challenges of providing care across generations by children and young adults to their parents and grandparents. Most of this work has focused on children under the age of 18 who provide care to family members with mental and chronic health conditions (Aldridge, 2006; Becker, 2007; East, 2010). A smaller, but growing body of literature regarding the experiences and impacts of young adult care provision (18–35 years) has emerged in recent years, pointing to the many consequences of care, both negative (i.e., delayed developmental milestones, educational and career disruptions, social isolation) and positive (i.e., emotional maturity, enhanced capacity to organize; Pope et al., 2018; Thomas et al., 2003). It should be noted that throughout this article we use the word “carer” instead of “caregiver.” In recent years, activist groups have taken up the term carer in order to contest the binary, unidirectional, and nonreciprocal assumptions embedded within the term caregiver (Carers Canada: www.carerscanada.ca).
Although the gendered nature of care has been thoroughly addressed within the broader feminist literature on aging and care over several decades (e.g., see Calasanti, 2009; Neysmith et al., 2012), considerations of women’s unique realities in the context of young adult intergenerational care have only recently received attention (Silverman et al., 2020). Similarly, considerations of the intersection of gender and age among ethnocultural minority, immigrant, and racialized carers have been underexplored. Reasons for this include the fact that expectations of care within families, as an expression of filial piety/family obligation, persist regardless of gender and age (Chappell & Kusch, 2007; Rudolph et al., 2011). As well, economic, social, and structural precarity has been theorized as contributing to an increased sense of commitment to intergenerational and reciprocal forms of care within these populations across age and gender groups (Ferrer et al., 2017a). Still, there is some indication that among ethnocultural minority and racialized carers, gender norms in care are similar to the general population, as men tend to take on the role of carer in addition to the realization of developmental milestones (i.e., educational/employment pathways and marriage), while women are more likely to forego or delay these milestones, to cohabitate with care recipients (Jones et al., 2011; Rudolph et al., 2011), and to care for both parents and in-laws. In general, the absence of a gendered analysis of care within ethnocultural, immigrant, and racialized communities renders women’s lived experience under Eurocentric, hetero-patriarchy 1 invisible, leaving their subjugation and exclusion, as well as their agency, undocumented. There is much to be explored in the context of care across generations and within ethnocultural minority, racialized, and immigrant contexts, particularly with respect to documenting the life stories of care from the perspectives of young adult women carers.
Using a feminist-narrative lens, our research sought to investigate the life-course experiences and trajectories of young adult carers, defined as between the ages of 18 and 35 due to the developmentally significant changes that tend to occur during this period (Dellmann-Jenkins et al., 2000). The project, based in a large Canadian urban center in the province of Ontario, explored the stories and meanings of providing care, centering on life-course challenges and opportunities. In this article, we tell the stories of three racialized young women interviewed as part of the larger project in order to illuminate their unique experiences of care and to better understand the role of racialization and migration in shaping both their lived experiences of and the meaning attributed to care. Using a feminist-informed adaption to the intersectional life-course approach (Ferrer et al., 2017b), we explore these women’s perspectives on agency, resilience, and resistance in light of personal and structural barriers faced in the context of care. We present a portrait of each woman’s story before highlighting both the shared and unique themes within and across stories. We conclude by suggesting recommendations for change to the design and delivery of health and social care services in order to more comprehensively attend to the challenges facing racialized, first- and second-generation 2 young adult women carers and their families.
Review of the Literature
Approximately 1.9 million Canadians aged 15–29 are actively engaged in care responsibilities, most often for a grandparent or parent (Bleakney, 2014). The number of young carers, however, is likely higher, as young carers often do not identify themselves as such (Boumans & Dorant, 2018; Leu et al., 2018). Despite this prevalence, research on carers has tended to focus on adults aged 40–60, often at the height of their career and familial responsibilities, and to a lesser extent, child carers under the age of 18 (Butler & Astbury, 2005; Sinha, 2013). From a Canadian policy perspective, awareness about the challenges facing young carers, and appropriate policy and program development, continues to lag behind when compared to other countries such as the UK (Stamatopoulos, 2016).
The limited research conducted with young adult carers points to a range of common positive and negative impacts including experiences of parentification (also known as role reversal, when a child takes on responsibilities typically reserved for a parent), social isolation, and alterations in life-course trajectory (Thomas et al., 2003) as well as the development of resilience (Pope et al., 2018). An even greater complexity of experience is unearthed when taking into consideration ethnocultural minority identity, from the cultural norms placed on young carers (Phar et al., 2014) to the impacts of taking on a caring role in a society whose health care system is often insensitive to ethnocultural diversity (Brotman & Ferrer, 2015).
Given the heightened level of family responsibility, young carers often face social isolation. Many young carers have limited resources (emotional and financial) to engage socially, and as a result, their caring role can be experienced as distancing them from their peers (Thomas, 2003). Children and young adults who are family carers are also more likely to be absent from school, perform more poorly academically, report higher levels of stress (East, 2010; Thomas et al., 2003), and experience a lack of understanding from both teachers and peers (Butler & Astbury, 2005). For young adult carers, the ages of 18–35 are developmentally significant, encompassing a transitional period into adulthood, when one potentially engages in many impactful decisions regarding education, careers, partnership, and child-rearing, among others. When this period includes family care, a young adult carer can lose out on time-sensitive activities for future development (Dellmann-Jenkins et al., 2000; Heyman & Heyman, 2013).
Despite the potential negative impacts of care on youth and young adults, these experiences can also be positive. They can help young people mature and gain life experience, strengthen their family bonds, cultivate sensitivity to others, develop resilience and effective coping mechanisms, and learn to manage stressful situations (Day, 2015; Greene et al., 2016; Heyman, 2018; Heyman & Heyman, 2013; Levine et al., 2005; Pope et al., 2018; Shifren & Kachorek, 2003). Role reversal can also be experienced as positive, when prior close relationships are experienced as being enriched through the act of care provision (Petrowski & Stein, 2016) or, in the case of immigrant families, when care is perceived to benefit the overall well-being of the family unit (Burgos et al., 2017).
While research has brought to light important new understandings of the experiences of young adult carers, there remains a dearth of literature addressing how one’s ethnocultural, racialized and/or immigrant identity, and social location affects young adult carers’ experiences, despite knowledge that culture can influence both attitudes toward care and roles and responsibilities irrespective of age (Lai, 2010). One of the more extensively explored topics concerns adherence to concepts of filial piety/family obligation and how this impacts an individual’s understanding of care. Filial piety defines familial roles, guiding children to be respectful of parents, and placing family needs above individual interests (Khalaila & Litwin, 2011; Lai, 2010). Care by children is often viewed as necessary to the fabric of the life of a family and serves to support the development of a child (East, 2010; Lai, 2010; Phar et al., 2014). According to research, belief in the importance and benefits of filial piety/family obligation exists within many cultural communities. For example, filial piety within Chinese communities has been found to help mediate stress and acts as a buffer against depression, in both diaspora and home country contexts (Lai, 2010; Pan et al., 2017). In addition, within filial systems, women, mostly spouses or daughters, are often the primary carers to parents and elders (Chappell & Kusch, 2007; Pharr et al., 2014; Rudolph et al., 2011), though there can be substantial variance between cultures in how care expectations are delineated with regard to gender (Jones et al., 2011; Pharr et al., 2014). Furthermore, familial relationships within cultures where filial piety is important cannot be understood as unidirectional, with the care recipient passively receiving support from family members. Care recipients are often engaged in complex care relationships with their wider families, providing care and support to others in reciprocal dynamics that may be overlooked by outsiders to the community (Ferrer et al., 2017a).
Although numerous studies have pointed to the increased likelihood that ethnocultural minorities will care for their family members at home, as well as eschewing formal services (Lavoie et al., 2010; McCann et al., 2000; Mintzer et al., 1992; Napoles et al., 2010), prevalent Eurocentric and sexist stereotypes of collectivist culture, and women’s roles within families, tend to result in an overemphasis on this point, without understanding causal factors that contribute to these decisions. This often results in inadequate service provision (Brotman & Ferrer, 2015). For instance, service providers working with families from minority ethnocultural backgrounds often falsely assume that family members are prepared to provide care and fail to consider wider structural forces shaping diasporic realities and contexts (Brotman & Ferrer, 2015). It has been reported that a significant aspect of decision making within ethnocultural minority families relates less to culturalist values and more to mistrust and the perception of discrimination in society generally and within health and social care services specifically (Napoles et al., 2010).
Understanding diversity within and across cultures is also necessary. Experiences of care cannot be assumed to be universal among people from similar ethnic and cultural backgrounds; variation not only occurs naturally within ethnocultural groups but is also influenced by an individual’s complex relationship between their background and the wider dominant culture (Asai & Kameoka, 2005; Flores et al., 2009). An individual’s particular caring role may be defined by a multifaceted interplay of more “traditional” values and the individualist values predominant in Global North societies (Flores et al., 2009). Furthermore, professional training can sometimes preclude service providers from taking into consideration how race, gender, and class impact health care delivery because of a discourse of “treating all people the same” (Brotman & Ferrer, 2015; Johnson et al., 2004). This evidence points to a concerning lack of attention to the diversity among carers and to the invisibility of the unique concerns and realities of racialized and immigrant young women carers, which represents a significant gap in both research and practice.
Methodology and Theoretical Framework
The research project on which this article is based explored young adult carers’ everyday lived experiences and the impacts of care responsibilities on their life-course. The project used a feminist-narrative approach in order to capture the lived experiences of carers over time, the meaning they attributed to their experiences as well as call attention to the helping and hindering forces which shaped those experiences. Narrative forms of inquiry focus on both context and meaning by asserting the central importance of individual turning points, as well as the social context in which they occur. Interviews are usually conducted as conversations, and the data are therefore seen to be “coconstructed” between researcher and participant (Brotman & Kraniou, 1999; Brotman et al., 2020). For the current article, we adapted our analysis of stories told by the young racialized women carers to take into account intersectional identities and interlocking forms of oppression through the application of a feminist-informed adaptation to the intersectional life-course approach (Drummond & Brotman, 2014; Ferrer et al., 2017a, 2017b). In this way, we remained consistent with the approach used in the larger project but enabled an accounting of stories that highlight intersectional identity (gender, race, class, age, and citizenship) and structural forms of oppression (invisibility, exclusion, and erasure) as central features of meaning-making and analysis.
An intersectional life-course perspective is based upon the categories of (1) major life events, timing and the structural forces which shape these events; (2) “linked lives” in both a local and transnational context; (3) categories and processes of differentiation (i.e., identity, social location, and processes of othering); and (4) oppression, agency, and resistance. Each of these categories is interconnected and illuminate intersectional realities, structural oppression and processes of differentiation across time and borders, and which are explicitly and/or implicitly embedded within individuals’ life stories, experiences, and perspectives (Ferrer et al., 2017b). The concept of linked lives is particularly important in the current article because it can support the idea that care is seldom experienced individually and invokes relationships between individuals, families, and communities across generations. Thus, the concept of globally linked lives takes into account how people organize their lives, and formulate their identities based on relationships that occur with family, ancestors, between generations and across transnational contexts. (Ferrer et al., 2017b, pp. 12–13)
In the larger study, the research question asked: What are the lived experiences of young adults caring for an older adult with a disability or a chronic physical, cognitive, or mental illness? We defined “young adulthood” as ranging in age between 18 and 35 years old, yet we were flexible with our criteria, as young adulthood is related not only to chronological age but also to lived experiences and stages of life. Participants were recruited through a combination of tactics: social media, word of mouth, and reaching out to practitioners in numerous governmental health agencies and community organizations in the province of Ontario, Canada, in which the research took place. The principal investigator (Author 2) conducted at least two interviews with each participant, each lasting approximately 1½ hr. During those interviews, the principal investigator employed multiple forms of data collection: (a) social network maps, (b) participant-driven photography, and (c) caring lifelines. A detailed description of interviews and lifelines is presented here as they make up the data sourced for the current article. During the first interview, after gaining a broad understanding of participants’ care contexts and asking them to map out their social connections (Campbell et al., 2019), the researcher asked participants to draw a “careography,” an innovative lifeline tool developed by Orzeck (2016) for eliciting conversations about carers’ important turning points. Using markers and a large piece of paper, carers created a lifeline of significant events in their own lives, as well as, in a parallel lifeline, significant events in the life of the care receiver (Orzeck, 2016). These lifelines provided a visual representation of participants’ care trajectories over the course of many years and facilitated conversations linking time and events.
During the second interview, typically organized a few weeks after the first, the participant and researcher revisited the social network map and careography, as well as looked at photographs taken by the participants of important aspects of their everyday lives. All interviews were transcribed. Transcripts used for this article were coded and analyzed using Dedoose Version 8.1.8 software. 3 The fact that there were multiple forms of data collection (social network maps, photographs, carer lifelines, and researcher journal notes) added to the rigor of the study, as it allowed for a triangulation of the data. Yet one limitation of the study is that although the participants spoke about their stories of care from a longitudinal perspective, the researchers did not follow the carers over time.
This article tells the stories of Shani, Sandra, and Nadia, three young adult racialized women with personal and familial experiences of migration and care. These three women were selected as the focus of this article, as their stories provide the most complete portraits of migration and care. While each of their stories is unique, pointing to the multiple intersections of identity and migration across time, there are also shared experiences of family, community, school/work pathways, and services. Their stories of care, including a reproduction of the unique lifeline they drew during the interview (the format of which is their own creation), are followed by a thematic analysis using the four categories of the feminist-informed intersectional life-course perspective. This project adhered to Canadian Tri-Council guidelines and obtained ethics approval from the University of Ottawa and McGill University. For the purposes of ensuring anonymity and confidentiality, participants’ names have been changed to pseudonyms, and geographical locations generalized. Some interviews were conducted in French; in those cases, quotes were translated into English for the purposes of this article.
Findings: Portraits of Care
Shani’s Portrait
Shani is a 25-year-old woman from the Middle East. Her family moved extensively within the Middle East, Europe, and the United States, escaping violence and political turmoil and seeking a permanent migration opportunity. After her parents’ divorce when Shani was a young child, Shani immigrated to Canada from the United States with her mother and siblings. The family made several moves across Canada before settling in a large city in Ontario. Shani currently lives with her mother, brother, and grandmother and has a sister living in Toronto with whom she speaks regularly. Shani is the eldest of her siblings. In 2008, her grandparents moved in with the family after her grandfather had a stroke. Her mother provided most of the care at first, but after a few years, her mother was required to work longer hours and so Shani took on more care responsibilities, accompanying her grandparents on errands, going on walks with them, and driving them to social engagements. This lasted until her third year of university, after which she moved out to live on her own and found a job that required her to travel extensively. A few years later, Shani moved back into the family home after her grandfather became seriously ill as a result of complex chronic disease. As Shani explained, “my grandfather got really ill and I felt like my grandmother and everyone else needed me so I moved back home.” Because her job required her to travel, Shani made the difficult decision to quit her job so that she could provide full-time care to her grandfather. In 2016, after a month in the hospital, her grandfather passed away. Subsequently, Shani began providing an increasing amount of care to her grandmother, aged 73. At the time of the interviews, Shani was her grandmother’s primary carer.
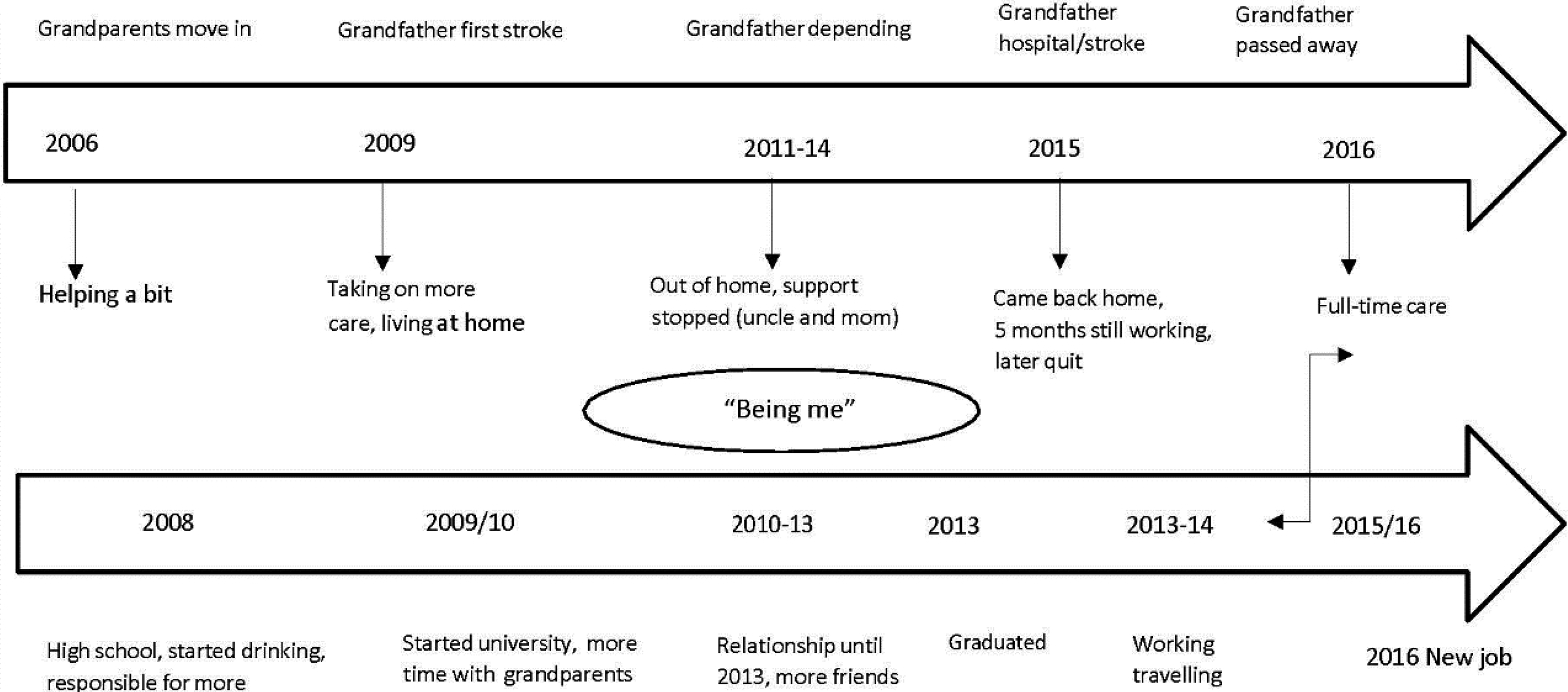
Shani’s careography.
Shani has a strong sense of filial obligation and is close and committed to her grandmother. She believes that, as an older immigrant, and someone with complex medical and psychological issues, her grandmother experiences a significant degree of community disconnection and social isolation; as such, Shani is concerned about providing social and emotional support. Despite the challenges and pressures of providing care, Shani’s commitment to family and her sense of responsibility help her juggle work and family: It’s just I have to work around how she feels on a day-to-day basis and I found a position where I can take the time off or I can take the day off just to be there for her. So yeah, I’ve adjusted. …my mom’s a single mom and I think because I’m the eldest of the family, I took on that responsibility and, of course, you develop a connection, especially with my grandmother because she has so many mental health illnesses that no one can understand her more than me and…she’s much more comfortable talking to me about what’s going on than anyone else…because my grandma…understands I know what she needs right away, so she doesn’t feel as comfortable anywhere else and she’s become so dependent on me and so taking her out…we’re both going to have fun tonight.
Shani’s future plans include her grandmother and mother. She was recently accepted into a graduate distance education program and hopes to find a management job near her family after graduating. Her dream of a property includes sharing it with her grandmother. She told us: If that was to happen, I think my grandmother would go under my wing, which I’m fine with that. I think I’ve always known that and I’ve always financially been saving money for that…knowing that I need a one-bedroom downstairs on the first floor with a washroom. So if ever my mom ever needed it, my grandmother would go under my wing…my mom…she took on a lot and I think she’s ready to just take time off for herself, which I want to give her, that capability without having that strain…knowing that there’s someone else there to take care of [my grandmother], so I’ll let her do what she wants to do. Honestly, when I was a kid I had a lot of hatred for the fact that I was given that responsibility, not just for the caregiving, but also taking care of my siblings…because my mom has always been a single mother. So I was always frustrated that I was dealt that…. I hated that responsibility when everyone else was doing a whole lot of other stuff. But it grew into me and I’ve become a more independent person and not have to rely on other people based on what I’ve experienced. you’ve got to settle, you’ve got to figure out another way to do things and I’ve learned a lot about myself and…. I’ve become more humble, you kind of have a bigger heart. And I think that that grew in me a lot and I did have a temper…but that to me is long gone. I think I’ve developed a sense of love to care.
Finally, Shani sees culture as playing a role in shaping family values and care to grandparents, although she says that she is not “very close to the Arab culture” and outwardly rejects “the pressure to marry and have a husband.” Still, she “like(s) to keep it around because my grandmother likes it, so we listen to Arabic shows and listen to some Arabic music…she’s very religious so I’ll do some sessions of reading the Koran…” and Shani maintains some involvement in her local Arabic community for her grandmother’s sake. They occasionally attend cultural dance events together.
Sandra’s Portrait
Sandra is a 36-year-old, second-generation woman of mixed-race descent who identifies as queer. Her father immigrated to Canada from East Asia 30 years ago with his first wife (now divorced). Sandra has one brother who lives in a different city and who is estranged from their father and thus not involved in his care. Her mother completed suicide when Sandra was a child. Sandra describes her relationship with her father, now 73, as close: “Like I’m his person, like he’s also mine.” Sandra sees herself as a lifelong carer; her father has lived with depression for much of his life and has many challenges. Since 1998, when he lost his job, he has not been able to work; this added to his depression. Nonetheless, he had been able to save money in order to continue to provide financially for his children. When Sandra was 14 years old, during a time of crisis, she took on a more significant role “taking care of things at home.” She has provided care since that time, a role that ebbs and flows according to her father’s mental and physical health status. In the interview, she described a kind of symbiotic relationship with her father with regard to her caring role: “He got a little more independent, I got more independent.” In the past year, her father was diagnosed with a rare form of cancer. He had a complex surgery to remove a tumor, followed by radiation treatments. This occurred during her graduate studies, and while she maintained her studies as best she could during that time, she also moved with her partner back to the city in which her father lived (about 400 km away). She and her partner stayed with him during his recovery following surgery and radiation treatments. As he got progressively better, Sandra and her partner moved out of his home but continued to live nearby.
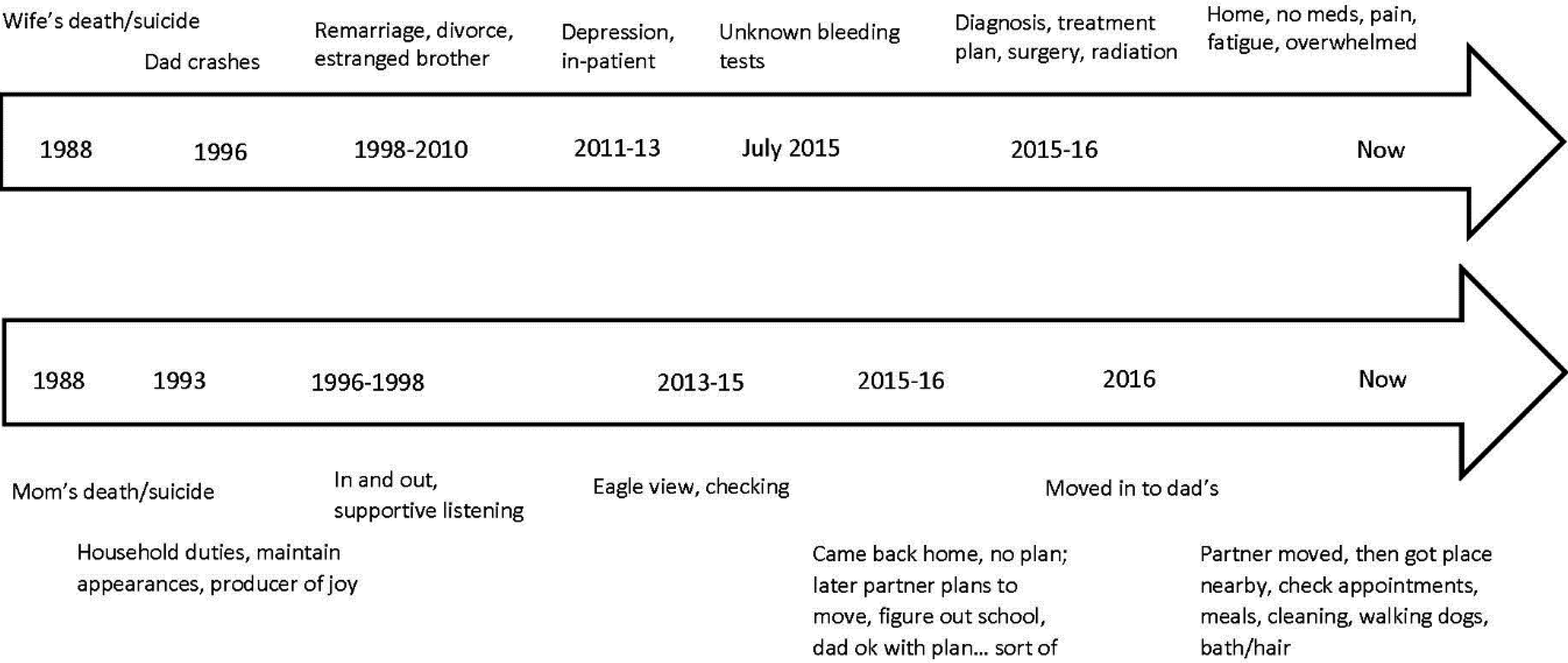
Sandra’s careography.
Currently, Sandra provides mostly organizational support, accompaniment, and emotional support. She stated: …I help him keep track of appointments and that type of stuff. I help him organize his medication, make sure that he understands updated medicine charts. I also help him communicate with medical professionals…a lot of when he feels overwhelmed by everything, just talking him down and listening to him and trying to kind of gauge what would make his life easier…because of his depression he often will push people away. So oftentimes he’ll be like “no, you don’t have to come, I’m going to do this by my own, I’m just going to suffer, my life is terrible now, this is just what I have to do.” And it’s like okay well, you also do not have to do it on your own, right? So sometimes it’s just like kind of navigating that along with the pain…
Sandra is the sole carer for her father, and there is no contact with extended family. Her father’s first wife, who Sandra identifies as a “kind of aunt,” has helped out periodically, particularly when her father was in hospital and postsurgery, but as things have stabilized, she has had a more limited role. Sandra describes her aunt as someone who brings a certain cultural familiarity and perspective on her father’s personality and life history, which Sandra values.
Sandra is insightful and reflects in-depth about her father’s and her own experience of illness and care. She is concerned about his and her own sense of cultural belonging and community connection, and the impact of migration and racialization on how her father (and other marginalized people including queer people) is treated in society and within health and social care services. As a graduate student and professional in the health and social care field herself, she has had the opportunity to think about her own relative privilege in contrast to other migrants, racialized people, and queer people and to question taken for granted assumptions about immigrants in the health care system. She spoke about these concerns in relation to some of the microaggressions her father has faced from health care professionals in the following quote: One of the reasons why I want to participate in this research is because I think that hospitals don’t always know how to treat immigrants and sometimes there’s a lot of bias there or assumptions that people don’t understand them or that…so many doctors would talk to me and not him; and I’m like; he’s lived here for 30 years, his English is beautiful, so what, he has an accent.
Sandra has a desire for connection to her cultural community, something she shares with her father and she sees this as a response to exclusion that she engages in with her father. As an immigrant, he misses a sense of belonging to his home and community. She seeks out opportunities within their East Asian community and calls these outings important and fun in that they are “buddies” in their enjoyment of events.
Although Sandra has managed to continue her studies off and on while providing care during this current crisis, she has had to put some of her other important life goals on hold, one of which is thinking about and having children. She described the feeling of putting personal projects on hold as “like just vibrating kind of in one spot.” She also worries about what will happen after her father dies and is concerned about losing connection to family and culture, both for herself and for the potential children she may have. But she feels fortunate to have the support of her partner, her partner’s family, and her friends and colleagues. As a student in a helping profession, and as a queer racialized woman, she has what she describes as a rich and unique opportunity to learn about social exclusion, resilience, and resistance firsthand; undertake assignments that explore her and her father’s lived experiences; and find community and collegial solidarity. She knows that this is a privilege and is grateful. She explained that her experience of care in childhood, youth, and young adulthood has made her a more caring and resilient person and she seeks out those traits in others. Sandra explained: My dad has impacted my decisions all my life, right?…. I [have always] date[d] people who are very solid…people who will just stand by you and do things and get stuff done. I’ve always felt like I needed that because I didn’t have that at home, but also because my family requires that…and of course it’s not simply that’s why I pick these people (laughs), but I’ve noticed a pattern that I find really steady,…loyal people who are like…you just brush off your hands and you get things done.
Nadia’s Portrait
Nadia is a 26-year-old woman from French-speaking West Africa. She immigrated to Canada 8 years ago to attend school, and she lives with her sister. Another sister lives close by. Her father, 71, came alone for a 1-week visit in 2016 (both parents and extended family still live in West Africa). While staying with Nadia and her sister, he began to feel ill. Nadia accompanied her father to several urgent care clinics, receiving different information about the cause of his problems, and treatments on each visit. On a visitor’s visa, and with his travel insurance covering only specific costs, her father was required to pay for all of his health care and treatment out-of-pocket. The day following a visit to a local clinic, Nadia’s father began having difficulty breathing and walking, so they went to the hospital emergency room. The doctors told them the father was in a grave situation; he had water on his lungs, a blood infection, and “silent heart attacks.” They discovered that he also had pancreatic cancer. Unaware that he had previous problems with his health before the trip, Nadia was surprised to find out that he had been falling back home and was told by doctors there that this was the result of long-standing pneumonia. Nadia told us: …all that was revealed, so he was sick for a very long time and he knew his situation, but he didn’t tell us. And it is even the reason why he came to see us for one week…. And since we are all here in Canada and he was in West Africa, he didn’t want to die without seeing us.
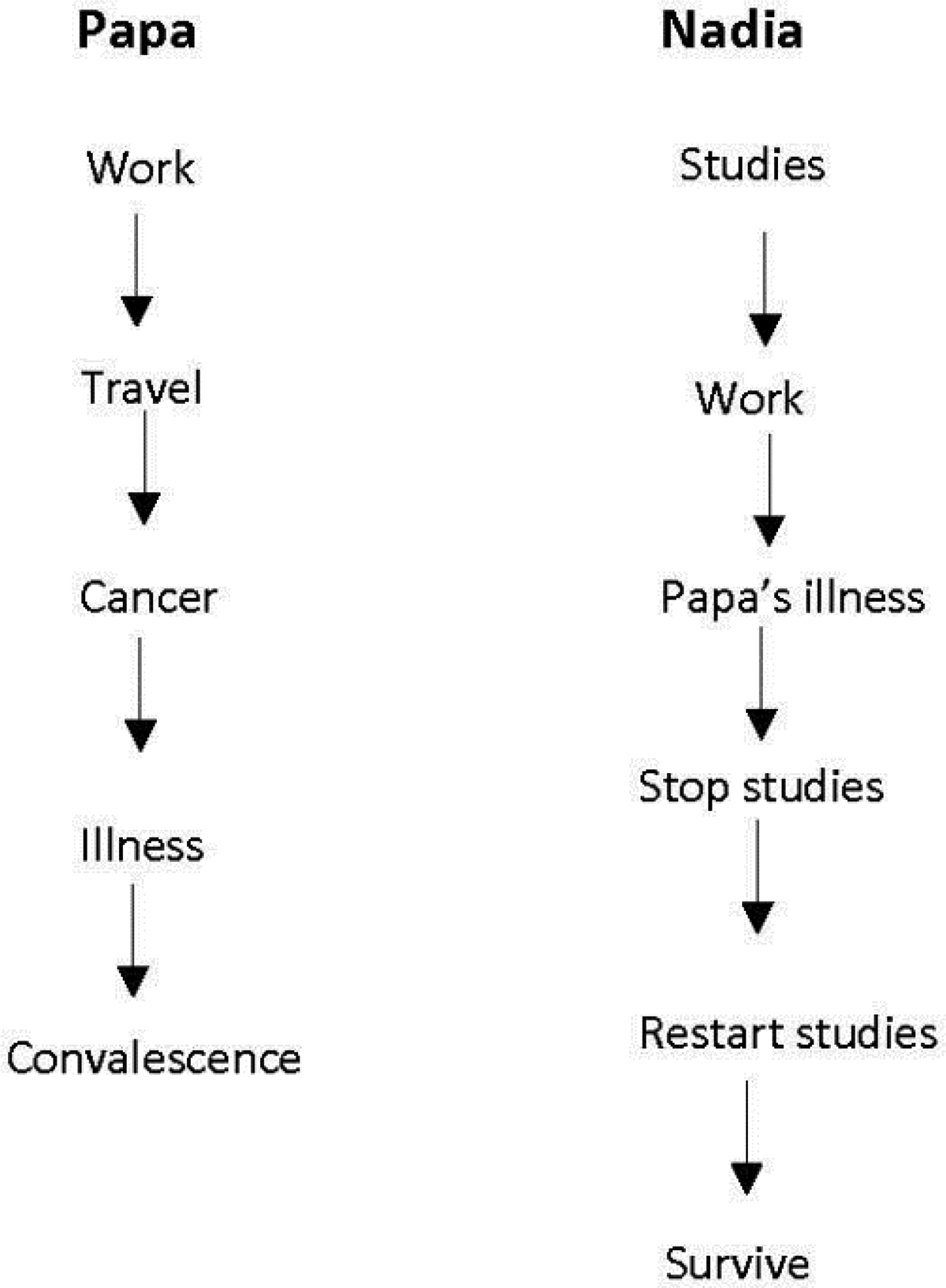
Nadia’s careography.
In order to accompany her father to appointments and on other errands, Nadia must often abandon her work and rush around. Differences between health care practices in her home country and Canada have also added to the burden of caring for her father. At home in West Africa, one can go to any clinic or pharmacy, but in Canada, health services are not coordinated. So she has to run to different places for prescriptions and follow-up based upon where her father decides to go on any given visit. She also worries about her father’s financial situation.
Her mother recently arrived from West Africa in order to help with care tasks and has been sleeping with Nadia in her bedroom. Instead of helping the situation, Nadia finds that her presence has only increased her level of responsibility and lack of privacy. For example, Nadia decides to move into the living room and sleep on the sofa because her mother is not sleeping well. So now Nadia finds herself without a room in which to rest or be alone. She told us: “…my life is lived in the living room now, on the sofa.” Sleeping in the living room makes Nadia feel as if she has no life: “I no longer have a life…there is not one moment when you can close the door to study, they are constantly there.” She also says that her father does not consider privacy as important, as this is not his cultural or personal practice; therefore, he constantly enters into her space, reading in the living room, for example, rather than in the library set up in his own room. In order to study, she must typically wait until around midnight when her father goes to bed. Still, she says that she “does not require a lot of sleep” and so is able to cope. Also, because her mother is unfamiliar with the Canadian system and has her own way of doing things, Nadia must provide accompaniment and cultural interpretation for her. As one example, her mother prefers to buy fresh groceries each day for each meal, rather than make a larger purchase in one trip, adding to the time and energy required of Nadia to accompany her.
Because of her care tasks, Nadia decided to put her studies on hold for a few months while her father stabilizes but after a few months was able to return to school to continue her master’s degree. Still, Nadia feels that she has no choice but to put herself and her goals aside and says that she can no longer plan for the future. For example, while she used to want to pursue a doctorate, this is no longer the case. And while she feels pressure from the family to be the primary carer she understands the meaning and importance of filial piety and considers her family as her most significant social network. She also communicates daily with extended family back home to share news and receive support. She is exhausted and would like to return home but cannot do so during this time of crisis. She told us: Now, I can no longer make plans, and I tell myself I am the only one that can return, because the others, they work. Me, I don’t work so…. And mentally, I am no longer interested in doing a doctorate, because I no longer have the mental energy, I am mentally exhausted, and so I will certainly return to my home.
A Feminist-Informed Intersectional Life-Course Interpretation of Women’s Stories of Care
Shani, Sandra, and Nadia’s stories demonstrate the unique and diverse experiences of care among young racialized women. The impact of migration, either their own or those of the people for whom they are caring, has shaped both their personal and structural realities of care in a myriad of ways. The following thematic analysis is framed by the four overlapping categories of the intersectional life-course perspective (Ferrer et al., 2017b) and centers on a feminist-informed analysis of women’s experiences as being shaped by Eurocentric and hetero-patriarchal discourses and practices of care embedded within these categories, namely (1) timing, events, and structures; (2) locally and globally linked lives; (3) categories and processes of differentiation; and (4) oppression, agency (resilience), and resistance. What is made evident in the telling of these three stories is that young first- and second-generation racialized women face particular challenges and tensions within the provision of care embedded within their intersectional identities and social locations. These challenges and tensions also engender forms of agency (resilience and resistance) in the face of personal, familial, cultural, and structural forces that demonstrate both strength and compassion.
Timing, events, and structures
Shani, Sandra, and Nadia share many of the challenges of young women carers in general (Brotman et al., 2020). For example, they described how providing care to parents and grandparents as youth and young adults impacted their identity, sense of safety and control, and opportunities to self-actualize. Events such as health and mental health crises of parents and grandparents, and the limited availability of other family members to provide care, resulted in all three women taking over household and other tasks and putting their own needs aside. Decisions to delay or quit work and/or school were seen as key turning points in their lives and in solidifying their identities as carers. All three also described realities common to all carers, including stress, reduced physical and mental well-being, a lack of privacy and free time, financial constraints, and limited or disrupted educational and career pathways (Fruhauf & Orel, 2008; Thomas et al., 2003). The structures and spaces in which key meaningful events took shape were diverse, but for all three participants, these included intersections of (im)migration pathways and their corresponding policy/program restrictions, health and social care systems, educational and work spaces, cultural communities and, most importantly, home as the primary site of family care. Structural constraints, including the lack of supports and recognition, led to unique experiences of barriers resulting in delays in the women’s achievement of developmental milestones. This will be addressed in more detail in the subsequent categories.
Globally and locally linked lives
All three women described having little or no time to make friends and to socialize outside of their close family circle and have instead focused on the care receiver and other close relatives as their main social network. This reality is supported in the literature, which identifies the family as a primary social network among immigrant youth (Burgos et al., 2017). Sandra, in particular, having provided care to her father since childhood, described having had limited opportunity to build and sustain friendships early in life. Shani also spoke of having care responsibilities for siblings at a young age and feeling resentful at the time for missing out on the fun and freedom that others in her peer group experienced. For Shani and Nadia, the development of intimate relationships was also described as problematic. While Sandra experienced a larger social network and was in a long-term couple relationship, the fact that she was the only Canadian-born woman of the three may have given her increased opportunity and ability to build networks over the life course. In fact, both Shani and Nadia spoke to adjusting expectations, retreating, or not having available social networks like other peers because of the combined impact of migration and family care. As a recent migrant, Nadia expressed a disruption to her sense of community as having had an impact on her well-being and described her desire to “return home” in the face of exhaustion, letting go of the goals that first brought her to Canada. While her sisters were a source of support, they simultaneously were experienced as a source of pressure which made it difficult for Nadia to find solidarity in her adopted country.
As with many international migrants, transnational relationships continue to be of utmost importance in achieving a sense of belonging and support (Brotman & Ferrer, 2015), and Nadia described daily contact with the extended family in West Africa by telephone as important. This supports the relevance of globally linked lives among migrant women who have either recently arrived or who have temporary migration status. Similarly, Sandra’s experience of belonging to queer community facilitated her sense of connection. Belonging to queer community also helped her build empathy for other marginalized peoples and develop long-term strategies of survival and resistance not available to migrant groups outside the family unit, particularly those with fewer opportunities for cultural and social connection within a Eurocentric host society. Sandra spoke of her sense of privilege in being able to enact solidarity both within her queer and school communities, recognizing how racialized recent immigrants would likely experience more intense forms of exclusion and disconnection.
All three women reported that their experiences of young caring shaped their perspectives and expectations regarding social and intimate relationships. For example, Sandra spoke about her efforts to seek out friendships and partnerships with people like herself; stable, committed, believing in family obligation, and willing to do what it takes to get things done regardless of self-interest. All three spoke of the desire to connect to people who would understand and support their choices in symbolic and practical ways. Shani articulated a willingness to do for herself, by herself, rather than engage with a social network with little understanding of her values and role.
Categories and processes of differentiation
In terms of their own identities as racialized, first- or second-generation women, all three participants spoke of tensions negotiating the values of collectivism and individualism within the context of their life journeys, which is consistent with the literature on the experiences of youth and young adults within immigrant families (Burgos et al, 2017). This reality is also shaped by gendered caring relations across the life course (Silverman et al., 2020). For example, Nadia struggled with the need for privacy within a family in which collective identity superseded personal need. All three described tensions in self-actualizing and embodying deeply held beliefs about filial responsibility across generations. Living this tension was a source of both stress and strength. The way this tension is lived is unique to racialized young women carers who can be challenged to integrate both collectivist culturally informed familial values (emanating from self and others) and individualist values of self-determination and choice prominent within the host society and youth cultures. Expressions of resulting identity negotiation (between communal and individual values) have been theorized as a reality of hybridized subjectivity (Brotman & Kraniou, 1999) common to first- and second-generation women from immigrant families who are multiply situated across cultures and communities. Still, the role of collectivist forms of familial obligation is often integral to the well-being and survival of racialized and immigrant families and communities.
The literature has reported on how family and community are protective factors in the struggle against oppression, and so collectivist values are potentially significant in the identity development of racialized youth, promoting resilience and resistance across the life course (Brown, 2008). In particular, the process of “gendered racial socialization” within families has been identified as central to supporting racialized young women’s capacity to counter interlocking forms of gender and racial oppression (Brown et al., 2017) and is important to understanding the commitment to fulfilling family care obligations as an integral aspect of identity among racialized first- and second-generation young women, despite personal challenges in doing so. In our study, participants described feeling both connected to and disconnected from their cultural and religious roots (i.e., as is the case when Shani stated both that she is not connected to Arabic culture/community at the same time as she said that she continued to enjoy participating in activities with her grandmother). For Sandra, a second-generation East Asian Canadian, participating in East Asian culture/community fulfilled a deep need for connection to both her father and the wider East Asian community, something that she feared losing once her father dies. For Nadia, as a recent migrant to Canada, and without connection to a larger West African local community, only her available local, and extended transnational, family provided her with a sense of belonging and connection to culture. At the same time, she also had ambivalent feelings about the presence of both her parents in her home because of the responsibility engendered by this, to both provide hands-on care to her father and cultural interpretation and accompaniment for her recently arrived mother. The additional support that her mother provided to care for her father did not compensate for the added pressure of being the mediator and negotiator between her family’s cultural knowledge, values, and experience with that of the host Canadian society.
Oppression, agency, (resilience), and resistance
All three women described being fiercely independent and strong-minded as a means of enacting resilience as carers. They held this discourse despite the sometimes negative impacts of care such as frustration, exhaustion, and delayed achievement of goals. Their agency, in the forms of both resilience and resistance, was evident in the fact that, despite many disruptions, financial precarity, and social isolation or disconnection, they continued their educational journeys, at least to some extent. Reducing or leaving work in order to care did not stop them from attaining some of their educational goals. This may reflect, in part, the cultural and familial values of education imparted by many immigrant parents and grandparents and internalized by young adult carers, for whom educational achievement is seen as a marker of success and a personal, familial, and community goal of migration (Fuligni & Fuligni, 2007). “Success” is, however, constrained by structural and intersectional forms of oppression (i.e., gendered, racialized, and economic experiences of othering), which limit racialized immigrant women’s opportunities to use educational achievements to improve social and economic conditions for themselves, their families and communities, especially in light of care responsibilities. This is reflected in the participants’ stories of delayed, interrupted, or reduced education or employment, as well as expressed concerns regarding their future capacity to accumulate savings, which resulted from their intersectional experiences of care within the context of immigrant family life.
Resistance to domination and control was demonstrated in several ways. This included both personal/familial forms (such as in Shani’s refusal to accept patriarchal views of marriage) and structural forms (such as in Sandra’s story of supporting her father’s resistance to microaggressions experienced in the health care system). All three spoke of important efforts to buffer the experiences of exclusion faced by their care recipients as a result of migration. All three noted how structural constraints related to access to care for migrants, including temporary and permanent migration categories, persist across time and place. Nadia’s accounts of how financial and health precarity, as a result of her father’s temporary migrant status in Canada, impacted his ability to receive adequate, appropriate, and affordable care. Sandra spoke to how racist discrimination in the forms of erasure and invisibility is made manifest for immigrants regardless of the length of time in the host country. All three participants spoke about how social isolation and a deep sense of a lack of belonging based on the intersections of cultural, racialized, language, and citizenship status permeated through time and context.
Conclusion and Recommendations for Change
A feminist-informed intersectional life-course interpretation of participants’ lived experiences illuminates the ways in which agency is constrained by the realities of care, including tensions between personal, familial, social, and structural values and forces, as well as the ways in which agency is enacted through resilience and resistance strategies on the part of first- and second-generation racialized young women. There are many lessons for social work intervention and service delivery across sectors in these stories of resilience and resistance. First and foremost, it is important to reiterate previous research in stating that inadequate attention has been placed on the particular realities and experiences of young adult carers across the health and social services network (Leu et al., 2018), and on gender, racialization, and migration as dimensions of this care (Mintzer et al., 1992; Pharr et al., 2014). Given the minimal policy and programmatic attention to the impact of structural oppression on carers’ lived experiences and capacity to care, it is no surprise that the intersection of identities and social locations (i.e., gender, race, class, and citizenship) is largely absent from the design and delivery of carer services (Calasanti, 2009). Given the experience of social isolation and disconnection among both young racialized first- and second-generation women carers and their care recipients within broader social networks, as well as within education, employment, and health sectors, this lack of attention contributes to unique forms of social exclusion. Adapting existing support services as well as addressing intersectional discrimination within the health and social care system is necessary. Examples raised by all participants include the need for culturally safe 4 support, trust building for themselves and care recipients within health and social care services, elimination of microaggressions, and the removal of barriers within migration regulations in order to support full and equal access to services and financial support, particularly during health care crises. Only with culturally safe, relevant options young adult racialized first- and second-generation women carers will be able to maintain physical and mental well-being, engage more satisfying social networks, and actualize their identities and values in life and within reciprocal relations of care.
Footnotes
Authors’ Note
This project adhered to Canadian Tri-Council guidelines and obtained ethics approval from the University of Ottawa and McGill University. All names used in the article have been changed to pseudonyms, and geographical locations generalized, for the purposes of ensuring anonymity and confidentiality.
Acknowledgments
Thank-you to the research participants who shared their stories with us. We would also like to acknowledge Michelle Lawee, research assistant, for her earlier work which contributed to the development of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This project was funded through an Insight Development Grant from the Social Sciences and Humanities Research Council of Canada (Project #430-2016-00003).