
Abstract
The social and health care needs of transgender people is a growing focus within social work literature. Attention to social and physical health disparities suggests that transgender-affirming services are an often unmet need. As ways to improve services are explored, attention must be paid to the diverse identities of transgender people. Although a large number of transgender people identify as nonbinary, the majority of research has examined the experiences of transgender men and women, thus often overlooking the unique experiences of those whose gender is outside of a dichotomous binary. A stronger understanding of the experiences of people who identify as nonbinary is essential for advancing affirming social work policies and practices. This photovoice study examined identity support and stigma faced by nonbinary young adults. Participants identified several themes related to seeking care from service providers and described the presence of assumptions contributing to their identities being pathologized. Findings show that nonbinary young people, like their binary transgender peers, experience discrimination in their interactions with providers and society more generally. However, the binaristic assumptions that are described add an important dimension to existing literature. Overall, the findings call for an increasingly queer understanding of gender among social work scholarship and practice.
Keywords
For nonbinary people, gender is experienced as not only different from their assigned sex at birth (like other transgender people) but also as outside the dichotomous male/female binary altogether. Nonbinary people experience and express their genders in many diverse ways but share a sense of understanding their gender as not exclusively or stagnantly categorized by male and female distinctions (Richards et al., 2016). Although there has been an increase in social science literature focusing on transgender populations, much of these works have explored the experiences of transgender men and women, while very few have focused specifically on nonbinary people (Matsuno & Budge, 2017). Yet, as the field of social work advances to best meet the needs of queer and transgender communities, it is necessary for practitioners, researchers, and educators to recognize the diversity of transgender identities and to seek to further understand gender-based experiences as well as the related social service needs of those who are nonbinary.
This article was coauthored by three scholars at different stages of our careers, one of whom (P.R.) also drew from their lived experience as a nonbinary young adult. In this article, we describe a critical feminist arts-based participatory action research (PAR) study that utilized photovoice with a group of nine nonbinary young adults. Group members reported perceived barriers to health and human services including pathologizing attitudes, identity bifurcation, and gender-based assumptions. Findings highlight the ways in which social work scholars and practitioners can work toward a greater understanding and affirmation of gender diversity while improving the delivery of services. In addition to practice and policy implications, we discuss research implications and consider opportunities for future research with nonbinary young people as well as the benefits to the use of arts-based inquiry and PAR.
Background
Among the growing body of literature focusing on transgender health and wellness are several themes suggesting the pervasiveness of stigma, discrimination, and resultant negative social and health outcomes. Transgender people report facing high rates of gender-based harassment and violence occurring pervasively across social settings and environments. Such violence ranges from verbal harassment to physical and sexual assault, with family members, intimate partners, and strangers as the perpetrators. (Bradford et al., 2013; James et al., 2016; Kenagy, 2005).
Recent literature notes that transgender people experience housing, employment, and economic disparities that present vulnerabilities, additional risks, and inequalities (James et al., 2016). Economic inequality is a leading cause of health disparities (Woolf & Braveman, 2011), and many transgender people report being uninsured or underinsured (James et al., 2016). This, coupled with transphobia and discrimination, results in hostile treatment environments and makes health care exceedingly inaccessible (Bradford et al., 2013; James et al., 2016; Kenagy, 2005).
Unfortunately, similar barriers to service manifest when transgender people pursue mental health care. Individuals report that cost, a lack of provider competency, and transphobic experiences have prevented them from accessing care (James et al., 2016). Given increased rates of mental health needs reported by transgender people as a result of harassment and discrimination, these findings raise significant concern (Clements-Nolle et al., 2006; Grant et al., 2011; Kenagy, 2005; Tebbe & Moradi, 2016).
According to the 2015 U.S. Transgender Survey, approximately 35% of transgender people report identifying as nonbinary (James et al., 2016) yet are often excluded from consideration compared to transgender men and women. Among existing literature focused on nonbinary people, there is evidence suggesting that nonbinary people might face higher rates of discrimination than their binary transgender peers (Budge et al., 2014; Harrison et al., 2012; James et al., 2016). Scholars have emphasized nonbinary experiences of microaggressions, including the intentional and unintentional use of disaffirming gender-based language, as well as institutional discrimination evidenced by exclusively binary physical spaces such as bathrooms (Furman, 2017). Further, nonbinary people may face feelings of separation compounded by erasure from within lesbian, gay, bisexual, and transgender (LGBT) communities, as well as specifically from binary transgender peers (Budge et al., 2014; Losty & O’Connor, 2017; Rankin & Beemyn, 2012). Given the prevalence of discrimination, it is not surprising that nonbinary people also report rates of anxiety and depression greater than that of the general population (Budge et al., 2014).
Research has focused on how the impacts of discrimination can be moderated by social supports (Budge et al., 2014) and the ways in which access to and the use of diverse and affirming gendered language can support nonbinary people’s understanding and communication of their identities (Harrison et al., 2012; Saltzburg & Davis, 2010). For many, a binary or nonbinary transgender identity can be linked to a sense of resiliency, expressive freedom, and connectedness to social activism and queer/transgender community (Riggle et al., 2011; Shelton et al., 2017).
In this study, we advance previous research in partnership with a group of nonbinary young adults. We used PAR to center the voices of nonbinary young adults as they examined experiences of identity support and stigma. Collectively, the group identified the following research questions: (1) What do others need to know about being nonbinary? (2) How is my gender identity supported? (3) How is my gender identity not supported? (4) How can support for nonbinary people be improved? At the start of the group’s six meetings, the roles and project responsibilities of the principal investigator (PI; first author), research assistant (third author), and the group members were discussed. It was agreed that we, the PI and research assistant, would function as group meeting facilitators and the group members would serve as both the primary sources and analysts of the photographic data. The group agreed that having us facilitate group meetings provided space for participant coresearchers to be focused on engaging with one another, sharing data, and analyzing their experiences.
As the young adults involved in this study engaged in a reflective process of data collection and analysis, they identified salient experiences across the domains of social connectedness, family relationships, educational environments, and access and utilization of health and human services. Although numerous themes were identified, this article focuses on improving access to health and human services.
Method
Just as there are many feminisms, there are varying approaches to feminist research. Research is often labeled as “feminist” when it is grounded in feminist theories, addresses issues related to gender, and critically examines power and praxis (Gringeri et al., 2010). Methodologically, feminist research frequently engages in data collection and analysis activities that challenge the power dynamics between study participants and researchers (Devault, 1999). Our inquiry was grounded in critical feminist theory, which posits that it is not enough to advance women’s equality within social structures that perpetuate other forms of marginalization. Rather, critical feminism moves toward a deconstruction of the very social systems within which oppression is embedded (Wildman, 2007). This theoretical orientation grounded the study, informing the selection of research questions and our partnership with the participant coresearchers.
We chose PAR as a method well suited to our critical feminist approach, in part because of PAR’s emphasis on social change and power-sharing (see Capous-Desyllas & Bromfield, 2018; Mountz, 2016; Singh et al., 2013). Based upon the assumption that those directly impacted by an issue are best equipped to understand it, PAR engages those who might typically be positioned as “subjects” instead as coresearchers (Kemmis & McTaggart, 2005). Mountz (2016) has noted that participant and community-engaged methodologies are appropriate for feminist-based inquiry due to their ability to “…uncover subjugated knowledge and illuminate relatively unexplored phenomena” (p. 289).
Given our relationship to the field of social work (the first author is a social work educator and service provider, the third is a social work student, and the second is an educator in an allied field), we are drawn to PAR’s alignment with the field’s professional values, its commitment to justice, social transformation, and the prioritization of local knowledge (Altpeter et al., 1999; Cosgrove et al., 2020). Furthermore, the community-focused nature of PAR presents opportunities for social work to move away from medical models of practice while centering the profession’s commitment to research and practice being mutually informed by one another.
Previous researchers have utilized participant-driven and action-oriented methodological approaches with lesbian, gay, bisexual, transgender, and queer (LGBTQ) communities, including work focused on the experiences of LGBTQ former foster youth (Capous-Desyllas & Mountz, 2019; Mountz et al., 2018) and to conduct a community wellness assessment with transgender individuals (Hill, 2016). Scholars are increasingly recognizing the importance of these methods for work with transgender communities, given that research is frequently used in ways that exploit, pathologize, or misrepresent their identities, experiences, and needs (Furman, 2017, Singh et al., 2013). When done effectively, PAR and community-based participatory research (CBPR) operate in such a way that transgender community members identify research questions, engage in scientific inquiry, and disseminate findings in ways that are socially beneficial and reflective of the community’s needs and priorities.
Researchers conducting PAR and CBPR use a variety of methods that span from quantitative techniques to qualitative and mixed methods. Increasingly, arts-based methods have been used to reflect the experiences of those who may not be accurately represented through traditional data collection approaches (Knowles & Cole, 2008) or who may have difficulty expressing ideas through words due to varying degrees of literacy. One specific method is the use of photovoice. Developed by Wang and Burris (1997), photovoice blends photography and Freire’s (1970) approach to critical dialogue. Photovoice methodology positions study participants as coresearchers who photographically document lived experiences related to research questions. Participant coresearchers engage in individual analysis of their work and offer narrative context for their images as they share them with the larger research group. The photographs and their supporting narratives become the focus of group-based analysis, and the group collectively identifies salient themes related to their research questions. The photographs and the study’s findings are then shared with community stakeholders to inform policy and promote community change (Wang & Burris, 1997). To complement the photovoice process, we also used interpretive phenomenological analysis (IPA) to link salient themes to existing literature, as we elaborate below.
Photovoice is well suited for work with communities that experience marginalization, as the research process offers opportunities for empowerment while placing value on local and emic knowledge. The images developed in a photovoice study serve both as research data and visual representations of a study’s findings. In doing so, they offer a lens through which one can see often hidden or unexamined perspectives and bring attention to the concerns of marginalized community members.
Situating the Authors Within the Research
Recognizing the role of relationships and positionality within all phases of the research process, we have reflected upon our own identities below. Likewise, the authors directly involved in the photovoice group meetings discussed our identities with the group members.
The first author, Darren, is a social work practitioner and scholar for whom this study served as his dissertation research. Darren is a white, cisgender queer man who has spent nearly two decades engaged in work with queer and transgender young people as a social work clinician, educator, and community organizer. The second author, Christine, is a white, cisgender, heterosexual woman serving as a dissertation committee member on this research project and technical expert throughout data collection and analysis. She previously utilized the photovoice methodology with youth and is a maternal and child health researcher with expertise in Positive Youth Development and youth engagement in research. The third author, Parker, reviewed this article for accuracy in the presentation of findings. Parker is a white, queer, nonbinary young adult who worked with Darren to facilitate the photovoice meetings and analyze the data. Parker is a social work student whose personal and professional experience facilitated a strong connection with the project and the participant coresearchers.
Sampling and Participants
The photovoice group of nine nonbinary young adults from New York State’s Capital Region met 7 times from September to December 2018. Participants used meetings to develop research questions, collect data, participate in group-based data analysis, and share findings with key stakeholders. We recruited participant co-researchers after obtaining approval from the University at Albany institutional review board (IRB). In order to be eligible to join the research group, individuals were required to self-identify as nonbinary, be between the ages of 18 and 25, and be able to attend scheduled group meetings. Through the distribution of flyers and recruitment through LGBTQ social media groups, purposeful sampling methods were used to develop the membership of the photovoice group. All group members were given a US$25.00 gift card for each meeting they attended. Table 1 provides an overview of the group’s composition.
Participant Coresearcher Demographic Characteristics.
During the first photovoice meeting, the group spent time discussing photovoice ethics as described by Wang and Redwood-Jones (2001) and guidelines set forth by the IRB. Central to these ethical considerations were issues related to group and project processes, as well as the development and representation of photographic images.
As a PAR project, the group was committed to community-based action and recognized that there would be opportunities for group members to publicly disclose their participation in the study. To address this and not disclose the identity of group members who wished to remain anonymous, participant coresearchers signed multiple consent forms. One consent form provided permission for their images and other data to be shared, as long as personally identifying information was removed. An additional form was made available to group members documenting their permission for their identity to be known at voluntary events or activities they chose to participate in. The group agreed to not include other people in their photographs and thus, additional consent forms were not required.
Data Collection
The participant coresearchers’ photographs and their narrative descriptions of the images served as the study’s primary data. Individual group members analyzed their own work before sharing images and narratives with others for group analysis. Additionally, audio recordings of meetings served as additional data that we analyzed following the conclusion of group meetings.
Data collection began at the first meeting when group members engaged in a journaling exercise where they reflected on the key issues and topics they felt others needed to know about their nonbinary experiences. These reflections informed continued discussions resulting in the group reaching consensus about the research questions they would use to guide their photography. These questions included (1) What do others need to know about being nonbinary? (2) How is my gender identity supported? (3) How is my gender identity not supported? (4) How can support for nonbinary people be improved?
The group took photographs that represented their responses to each of their questions. Reflecting on their photographs, coresearchers were asked to provide context for their images and completed a “SHOWeD” analysis worksheet. The “SHOWeD” technique, developed by Wang (1999), asks participant coresearchers to reflect upon images by addressing five key questions (abbreviated by acronym “SHOWeD”): “What do you
Data Analysis
Data analysis was comprised of two phases. The first phase engaged a group-based analysis that is common in photovoice studies (Wang & Redwood-Jones , 2001; Wang, 1999). During the second phase, we engaged in an IPA of all collected data. Both of these phases of analysis are described below.
Phase 1
Participant researchers displayed their images along with their corresponding SHOWeD worksheets on the walls of the meeting room and participated in a “gallery walk” during which they viewed one another’s images and wrote reflective responses to what they saw. Following this viewing, participant researchers gathered for a facilitated discussion. This discussion explored what the group interpreted as key points from their work. The group identified commonalities across the data and began to note how these emerging themes could be used to articulate a response to each of their questions.
We reviewed group notes and audio recordings from the analysis meetings and presented a summary of key findings identified by the participant researchers to the group for approval. These findings, along with the group’s artwork, were presented at an exhibit held at a local university that offered free event space. Five of the nine group members curated and hosted the exhibit, during which time they discussed their findings with the guests. During the exhibit, the group displayed photographs and their individual SHOWeD analysis worksheets. Photographs containing images of group members who did not consent to being publicly identified as part of the study were omitted from the exhibit, resulting in a total of 30 images being displayed. Photographs and their corresponding materials were organized by the research question, and each section of images concluded with a written summary of the group’s key findings.
Community advocates and professionals, including all authors, attended the exhibit. Attendees included social workers, representatives of LGBTQ-serving organizations, public health professionals, and educators. The photovoice group members selected these attendees because of their perceived ability to apply the group’s findings to practice. Upon arrival, guests signed in and were greeted by a participant coresearcher who briefly explained the project. The formal portion of the exhibit began by us describing PAR and photovoice and the group members introducing themselves and offering their personal reflections about the project. Next, guests were invited to enjoy refreshments and casually walk through the space, viewing photographs and discussing them with group members.
A total of 13 guests attended the exhibit, and 10 of the attendees opted to participate in a postexhibit discussion. These 10 attendees signed informed consent forms and participated in an audio-recorded conversation with the photovoice group members (facilitated by the first and third author). Transcripts from this conversation were included in the second phase of analysis. Following the exhibit, the group met one final time to debrief to project. Group members completed anonymous feedback forms where they were asked to share the things they enjoyed most and least about the study. Table 2 provides an overview of data collection activities and Phase 1 of analysis.
Overview of Research Activities.
Phase 2
Following the completion of the photovoice group meetings and exhibit, all audio recordings were professionally transcribed. Transcriptions of the group’s meetings and the discussion with exhibit guests, as well as the SHOWeD worksheets, were uploaded to ATLAS.ti Version 1.6.0. Inclusion of the SHOWeD worksheets ensured that further analysis of photographic data, and the transcribed discussions about them remained grounded in participant coresearchers’ experiences. An IPA approach, as outlined by Smith et al. (2009), guided our coding of the data and helped to further develop the findings identified by group members. Like other forms of phenomenology, IPA seeks to understand a phenomenon of interest through inquiry into the lived experience. IPA was selected as a complementary methodology for further analysis as it, like photovoice, focuses not only on participant experiences but also on the meanings and interpretations that participants assign to such experiences. IPA adopts a curious approach to inquiry-seeking to understand a small group of participants’ perspectives (Smith et al., 2009). Further, IPA’s emphasis on participants’ unique interpretations of experience rejects the positivist idea of a singular objective truth. For these reasons, IPA was intentionally selected as a method of analysis to complement and honor PAR’s commitment to maintaining participant perspective.
The first step of this analysis involved us each reviewing the same two transcripts individually and taking detailed notes to identify possible codes (guided by the prior findings of the group). We had ongoing dialogue about possible codes and established a shared understanding of their application across data. Once code agreement was reached, we coded the remaining transcripts. Following three cycles of coding, data were organized into emergent themes and compared to those identified by participant coresearchers, ensuring group voice and perspective remained centered as nuanced phenomenological interpretations were developed.
Findings
Throughout the presentation of findings, pseudonyms are used for participant researchers. Additionally, readers will note the use of gender pronouns endorsed by the individuals being referenced. These pronouns often include the singular use of “they/them.” One group member requested the use of “she/her.”
The young adults involved in this PAR study noted several ways they felt their gender identities were stigmatized and not supported. Group members shared the ways they experienced a lack of support and at times hostility, from family and peers, in school, at work, and from within LGBTQ communities that adopted binary-centric assumptions regarding gender. A significant area in which challenges related to identity stigma occurred was related to group members’ experiences accessing health and human services. Group members described desires to pursue emotional and mental health support, as well as physical health care but avoided such services due to fear of gender-based stigma. For many, these fears were grounded in the realities of their past experiences.
Identity Bifurcation
In an effort to have their needs taken seriously, group members described how they share some parts of their identity and withhold others. Whether seeking medical or mental health care, the group noted that they felt their concerns would not be taken seriously if they were perceived as “too complex.”
Dev, a 20-year-old identifying as a disabled, Filipino and white, gender-queer pansexual, who was working toward completion of their bachelors degree, shared an image titled “Leaves” (Figure 1). Their photograph showed leaves carefully organized into two distinct groups based upon color. In sharing their photograph with the group, Dev emphasized how forced and artificial this binary organization was, given that the leaves contained many colors and naturally fell to the ground mixed together. Dev’s image was meant to show the absurdity of such a rigid social organization of gender.

Leaves-Dev.
At the exhibit, Dev displayed their “Leaves” photograph and discussed it. The photograph, the narrative accompanying it, and Dev’s description stood out to a white, cisgender female social work clinician. During the postexhibit conversation between participant coresearchers and exhibit guests, the group reflected on Dev’s image and noted that when services were accessed, providers often do not offer the nuanced space for uniqueness in identity to be expressed or understood. The aforementioned social worker noted that the loss of such uniqueness was detrimental to meaningful care. Continuing, this social worker shared that Dev’s photograph was jarring and made visible an identity bifurcating process that was otherwise invisible. The worker stated that “I really liked that the picture disrupts the idea of the taken for granted-ness [of simplifying and categorizing gender and identity] that people just float along and don’t challenge because we’re just so accustomed to it that it’s almost like invisible to us.”
Victoria, a 20-year-old group member identifying as Black who described her gender and sexuality as queer, shared her photograph of a messy bedroom and titled it “Redo” (Figure 2). Victoria shared with the group that she had attempted to receive mental health services in the past. She reported frequently feeling as though full disclosure to mental health providers of her identities as a nonbinary and queer person had and would continue to result in stigma and pathologization. Victoria’s image depicted a cluttered space that has “a lot going on.” For Victoria, this represented various aspects of her identities and the ways they are interpreted by the world. Reflecting on the image, she shared,

Redo-Victoria.
I have a lot of shit going on up here (pointing to her head) and I kinda forgot about my sexuality and my gender when I was really going through some shit because people force you to choose, do you want to deal with your gender? Do you want to deal with your sexuality? Do you want to deal with your queerness or do you want to deal with your mental health? They don’t see how those things interact and that it makes it difficult because they’re such big parts of my life. Maybe not who I am all together, but if they don’t interact, then none of them can be discussed in a meaningful manner.
Group members spent time at meetings and their photo exhibit, discussing the ways they perceived service providers to assume that their request for care was part of “attention-seeking.” Consequently, the group noted that they felt the need to share and withhold various elements of their identities and experiences in an effort to navigate relationships with providers. These perceptions were not held by group members alone. In fact, during the photo exhibit, community service providers noted this theme in the artwork and brought it up in the conversation that followed. One white transgender man working in a clinical social work practice shared, I think that’s very striking to recognize that people have overlapping identities and have to navigate that in terms of safety. “Which identity do I share? Which identity do I live and how do I show my true self when having to choose between identities?” [As providers] how do we see the whole person? It’s really important. Two years ago I became physically disabled. Suddenly that was part of my identity and I didn’t have a choice about expressing it to people and it seemed my gender had to take a back seat. It was like, I’m walking in here and they already know I’m a “cripple” so I can’t be like, I’m nonbinary too, because that’s just too many things, that’s going to be freaky for them.
Pathologizing Attitudes
The young adults in this study shared ways in which they experienced their gender being pathologized by providers. While images like Victoria’s “Redo” (Figure 2) represented challenging experiences with providers, it was the group’s analysis of the collective body of photographs that allowed this theme to emerge as one of the most salient experiences among participant coresearchers. A number of group members noted that when seeking counseling for mental health concerns, providers often directed clinical focus to their gender, suggesting that it was of more significance than (or was the driving force behind) the difficulties they were facing. Delaney, a white 21-year-old college student identifying as a physically disabled nonbinary bisexual, shared, I was 15 and in therapy for the first time and I thought it was okay to talk to my therapist about whatever so I mentioned being nonbinary, and I very clearly remember her being like, “Are you nonbinary because you don’t have any good women role models?” I was like, “First off, that’s the exact opposite of what is true for me. I am from a long lineage of trash men and the only good role models I’ve ever seen have been women. If that was how it worked, I would be very much a woman.” At the same time, it sent this message of my gender is something to be psychoanalyzed and is something that you can solve. A couple years back, I was in and out of inpatient at [local psychiatric hospital], obviously for mental health…but I couldn’t go through it as a nonbinary person. I was like, “Hi, I’m Karmen. I’m a woman.” It sucked. If you have mental health problems or are in some way perceived as “deviant,” the medical community will label you. This is a major fear that myself and a lot of other chronically ill, nonbinary people experience, it’s like, Oh, is exposing or outing myself going to make my other problems not get treated?
For many in the group, there was a perceived need to “hide” their gender from providers. This resulted in feeling as though they could not be their full selves or authentically express their gender. Such experiences created barriers to service utilization. When services were accessed, pathologizing comments and the feeling of being stigmatized contributed to a continued sense of hesitance in seeking future care.
Binary Assumptions
Much of the lack of support reported by the group was connected to pervasive binary assumptions about gender. These “binaristic” assumptions (a term used by the group) showed up throughout daily life, often in seemingly mundane ways. River, a 22-year-old identifying as Latinx and white, shared a photograph titled, “Just for Men” (Figure 3). Their image showed a box of hair dye that was strategically marketed for male-identified people. The group spent time discussing how this binarism may go unnoticed by many. They also discussed how it reinforces gender paradigms that show up elsewhere in life, including when one is accessing health and human services.
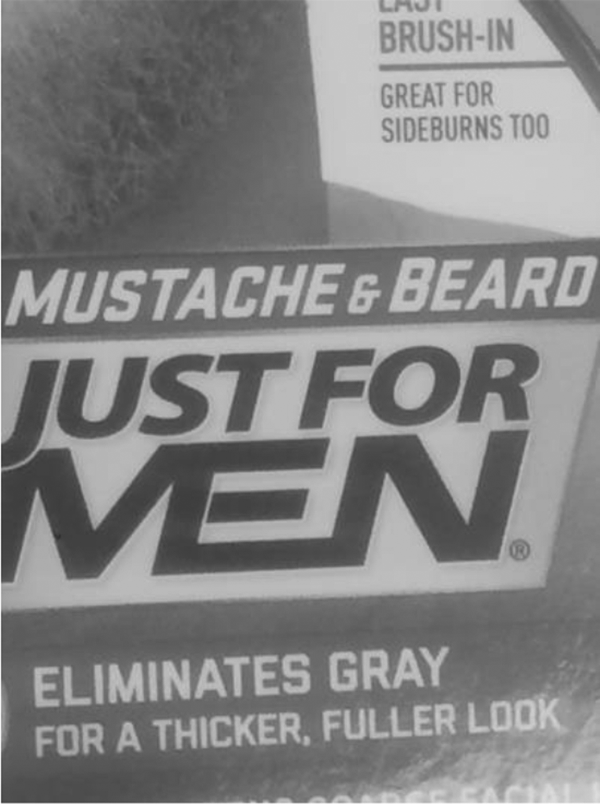
Just for Men-River.
Participant coresearchers in the group reported that they experienced binary assumptions from service providers who had a reputation for offering affirming care to other transgender clients. Two group members shared experiences they had with providers whom they perceived to be generally transgender-affirming and who offered transgender-specific services. Despite these providers’ commitment to gender affirmation, they failed to use the group members’ “they/them” pronouns and made binary assumptions communicated through the questions on intake forms, the language used during interactions, and through physical environments like bathrooms.
Group members described encountering these assumptions when they visited clinics and completed paperwork that provided exclusively binary gender options. While no group members took photographs specifically targeting the issue of paperwork, the topic often came up in discussions regarding binarism within clinical spaces, and many in the group stated they felt such paperwork was simply a manifestation of deeply entrenched assumptions. As Dev commented, “I think binaries make things easier to understand but are really harmful to those of us shoved into a box.” This harm was done when group members sought service but immediately felt rejected by the binary language found on forms or used by staff. As Delaney noted, “Simple things like using gender-neutral pronouns and not having a check box for just ‘male or female’ makes a difference. I think people notice when you use ‘they’ instead of ‘he or she,’ or at least nonbinary people notice.”
During the group’s discussion with the exhibit guests, there was a significant amount of conversation around the importance of inclusive paperwork. Some service providers felt trapped by the need for their paperwork to capture categorical and discrete identity information for state and federal reports. One white, nonbinary, and queer exhibit guest who was an administrator at a local reproductive health care center shared, “[discrete and binary categories on paperwork] are a big thing within health care. Everything needs to be a checkbox, it’s a ‘yes’ or ‘no,’ so as much as you see the binary in everyday life, in the medical field in general it is even more so.” Krissy (a white 22-year-old queer college graduate) heard this concern and empathized but felt that regardless of difficulty, changes needed to be made. Krissy shared that they had completed demographic data collection and reporting for a senior project and stated, I’m frustrated, because people have to decide do I stick to the language that I’ve always known…just have it be simple, or could I just take five more minutes to come up with another option?

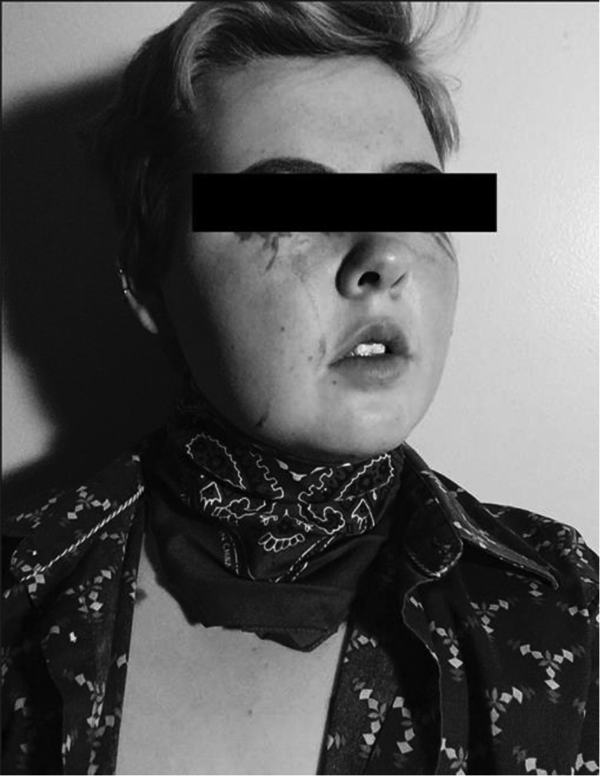
Assumptions-Karmen.
Assumptions About Nonbinary People
Group members discussed how binarism resulted in nonbinary invisibility. They noted that this was complicated by others’ assumptions about what it means to be nonbinary.
Despite a general sense of invisibility, the group felt that when others considered the experiences of nonbinary people, they often did so in a way that endorsed a very narrow view of nonbinary identity and experience. Ty, a white 20-year-old identifying as a bisexual college student, presented an untitled photograph (Figure 5). In this self-portrait, Ty intentionally blends colors and clothing to symbolically represent what being nonbinary means to them. In sharing their photograph, Ty explained that they hoped it brought attention to the problem of “people assume [ing] a non-binary gender is about androgyny and looking queer.” Ty continued by expressing that they created their image to help people realize that “not all nonbinary people are the same and that there so many ways to be nonbinary.”
Untitled-Ty.
Continuing the conversation about the invisibility of nonbinary diversity, Delaney stated, “[there are] perceptions of nonbinary people as all white, thin AFAB [assigned female at birth] and able-bodied.” For participant coresearchers who did not embody this stereotype, their gender was made even more invisible. For participant coresearchers who identified as people of color, they described navigating environments of racism, transphobia, and binarism. For some, this occurred in both “straight and cisgender” spaces, as well as those that were otherwise queer. Victoria reflected on stereotypes about nonbinary people and shared, [it’s] like that’s the only way to be queer. That’s the only way to be nonbinary and make it palatable to the outside world. I relate to that a lot because I’m not able bodied, I’m not thin, I’m not white. So, moving through queer spaces is a little bit different for me because there are a lot of things that I have to deal with. Just because you’re queer doesn’t mean you’re not racist.
The Power of Language
Although the group collectively discussed the challenges they faced as a result of assumptions communicated through language, language was also a tool of significant affirmation. Contrasting the Diagnostic and Statistical Manual’s (DSM) gender dysphoria diagnosis (which many felt was pathologizing of their gender), several group members used the term “gender euphoria” to describe the experience of joy and affirmation they felt when people used their correct names and pronouns. One group member, Delaney, shared an image titled, Sticks and Stones May Break my Bones but Language Can Affirm me (Figure 6). The photograph depicts lettered tiles from a game and the artist stated, “When inclusive language that doesn’t force me into a false binary is used, I feel instantly more at ease.” They further explained, “It is a subtle way to show nonbinary people that they will be safe and will be able to come out.” Coresearchers agreed with Delaney’s experience and reported that the use of affirming language was one of the most significant ways they felt supported. For members of the group, affirming language included the use and endorsement of the descriptive gender terms they used for themselves, use of their chosen name, and use of affirming gender pronouns.

Sticks and Stones May Break my Bones but Language Can Affirm me-Delaney.
Overall, the findings identified several significant themes related to identity affirmation and stigma as participant coresearchers pursued health and human services. Participant coresearchers shared that they pretended not to be nonbinary so that they could access care without judgment. Group members shared that, in an effort to avoid mistreatment, they needed to strategically calculate which experiences and portions of their identity they shared with their service providers. Many in the group felt they needed to take such precautions even in situations where providers are supportive and affirming of binary transgender patients’ identities. Further, some group members felt they had to navigate environments in which their racial and ethnic identities were marginalized and worried that being out as nonbinary would become “too much” for providers.
Discussion
Findings from this study build upon literature regarding transgender peoples’ experiences interacting with social service and health care systems, while also making original contributions focused specifically on nonbinary young people. As our literature review showed, it is well-documented that health care stigma and discrimination often prevents binary and nonbinary transgender people from accessing needed services, thus perpetuating health disparities (Grant et al., 2011; James et al., 2016). Our qualitative analysis underscores the pervasiveness of such stigma within health and human services, while also presenting a rich understanding of the meaning such experiences hold for nonbinary young people.
Several participant coresearchers in this study shared instances of outright discrimination, while others noted experiences of microaggressions (see Nadal, 2008). Although previous research on transgender microaggressions focuses on transgender men and women, much of what the nonbinary participant coresearchers in this study reported can be categorized within Nadal et al.’s (2012) framework, specifically within their discussion of the endorsement of gender normative and binary behaviors and the use of incorrect gender terminology (p. 64). Findings from the current study thus suggest that Nadal et al.’s (2012) categorization of transgender microaggression may be useful in understanding both binary and nonbinary experiences.
Many of the group’s reported experiences may be shared by binary transgender and nonbinary people alike. However, the findings of this study suggest that for those who are nonbinary, such experiences occur within a “binaristic” social context that renders their identity inconceivable to others. Consequently, the manifestation of gender paradigms in the form of exclusively binary intake and clinical paperwork, bathroom options, or gender segregated treatment result in no inclusive option for those who are nonbinary. For those in this study, experiences of marginalization and invisibility persisted even as binary transgender visibility increased.
Ultimately, the findings suggest that increased attention to gender-related language in both personal interactions and service-related paperwork are practical ways to enhance the affirmation of nonbinary genders. Further, this study supports the critical feminist aims of examining gender-related power structures that render some identities invisible. Bringing continued nuance to these considerations, findings encourage both social work practitioners and scholars to further problematize dominant paradigms of gender that, while increasingly inclusive of some transgender people, further perpetuate essentialist and “binaristic” notions of both cisgender and transgender identity.
Implications
This study has implications for those engaged in direct social work practice, policy, and research. In each of these areas, there are opportunities to continue advancing transgender-focused work that is affirming of both binary and nonbinary identities.
Practice and policy implications
Both binary and nonbinary transgender people report heightened rates of discrimination, stigma, and related mental distress (Budge et al., 2014; Harrison et al., 2012; James et al., 2016). Social workers must be prepared to meet both the gender-specific and the general mental health reasons a transgender client may seek their services. There is an ongoing need to critically examine the ways gender pathologization occurs within practice. One such target for critique is the nature of the DSM transgender-related diagnosis of “gender dysphoria.” While such a diagnosis may help some to access transgender-related health care services, it continues to perpetuate cisnormativity, binarism, and gender essentialism. Further, the DSM can function as a barrier to care for those who struggle to access mental health care services, or who do not wish to have their experience of gender connected to a clinical diagnosis, or who do not meet the diagnostic criteria (as is the case for some nonbinary people). Indeed, our findings support the comprehensive critique of the DSM’s previous and current transgender-related diagnoses presented by other scholars (see Burdge, 2007; Lev, 2013; Spade, 2003).
While the findings of this study certainly encourage broad systems-level changes and shifts in social gender paradigms, there are also many smaller scale local and individual-level shifts that can improve nonbinary people’s access to services. Providing inclusive gender options on client paperwork, inclusive bathroom options, and adopting the practice of sharing one’s own and asking about others’ gender pronouns, are all ways to make relatively small changes that can have a significant impact on clients’ experiences. Smaller scale changes can provide an opportunity for nonbinary genders to become increasingly visible. Such visibility can have a positive impact on individuals’ sense of affirmation while also contributing to a shift in social gender paradigms.
Research implications
Beyond practice and policy implications, this study raises important questions about who is and is not represented in the growing body of transgender-focused literature. The way a researcher operationalizes what it means to be transgender inherently sets imperfect inclusion and exclusion criteria within a study. Likewise, the recruitment language one uses may attract or deter various potential participants. Consequently, it is likely that many nonbinary people are participating in research studies, while having their unique identities and voices misrepresented as those of transgender men and women.
As this study shows, arts-based inquiry and PAR are well positioned to address the limitations of previous research. Arts-based research is appropriate for engaging with communities that may be underrepresented (Knowles & Cole, 2008), and arts-based approaches have been successfully utilized in collaborative studies with transgender people (Furman, 2017; Hill, 2016). The continued use of methods that promote reflective explorations of gender may be beneficial in efforts designed to further explore participants’ experiences while providing opportunities to understand gender diversity without being hindered by paradigmatic bias.
Like other PAR with queer and transgender people (Capous-Desyllas & Mountz, 2019; Furman, 2017; Hill, 2016; S. Mountz et al., 2018), this study echoes the argument that participant-driven methodologies produce results that can positively impact participants, as well as their broader social environments. Specifically, the collaborative nature of this study cultivated a sense of trust and rapport among group members. As the group meetings ended, six of the participant coresearchers indicated they would not have shared as much had they not been working within a PAR group comprised of other nonbinary people. These group members expressed a sense of feeling as though they were able to authentically contribute to and influence the project’s direction and, as one such individual shared, “[other approaches to research] call for impersonal answers. We are wanted as sources of information, but it’s very rare to be able to get personal about it.”
The study also exposed important gaps in existing literature warranting future investigation. Additional research is needed to further explore the intersection of nonbinary people’s gender and other identities (race, ethnicity, class, etc.). Such inquiries could further explore what this study noted as identity bifurcation. There is also a need for research that examines nonbinary young people’s development of support systems and their navigation of identity within social environments that lack gender-inclusive representations.
Limitations
There are a number of limitations to this study. First, its methodological design was dependent upon both arts-based and group-based work. As such, those not represented by this sample may include those who may not have been interested in such approaches, or who were uncomfortable being “out” to others, or who faced social isolation that prevented them from being engaged in the networks through which recruitment occurred. Secondly, the majority of the participants who made up the photovoice group identified as white. Given the heightened rates of stigma, harassment, and physical violence faced by transgender people of color (James et al., 2016), future research should look specifically at the experiences of nonbinary people of color. A third limitation is that additional contextual data were not collected from group members. For example, while most group members reported past or present college enrollment, there was no systematic collection of data related to degree status, work experience, and so on. The lack of these details limits the ability to fully contextualize data and findings. Lastly, while we argue that photovoice and IPA are methodologically well aligned, the IPA phase of data analysis may be seen as a departure from the study’s overall PAR focus. This limitation is further noted as the analysis was conducted once group meetings concluded.
Despite limitations, this study draws from rich and diverse forms of data that help address the unique experiences of those in the group. The study’s innovative design produced trustworthy findings and offered a meaningful experience for those it engaged. Findings also lay the groundwork for continued scientific inquiry and improved practice related to service provision to nonbinary young adults.
Conclusion
Nonbinary young adults, like their binary transgender peers, face discrimination and harassment. While such experiences suggest a heightened need for access to health and human services, the participants in this study reported that service providers often contributed to feelings of stigma and rejection. The nonbinary young adults in this study described unwelcoming and unsafe interactions with the service providers whom they reached out to for support. These interactions were characterized by problematic gender-based assumptions, identity pathologization, and barriers to identity disclosure, even from those providers known to be supportive of transgender people. As we argue, simple steps can be taken to increase providers’ capacity to meet the needs of nonbinary young adults in affirming ways. Attention to inclusive paperwork, inclusive physical spaces, and critical attention to personal beliefs about gender can serve to reduce barriers to care and may promote service access and utilization.
Ultimately, this study calls for an increasingly queer understanding of gender. Such a shift in paradigmatic thinking is beneficial to the field of social work, as its absence promotes the reinforcement of essentialist understandings of human identity. Continued efforts to advance transgender inclusion must include a deepening in our understanding of not only transgender men and women but also of those whose identities fall outside the binary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University at Albany’s School of Social Welfare, William J. Reid Doctoral Student Dissertation Scholarship Award.