
Abstract
Disasters, both natural and human-caused, can generate significant stressors for individuals, families, and communities, and research has documented an increase in the prevalence and severity of violence against women following these events. This article reviews research documenting the prevalence and severity of violence against women in disaster settings and provides a framework for intimate partner violence professionals to cultivate resources and capacities that promote women’s safety and well-being before, during, and after a disaster. Framework objectives include increasing awareness and capacity to respond, promoting safety planning, ensuring basic needs are met, providing comfort and support, connecting to long-term services, and promoting psychosocial recovery.
Between 2005 and 2015, approximately 1.7 billion people have been affected by disasters worldwide, resulting in $1.4 trillion damages and 7 million deaths (United Nations Office for Disaster Risk Reduction, 2016). Disasters include natural (e.g., hurricane, tornado, earthquake) or human-caused events (e.g., chemical spill, mass shooting) that affect individuals, families, and communities. Disasters may cause significant emotional trauma and stress, can injure or kill individuals, may disrupt social support systems, and can threaten basic human needs such as access to food, water, and housing (Becker-Blease, Turner, & Finkelhor, 2010). Between 2010 and 2015, there were 720 U.S. disaster declarations in which a state or tribal government requested and received federal aid due to the severity and magnitude of the event (Federal Emergency Management Agency [FEMA], 2016a).
While disasters can broadly affect a community, they do not affect all community members equally. In the disaster literature, the term “social vulnerability” refers to various social attributes and conditions (e.g., poverty, age, race, ethnicity, health, and gender) that place human populations at increased risk for negative or adverse consequences resulting from a disaster (Cutter, Boruff, & Shirley, 2003; Tierney, 2014). With regard to social vulnerabilities, feminist scholars and sociologists have highlighted the ways in which women are more vulnerable to negative impacts of disasters than are men, primarily due to social and structural inequalities (Enarson, 2012; Fothergill, 1999). Enarson (2012) points out that women have higher rates of poverty than men, which often exposes women to living in high-risk residences (e.g., trailer homes), living near neighborhood contaminants (e.g., living near hazardous facilities and in low-income communities), and having inadequate access to proper nutrition and health care. Each of these factors may increase the severity of women’s disaster experiences and may reduce the access to resources needed for disaster recovery. In addition, women’s roles as primary family caregivers may expose them to increased disaster harm as they strive to protect others during and after the event (Fothergill, 1999). Disaster studies also indicate that racial and ethnic minority women, in particular, face more challenges and have less access to services and resources in disaster settings, due to social inequalities such as institutional and interpersonal racism language barriers and distrust of governmental authorities (Bolin, 2006; Peek & Fothergill, 2008; Pulido, 2000). For example, Peek and Fothergill (2008) found that following Hurricane Katrina, low-income, female, African American survivors faced more recovery challenges, were more likely to be displaced to unfamiliar places, and have fewer post-disaster resources.
Additional studies examining social vulnerability also report that rates of emotional and physical violence against women increase in the aftermath of disasters (Enarson, Fothergill, & Peek, 2006). Intimate partner violence (IPV) includes “assaultive and coercive behaviors” by a perpetrator to control a current or former intimate partner (Tjaden & Thoennes, 2000, p. 5). Research indicates that the prevalence and severity of IPV can have a compounding effect on a woman’s post-disaster mental health and recovery (Anastario, Larrance, & Lawry, 2008; Buttell & Carney, 2009; Enarson, 1999; Harville, Taylor, Tesfai, Xu, & Buekens, 2011; Lauve-Moon & Ferreira, 2016; Schumacher et al., 2010). Writing on the 2-year anniversaries of Hurricanes Katrina and Rita, Ross-Sheriff (2007, p. 7) challenged feminists, social workers, and other helping professionals to focus on improving IPV services for women after disaster: Women and girls will continue to be victims of violence after disasters…we must take steps to make girls and women safer…We must focus on direct services, during and after disasters, that are gender effective. We must act to develop emergency preparedness responses and recovery policies that are gender aware. We must learn to recognize and affirm their strengths.
Violence Against Women and Disasters
A growing number of studies have documented an increase in the severity and prevalence of IPV in post-disaster contexts (Anastario et al., 2008; Buttell & Carney, 2009; Enarson, 1999; Harville et al., 2011; Lauve-Moon & Ferreira, 2016; Schumacher et al., 2010). For example, among 77 domestic violence centers surveyed in Canada and the United States (Enarson, 1999), the centers most significantly affected by disasters reported higher service demand up to 1 year after the events. Communities have reported as much as a 50% increase in police reports of domestic violence after a disaster (Norris, 2014). Following the Red River Flood in Grand Forks, North Dakota, domestic violence providers reported an increase in IPV cases and in requests for IPV services (Enarson & Scanlon, 1999; Fothergill, 1999). Several studies also show an increase in IPV rates and severity in communities affected by Hurricane Katrina in 2005 (Anastario et al., 2008; Buttell & Carney, 2009; Harville et al., 2011). Schumacher and colleagues (2010) surveyed 445 married or cohabiting persons who were living in the 23 southernmost counties of Mississippi at the time of Hurricane Katrina and found that the proportion of women reporting psychological victimization increased from 33.6% to 45.2% 6 months after Hurricane Katrina. Additionally, reports of physical victimization nearly doubled from 4.2% to 8.3% (Schumacher et al., 2010). Anastario, Larrance, and Lawry (2008) assessed changes in IPV rates after Hurricane Katrina among internally displaced people living in FEMA trailer parks in Mississippi from 2006 to 2007. They found the rate of IPV increased following the hurricane from 12.5% in 2006 to 34.4% in 2007 (Anastario et al., 2008).
Several explanations have been suggested for why IPV rates increase in disaster-affected communities. For instance, disasters may affect changes in intimate partner relationships through reduced marital satisfaction (Banford, Wickrama, Brown, & Ketring, 2011), increased aggressive methods of conflict resolution (Harville et al., 2011), or strained communication between intimate partners (Lowe, Rhodes, & Scoglio, 2012). Others have noted the increases in post-disaster stressors such as housing and financial disruptions (Sety, 2012) and unemployment (Lowe et al., 2012) often contribute to increased rates of IPV (Enarson, 1999; Frasier et al., 2004; Houghton, 2009).
Furthermore, studies indicate that disasters may affect not only the prevalence of but also the severity of IPV and its effects (Enarson, 1999; Lauve-Moon & Ferreira, 2016; Schumacher et al., 2010; Sety, 2012). Disasters may exacerbate the effects of ongoing abuse by disrupting access to important supports such as social and family systems that might offer practical and psychological assistance to IPV victims (Sety, 2012). Following the Deepwater Horizon oil spill, Lauve-Moon and Ferreira (2016) found that women directly impacted by the event were approximately twice as likely to experience both physical and emotional IPV and women who experienced both emotional and physical IPV were 5 times more likely to report that they rarely or never received the social and emotional support they needed post-disaster. Moreover, women experiencing IPV post-disaster often encounter muted responses from social service providers, who themselves may be overwhelmed by “increased demand with reduced capacity” as a result of the disaster (Sety, 2012, p. 4). Enarson (1999), for instance, found that domestic violence centers in Canada and the United States that were affected by disasters reported higher service demand for up to 1 year after the events.
In fact, depending on the nature and severity of the disaster, IPV service infrastructure—such as domestic violence shelters and social service organizations—may have reduced capacity including disrupted communication networks and referral pathways (Jenkins & Phillips, 2008) or damaged or destroyed buildings (Sety, 2012). Similar strains are often placed on law enforcement, criminal justice, and health services that might otherwise respond to—or ideally prevent—IPV (Jenkins & Phillips, 2008). These disruptions may impede not only IPV services but also IPV reporting, communication, counseling, protection, and referral (Enarson, 1999; Jenkins & Phillips, 2008; Sety, 2012). Furthermore, disaster responders and providers may not be adequately equipped or trained to provide IPV-related services to women (Enarson, 2012; Jenkins & Phillips, 2008; Parkinson & Zara, 2013).
Finally, studies indicate that IPV may have a compounding effect on a woman’s post-disaster mental health and recovery. In the aftermath of Hurricane Floyd, for example, women who experienced IPV were more likely to report perceived stress, psychological distress, somatic complaints, and post-traumatic stress disorder (PTSD) symptoms (Frasier et al., 2004). Schumacher and colleagues (2010) reported that IPV reports were associated with a greater risk of post-Katrina depression and PTSD among women. Likewise, Anastario and colleagues (2008) found that women who reported post-Katrina IPV were approximately 10 times more likely to report symptoms of depression than women not experiencing post-disaster IPV. Similarly, Mechanic, Weaver, and Resick (2008) reported that 39% of women who experienced postflood IPV developed PTSD compared to 17% of women who did not experience abuse. Moreover, 57% of women who experienced postflood IPV developed major depression compared to 28% of nonabused women (Mechanic, Weaver, & Resick, 2008).
In summary, multiple studies offer evidence that women experience increased rates of IPV after a disaster and that IPV can have compounding effects on women’s mental health and post-disaster recovery. This suggests that IPV services should be integrated into disaster-related assistance and services. In the following section, we provide an overview of the theories of community resilience and empowerment and how they inform our IPV and Disaster Framework. This framework is designed to integrate services and resources that address violence against women across the phases of a disaster (i.e., before, during, and after disaster).
Theoretical Framework
The theoretical models of community resilience and empowerment provide an ideal lens for guiding efforts to promote resources and well-being for women experiencing IPV in disaster contexts. Resilience has many definitions but is generally defined as a process of adaptation and recovery from adversity or a traumatic event (Masten & Obradović, 2008). When applied in the context of a community disaster, Norris, Stevens, Pfefferbaum, Wyche, and Pfefferbaum (2008, p. 127) describe four main “adaptive capacities” that facilitate community recovery after a crisis or disaster. Within this model, the four adaptive capacities include economic development, social capital, information and communication, and community competence. Each adaptive capacity includes several components and dimensions. For example, economic development includes components of fairness of risk and vulnerability to hazards and equity of resource distribution, while community competence includes dimensions of community action, political partnerships, and collective efficacy and empowerment. A primary concern highlighted in this model is attending to social vulnerability (e.g., race, ethnicity, age, IPV victims) and generating a variety of necessary resources within communities experiencing crisis or disaster (e.g., housing, employment, social support, medical care). Thus, resilience of a community depends upon capacities and resources being made available to all community members through programs and services that seek to promote mitigation, preparedness, response, and recovery in the event of a disaster (Norris, Stevens, Pfefferbaum, Wyche, & Pfefferbaum, 2008).
In connection with the theoretical principles and components of community resilience following disaster, we identified the process of empowerment in the area of IPV as an important guide for constructing our IPV and Disaster Framework. The empowerment of victims of IPV has long been considered the core model for services in the field of IPV (Cattaneo & Chapman, 2010). While there are various definitions of empowerment, generally the IPV literature focuses on cultivating a process in which a person who lacks power sets personal goals to gain power and control over their lives by accessing and developing skills, community resources and supports, and self-efficacy (Cattaneo & Chapman, 2010). Essentially, an empowerment perspective places an emphasis on overcoming oppression through constructing consciousness-raising and cultivating resources and capacities for women experiencing IPV (Danis & Bhandari, 2010). According to Lum (1996) and Bush and Valentine (2000), IPV professionals utilize a variety of strategies to empower women experiencing IPV through the practice of support and advocacy. These empowerment strategies include educating professionals in various systems about barriers and difficulties faced by women experiencing IPV, identifying and recognizing the strengths of women, obtaining additional resources for women so that they can achieve independence, and building connections between women with shared histories (Bush & Valentine, 2000; Lum, 1996).
IPV and Disaster Framework
Building upon the principles and components of community resilience and empowerment (Busch & Valentine, 2000; Lum, 1996; Norris et al., 2008) along with disaster and IPV research (Enarson, 1999; Jenkins & Phillips, 2008; Parkinson & Zara, 2013; Schumacher et al., 2010), we provide a framework for professionals working in IPV shelters and coalitions (e.g., social workers, counselors, advocates) to promote women’s safety and wellness in each disaster phase. Emergency management often conceptualizes disasters in four phases (e.g., mitigation, preparedness, response, recovery), and we utilize this perspective to identify IPV and disaster objectives and strategies for use before, during, and after a disaster (FEMA, 2016b). The following sections provide an overview of the framework and the objectives included in each phase (e.g., promote stabilization and safety), and suggested strategies for accomplishing objectives are also provided (e.g., assist in creating disaster safety plans). See Table 1 for a summary of all objectives and strategies.
Intimate Partner Violence and Disaster Framework.
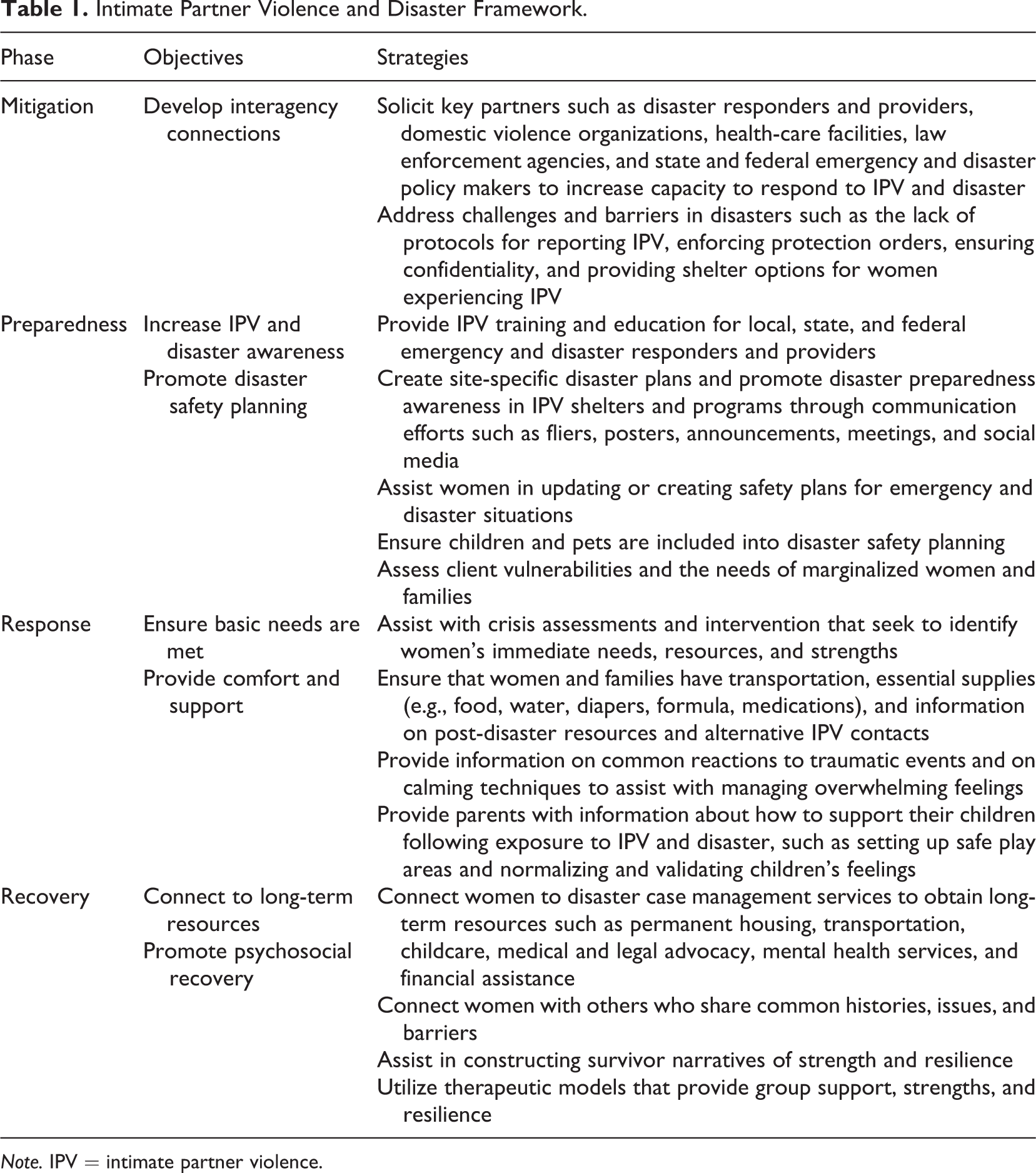
Note. IPV = intimate partner violence.
IPV and Disaster Mitigation
The disaster mitigation phase involves participating in activities that identify risks and hazards to reduce or eliminate the impact of a disaster incident (FEMA, 2016b). Correspondingly, efforts can be made to mitigate women’s risk of IPV and reduce or eliminate IPV-related challenges and barriers experienced by women in disaster settings. From a mitigation perspective, IPV professionals can promote empowerment for women experiencing IPV by developing community connections to increase capacity to respond to IPV and disaster.
Develop connections to increase capacity to respond to IPV and disaster
The first strategy is to develop connections with community organizations and systems that are active in responding to a disaster. IPV professionals can solicit support and collaboration from local, state, and federal disaster responders and providers, health-care facilities, law enforcement agencies, and domestic violence organizations. Developing connections before a disaster is important because it provides time to create trust and understanding between organizations ahead of an emergency. Organizational connections can ultimately facilitate IPV and disaster-related information dissemination (Stephens, Rimal, & Flora, 2004) and may facilitate better response if a disaster occurs.
As connections among organizations are formed, IPV professionals can advocate for an IPV focus within the disaster response system. This includes developing protocols for reporting IPV, fostering awareness of the importance of enforcing IPV protection orders, ensuring IPV victim confidentiality, and providing safe shelter options for women experiencing IPV (Enarson, 1999; Jenkins & Phillips, 2008; Parkinson & Zara, 2013). Developing an IPV focus within the disaster response system provides opportunities for community organizations to identify and tailor gaps in services that their agencies may be able to address to improve the safety and well-being of women in disaster settings. By advocating for an IPV focus in disaster response systems, IPV professionals can improve local community capacity to respond to IPV in the wake of disaster.
IPV and Disaster Preparedness
The disaster preparedness phase involves participating in activities before a disaster to help individuals, families, organizations, and communities prepare to respond to a disaster if one occurs (FEMA, 2016b). Preparedness objectives for IPV professionals can include creating IPV and disaster public awareness initiatives and promoting disaster safety planning.
Increase IPV and disaster awareness
IPV professionals can participate in several activities before a disaster to better prepare individuals, families, organizations, and communities to respond to IPV and disaster if an event occurs. The first preparedness strategy is to increase IPV and disaster public awareness. Numerous local, state, and federal emergency management professionals respond in the event of a disaster. However, emergency management professionals are often not adequately trained on responding to the safety concerns and needs of women experiencing IPV (Parkinson & Zara, 2013). Since emergency management professionals are often the first line of response for many people who experience disaster, education and training in IPV and disaster is essential. IPV professionals can be directly involved in these efforts by providing emergency management trainings and educational information on IPV and disaster. Key knowledge components to provide in trainings for disaster professionals include the nature and dynamics of IPV, what to do if IPV is disclosed, and how to connect IPV survivors to services, support, and housing (First, 2014).
In addition to increasing IPV awareness among disaster professionals, IPV professionals can partner with disaster professionals to provide IPV shelters and programs with training and education in disaster preparedness (Enarson, 1999; Parkinson & Zara, 2013). IPV professionals can also promote disaster preparedness awareness in IPV shelters and programs through communication efforts such as fliers, posters, announcements, meetings, and social media. Social media, particularly, may be a helpful tool for increasing disaster preparedness awareness among a variety of organizations and settings (Houston et al., 2015) and can function as a useful tool for connecting IPV professionals and clients to disaster preparedness information ahead of an event. IPV programs are increasingly using social media networks to promote IPV awareness initiatives (National Association to End Domestic Violence, 2016), and these efforts could also promote greater awareness of disaster preparedness activities.
Promote disaster safety planning
A second disaster preparedness strategy is to assist women in creating safety plans for both nondisaster and disaster situations. Safety planning with a woman in an abusive situation is one of the most significant interventions IPV professionals can employ to support a woman’s safety and empowerment (Danis & Bhandari, 2010). A safety plan is a personalized, practical plan that includes short- and long-term strategies to remain physically and emotionally safe in an environment that may threaten an individual’s safety (Danis & Bhandari, 2010). IPV professionals can further promote a woman’s safety and empowerment by incorporating practical plans and strategies to remain safe if a disaster were to occur. For example, safety planning for a disaster includes creating an emergency kit (e.g., flashlights, first aid kit, food and water, charged cell phone) and identifying safe areas for individuals to reside in each type of disaster (CDC, 2016). When safety planning for a disaster, children should be included in the planning process and should be informed about safe areas they can go to and safe people they can contact in a disaster (CDC, 2016). Likewise, the needs and safety of family pets should be included in disaster safety planning (e.g., evacuating pets, identifying places to board pets, having pet food and medicine; Sebolt, Williams, & First, 2014).
IPV professionals can also connect with their local emergency management offices to identify disaster hazards present in their IPV shelter or program area (FEMA, 2016b). After identifying potential hazards and risks, emergency and disaster plans should be created to these issues. Emergency and disaster plans should include communication plans, evacuation procedures, safe areas for sheltering in place, and a medical response contact (FEMA, 2016b). When creating emergency and disaster plans, vulnerabilities of clients should also be assessed, as different women will have varying needs during and after a disaster (Enarson, 1999; Jenkins & Phillips, 2008). For instance, the needs of marginalized populations such as refugee and migrant women (e.g., bilingual services, legal advocates) and the needs of women with disabilities (e.g., accessibility, medical supplies and devices) should be assessed and incorporated into emergency and disaster plans. After emergency and disaster plans have been developed, these plans should be practiced regularly among IPV staff, clients, and volunteers (FEMA, 2016b; Enarson, 1999).
IPV and Disaster Response
The disaster response phase is the time during and immediately following a disaster and focuses on securing survivors’ immediate safety and basic needs (Dass-Brailsford, 2010; FEMA, 2016b). IPV professionals responding to a disaster event can promote empowerment for women and children by ensuring their basic needs are met and providing them with comfort and support.
Ensure basic needs are met
Disasters can inflict a variety of harms to individuals and families (e.g., injury and death, property loss and displacement, financial harm, mental health consequences; Galea, Nandi, A., & Vlahov, 2005). Following a disaster, IPV professionals should first assess the extent and impact of the damage caused by the disaster and identify available capacities and supports to meet survivors’ immediate needs (FEMA, 2016b; Enarson, 1999). Although the impact of a disaster may vary, basic needs that often arise immediately following a disaster are food, shelter, medical care, and comfort (CDC, 2016). IPV professionals can assist clients by making sure these basic needs are met. As a result of a disaster, IPV shelters and programs may be temporarily or fully damaged immediately after the event (Houghton et al., 2010) and therefore clients may need to evacuate to a new location. IPV professionals can help ensure that clients have transportation, essential supplies (e.g., food, water, diapers, formula, medications), and information on post-disaster resources and alternative IPV contacts such as the state domestic violence hotline or the National Domestic Violence Hotline (Enarson, 1999).
Provide comfort and support
Disasters can be severe, traumatic events that cause widespread psychosocial reactions among survivors (Dass-Brailsford, 2010). Common stress reactions experienced by survivors of disasters are shock, disbelief, anxiety, fear, sleep disturbances, anger, distress, and grief (Dass-Brailsford, 2010). Disaster and IPV situations are both often characterized by loss of safety and control. Acknowledging and encouraging a woman’s strengths and positive coping skills has been shown to promote her empowerment in crisis situations (Black, 2003). IPV professionals can also provide information on common reactions to traumatic events and on calming techniques to assist with managing overwhelming feelings (Dass-Brailsford, 2010). Likewise, comfort and support should be provided to children exposed to IPV and disaster. Children often encounter difficulty expressing their emotions and making sense of crisis (Dass-Brailsford, 2010). IPV professionals can provide parents with information about how to support their children following exposure to IPV and disaster, such as setting up safe play areas and normalizing and validating children’s feelings (First, 2014).
IPV and Disaster Recovery
The recovery phase of a disaster includes actions individuals, families, organizations, and a community conduct to rebuild and recover following a disaster (Houston, 2012). In the recovery phase, individuals, families, organizations, and the community begin to shift from responding to the disaster to rebuilding and recovering from the event (Dass-Brailsford, 2010). IPV professionals can empower women experiencing IPV and disaster by connecting them to long-term services and promoting psychosocial recovery.
Connect to long-term services
In the longer term following a disaster, when temporary assistance services begin to recede (e.g., disaster shelters, crisis counseling services), many women will continue to experience poverty, displacement, mental and physical health concerns, and other stressors, each of which can be associated with an increased risk for IPV (Enarson, 1999). When considering the recovery needs of women and families experiencing IPV and disaster, a primary challenge is securing long-term services such as affordable housing and child care (Reid, 2013). Assisting women in securing available disaster assistance services such as case management can help connect them to long-term services, such as affordable housing, insurance claims, child care, and health services, and can empower women to achieve safety and independence. Such support may serve both protective and promotive functions within the client’s social environment and thus empower women to achieve independence and safety.
Promote psychosocial support
Disasters may also disrupt informal resources such as social and family systems that can provide practical and psychological support to help victims cope with IPV (Lauve-Moon & Ferreira, 2016). Developing social support has been recognized as an important protective factor among both women experiencing violence (Levendosky et al., 2004) and survivors recovering from disaster (Kaniasty, 2012). In an effort to provide mutual support and connectedness, connecting women with others who share common histories, issues, and barriers is an important strategy for promoting long-term empowerment (Lum, 1996). Utilizing group-based services is one way that IPV professionals can connect women experiencing IPV and foster social support. Following a disaster or collective trauma, group work has been found to be a helpful tool for building connectedness and mutual support (Malekoff, 2017), and given its capacity to “involve large segments of an affected community, agency, or organization,” group interventions can be an effective and timely tool to reach a larger population (Jarero & Artigas, 2012, p. 221).
In the aftermath of a crisis (e.g., disaster, IPV), survivors often struggle to describe and make sense of the trauma they have experienced (Dass-Brailsford, 2010). Thus, helping individuals to develop narratives of resilience and empowerment is an important strategy to promote coping and recovery following a disaster or IPV (Solnit, 2009). In addition, arts-based interventions delivered in group settings (e.g., digital story-telling, photovoice, art therapy) can be helpful in promoting collective narratives of strength and resilience following disaster and IPV (Anderson, 2010; First, Mills-Sandoval, First, & Houston, 2016). Arts-based interventions can provide the mechanism for a narrative and creative process that allows women to “re-story” their experiences of abuse and disaster so that they may envision their individual and collective strengths (Anderson, 2010). Utilizing therapeutic models that provide group support, strengths, and resilience can further empower women to rebuild and recover from disaster and IPV destruction.
Directions for Further Work
Over the past few decades, researchers and practitioners have highlighted the severity and prevalence of IPV experienced by women in disaster settings (Anastario et al., 2008; Buttell & Carney, 2009; Enarson, 1999; Harville et al., 2011; Lauve-Moon & Ferreira, 2016; Schumacher et al., 2010). The current article described key objectives and strategies to help IPV professionals promote women’s safety and empowerment in IPV and disaster settings. Even so, much more work is needed to better understand and address the needs and vulnerabilities of IPV victims in disaster settings. Below we highlight two areas needing further development. First, effective policy solutions are needed to integrate IPV services and resources into disaster settings. Second, additional research is needed that examines intersectional dimensions of women’s experiences of IPV and disaster. Each of these areas is described further below. We believe social work is well suited to lead this work, given the profession’s involvement in disasters and promotion of crisis intervention, community organizing, and social justice (Galambos, 2005).
First, social workers in partnership with local communities and organizations can advocate for public policies that protect women against violence in disaster settings. In the United States currently, the primary law that underlies the role of the federal government in presidentially declared disasters is the Robert T. Stafford Disaster Relief and Emergency Assistance Act, which provides states and localities with financial, technical, and logistical support during disaster or emergency events that overwhelm their capacity to respond (FEMA, 2016b). However, within the Stafford Act, there are no disaster assistance funds or resources dedicated to address the needs and vulnerabilities of IPV victims in disaster settings (Lauve-Moon & Ferreira, 2016). For example, a primary obstacle faced by victims of IPV and disaster is securing affordable housing after a disaster. The current rental assistance policy in the Stafford Act limits funding to only one head of each predisaster household. This provision can create vulnerability for a woman living with an abusive partner, as it limits her option to leave that partner and acquire her own housing (Menard, 2001; Reid, 2013). Thus, the development of disaster policy that considers the post-disaster needs of victims of IPV is needed. Social workers’ involvement in disaster settings has long emphasized the unique needs of vulnerable populations in disaster events and has stressed the value of services, resources, and effective policies for such populations (Galambos, 2005), and thus social workers are needed as policy advocates in the domain of IPV and disaster.
Second, research on IPV and disaster often considers gender as a homogeneous category, thus implicitly assumes that women experiencing IPV essentially share the same life experiences (Lockhart & Mitchel, 2010). However, in reality, various dimensions of social inequality can intersect to create unique challenges to women experiencing IPV. Therefore, it is important to recognize intersecting social inequalities that shape women’s experiences of IPV, such as race and ethnicity (Sokoloff & Dupont, 2005; Sewpaul, 2013), national origin (Zadnik, Sabina, & Cuevas, 2016), migration (Mehrotra, 2010), class, (Sokoloff & Dupont, 2005), physical ability (Rich, 2014), and living in a rural or urban environment (Sandberg, 2013). Future disaster and IPV research should examine various dimensions of social vulnerability and risk from an intersectional framework, and these results can then be utilized to improve and expand our proposed IPV and disaster framework. In addition, research is needed to examine how different types of disasters (e.g., natural, technological) impact women experiencing IPV, as few studies have examined the impact of technological disasters, on women experiencing IPV (Lauve-Moon & Ferreira, 2016).
Conclusion
Multiple studies offer evidence that disasters can increase the prevalence and severity of IPV and have compounding effects on women’s post-disaster recovery. Therefore, IPV services and resources should be integrated into disaster-related assistance and services. Professionals working in IPV shelters and programs can utilize the IPV and Disaster Framework to implement services and resources to address violence against women in disaster settings. Moving forward, policy solutions are needed to integrate IPV services and resources into federal disaster assistance plans, and additional research is needed that examines intersectional dimensions (e.g., race, migration, socioeconomic status, physical ability, age) related to women’s experiences of IPV and disaster.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Disaster and Community Crisis Center (DCC) at the University of Missouri, a partner in the National Child Traumatic Stress Network, which is funded by the Substance Abuse and Mental Health Services Administration (SAMHSA), U.S. Department of Health and Human Services (DHHS).