
Abstract
Youth-centeredness presents a “deficit model” of aging and stigmatizes elders. Social constructions reduce the aging process to illness and asexuality. Western conflations of beauty and youth render older adult sexuality disgusting and/or abnormal. Grounded theory methods utilized to interview older women (N = 20) about love, intimacy, and sexuality reveal more complex and heterogeneous narratives than we are socialized to believe. While important commonalities were reported across age cohorts, relationship statuses, and sexual orientations, sociohistorical as well as psychosocial factors, such as the feminist movement, attitudes about aging, experiences of ageism, and views on sexuality, demonstrate both within- and between-group differences.
Keywords
Ageism is a problem that is both reflected in and reinforced by projections of older people in mass media, perceptions held by social others, and the views and values we ourselves hold (Butler, 1969; Corbin, 2013; Saltzman, 2010). Despite being the one “-ism” that we will all experience if we live into old age, sociologists argue that pejorative projections of aging persist because they are built into the very fabric of our society; that is, an institutional ageism exists within the American infrastructure itself. According to social constructionists, these structural forces perpetuate myths about aging and universalize aging experiences that have been critiqued by social gerontologists dating at least back to Butler’s (1969) allegation that ageism is simply “another form of bigotry.”
Despite sex being a significant desire and need that all humans share and experience throughout the life course, older adults’ sexual expression is often ignored or ridiculed by younger members of society. A recent study found that female caregivers aged 60 to 80 feel ageist constructions depict them, and older women in general, as asexual (Drummond et al., 2013). That is, our youth-centric society problematizes aging bodies, assuming that aging negates the interest in or ability to be sexual; therefore, medicalized contemporary social constructions of the aging body relegate older adults to a sick, inherently asexual role. Our cultural entwinement of sexuality with youth and beauty encourages people—of all ages—to perceive the sexual expression of older adults as disgusting and abnormal, and those who are sexual may be labeled as deviant.
Ignoring the sexual interests of older adults or labeling these interests as repugnant and abnormal is damaging to the older adult population and each of us as we ourselves age. Some older adults are embarrassed by their active sexuality, and others do not act on or admit to having sexual urges or interests because they internalize society’s stereotype of their asexuality (Lindau et al., 2007; Watters & Boyd, 2009). Even those who do not allow this stereotype to affect their behavior are affected by the corrosive assumptions of their asexuality (DeLamater & Moorman, 2007). If they internalize the social construction of sexuality vis-à-vis aging, then older adults demonstrate tacit compliance with ageist American cultural values and expectations. This research examined the experiences of older women and sexuality, and our findings contribute to the sociological and gerontological literatures debunking the stereotype of older adults’ asexuality and challenging the conflation between youth and sexuality.
If all women are sexually objectified and subjected to the male gaze, then older women are particularly disadvantaged by youth culture (Slevin & Mowery, 2012). They are affected by what Daniluk refers to as the “twin prejudices” of ageism and sexism (as cited in Barker, 2004, p. 49). Such experiences of stigmatization and discrimination position older women as doubly invisible. Since ageist societies encourage older people, women especially, to be invisible, people too often rely on stereotypes to understand that which they cannot or do not see. In the realm of sexuality, this means that many people assume all older adults are asexual. Mass media, including advertising, newspapers, television, movies, and music, reflect and simultaneously reinforce such negative stereotypes of aging commonly held in American society (Corbin, 2013).
Sociologists have long argued that adequate representation of homosexuals in the mass media is lacking and that the homophobic messages that do exist together marginalize those who identify differently. Accordingly, conceptualizations of sex are caught up in a heteronormativity that defines “sex” as the penetrative practice of a penis being inserted into a vagina (Averett, Yoon, & Jenkins, 2011). Heteronormativity demonizes homosexuality and disparages homosexuals. In concert with Hill Collin’s (1991) work on intersectionality and those highlighting the role of time and context in shaping subjective experiences (Hulko, 2009; Mehrotra, 2010), we argue that older lesbians are “triply invisible” due to their age, gender, and sexual orientation. Multiple layers of invisibility have significant implications, such as greater probability of internalizing societal stereotypes and experiencing associated negative effects. It only takes consideration of the quadruply invisible, such as an older lesbian of color, to realize the potential snowball effect of discrimination. Unless the problematic statuses that women are relegated to are exposed, they cannot be confronted.
Historical Background and Literature Overview
Our patriarchal society historically framed “pleasure” from a man’s perspective, making it a woman’s marital duty and expectation to please her husband (Laumann, Gagnon, Michael, & Michaels, 1994; Sewpaul, 2013). Conceptualizations of sex and marriage have radically changed over time, and women’s sexuality and satisfaction are now championed rather than systematically ignored (Laumann & Michael, 2001). While Baumeister’s (2000) theory of feminine plasticity asserts that sexualities are shaped by culture and socialization, the sexual views and values held by those cohorts of women who are currently older adults and came of age directly proceeding or during the second wave of feminism and the sexual revolution have not been adequately examined. In particular, if sexuality is influenced by sociocultural and situational factors, then we would assume that the relevant social movements, here the feminist movement, shape women’s views and values related to love, intimacy, and sexuality.
With the contribution of the second wave of feminism and the sexual revolution, men’s sexual dysfunction was also no longer seen as solely a woman’s problem. Increases in media attention and pharmaceutical treatments both reflect and reinforce the medicalization and increased diagnosis of sexual dysfunction. Viagra, the most commonly used treatment for erectile dysfunction (ED), was discovered accidentally in a drug trial for a pill to fix heart problems that resulted in prolonged periods of erections (Loe, 2004a). Shortly thereafter, a medical condition (ED) was “discovered” in medical practice, and Viagra was prescribed as a drug to help (Loe, 2004a). This arguably led to the overdiagnosis of sexual dysfunction, as such a medicalized and deficit-based model enabled men to seek a quick fix for their problems while ignoring any potential social or psychological causes and unintended consequences. The emergence of Viagra and similar products had the positive effect of bringing attention to older adult sexuality, but it also bolstered our cultural problematization of older adults’ sexuality (Burgess, 2004; Katz & Marshall, 2003).
In the last decade, a paradigm shift, referred to as the “new aging” movement by social gerontologists, has occurred in which sexual decline is no longer seen as an inevitable, natural part of aging. This portrayal, while seemingly better than older adults being framed as sick and dysfunctional, is also damaging because older adults are now expected to have ageless, fully functional bodies and libidos (Katz & Marshall, 2003; Marshall & Katz, 2002). The inflation of sexual expectations at all ages, an unfortunate consequence of a highly medicalized pharmaceutical era, causes potential problems (or increased pressure) for all of us. Both the stereotype of older adults’ asexuality and the emerging “new aging” movement’s overemphasis on sexuality have a number of serious social consequences for the older adult population and society in general. Given the “cascade of effects” critics claim are common in modern medicine, the advent of Viagra and concomitant attention to older adult sexuality, while helping many (mostly men), has also created new problems for others, including women for whom the medications have resulted in physical issues, couples whose libidos are now inconsistent, and those for whom relationships are terminated as a result (Loe, 2004b).
The generally problematic nature of a homogenized and overly simplistic approach to the older adult population is all the more apparent as an expected four million people will be members of this population by 2030 (Reingold & Burros, 2004; Ritter, 2011). Now that the Baby Boomer generation has begun to turn 65, specific attention is being called to the rising number of older adults who may face discrimination and mistreatment, particularly in the realm of sexuality (Thompson, 2008), which makes this research timely and important.
Most sexuality scholarship focuses on younger populations and so-called reproductive technologies, so there is a lack of significant research on older adult sexuality. Many target a specific age-group, such as the 18–35 cohort, although others claim to encompass the entire population, yet limit themselves to 18–55 or 18–60. Of the studies conducted with older adults, most are of the young-old, typically under 70 or 75. There is a dearth of literature on homosexual older adults, and even less that encompasses both hetero and homosexual older adults (Slevin & Mowery, 2012). Therefore, this exploratory study contributes to the literature on both hetero and homosexual older women’s sexualities. This research reveals the myriad consequences of American social constructions of older adults, underscores the important roles social workers occupy, and suggests policy implications of current and future approaches. It is only through considering and remedying both the individual experience and systemic approach to older adults that we can, as a society, move toward rectifying how we treat this important and disadvantaged population.
Method
This exploratory study was conducted using qualitative interviews to capture older women’s subjective experiences, views, and values related to love, intimacy, and sexuality. Data were collected using nonprobability sampling, specifically convenience and snowball sampling. Respondents were originally recruited from the Worcester Senior Center, where the first author placed informational flyers and enlisted volunteers. Since we were interested in understanding both homosexual and heterosexual women’s experiences, information about this research project was posted in several lesbian, gay, bisexual, and transgender (LGBT) Elder Network newsletters in Worcester, MA. These recruitment methods garnered 10 respondents and the remaining women were obtained through snowball sampling and recruitment at a women’s-only gym. Only one woman declined participation after expressing initial interest and learning of the study objectives.
Interviews began after receiving approval from the Human Subjects Committee at the College of the Holy Cross. Cross-sectional semistructured in-depth interviews were conducted face to face, and they lasted between 25 and 80 minutes. The interviews were conducted at locations of the participants’ choosing, including their home, place of work, or Senior Center.
Before each interview began, permission to be interviewed and audio recorded was obtained verbally and through written informed consent. Participants were assured of the confidentiality of their interviews and all potentially identifying data were removed and pseudonyms were assigned to each respondent. In the spirit of qualitative research, a tentative interview guide was used to elicit accounts of older women’s sexuality and while conversations generally flowed smoothly, prompts were used as needed to elicit additional information. To minimize potential researcher and respondent bias, inductive research methods were used. This approach assumes that participants are the experts and encourages them to steer the conversation in directions that resonate with them rather than assuming what is important to them a priori. While the guide was used to facilitate discussion, it was not followed linearly or comprehensively, and topics were added as and when they arose in the interview context.
All interviews were recorded and transcribed verbatim. Theoretical and substantive memos were written immediately following every interview. After the interviews were conducted and transcribed, they were manually coded, line by line, by both authors following a grounded theory approach (Corbin & Strauss, 1998; Glaser & Strauss, 1967). From this iterative process, a scheme was constructed to identify themes and patterns among respondents, as well as interesting outlier cases. This thematic analysis produced the research findings that will be reported subsequently.
Demographics
The demographic breakdown of the 20 (N = 20) participants’ age, marital status, sexual orientation, and race is provided in Table 1.
Variables of Age, Marital Status, Sexual Orientation, and Race.
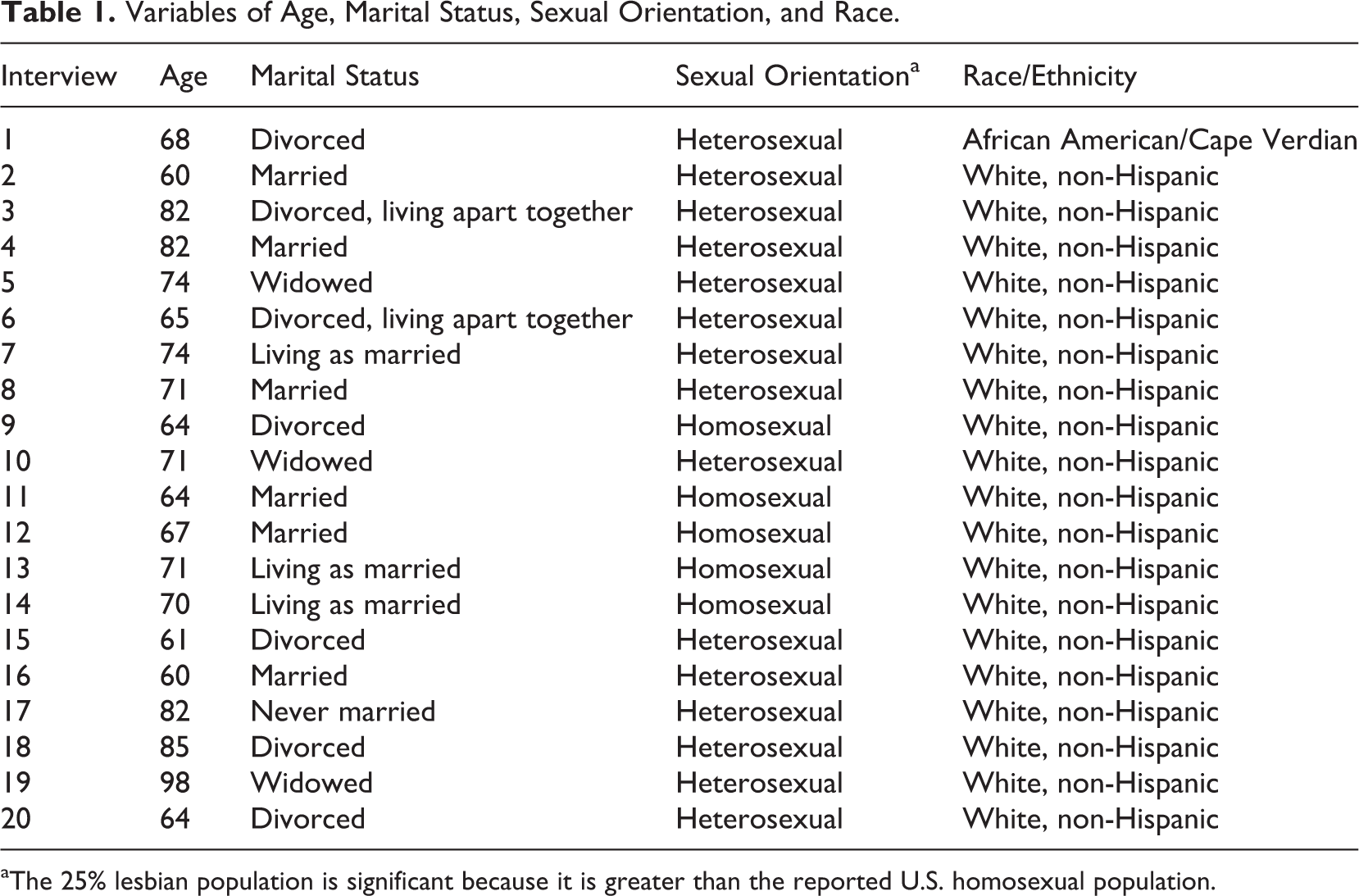
aThe 25% lesbian population is significant because it is greater than the reported U.S. homosexual population.
As Table 1 reveals, the 20 women interviewed ranged in age from 60 to 98, with an average age of 72 years. While we understand the importance of “cohort studies” advanced by Matilda While Riley and other social gerontologists since the 1970s, our sample was not big enough to permit such subset analyses. Also, only one respondent identified as a race other than white. While this was not intended or anticipated considering recruitment focused predominantly on urban areas where all races are well represented, this is a significant limitation of the study. Seven of the respondents (35%) were divorced, two of whom were in serious relationships, but opted for “living apart together” rather than cohabitating with their significant others. Six participants (30%) were married, although another three respondents (15%) were “living as married.” Two of the three living as married had been relegated to this status as lesbian partners who were not allowed to marry formally until very recently. Another three respondents (15%) were widowed and one participant had never been married. The next section explores a few of the common trends that arose from continuities among the women’s narratives.
Results
Study participants noted that many historical and social events had influenced their views, values, and thus experiences of love, intimacy, and sexuality. In particular, the historical epoch in which respondents came of age was relevant. The women’s movement in particular was said to play a profound role in their interpretations of sexuality. Likewise, participants reported that the long-standing American cultural devaluing of age and aging, that Butler coined “ageism,” has had the unintended consequence of fostering conflations of youth and beauty, stereotypes of older adults as asexual and subsequently medical oversight of older women’s sexual health. These two main themes revealed in the study narratives will both be discussed in further detail.
Impact of the Feminist Movement
When asked about events and experiences that had shaped their views and values related to love, intimacy and sexuality, almost all respondents (n = 18) reported that the feminist movement
1
had a significant affect. Interestingly, half of them felt the impact of the feminist movement was positive, while three (20%) reported it was negative because of how it impacted men and culture. Another 20% each were ambivalent or saw positive and negative aspects of the movement and differentiated between the feminist movement and sexual revolution (citing they felt the former was positive and the latter was negative). The following is an illustrative array of their varying perspectives: I don’t think people thought about how changing the role of women would change their relationship to men and disrupt that balance. They didn’t think about how men would react…Men defended their masculinity and are more aggressive and war-like now. The sexual revolution made women more like men, which was not a worthy goal…They didn’t consider that changing the shape of the yin would affect the yang…The movement created a tug of war and a fight for power. (Eloise, age 82, heterosexual, divorced) I think the girls today are really suffering. In a different way than we did, we were held down and expected not to engage in sexual affairs until we were married…So I think girls have gone backwards a little bit. Guys used to treat you nice and with respect, opening doors and helping you with your coat…and when you were dating, no was no. Today you say “no” and they say, “yeah you want it…” Although the girls today have a lot more sexual freedom, it comes at a cost. (Johanna, age 71, heterosexual, widowed)
Women like Eloise and Johanna were concerned with how the feminist movement influenced gender dynamics. Eloise believed that women have become more like men and this upset the status quo or balance of “yin and yang,” while Johanna observed that relationships between men and women have been negatively altered and are less respectful as a result. She explained that women today are held down in a different way than her generation was, but they are held down all the same. By comparison, as noted subsequently, most women saw the movement more positively, such as Pamela’s observation that sexual barriers for women were broken down. Priscilla corroborated this view as she witnessed her friends seek divorces from stifling husbands. In breaking down the barriers for girls and women to be sexual, to admit to being sexual…it blew the walls down…I would say I was more empowered in my relationships. It made me an equal sexual partner with men. (Pamela, age 64, homosexual, divorced) During this time, I had four friends seek divorces from their husbands. But I feel it didn’t really affect me much, I feel like I was there before it happened. (Priscilla, age 82, heterosexual, married)
Anne, however, differentiated between the feminist movement and sexual revolution, associating the former positively with extended rights and the latter negatively with promiscuity. The sexual revolution and wave of feminism are two separate things. They are intertwined and I’m not sure which came first, like the chicken and the egg…The sexual revolution led to almost anything being okay with anyone at anytime, which was grossly under and over-stated. Feminism is an understanding that women are equal citizens, which ought to be honored, expressed, and woven into policy. (Anne, age 67, homosexual, married) I would have loved to have more children but rarely had unprotected sex…I took birth control throughout my marriage because of societal pressures to have only 1 or 2 kids. My husband did not want kids either…There’s a freedom but it stifles you in some ways…I suppose the sexual revolution was positive because I worked with women who had abortions and put up children for adoption and chose to be single mothers to not wait for a man to become a mother. (Mona, age 65, heterosexual, divorced) I grew up in the era of free love, the liberal movement toward the sexual revolution. It was a tough time for a young woman because sex was a free act to do with whoever in the moment, it messed with my head. I went along with that wave, but it made me feel hollow having sexual relationships without any kind of love with different guys…It left me feeling a little bit traumatized. But I think it’s good for women to have empowerment…The sexual revolution said, “I am woman, I don’t need men to define who I am.” I think it gave us equal footing. (Dolores, age 60, heterosexual, married)
These accounts demonstrate how important the feminist movement was for the women in this study. While Mona recognized it allowed other women to construct families in ways they could not before, the movement affected her personally in a negative manner because she felt pressured to use birth control and not have many children. Dolores’ youth and innocence during the feminist movement led her to experiment, having sex with a number of partners without what she defined as love or commitment, which left her confused, unfulfilled, and, in her words, “traumatized.” Despite these experiences, she looked back on her life and was grateful to have grown up when she did because she felt equal to men. The feminist movement allegedly affected many respondents by making them more open or liberal in their thinking, allowing them to be driven less by past, more restrictive cultural constructions of femininity. I think my ex-husband very much wanted a good minister’s wife who would raise the children, do things for the Church, a very traditional role. I began to move out of that role…The feminist movement certainly gave us space to be gay because it wasn’t anything that would have been possible at the time I got married. (Megan, age 71, homosexual, living as married) I think it was the feminist revolution that made me realize that my marriage was not as healthy as it should be. It opened my eyes to many things I couldn’t take a look at otherwise. We were occupying roles and one of the things the feminist movement did was to break up those boundaries and ask why they existed. It was empowering…The feminist revolution helped me to evaluate the quality of the relationship I was in, and I felt encouraged to own my life for myself and think about what I wanted to do apart from the relationship. (Lydia, age 70, homosexual, living as married)
Some study participants reported that the feminist movement exposed the circumscribed social roles they were occupying in their relationships, allowing them to potentially negotiate more equality with others or, like Megan and Lydia, to rid themselves of these scripts entirely by ending their relationships. Both Megan and Lydia realized they were gay during this period and actively pursue homosexual relationships, which is something neither felt was possible or available to them beforehand. The women who sought divorces or ended their relationships acknowledged that they were not in good relationships to begin with and the feminist movement simply helped them to see that by providing alternative gender role scripts to which they could ascribe.
These findings reveal that the overwhelming majority of respondents felt that the feminist movement had a significant impact on their conceptions and experiences of sexuality throughout their life course. Clearly, for most of these women, important social roles were negotiated throughout their lives, and they credited the feminist movement with giving them the impetus, directly or indirectly, to challenge various gender and sexual scripts. In this way, the historical period in which these women came of age was depicted as a pivotal factor in their biographies.
Ageism, Aging, and Asexuality Stereotype
Living in an ageist society has myriad potential consequences. In concert with the enduring cultural ageism American social gerontologists expose, the second major finding was that the women interviewed felt disrespected or judged vis-à-vis their expressions of love, intimacy, and sexuality, to varying degrees. The following comments provide a snapshot of what many women felt or observed: If sex is fulfilling and pleasurable there’s no reason why we shouldn’t. Younger people focus on disability because that’s what age is looked upon as. But inside I feel like I always did. Sexual activity is healthy and invigorating. I would tell people it’s none of their damn business and sex is not a spectator sport…here we are warehoused if we’re not careful. (Eloise, age 82, heterosexual, divorced) And some couples I know talk about the ageism they feel…I think there is more of a line once you retire. If you’re still working until 70 and people still see you as active in a working sense, that’s one thing. But once you retire, you’re in another category. It doesn’t matter how youthful or active you may be, somehow you get put in this category. (Megan, age 71, homosexual, living as married)
These comments suggest that study participants believed that members of society view age and people who are aging through a deficit-based lens, especially those members who are no longer participating in the paid workforce, and the loss of such important societal roles was keenly felt by respondents. These impressions exemplify what Goffman (1963) referred to as “felt stigma,” a fear or anticipation of stigma evident in interaction. Some respondents feared being treated differently or discriminated against, thus anticipating ageism. Both Eloise and Megan alluded to the precarious position they and their peers are in, being marginalized from society by using binaries (e.g., sexual or not, working or not, aging well or not, physically active or not, demented or not). For example, Eloise felt most members of society associate old age with disability, putting older adults at risk of being “warehoused if we’re not careful” (i.e., placed in nursing homes). Such dichotomies, including assumptions that older adults are asexual, label older adults as “have-nots,” which relegates them to the status of “other” as well as polarizing society members into groups of “old” versus “young” and, perhaps more insidiously “us” versus “them.” In a modern capitalist society, employment is an especially salient realm where this distinction is made because we are socialized to associate older age with retirement and assume the latter means elders are not active, youthful, and contributing to or participating in society.
While the overwhelming majority of the women talked about experiencing ageism, many also expressed that they did not feel their age. Many explained that they still felt young and active, expressing surprise at their numerical age and staunch opinions that they were aging well: I haven’t gotten old yet, just older. (Mona, age 65, heterosexual, divorced) I am in pretty good shape and a lot of times I don’t perceive myself as old, I feel young…I think the saying, “You only feel as old as you are,” it’s true…There are days that I feel like I’m twenty, I know I’m not twenty but some days I feel like it because I feel good. (Ella, age 71, heterosexual, married)
Ella’s and Mona’s comments are representative of their peers’ perspectives that their age is “just a number,” something that does not necessarily dictate who they are or directly affect how they feel about themselves. This supports what medical anthropologist Kaufman (1986) long ago argued: that older adults talk about themselves as ageless, as their identities demonstrate continuity regardless of their age or stage. That is, our identities are not static but incorporate changes as we age and/or experience adversity. The women in this study expressed constructions of self that were similarly enduring, which lead them to feel particularly troubled by the ageism and stereotype of older adults’ asexuality they experienced as they aged.
Interestingly, there were a few women who were acutely aware of their aging and at least two of them attributed their extramarital affairs to their own experiences of aging and ageism: The 50 s are a turning point for appearance and beauty, and I felt my window of opportunity to look and feel younger was ending. There’s a natural midlife crisis where your attractiveness weighs against your mundane existence with the routine predictability of life. It’s natural to wonder if you can attract other people anymore, I think it’s part of the aging process. I had an affair as part of my midlife crisis, I wanted to play out this fantasy in my head. (Dolores, age 60, heterosexual, married) You know, I felt very young and sexual until I was 70…it was at 70 that my attitude really changed and what was important to me changed…I felt I’d finally matured into an older woman…I stopped having affairs. My ego has always been important to me and at 70, I lost it. I had had 30 year affairs, 20 year affairs, and others but the intrigue and interest subsided…(Priscilla, age 82, heterosexual, married)
Both Dolores and Priscilla experienced aging as intense and negative and used this to explain extramarital affairs. These women attributed their affairs to similar triggers, such as their (perceived to be diminishing) ego and feelings of attractiveness. While there were many parallels in their accounts, one drew on experiences in her 50s and the other from her 70s. Yet, these similar rationales were used by the former to begin an affair and by the latter to end a number of them. Dolores used the affair to prove to herself that she was still attractive and sexy. Priscilla, meanwhile, explained that “ego” and needs to get sexual satisfaction, as well as the interest and intrigue of an affair, were what drove her to have multiple affairs that lasted decades. By her 70s, she experienced a change of perspective regarding what was important in life and affairs no longer intrigued her. Despite the 20-year age gap between these two women, both of their aging experiences generated a desire to have affairs. Priscilla attributed the infidelity throughout her life to her “ego” just as Dolores credited her single affair to a decreasing sense of attractiveness. Given our culture’s obsession with youth and beauty, it is no surprise that the presumed inverse relationship of aging and attractiveness may lead older women to feel inadequate or past their prime.
The stereotype of older adult asexuality is a significant manifestation of our ageist society. While the majority of respondents (n = 16) were aware of assumptions of older adult asexuality, six felt members of our society, while still ageist, have largely gotten over that stereotype. They explained that they saw it as passé, perhaps commonplace during the time of their parents’ generation, but that we have modernized and moved past this. Interestingly, two women thought it was a stereotype that described men, but not women, because, as Marshall and Katz (2002) also suggest, the saturation of ED commercials fixates on older men’s sexual problems. The women had much to say about the stereotype of older adult asexuality: I think it’s partially because aging is seen as disgusting in this youth culture. And so sex among disgusting beings is even more disgusting. And if most of the old people they know are their parents and grandparents, they don’t want to think about it anyway. (Pamela, age 64, homosexual, divorced) It’s like trying to expect young people to not have sex. It’s part of human nature. I think with the same regard on the young end of the bell curve, the intensity and frequency and choice of style might vary. But, don’t be trying to box folks in. (Christine, age 62, homosexual, married) I think you have to be careful with any kind of generalization like that, it doesn’t apply to everyone. Sure it’s true of some that they’re not interested anymore, but some people definitely have an interest and it’s important to them…I think people need to start thinking of this age group as sexually active, it’s definitely a possibility. (Kimberly, age 61, heterosexual, divorced) I believe there’s a level at which passion continues, but it’s less often. The body responds differently, but I sometimes feel resentful about the attitude that when you get older that there’s no life left in you. I don’t appreciate that because I don’t think it’s true. (Megan, age 71, homosexual, living as married)
Some respondents theorized why the stereotype exists and persists, like Pamela’s observation of the interplay between our culture’s ageism and obsession with youth and sex that leads older sex to be viewed as disgusting or deviant. Either way, these women did not appreciate the stereotype of older adult asexuality because they viewed it as ageist and did not like being boxed into specific categories. Christine, Kimberly, Megan, and others mentioned that sexuality and sexual interest may vary with age, but the experience is highly individual and different for everyone at every phase of the life course.
In concert with Kaufman’s (1986) findings, many of the women felt views on sexuality and experiences of sex persisted over time: And I think as a nurse I did not believe that because I know sexuality…My patients in the nursing home still wanted it…I would say your sexuality will remain with you until the day you die and it is your attitude about sex that will change your physical aspects about sex. People don’t change, if you’re a sexual person at 21, you’ll be a sexual person when you’re 81. (Marcie, age 68, heterosexual, divorced) I know some people who are hot for sex and they’re really old, but they’ve been hot for sex their whole lives. (Stella, age 74, heterosexual, living as married) I believe whatever you are when you’re younger projects when you are old…so if you were sexual or angry or whatever, then you will be the same when way when you are older. (Ella, age 71, heterosexual, married)
These women felt that one’s outlook on sex and experiences of sexuality are relatively constant throughout the life course. Ella and Stella felt desire for sexual relations later in life correlated strongly with interest in these activities when younger. Marcie corroborated, elaborating that those who experience a substantial shift in their interests over time do so as a result of something in the external environment, such as an event that shapes one’s attitude and, subsequently, their sexual interest. This supports Baumeister’s (2000) theory of plasticity of the female sex drive, as well as Christine’s and Kimberly’s commonsense avowals that sexuality and age interplay differently for every individual.
Admittedly, some women noted changes in their sex drive or desires over time; while several observed an increase in their desire over time, most women reporting a change felt that they currently had less sexual desires or needs than when they were younger. Famed feminist Gloria Steinem recently shared similar views, stating her less active sex drive allows her to be free to focus on other important things (Spencer, 2014). Respondents who noted a change had mixed reactions to it, some sharing Steinem’s relief or even sense of liberation and others grieving the loss of their urges, like Priscilla and her “ego.” In support of Loe’s (2004b) findings, some women experienced their changing sex drive as particularly problematic when it conflicted with their partner’s needs.
This has become more prevalent with the influx of medication to prevent male impotence, such as Viagra. The vast majority of the women interviewed expressed concerns regarding how Viagra may alter sexual relations, such as increasing the pressure on men to perform sexually at the dismay of some of their female sexual partners who felt this part of their relationship was over. This has ramifications for partners’ mental and emotional health as well as that of their relationship (Loe, 2004b). Some women speculated Viagra exacerbates the partner gap, whereby men of their age seek younger women, given the additional ability and/or pressure to perform with the advent of medication to “treat” sexual dysfunction. Other women were frustrated with the lack of viable alternatives aimed at helping women and some respondents were discouraged that Viagra was ineffective in assisting their partners to satisfy their needs. Clearly, it is short-sighted and naive to homogenize, universalize, and generalize all older adults into a category of asexuality when they are a more diverse group of people than ever.
The asexuality stereotype is particularly problematic because it impacts the older adult population in overt and covert ways. Seven of the women reported that assumptions of older adult asexuality do not impact them directly but felt that it affects their peers. These accounts support the legitimacy of the assertion that most members of the older adult population believe that their peer group is negatively impacted by the cultural stereotype of asexuality. By contrast, only five women thought they and their peers were not impacted by the stereotype, and six women were unsure. Meanwhile, two interviewees relayed their experiences of being negatively impacted by the stereotype in terms of younger members of society making disparaging remarks or gestures that made these women feel embarrassed about their age or body. While the women differed in terms of the perceived effects of the stereotype of older adult asexuality, nearly half of the women suggested that the stereotype problematically affects older women.
Covert effects of the stereotype of asexuality arguably include physician oversight of or lack of attention to older women’s sexualities. Skultety (2007) found that a patient’s sexual history and current relations are typically a topic touched upon by doctors in a comprehensive biopsychosocial questionnaire, yet half of the women in the present study reported neither their primary care physician nor gynecologist inquired about their sexual relations in the last several years. Four women spoke to their primary care physician only, as they no longer saw a gynecologist after aging out of pap smears or being menopausal. Only four of the women spoke with their gynecologist or primary care physician about their sexual relations, and two of these women had not been to a doctor in years.
More than half of the participants reported that their doctors did not talk to them about their sexual relations. Perhaps the women’s physicians subscribe to the stereotype of older adult asexuality, foregoing this topic during visits with older female patients because they presume it is not applicable. While nearly every woman who reported that her doctor did not inquire about the topic attributed the cause to factors such as the death of a spouse, a divorce, homosexuality, sexual dysfunction, or assumptions patients were proactive, perhaps the hegemony of the medical establishment in American society obfuscates how doctors’ assumptions, as members of an ageist society, about older women’s asexuality shape medical practice.
In summary, there were a number of significant continuities between respondent’s stories. These women felt that the feminist movement was formative to their current views about and experience of love, sex, and gender roles. They also had a variety of values related to and experiences with aging and ageism, which was most obvious in the asexuality stereotype and the medical oversight of their sexual activity. The themes that emerged suggest that despite the uniqueness of each narrative and the multiplicity of women’s experiences throughout the life course, older women’s sexuality involves strong commonalities across time, relationship status, and sexual orientation.
Discussion
Both aging as a social process and older adults’ individual experiences are devalued in modern American society and many of our social institutions. As Butler claimed about his medical school training almost half of a century ago, American cultural values both reflect and reinforce pejorative views on aging—or “ageism.” This institutional ageism leads to an internalized stigmatization of aging and the aged and thwarts meaningful social change. Insight into older women’s attitudes about and experiences of sexuality can help combat both structural manifestations and personal experiences of ageism. In the process of learning about the subjective experiences of older women, our data add to the gerontological literature debunking both the conflation between youth and sexuality and the stereotype of older adult asexuality. In analyzing the women’s narratives, a number of significant trends emerged. The feminist movement was an overarching theme pervading these women’s narratives, impacting their identities and attitudes about nearly everything. Respondents’ experiences of aging were negatively affected by overt stereotypes of asexuality and social conflations of youth and beauty as well as covert medical oversight of their sexual activity.
If some of these women’s doctors failed to address their sexual relations because they subscribe to the stereotype of older adult asexuality, as has been suggested in prior research with older women (Drummond et al., 2013), then these findings can inform clinical practice by encouraging doctors to incorporate biopsychosocial evaluations as part of standard practice, as the whole individual must be considered when looking at any micro system of the body. Since there are both implicit and explicit forms of ageism in our culture, ageism manifests itself in myriad ways with wide-ranging effects.
This study is of particular importance because there is a paucity of research on the sexuality of older adults, and specifically older women’s views, values and experiences of love, intimacy, and sex. Arguably, such omissions in the literature reflect the stereotype of older adult asexuality, the predominance of male sexuality (or dysfunction, more aptly) when old adults are addressed, and the invisibility of this population due to sociocultural factors and intersecting identities (Hill Collins, 1991). People’s disinterest in, and sometimes disgust about, older adult sexuality relegates it to a less fashionable area of study than the youthful sexuality predominantly represented in the media. If the cultural avoidance reinforces the stereotype of older adult asexuality, then further research on the topic might begin to help combat this. This study was designed to include both hetero- and homosexual women, women of every relationship status, and women 60 and older, which allowed interrogation of assumed differences based on age, sexual orientation, and relationship status.
Like all studies, however, this research has a number of limitations. The participants who were recruited may be more homogenous due to the use of snowball sampling. Demographically, the lack of minority races and women who have never been married is not representative. Since roughly half of the participants were recruited through the Worcester Senior Center, the perspectives of women over 60 who choose not to attend senior centers or who reside in assisted living and nursing home facilities are not included. These limitations reveal the scope of this research, as well as recommendations for future research on the topic of older adult sexuality. Future studies should examine how narratives are affected by ageism and cultural constructions of sexuality and sexual functioning according to core sociological variables such as race/ethnicity, socioeconomic status, gender, and sexual orientation.
The advent of medications like Viagra and the related attention to sexual dysfunction has extended the medical gaze to include libido, which heightens expectations of sexual performance. This results in a false dichotomy of sexuality whereby we are either asexual or sexually enhanced beings. For seniors, ageism manifests through such essentializing stereotypes that problematize the process of aging itself as well as individual aging bodies. Stereotypes that suggest we are (or should be) highly sexual beings in general and that older adults in particular are either asexual or sexually enhanced have negative consequences, including on older people’s views of themselves, other’s treatment of this population, and the institutionalization of this ageism into policy and practice. Older adult sexual expressions are stigmatized not because the actions are abnormal, but because deviance is socially constructed. Older adult sexuality is framed as violating several norms, so people’s negative reactions to older adults’ sexual expressions reinforce the notion that these actions are deviant.
Arguably, this stereotype of older adult asexuality persists despite contradictory evidence because people have confirmation biases (Kimmel, 2000) in which their observances of the expected behavior in their lives or media depictions reinforce their beliefs (Corbin, 2013). The media powerfully contributes, as older adults are often utilized for comic relief or ignored (Saltzman, 2010). Older adults’ appearance in ED advertisements medicalizes sex, as older people can no longer be sexual without medical intervention. Beyond the topic of ED, sexual older adults appear so infrequently in the media that their sexuality is seen as a joke or caricature (Saltzman, 2010). In this way, behavior that disputes the stereotype is easy to ignore or delegitimize as an anomaly.
The stereotype of older adult asexuality perpetuates the status quo and the proliferation of beauty products, specifically for antiaging, as well as pharmaceuticals and devices to ameliorate or correct sexual problems because these industries thrive on people’s fears of aging and presumed asexuality. Assumptions of asexuality also benefit the younger segments of society in that negating older adult sexuality validates youthful sexualities, allowing us to deny aging and death and allegedly lead our lives unencumbered. Despite the profitability of the stereotype of older adult asexuality, it would benefit us—especially the older adult population but all of us as we envision our own aging experiences—to debunk this myth.
The cultural relevancy of this study is far reaching. This research is significant to scholars of gerontology, sociology, and psychology, as well as academics with specialties in medicine and medical ethics, social work, public health, history, gender, sexuality, and LGBT studies. It is particularly important to modern medical practice in America, which has medicalized sexuality and aging and arguably neglects older women’s sexualities. This has public health implications, given the increase in older adults living with human immunodeficiency virus/acquired immune deficiency syndrome and sexually transmitted diseases, diseases that often remain undiagnosed and untreated because they are interpreted as signs of aging. The implications for LGBT issues are also significant, as the narratives spoke to commonalities among all women and all relationships, providing a boon to the LGBT community’s calls for equality in opportunity and treatment.
This research could be beneficial to scholars of aging, as well as to people who work with the older adult population, especially social workers. Social workers are essential to improving the individual and systematic treatment of older adults because they serve pivotal roles as educators, trainers, community organizers, therapists, advocates, lobbyists, and policy practitioners (International Federation of Social Workers [IFSW], 2012). Improving the treatment of older adults aligns with social work values of dignity and respect and their mission to help poor and vulnerable populations, such as older adults (National Association of Social Workers [NASW], 2008).
Social workers are in a particularly advantageous position to help older adults because they work on the frontline with the population and are conduits between this relatively isolated population and the community. Through education, counseling, and advocacy, social workers can promote social integration by helping older adults work through felt and enacted stigma and advocate for themselves in policy and social service sectors, as well as in their interactions with members of society (IFSW, 2012). As community organizers, they can assist coalitions of older adults, groups such as local elder networks and Old Lesbians Organizing for Change, and mobilize people on a grassroots level to have their voices heard and their positions considered throughout the policymaking process and in practice.
Social workers also have an important role in educating and training others who work with older adults. Providing cultural competency and sensitivity training, especially queer sensitivity training, to people who provide direct services to older adults is vital (Ritter, 2011). This training could be modified and expanded to be utilized by various industries, such as insurance companies and unions, to encourage policies and practices that are more age-friendly and better address the needs of older adults (NASW, 2013).
Beyond practice and policy arenas, this study is pertinent to the general public because ageism is the one “-ism” that we will all experience if we live long enough. The general public may benefit from the cultural insight this study provides, as our societal treatment of the older adult population impacts our own sense of identity, self-worth, and satisfaction in life. Less pejorative conceptions of aging could help people to envision and experience their own aging more positively.
Sociologist and social gerontologists argue that stereotypes and myths of aging exist and persist as a mechanism of order and social control and to compartmentalize fears associated with death and aging. While evidence exists to debunk such myths, social institutions like medicine and the media maintain the status quo by concomitantly framing sex as abnormal or deviant, on one hand, and in need of medical enhancement/support on the other. Given the inevitability of aging and the inherent nature of human sexuality, it would benefit older adults and each of us as we ourselves age if universalizing stereotypes of elder sexuality and the conflation between youth and sexuality were dismantled. With predominantly negative images of aging, here vis-à-vis sexuality, is it any wonder that so few people embrace the thought of themselves as future old people?