
Abstract
Background
Blood lactate is commonly used in clinical medicine as a diagnostic, therapeutic and prognostic guide. Lactate's growing importance in many disciplines of clinical medicine and academic enquiry is underscored by the tenfold increase in publications over the past 10 years. Lactate monitoring is presently shifting from single to serial measurements, offering a means of assessing response to therapy and to guide treatment decisions. With the promise of wearable lactate sensors and their potential integration in electronic patient records and early warning scores, the utility of serial lactate measurement deserves closer scrutiny.
Methods
Articles included in this review were identified by searching MEDLINE, PubMed and EMBASE using the term “lactate” alone and in combination with “serial”, “point of care”, “clearance”, “prognosis” and “clinical”. Authors were assigned vetting of publications according to their specialty (anesthesiology, intensive care, trauma, emergency medicine, obstetrics, pediatrics and general hospital medicine). The manuscript was assembled in multidisciplinary groups guided by underlying pathology rather than hospital area.
Findings
Lactate's clinical utility as a dynamic parameter is increasingly recognized. Several publications in the last year highlight the value of serial measurements in guiding therapy. Outside acute clinical areas like the emergency room, operating room or intensive care, obtaining lactate levels is often fraught with difficulty and delays.
Interpretation
Measuring serial lactate and lactate clearance offers regular feedback on response to therapy and patient status. Particularly on the ward, wearable devices integrated in early warning scores via the hospital IT system are likely to identify deteriorating patients earlier than having to rely on observations by an often-overstretched nursing workforce.
Introduction
Blood lactate levels are increasingly used as a diagnostic tool and therapeutic guide in clinical medicine and their role in clinical practice has become a focal, and sometimes controversial, inquiry of academic interest. The growing interest in lactate is reflected in the tenfold increase in the annual number of publications on lactate in clinical medicine from about 200 to 2000 over the past decade.
Lactate has established a long history in medicine since its discovery in sour milk in 1780. In 1843 German physician-chemist Johann Josef Scherer was the first to demonstrate its presence in human blood after death. In 1891 Araki and Zillessen demonstrated that interrupting blood supply to the muscles of mammals and birds leads to the formation of lactate and that levels increased over time. 1
In 1984 Schuster published the first summary of studies examining the utility of lactate and concluded that “monitoring blood lactate is of considerable value for the metabolic monitoring of critically ill patients”. 2 It was not until 2009, however, that Bakker and colleagues published the first meta-analysis of over 150 reports and defined that measuring lactate concentrations helps risk-stratify critically ill patients and can provide an endpoint for resuscitation. 3
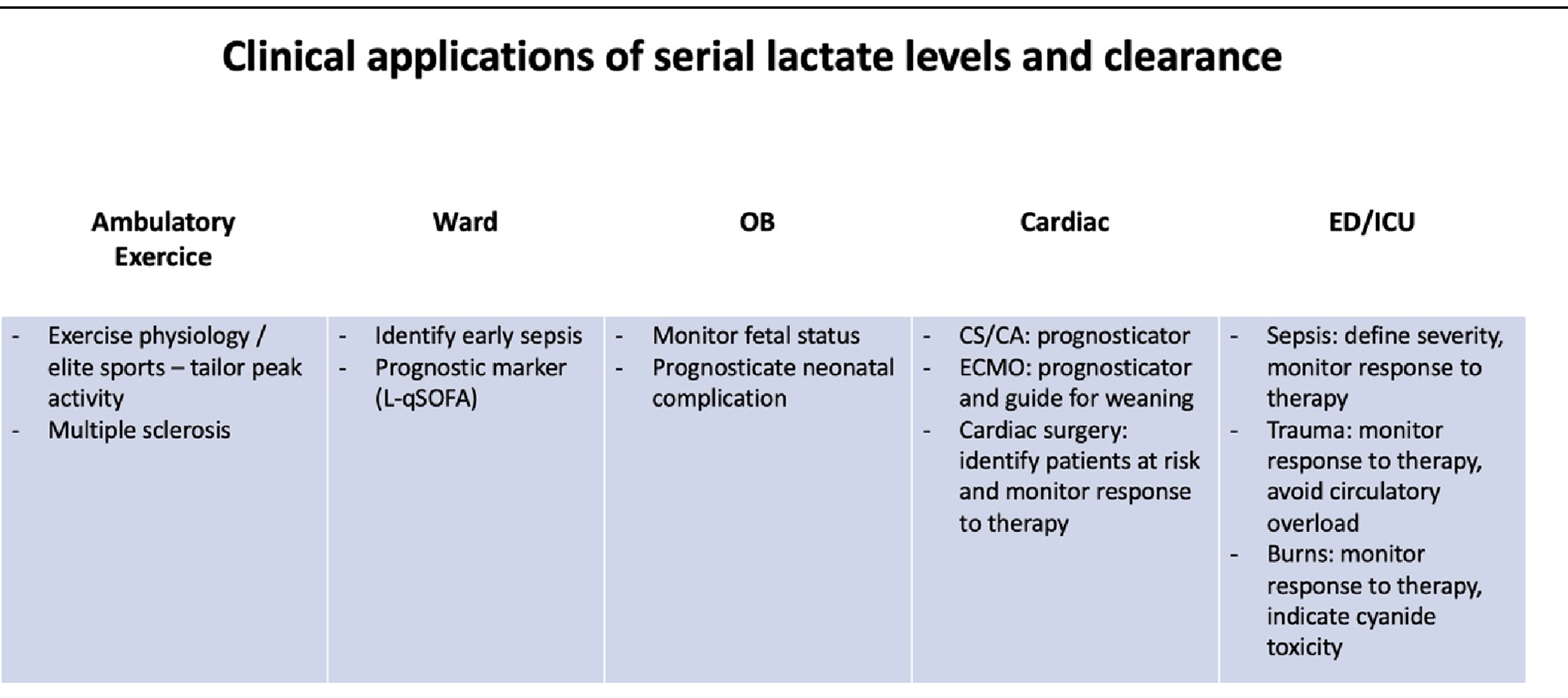
With the introduction of normalization of lactate as a goal for fluid resuscitation as part of the 2016 Surviving Sepsis Campaign bundle, 4 it has proliferated as an important tool in numerous clinical areas. 5 Most recently, lactate has become part of the International Consensus Criteria for Pediatric Sepsis and Septic shock. 6 Lactate is recognized as a marker of metabolic derangement from multiple pathological states allowing early detection of occult pathology and triggering clinical assessment and therapeutic interventions. Serial monitoring of lactate levels and clearance are particularly useful as they provide a means to assess response to therapy and guide treatment decisions. Lactate measurement is now a standard inclusion criterion in therapeutic trials of sepsis and shock. Common applications of lactate in clinical practice are shown in Table 1.
L-qSOFA – Quick SOFA Score with Added Lactate; CS – Cardiac Shock; CA – Cardiac Arrest.
Data and articles to inform this narrative review were identified by searches in MEDLINE, PubMed and EMBASE. The authors scrutinized the selected articles according to their clinical specialty. The manuscript was assembled by multidisciplinary groups according to underlying pathology. This review will focus on the clinical utility of serial lactate measurement in various clinical scenarios and its application as a prognostic and therapeutic guide.
Lactate Production and Metabolism, Lactate Clearance
Lactate production is a physiological response to physical stress. It is one of the most frequently measured parameters in clinical exercise testing as well as in training of elite athletes to tailor exercise intensity to individual needs. Its use has been expanded to evaluate severity of underlying pathology and it is recommended for stress testing. 7
Lactate is a molecule produced in large quantities during both aerobic and anaerobic metabolism with 2 main physiological properties: energy source, especially during exercise and main precursor of gluconeogenesis. Lactate production increases when cellular demand for energy exceeds its supply. It is a byproduct of glucose metabolism, glycolysis is activated when low tissue perfusion and hypoxia inhibit the tricarbocylic acid cycle, thereby stopping ATP production. Energy is produced by converting glucose into pyruvate, which is reduced to lactate. The liver and kidneys are the key contributors to lactate clearance. 8
Hyperlactatemia may arise from either insufficient oxygen delivery (type A hyperlactatemia) or from other causes not related to tissue hypoxia (type B hyperlactatemia). Another classification proposed that hyperlactatemia can be related to: (a) increased pyruvate production, including non-specific glycolysis stimulation by respiratory alkalosis, epinephrine, beta-agonists, (b) decreased pyruvate utilization leading to an increase in lactate /pyruvate ratio in hypoxemia-related hyperlactatemia and (c) decreased lactate clearance. Figure 1 provides an overview over lactate utilization in the body.
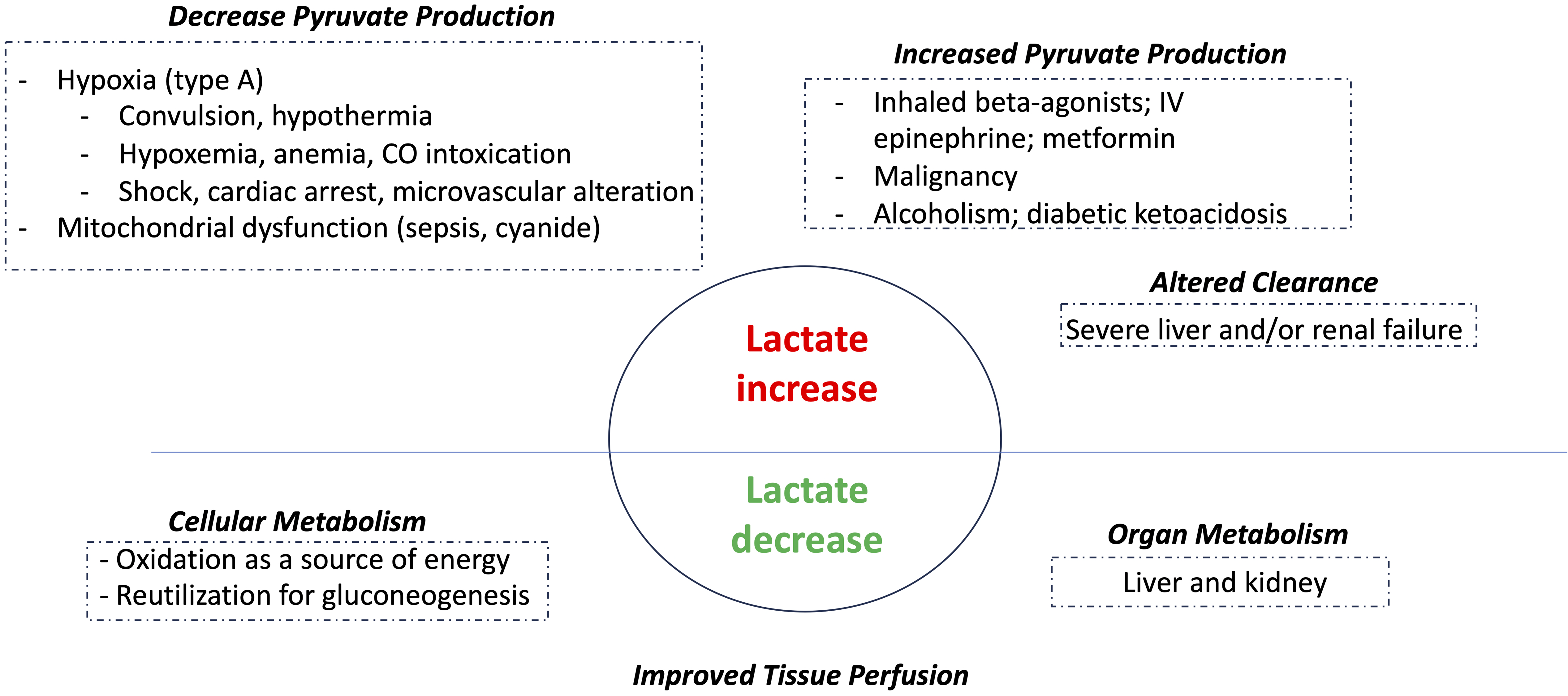
Lactate utilization.
Under physiological conditions with normal mitochondrial function, eg vigorous exercise, hyperlactatemia is not associated with acidosis. In such conditions, though glycolysis itself is acidifying, redox equivalents are utilized in the respiratory chain leading to net zero proton formation. Hyperlactatemia leads to lactic acidosis under conditions like sepsis or ischemia where hypoxia, mitochondrial dysfunction and/or renal dysfunction allow protons to accumulate causing the drop in pH.
Current State of Measuring Lactate
Although microdialysis catheters allow assessing lactate at tissue level, arterial and venous sampling is most common in clinical practice. There is a wealth of different benchtop, laboratory and point-of-care (POC), bedside devices available for measuring lactate.
Serial lactate measurements are desirable, enabling clinicians to observe the temporal course, calculate lactate clearance (lactate clearance %= (lactate initial − lactate delayed) / lactate initial × 100) and tailor therapy. Even though lactate analyzers are widely available, the current challenges in healthcare regularly lead to delays in obtaining a single result, let alone multiple measurements. This is particularly true in clinical areas / healthcare systems where lactate samples are analyzed in the laboratory. A new generation of analyzers, such as those integrated in indwelling catheters 9 or as a wearable interstitial microneedle arrays analogous to blood sugar measurement, 10 will facilitate repeated measurements and has the potential to change the landscape of utilizing lactate in clinical medicine.
Lactate Is a Clinical Tool
Lactate is a dynamic parameter and the body has excellent capacity to rapidly clear large lactate loads in situations like recovery from vigorous exercise or return of circulation after cardiac arrest. An initial measurement taken on admission to the ED or the ICU is able to raise red flags and help with risk-stratification. 3 Lactate levels taken early on during resuscitation are closely related to clinical outcomes. 11
The main utility of lactate, however, lies in serial measurements and using it for goal directed therapy. A retrospective trial in cardiac surgery has demonstrated that outcomes progressively worsen the higher the intraoperative lactate rise over time, independent of baseline 12 ; a metanalysis in 6000 patients with septic shock showed that lactate guided therapy may result in a greater mortality benefit than other early goal directed therapy. 13
The body's ability to reduce hyperlactatemia within 6 h after resuscitation is initiated has been shown to be a useful target in septic patients 14 and an effective tool for prognosticating in-hospital survival of patients with cardiogenic shock. 15
Lactate is increasingly being incorporated in risk scoring or in early warning scores. Adding it to the quick Sequential Organ Failure Assessment (qSOFA) to create L-qSOFA provides a superior tool for predicting in-hospital mortality of septic patients when compared to four other rapid assessment scores. 16
Incorporating lactate into the National Early Warning Score 2 (NEWS 2) has been shown to reduce time it took nursing staff to identify deteriorating patients and was found to be significantly superior to standard NEWS in predicting clinical deterioration in patients with dyspnea. 17 However, the complexities of obtaining lactate levels in a timely manner make this tool challenging for now.
Lactate in Cardiac Disease and Cardiac Surgery
Lactate in Acute Coronary Syndrome (ACS), Acute Heart Failure (HF)
There is good evidence that lactate is an important marker in ACS. Levels taken on admission to the Emergency Department (ED) were shown to be highly sensitive for the diagnosis of an acute myocardial infarct, particularly in patients with a history of more than two hours of chest pain. 18 As well as being a potential diagnostic tool, lactate provides valuable prognostic information. In a cohort of 1179 patients admitted for percutaneous coronary intervention (PCI) with a clinical diagnosis of STEMI (ST elevation myocardial infarction), those in the highest lactate tertile (≥1·8 mmol/l) had the highest 30-day mortality and double the number of patients requiring an intra-aortic balloon pump compared to the middle tertile (4·7% vs 7·6%). 19 The prognostic power extends to patients admitted with ACS with only mild symptoms of heart failure (Killip class II and III) and without cardiogenic shock. Mortality was 28% in those with admission lactate ≥ 2·5 mmol/l compared to 5% when lactate was < 2·5 mmol/l. 20
In patients with end-stage HF requiring left sided ventricular assist device (LVAD) insertion, 75% have normal lactate levels despite 93% showing a widened arterio-venous O2 difference. 21 Once a VAD has been implanted, post-operative hyperlactatemia – even if observed in the first 24 h - is associated with increased rates of re-operation, multiorgan failure and higher 90-day mortality. 22
Similar findings are true for acute heart failure patients treated medically. Patients presenting without signs of hypoperfusion, but elevated lactate (> 2 mmol/l) had a significantly higher mortality within the first year (HR 1·24) than those with normal lactate levels. 23
Lactate in Cardiogenic Shock (CS) and Cardiac Arrest (CA)
Despite recent advances in therapy, CS remains associated with poor outcomes. 24 This has not changed with the now available arsenal of percutaneous mechanical circulatory support devices and their ability to significantly improve haemodynamics. 25 Elevated lactate levels are an independent predictor of in-hospital mortality in patients with and without CS or CA. 26 Another recent study demonstrated that a second arterial lactate measured eight hours after admission was superior in mortality prediction compared to admission lactate only. 27
Lactate and ammonia measured on arrival in the ED after out-of-hospital CA had a nearly 100% positive predictive value; a lactate level of <5 mmol/l was associated with 39% mortality, rising to nearly 100% when > 10 mmol/l. Several studies have found an association between lactate levels and neurological outcome after CA. While initial levels of <5 mmol/l were predictive of normalizing Glasgow Coma Scale values, 28 neurological outcomes were significantly better the higher the lactate clearance, as determined by serial measurements at 6, 12, 24 and 48 h after admission. 29
Lactate in Extracorporeal Life Support (ECLS) for CS
Veno-arterial extracorporeal membrane oxygenation (VA ECMO) is a potentially lifesaving therapy but remains associated with poor outcomes. The Extracorporeal Life Support Organization registry reports around 40% mortality. When using serial measurements, the time taken for lactate to reduce by 10% after ECMO initiation is a strong discriminator for mortality. 30 These findings have been replicated by a study showing that lactate clearance is an independent predictor of 30-day prognosis. 31 For every 1% per hour increase in lactate clearance, survival increases by 16%.
A post-hoc analysis of the HYPO-ECMO trial revealed the pivotal prognostic relevance of serial lactate measurements in patients on ECLS for CS. Patients failing to significantly decrease lactate levels within the first 24 h after ECMO commencement have a higher 30-day mortality, which increases further when there is a second peak within 7 days. 32
Lactate in Cardiac Surgery
Hyperlactatemia and lactic acidosis are common sequelae of cardiac surgery and cardiopulmonary bypass. The relationship between serial lactate and adverse outcomes has been confirmed in multiple studies.33,34 A 8000 patient study analysing the highest lactate level within the first 3 postoperative days found that the degree of lactate rise directly correlated with 30-day mortality. 35 Measuring serial lactate in the first 24 h after cardiac surgery has also shown that levels of 3 mmol/l or more are associated with increased 30-day and long-term mortality. 36
Elevated lactate is a challenging finding to interpret and to act on, as the underlying etiologies vary during and following cardiac surgery. To better address this challenge, classifying hyperlactatemia based on time of presentation in the perioperative period has been found useful both for prognostication and management.
Lactate in Congenital Heart Disease
Blood lactate has been used as a marker of tissue oxygen debt, and of importance in monitoring brain and myocardial tissue perfusion. In neonates and children undergoing surgery for congenital heart disease, serial measurement is predictive of neurodevelopmental and cardiac outcomes as well as other adverse outcomes including death, use of ECMO or dialysis.37,38
Lactate in Trauma
Shock is common in severely injured patients. The most common cause of shock is hemorrhage, which rapidly leads to tissue ischemia and a lactic acidosis. Young and healthy trauma patients may present with pseudo-normal physiology, compensating for occult blood loss, until they rapidly deteriorate. During this period of compensation, lactate levels can be useful to detect the underlying occult hypoperfusion. 48 Serial lactate levels are used for determining the severity of shock and adequacy of resuscitation. A particular feature of patients suffering severe injuries is that, unlike other groups of patients included in this review, they are likely to undergo multiple operative interventions as part of their clinical management and suffer all the associated physiological stress.
Initial lactate measurement before arrival in hospital improves prediction of the need for major trauma activation, 49 urgent surgery, development of multiple organ failure, and death. 50 Lactate levels predict the need for resuscitative care 51 even in normotensive patients. 52 When added to clinical scoring tools lactate levels improve trauma level activation appropriateness. 49
Lactate levels on admission to hospital correlate with Injury Severity Scores 53 and need for blood transfusion, 54 even in patients with normal haemodynamics. Elevated lactate levels correlate with an increased risk for mortality in both adults55–57 and children.58,59 In this regard, lactate may be better than base deficit, another biomarker for severity of shock. The predictive value of lactate and base deficit does not appear to be influenced by alcohol or illicit drug use, 60 common in trauma patients.
The most recent consensus statement from the American Association for the Surgery of Trauma emphasizes the use of lactate levels during resuscitation. They suggest adjuncts like POCUS and APWA to complement the use of lactate levels. 61
Lactate levels should normalize if the resuscitation is timely and sufficient. Rate of clearance correlates with survival.62,63 Persistently elevated lactate levels within the first 24 h have been shown to predict mortality.64–66 Deteriorating lactate clearance is an independent predictor of increased mortality. 67
As lactate levels normalize, reducing fluid resuscitation / transfusion should be considered to avoid circulatory overload. 61
Trauma patients often undergo multiple operative procedures. Increased lactate levels post-surgery in elderly trauma patients predict both mortality and delirium. 68 Lactate clearance may aid in predicting recovery from bowel repair post injury. 69
Lactate in Burns
Major burn injury results in acute distributive shock with substantial intravascular fluid depletion in the first 24 h. Burns trigger an immediate inflammatory response that, unlike in sepsis or trauma, continues even after the initial endpoints of resuscitation have been reached.
Burn resuscitation cantered on formulaic fluid prescriptions targeting urine output 70 can lead to secondary complications such as poor gas exchange, fluid creep and compartment syndromes. 71 This has not only led to a change in the fluid combinations used, but also to the search for new goals to direct resuscitation. 72 Using serial lactate levels as the resuscitation goal can help reduce the total fluid volume in a safe and effective manner.73,74 Lactate by itself and or in combination with other biomarkers (eg, lactate / albumin ratio) has been shown to be useful in predicting short term outcomes after major burns.75,76
Measuring lactate levels (both peak values and rate of clearance) in patients with smoke inhalation injury can help predict the risk of developing ARDS. Persistent hyperlactatemia should alert clinicians to the possibility of cyanide exposure.74,77
Lactate and The Central Nervous System (CNS)
Our understanding of the role of lactate in the CNS has evolved over the last decade and the role of lactate in CNS pathology is now viewed beyond the lens of volume resuscitation. It is worth noting that there is no correlation between CSF lactate and cerebral blood flow or CSF lactate and blood lactate levels. 78
CSF analysis remains the cornerstone of diagnosing meningitis. CSF lactate can differentiate bacterial meningitis (>6 mmol/l), from partially treated meningitis (4-6 mmol/l) and aseptic meningitis (< 2 mmol/l).
Mild elevation of serum and CSF lactate are seen after seizure activity. The incidence and intensity of lactate spikes is dependent on multiple factors such as the type of epileptic disorder (status epilepticus or focal vs generalized seizures, motor vs nonmotor seizures). Hyperlactatemia was found in 24% of patients after single seizures and in 28% after status epilepticus. Elevated lactate levels more than six hours after the seizure may indicate ongoing epileptic activity or may prompt the clinical team to consider other causes. 79
Multiple sclerosis (MS) is a primary inflammatory demyelinating disease associated with progressive neurodegeneration. Impaired mitochondrial function has been hypothesized to drive neurodegeneration. Lactate levels are reported to be higher in patients with progressive MS compared to those with a relapsing–remitting variant. There is a suggestion that serial lactate measurements can help inform an MS patient's response to therapy. 80
Lactate in Liver Transplantation
The liver is the main site of gluconeogenesis from lactate. About 70% of circulating lactate are metabolized back to glucose there via the Cori cycle. Of the remaining 30%, 25% are metabolized in mitochondria rich tissues and 5% in the kidneys. 81
Patients with chronic liver disease often have elevated lactate levels. In patients with liver cirrhosis, lactate levels on admission to ICU are notable higher and clearance up to 50% lower in those who died within 28 days compared to survivors. 82
The same principle is true in liver transplantation. A 6-year review of 226 patients found that the lactate concentration measured immediately after post-operative ICU admission was associated with an increased 1-year mortality with an odds ratio of 1.25 (p < 0.001) per mmol/l increase; the cutoff was 2.25 mmol/l. 83 A bigger retrospective study with 1137 included patients, however, was not able to replicate these findings and concludes that, due to the complex nature of the disease and the procedure, a lactate alone is not a good predictor of poor outcomes after liver transplantation. 84
In another retrospective study involving 265 patients delayed early lactate clearance has been shown to be a strong predictor for early allograft dysfunction. The incidence of graft dysfunction and 1-year survival were 23% and 96% respectively in the group with normal lactate clearance, compared to 50% and 78% respectively in the delayed clearance group. 85
Lactate in Sepsis and Septic Shock
Managing sepsis requires swift identification and urgent intervention. Early recognition of septic patients using established scoring systems is crucial to reduce preventable deaths and improve morbidity, functional outcomes and resource utilization.
Patients with suspected sepsis benefit from serial lactate measurements, even if they are normotensive with stable haemodynamics, as recommended by the Surviving Sepsis Campaign guidelines. 86 As the clinical course of sepsis is variable, serial lactate measurements will help identify positive response to therapy or patient deterioration and need for ICU admission.87,88
The pathophysiology of sepsis is complex and varied, which often requires the use of multiple biomarkers to provide precise information. Elevated initial lactate levels >2 mmol/L, however, have been independently associated with increased mortality in patients presenting to ED with septic shock. 89 Furthermore, in many trials, lactate greater than 2 mmol/L is needed to define septic shock in a patient suspect of sepsis regardless of haemodynamics.
Establishing the severity using the SOFA score shows high prognostic accuracy in sepsis and septic shock but is challenging to obtain, particularly in low- and middle-income countries. The qSOFA score uses bedside observations and is increasingly being used to identify high-risk patients outside of ICU. Combining lactate measurement with the qSOFA score (L-qSOFA) can identify those at risk of death with greater accuracy than the qSOFA score alone. 90
The recent Phoenix Sepsis Score includes lactate as a marker of organ dysfunction and is a consensus tool for stratifying risk of mortality in children with suspected sepsis and septic shock. 6
Measuring serial lactate levels and lactate clearance in ICU offers numerous benefits in the management of critically ill patients. Rapid decreases in lactate levels indicate an appropriate response to treatment and suggest improved tissue perfusion and oxygen delivery.
Measuring lactate levels and calculating lactate clearance at 3–6 h is likely to assist defining patient prognosis more precisely than using one single measuring point. Six-hourly lactate levels of ≥3.5 mmol/L and 6-h lactate clearance of <24.4% were identified the optimal cut-off value in predicting 30-day mortality. 91 Tracking changes over time, healthcare providers can evaluate the response to treatment and adjust therapeutic strategies accordingly.
Sepsis Management on the Ward
Sepsis management outside the ICU remains challenging. It is recognized that mortality for sepsis patients treated outside the ICU is higher, ranging from 10% to 25%. 92 Several factors contribute to this, including delays in recognition, reduced monitoring frequency, underestimation of severity, resource limitations and delays between recognition and treatment initiation. This is further exacerbated by staffing difficulties, particularly at night.
Lactate levels offer a role in optimising evaluation and management of patients with suspected sepsis. In the ward setting, lactate can signal potential worsening of sepsis, prompting changes in therapy, surgical intervention or transfer to a higher level of care.
Earlier detection and treatment of sepsis has been shown to improve outcomes. 4 Elevated lactate can precede the manifestation of clinical symptoms, serving as an early warning sign of worsening sepsis. 93 Tracking lactate can facilitate earlier intervention and help assess response to therapy. Recent research suggests that early detection of patient deterioration, facilitated by continuous vital sign monitoring, can reduce mortality and ICU transfers compared to intermittent monitoring. 94
Delays in obtaining lactate levels may arise from prolonged phlebotomy response times and laboratory turnaround. Wider availability of appropriately calibrated bedside devices (POC or wearables) may alleviate the shortcomings in ward care, which could benefit patients with hyperlactatemia from other conditions.
Lactate in Obstetric Medicine
Fetal surveillance during labor is based on fetal heart rate recordings with cardiotocography (CTG), a method with high sensitivity but low specificity for fetal distress. To improve specificity and reliably, many departments have introduced intrapartum lactate measurements through fetal scalp blood sampling (FBS). Hypoxemia drives centralization of the fetal circulation, making capillary scalp blood a good site to detect hyperlactatemia early. 95 Careful sampling is possible once the amniotic membranes are ruptured and the cervix is dilated to 3 cm or more and the fetal scalp can be exposed transvaginally with an amnioscope.
In the presence of CTG abnormalities, FBS helps to guide timing of delivery. Multiple sampling allows clinicians to assess fetal status and safely guide timing and mode of delivery. 96
The two randomized controlled trials comparing pH versus lactate analyses Favor the latter with a trend towards better neonatal outcome. This is attributed to quicker sampling, less sampling and/or analysis failure and a shorter draw to result time.97,98 A 2015 Cochrane review 99 and the 2022 NICE Guideline NG229 support fetal lactate measurements when indicated. 100
Umbilical arterial blood lactate sampling after delivery is an effective tool for evaluating the management of labor, estimating the severity of birth academia and predicting neonatal complications including hypoxic ischemic encephalopathy. 101
Limitations
Utilization of lactate monitoring is supported by evidence but has limitations.
First, not all patients who could potentially benefit from lactate monitoring are tested due to delays in recognition in deterioration.
Second, availability of nurses or phlebotomists and access to analyzers compound the delays caused management of the sample, laboratory workflows/logistics, and ultimately result notification and integration into the patient electronic record.
Third, there remains the need for standardization and calibration across the various lactate analyzers, which can differ by up to 50% in their readings. 102
Fourth, clinicians need to be mindful of the challenges of interpreting lactate levels. Critical situations such as reperfusion and acute organ dysfunction as well as exposure to certain drugs such as metformin, epinephrine, lactated ringers, and propofol and malignancy or chronic liver/renal failure impact lactate.
Future Perspectives
As serial lactate measurement is increasingly used in clinical medicine, the call for ready and easy availability independent of staffing or device constraints will grow louder. Wearable devices providing continuous lactate readings and able to communicate with patients’ electronic medical records and early warning scores are likely to help decrease the number of hospitalized patients suffering delayed initiation of therapy only after they have clinically deteriorated. Telemedicine using wearables potentially offer remote monitoring at home to patients who would otherwise be kept in hospital. Subsequent earlier discharge from hospital or the ED might help healthcare providers to use available resources more efficiently.
Summary
Measuring serial lactate levels and determining lactate clearance offers several benefits including prognostic value, early detection of sepsis, goal-directed treatment strategies and regular feedback on response to therapy. Particularly on the ward, serial lactate monitoring can via indwelling devices integrated in the hospital IT environment have the potential to reduce the number of blind spots between nursing observations, thus making it easier to identify deteriorating patients early.
Advances in wearable device technology and telemedicine are promising to simplify lactate monitoring and integration into electronic patient records and early warning scores.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Falter, Kumar and Liu are members of the Abbott Diabetes Care scientific advisory committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this manuscript was supported with an educational grant [Ref: 4701131153] by Abbott Diabetes Care, paid to into the research account Florian Falter holds at Royal Papworth Hospital, Cambridge, UK. None of the authors received an honorarium.
The funder had no role in the study design, data collection, analysis or interpretation. They did not have a role in the decision to publish or in the preparation of the manuscript.