
Abstract
Keywords
Introduction
Approximately 100 000 critically ill patients receive both tracheostomy and gastrostomy tubes in the United States every year. 1 The ability to perform bedside tracheostomy and gastrostomy safely in Critical Care Units (ICU) has been well researched for the past 3 decades. Broadly, however, the research has analyzed these procedures independently and with limited consideration of their relationship.2–5 Given the frequent co-indication of tracheostomy and gastrostomy in patients with Ventilator Dependent Respiratory Failure (VDRF), recent research has investigated the benefits of a combined approach to these procedures.6–10 Importantly, earlier placement of gastrostomy tubes after tracheostomy is associated with decreased ICU LOS, hospital LOS and total hospital costs.6–9
At our institution tracheostomy and gastrostomy procedures have traditionally been performed by different services. Percutaneous tracheostomies are typically performed at the ICU bedside by a traveling service and the neurointensivist team on the Neurocritical Care Unit (NCCU). Until recently, none of our critical care teams had training or access to bedside gastrostomy methods. Critical care teams relied on consultation for Percutaneous Endoscopic Gastrostomy (PEG) and Percutaneous Radiographic Gastrostomy (PRG). These methods typically require scheduling and transport to the operating room (OR) or specialty suite at our institution. Due to the unstable nature of critically ill VDRF patients, and the associated difficulties coordinating procedure time and specialists in the OR and suites, gastrostomy tube placement was frequently postponed.
To alleviate coordination challenges, our institution adopted the PUMA-G System (CoapTech, Inc., Baltimore, MD) for Percutaneous Ultrasound Gastrostomy (PUG) placement. PUG is a bedside gastrostomy method shown to be safe and effective in the hands of critical care providers, including when performed concomitantly with bedside tracheostomy.7,11,12 Because PUG may be used by intensivists skilled in point-of-care ultrasound (POCUS), it is less subject to delays in care than other gastrostomy methods due to its point of care design and minimal equipment requirement. Our traveling service team of critical care providers and neurointensivist team performing bedside tracheostomy were trained in PUG in the summer of 2022. This group included 5 attendings and 2 Advanced Practice Providers (APP) with backgrounds in Trauma, Medicine, Surgery, and Neurocritical Care. The training process adopted, that had been successfully implemented at other institutions utilizing the PUMA-G System, required providers to complete an online PUG safety course and perform three or more PUG procedures on human sized training torsos provided by the company. Subsequently the trainee could proceed to bedside PUG cases, and to receive full credentialing, needing to complete 5 successful PUG cases proctored by a CoapTech clinical specialist or a provider credentialed in PUG.
Based on authors’ experience, our team hypothesized that implementing a combined ICU bedside percutaneous tracheostomy and PUG service across our hospital would reduce ICU length of stay (LOS) due to timely gastrostomy placement. In addition, we hypothesized that improved efficiencies in care would reduce hospital costs and overall hospital length of stay for patients with VDRF. We compared the characteristics and outcomes of VDRF patients requiring gastrostomy in a pre- and post- PUG team implementation efficiency study. To our knowledge, our team is the first to evaluate the impact of a centralized ICU bedside service for combined tracheostomy and ultrasound gastrostomy.
Methods
IRB approval was received from University of Miami to perform a retrospective chart review study comparing the impact of implementing an ICU bedside PUG service with the hospital's previous workflow (pre-implementation) at Jackson Memorial Hospital (JMH). JMH is one of the largest hospitals in the United States, a 1500+ bed, academically affiliated hospital within a large public health system in Florida. The first PUG procedure was performed on August 30, 2022, and therefore defined as the initial implementation date.
Patients indicated for both tracheostomy and gastrostomy while admitted to an ICU during the pre- and post-implementation periods from September 2021 through May 23, 2023 (ie, date range of IRB application approval) were included in the study. All PUG patients were evaluated for inclusion and the electronic medical record system (Cerner™) was queried for encounters in which patients were admitted to an ICU and had a documented ICD-10 code for gastrostomy prior to August 30, 2022, the implementation date. Further chart review was performed to assess patient inclusion criteria and extract clinical and patient demographic data. The institution's cost accounting system was queried for all hospital costs (ie, not charges) resulting from patients’ admissions.
A total of 273 patients who received gastrostomy at any time during the study period were examined for study inclusion. Of these, 172 patients were excluded from the analysis for not meeting study inclusion (eg, pre-existing tracheostomy or gastrostomy prior to ICU admission, or had no tracheostomy placed). To eliminate any impact of prior workflows, and enforce a washout period, twelve patients were excluded from the post-implementation group (ie, PUG group) because they were admitted prior to the date of PUG implementation. 2 and 2 patients, respectively, were excluded from the pre-implementation group and the PUG group for having length of stay or total hospital cost values greater than 3 standard deviations above study group averages.
Average ICU LOS, hospital LOS, and total hospital costs were calculated in assessing efficiency benefits of implementing a bedside percutaneous tracheostomy and PUG team. Patient demographics and clinical characteristics, such as ICU admission type, age, gender, APR-DRG severity weight (an administrative acuity classification incorporating admission diagnosis, severity of illness, and risk of mortality), inpatient mortality, COVID status and discharge disposition were compared between groups. Operational metrics were analyzed, such as average time from procedure indication or consultation to procedure completion. One-tailed t-tests were used to compare parametric continuous variables between the groups. Chi-squared tests were used to compare categorical variables between the groups. Prism statistical software (v. 10.1.1, GraphPad) was used for all analyses with a significance level of 0.05.
Results
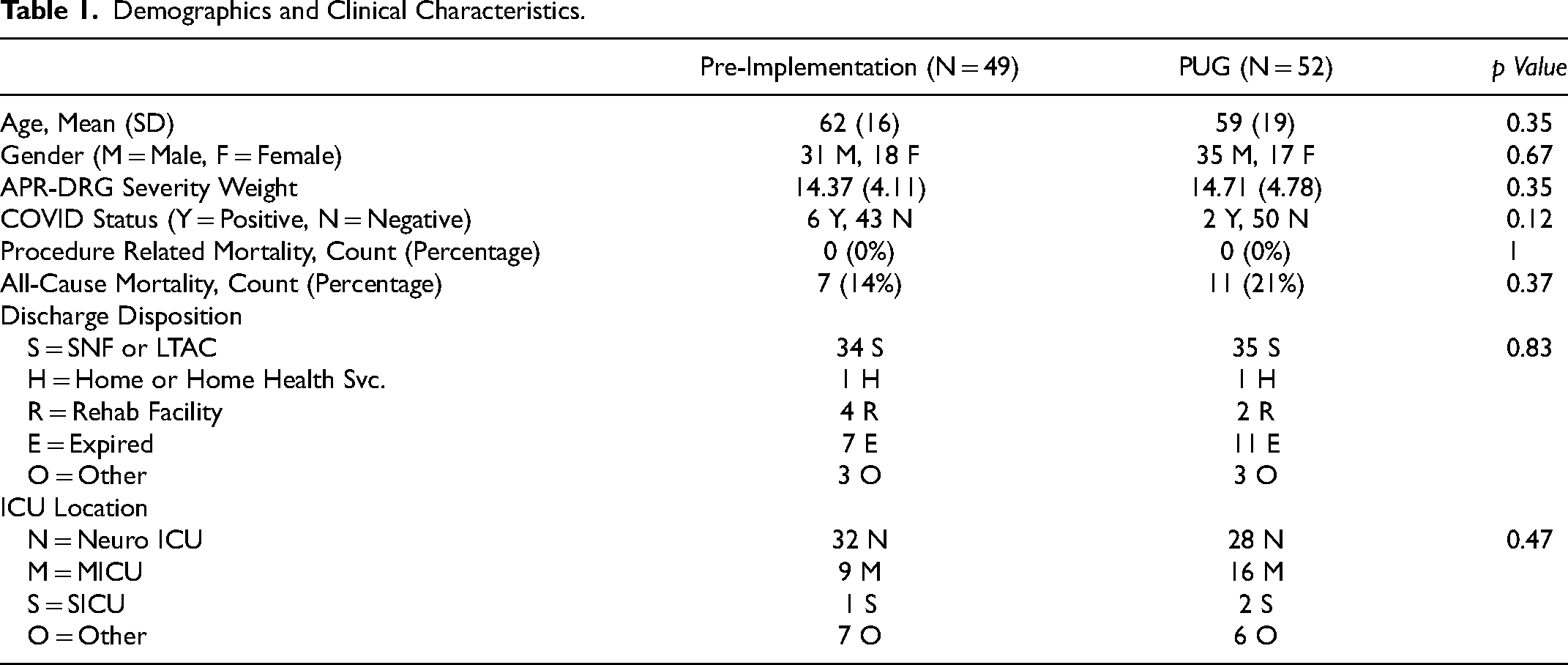
A total of 101 adult critically ill patients with VDRF received percutaneous tracheostomy and gastrostomy over the 20-month study period and were included in the analysis. 49 patients were included in the pre-implementation group and 52 patients in the PUG group. Table 1 demonstrates no significant differences were observed between both groups in mean age, gender, APR-DRG severity weight, COVID status on admission or ICU location type (Neuro ICU, MICU, SICU, Other).
Demographics and Clinical Characteristics.
The primary outcome comparisons of ICU LOS, hospital LOS, and total hospital costs are detailed in Table 2. PUG group patients had a significantly shorter mean ICU LOS (37.6 vs 48.5 days, p = 0.010) and spent on average 10.9 fewer days in the ICU compared to the pre-implementation group. PUG group patients also had a shorter mean hospital LOS (49.2 vs 63.9 days, p = 0.006) and spent on average 14.7 fewer days in the hospital. For PUG group patients, total hospital costs were significantly lower ($222 978 vs $257,756, p = 0.043), with an average difference of $34 778 in cost savings per patient.
Primary Outcomes.

There were no procedure-related mortalities in either group. No significant difference in in-hospital, all-cause mortality (14% in the pre-implementation group vs 21% in the PUG group, p = 0.37) was observed. There were no PUG “failures” requiring gastrostomy by another method, but in our initial patient evaluation process we did defer on two patients due to lack of a window. Lack of an adequate safe potential track for tube insertion is a concern common to PUG, PEG, and PRG and such cases are commonly referred for surgical gastrostomy tube placement. Although this study was not powered or designed to study safety, the ability to visualize abdominal organs using POCUS likely decreases the possibility of unintentional organ injury. No differences in discharge disposition were observed with most patients discharged to Skilled Nursing Facilities (SNFs) and Long-term Acute Care Hospitals (LTACHs).
Additional operational efficiency metrics regarding tracheostomy and gastrostomy procedure timing are compared in Table 3. Time from tracheostomy completion to gastrostomy completion (15.3 vs 6.8 days, p = <.001) and time from gastrostomy indication to gastrostomy completion (10.3 vs 3.6 days, p = <.001) were reduced by 8.5 and 6.7 days, respectively. Additionally, significant differences were observed in time from ICU admission to gastrostomy indication, and ICU admission to gastrostomy completion. 15% of patients in the PUG group had a concomitant bedside tracheostomy and gastrostomy procedure, while no patients in the pre-implementation group received concomitant bedside tracheostomy and gastrostomy (p = <.001).
Gastrostomy Related Efficiency Metrics.

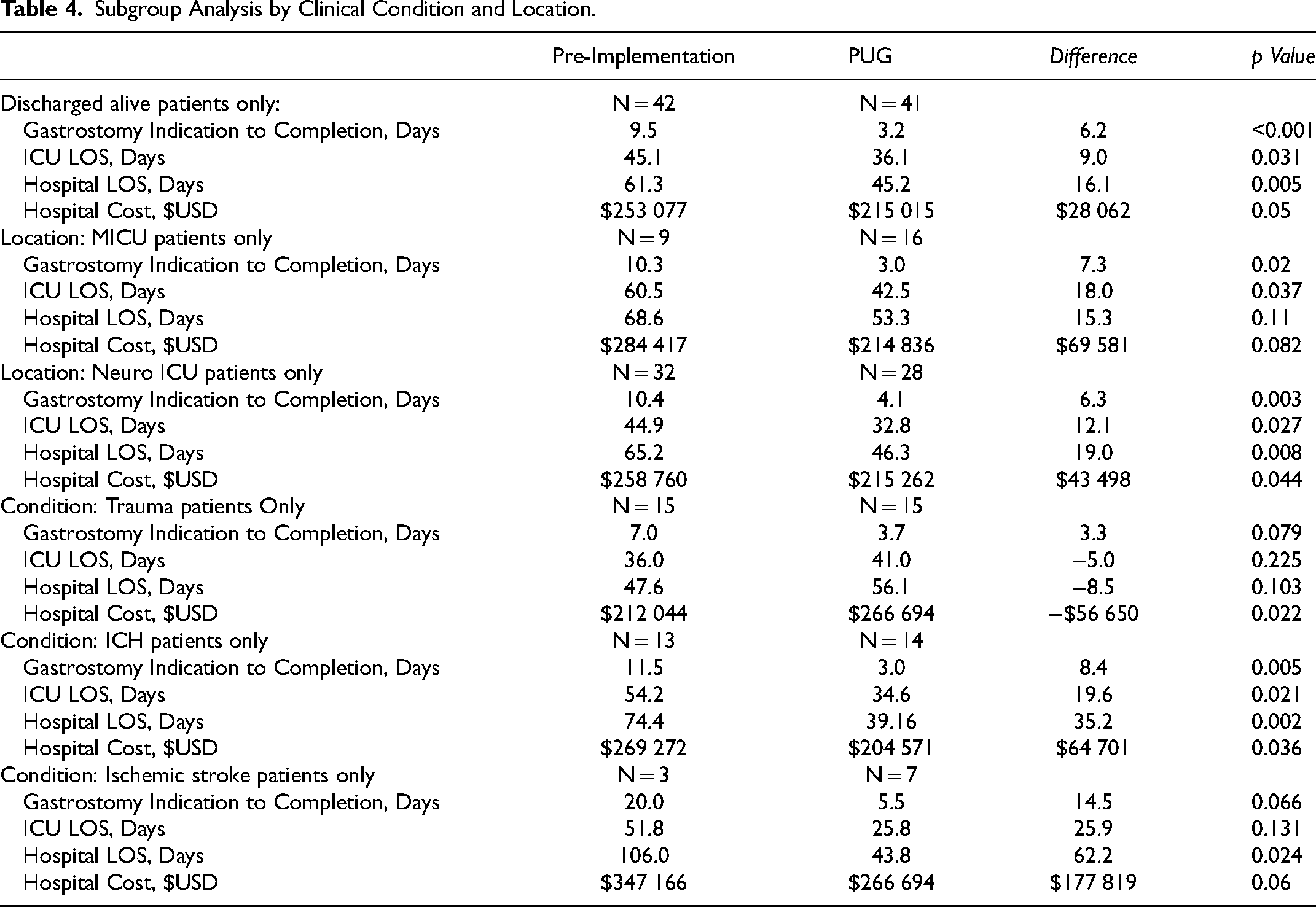
Subgroup Analysis by Clinical Condition and Location.
Discussion
Our study supports implementing a bedside percutaneous tracheostomy and PUG team to reduce ICU LOS, hospital LOS and total hospital costs in patients with VDRF. All study outcomes of interest were significantly different between the groups. Time from indication to completion of gastrostomy, ICU LOS, hospital LOS and total hospital costs were all found to be significantly decreased in the PUG group. Extrapolating this $34 778 per patient cost savings to the full PUG procedure group would result in an annual hospital cost reduction of $2.96 million at JMH ($34 778 × 64 × 12/9). Furthermore, decreasing ICU LOS and hospital LOS improves all patients’ care, by increasing availability of ICU and hospital beds for other acutely ill patients. Most poignant are delayed admission transfers of critically ill patients from the Emergency Department (ED), which are associated with higher in-hospital mortality. 13 Annualizing these results would have saved 915 ICU bed days and 1235 hospital bed days which would benefit patients in our health system awaiting transfer from the ED or elsewhere.
Bedside PUG performance was faster, occurring within an average of 3.6 days after documented need in the medical record, compared with greater than 10 days when suite or O.R. scheduling was practiced. Time from tracheostomy to gastrostomy also dropped on average by nearly 9 days, with 15% placed concomitantly in the PUG group. Furthermore, in the implementation (PUG) group, time from ICU admission to gastrostomy indication was also reduced by 6.7 days. These metrics suggest that PUG implementation was associated with both an increased clinical efficiency, as well as a more proactive approach to long-term enteral feeding. Our experience was that, like bedside tracheostomy, enabling critical care teams to perform PUG dramatically streamlined our workflows. In simple terms, by giving the bedside team control of the procedure, it was done faster. Furthermore, our critical care teams were empowered to initiate the procedure sooner in the care continuum, including concomitant to tracheostomy.
There were no significant in-hospital mortality differences between groups and mortality did not impact primary outcome measures on subgroup analysis (Table 4). The observed in-hospital mortality rates for both groups are consistent with literature reported rates, in-range with cited inpatient and 90 day mortality rates of patients with tracheostomy and gastrostomy tubes, 9.7% and 40% respectively. 1 The PUG group's greater in-hospital mortality rate (21% vs 14%) is consistent with existing literature, where observed results in retrospective tracheostomy and gastrostomy studies suggest that when timing of placement is decided upon by a physician, selection bias is introduced. Hochu et al observed a doubling of the in-hospital mortality rate when comparing concomitant procedures with “delayed” gastrostomy controls (ie 11% and 5.5%, respectively), with controls observed to have lower injury severity scores and better neurological status. 9 Prior to PUG implementation, physicians may have naturally excluded sicker patients from receiving gastrostomy. In our study, the pre-implementation group's delay to gastrostomy tube placement was on average 15 days after the tracheostomy, a timeframe in which critically ill patients in this group could have died before gastrostomy. Importantly, in-hospital mortality did not impact primary study outcomes. A subgroup analysis demonstrated the same statistically significant reductions (p < 0.05) in LOS and cost metrics (ICU LOS 45.1 vs 36.1, Hospital LOS 61.3 vs 45.2, Total Costs $253 077 vs $215 015) when excluding patients with in-hospital mortality. Therefore, the PUG group did not demonstrate statistical benefit due to having a 7% higher in-hospital mortality artificially decreasing LOS and hospital cost.
To our knowledge, this is the first study demonstrating a team of providers performing bedside percutaneous tracheostomy and PUG across multiple ICUs. Our team covered 6 ICUs including the trauma, medical and neuro critical care units within our 1500+ bed tertiary care center. The PUG procedure had a relatively straightforward learning curve and multiple members of the team were present for initial procedures to aid in competency building. Other authors have studied the benefits of concomitant procedures for patients and the health system including fewer patient handoffs and transport, minimizing exposure to isolation patients, minimizing scheduling complexity, and subjecting patients to a single instance of anesthesia.6,7,9 The efficiency metrics identified in this study suggest the improvements in lengths of stay are a result of the PUG team program enabling our care teams to become both more proactive in caring for critically ill patients, as well as more efficient in their workflow.
We appreciate that our 15% concomitant rate is well below other authors’ experience with PUG implementation. For example, Marshall et al demonstrated a 70% concomitant rate, however, their data was in a single mixed ICU setting. In our multi critical care unit system, providers were performing tracheostomies without PUG privileges (ie were not on the study team) and this led to a lower number of concomitant procedures. As more providers are trained in both tracheostomy and PUG we expect our concomitant rate to increase to levels demonstrated by other authors. Concomitant bedside tracheostomy and gastrostomy has other benefits besides timeliness, such as decreased total sedation, decreased care handoffs and decreased interrupts in medications and nutrition, therefore we expect our efficiency metrics and outcomes to further improve with a global concomitant approach.
We are the second study to demonstrate decreased ICU LOS and hospital costs in a mixed-ICU population of VDRF patients due to implementation of percutaneous ultrasound gastrostomy. 7 Other specialty-focused neurocritical care and trauma critical care studies have shown similar benefits, but have not considered general medical and surgical patients.6,8,9 Our PUG patients were from different ICUs with proportions of 31% medical, 54% neuro, 4% surgical and 11% other.
Subgroup analysis was performed based on both ICU location and clinical condition. Most findings continued in line with the primary analyses, with either statistical significance or strong trends in the various subgroups showing improved efficiency and cost outcomes in the PUG group. For example, the medical ICU subgroup demonstrated decreased LOS and costs (ICU LOS 60.5 vs 42.5 days, p = .037; hospital LOS 68.6 vs 53.3, p = 0.11; $284 417 vs $214,836, p = .082) with a significant decrease in ICU LOS in the PUG group. Interestingly, trauma was the lone clinical subgroup that did not see significantly improved time from g-tube indication to completion. ICU and hospital LOS were not significantly different in pre-post comparisons for trauma, but hospital cost was seen to be higher for the PUG group in trauma patients only. This trauma subgroup analysis provides interesting ground for a future study in our trauma patient populations, as it is not consistent with Hochu's findings of significantly shorter hospital LOS of 7 days in a trauma population receiving concomitant tracheostomy and gastrostomy procedures. 9
Limitations exist in a single center retrospective pre-post implementation study design. Lack of randomization and lack of provider blinding could interject bias in a study of this kind. As a retrospective study however, providers performing procedures pre- and post- implementation did not know they were being studied, an advantage which overcomes the Hawthorne Effect often seen in operations research. The study period did overlap with the tail end of the COVID-19 pandemic, but there was no statistical difference in COVID infections between the groups, with both group percentages low. All the subgroup analyses result in lower numbers of included patients and therefore reduced statistical power, where a small number of large data points can sway results. These subgroup analyses envoke intrigue and provide foundations for future inquiries with larger study groups.
Despite these limitations, our study, and other work by Marshall and Nobleza, supports a model of timely ICU bedside placement of tracheostomy and gastrostomy in patients with VDRF.6,7 Our team has continued to employ this model with increased focus on concomitant tracheostomy and gastrostomy.
Future work should focus on clinical outcomes not related to efficiencies in care, such as effects on patients’ nutritional status, conditioning, and ICU mortality across ICUs that employ concomitant tracheostomy and gastrostomy for all VDRF patients. Furthermore, future research should readdress the timing of tracheostomy, as prior work assessing the benefits of early versus late tracheostomy did not study the important relationship between tracheostomy and timely gastrostomy in patients with VDRF.14–16
Conclusion
This study supports implementing a bedside percutaneous tracheostomy and PUG team to reduce LOS and hospital costs within ICUs not already performing these procedures in an efficient manner. Bedside tracheostomy and PUG significantly reduced ICU LOS, hospital LOS and hospital costs, a per patient savings of $34,778, in patients with VDRF. We will continue to implement our team across our health system's ICUs and support future studies to determine other potential clinical benefits of concomitant bedside tracheostomy and PUG care models.
Footnotes
Acknowledgements
The authors would like to acknowledge the compassionate multidisciplinary care provided by the critical care clinical teams at Jackson Memorial Hospital.
Declaration of Conflicting Interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by CoapTech, Inc. to Jackson Health System to cover IRB fees and time and effort for Drs. Atallah and Patel to complete data collection activities. No other author(s) received financial support for the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by CoapTech, Inc. to Jackson Health System to cover IRB fees and time and effort for Drs. Atallah and Patel to complete data collection activities.
No other author(s) received financial support for the research, authorship, and/or publication of this article.