
Abstract
Introduction
Approximately 250,000 gastrostomy tubes are placed in the United States every year and at least 50% of gastrostomy tubes placed are in the critically ill patient population.1,2 The most common methods for placing gastrostomy tubes in critically ill patients are percutaneous endoscopic gastrostomy (PEG) and percutaneous radiographic gastrostomy (PRG), both typically requiring consultant assistance and operating suites.3,4 The ability to perform gastrostomy at the bedside in the Intensive Care Unit (ICU) utilizing mobile endoscopy towers has been documented since the 1980s; however, this approach has not been broadly translated into bedside gastrostomy placement as a standard of care.5,6 Studies have described safety, feasibility, and healthcare system benefits of bedside gastrostomy service models in critically ill patients via PEG.5,7-9 However, many critical care patients continue to have gastrostomy tube placement performed in operating rooms, or alternatively, at the bedside with a mobile endoscopy unit. Both approaches require coordination among multiple consulting services and associated equipment, leading to extended ICU and hospital lengths of stay (LOS) and increased healthcare costs.1,7
Critical care units with bedside tracheostomy services experiencing delays in timely gastrostomy, such as ours, have considered adding bedside gastrostomy options like PEG. Research has shown both gastroscopic and bronchoscopic bedside PEG placement as safe and feasible, but have not broadly considered the long-term safety, credentialing and medical-legal issues imposed by these methods.9-11 The transillumination technique in PEG is imprecise and cannot visualize subcutaneous organs in the vicinity of the stomach. The broad adoption of bedside PEG is challenging from a physician-credentialing and regulatory perspective. Bronchoscopes are not FDA-approved for gastrostomy placement, nor for gastrointestinal diagnostic surveillance below the larynx. Our team could not pursue bedside PEG as an option given credentialing hurdles in using gastroscopes and adding new procedures for bronchoscopes to physicians’ delineation of privileges associated with off-label device usage and the associated medical-legal risks.
Percutaneous ultrasound gastrostomy (PUG) is a broadly accessible bedside gastrostomy procedure shown to be safe and effective, using point-of-care ultrasound rather than endoscopy.4,12-15 Utilizing a magnetic gastropexy, PUG enables real time ultrasound visualization of the access needle and surrounding viscera during gastrostomy tract formation, similar to ultrasound visualization in central line placement. Due to the magnetic gastropexy, PUG is contraindicated in patients with implanted electronically active medical devices, however, PUG otherwise shares similar indications and contraindications as other percutaneous gastrostomy methods. Ultrasound availability enables PUG performance at the bedside by the primary critical care team or other consultants as soon as the need for gastrostomy arises. PUG can also be performed concomitantly with bedside percutaneous dilatational tracheostomy (PDT) in an effort to gain efficiencies in care and/or decrease healthcare costs, particularly when long-term care facilities require tracheostomy and gastrostomy tubes for patient discharge.7,16 Currently, no research exists to assess the efficiency or cost impact of performing bedside PUG on patients with ventilator-dependent respiratory failure.
We hypothesized that performance of bedside PUG by critical care attendings would positively impact efficiency and cost outcomes in ICU patients compared with usual care gastrostomy practice. We evaluated the characteristics and outcomes of critically ill patients in our 36-bed mixed medical/surgical ICU receiving bedside PUG and usual care gastrostomy.
Methods
The University of Maryland Baltimore Washington Medical Center is a 285-bed, academically affiliated community hospital within a large academic medical system. The ICU is a 36-bed, closed, mixed medical/surgical ICU managed by a physician group of ten Pulmonary and Critical Care Medicine board-certified physicians. All patients that underwent gastrostomy tube placement while admitted to the ICU were included for analysis. The local institutional review board at the University of Maryland School of Medicine reviewed the study and determined that it was exempt from full review.
Five of the ten critical care physicians were trained in PUG in order to perform bedside gastrostomy placement when indicated. Methods for performing PUG have been previously described by this group as well as others.4,13-16 Critical care physicians not trained in PUG relied on usual care gastrostomy placement processes (i.e. consultation and placement by gastroenterology or interventional radiology services in the operating suite). Patients received PUG or usual care gastrostomy based on which of these two groups of physicians were attending on the unit.
All ICU patients with ventilator-dependent respiratory failure who received a gastrostomy consult or procedure while in the ICU were included from July 2020 through March 2021 to align with available data from the current fiscal year. July 2020 also marked the end, or nadir, of the first wave of the COVID-19 pandemic in our region; therefore, hospital facilities and surgical resources had normalized. Clinical and demographic data were retrieved from the hospital's electronic medical record (Epic™), and economic data were retrieved from the hospital's cost accounting system including fixed direct, indirect, variable, and total costs for each unique hospital stay. The primary outcomes were LOS (ICU and hospital) and total hospital costs. Secondary outcomes included mortality and discharge disposition. Patient demographic and clinical characteristics thought to potentially influence LOS and hospital costs, such as age, COVID status, insurance status, and severity of illness were compared.
Patient demographics, clinical characteristics and outcomes data were compared between patients who received PUG and usual care gastrostomy. For parametric data, two-tailed t-tests were used to compare variables between the groups, and for non-parametric data, two-tailed Mann-Whitney U tests were utilized. Dependencies on age, gender, BMI, Service Intensity Score and COVID-19 status were evaluated. A significance level of 0.05 was used for all analyses. Of note, this study was not powered to assess morbidity and mortality benefits of performing bedside PUG on patients with ventilator-dependent respiratory failure. Stata Version 13.1 (StataCorp (2015). Statistical Software: Release 13. College Station, TX: StataCorp LP) was used for all analyses by a third-party research partner, TTI Health Research and Economics.
Results
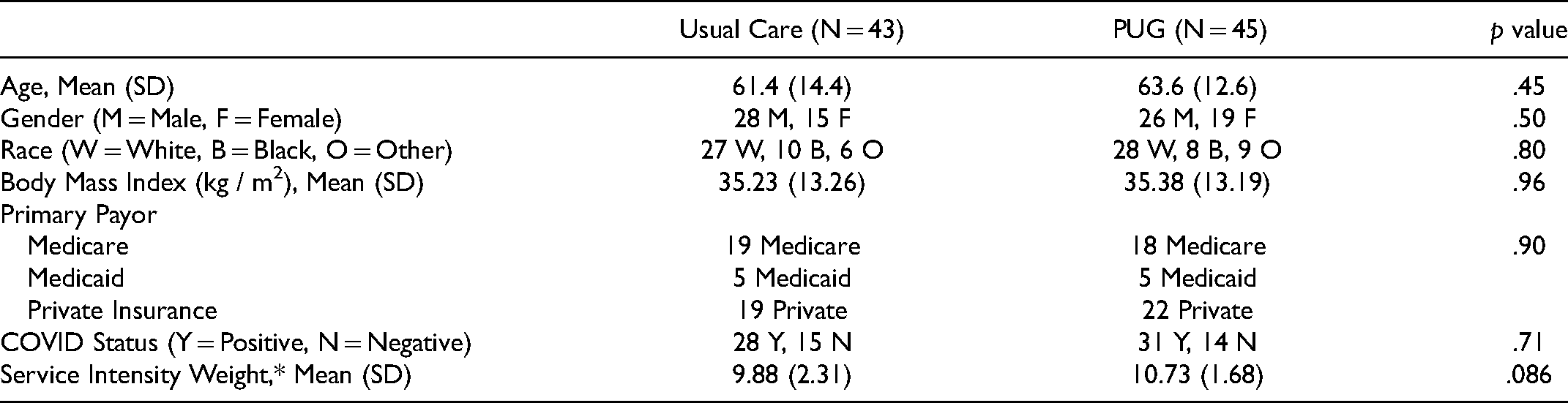
Over a 9-month period, a total of 90 adult critically ill patients with ventilator-dependent respiratory failure received percutaneous gastrostomy. Two patients, one from each group, were excluded for statistical purposes due to hospital lengths of stay in excess of 3 standard deviations from the mean. A total of 88 patients were included in the analysis. 45 patients were in the PUG group and 43 in the usual care group. The two groups were similar across patient characteristics as shown in Table 1.
Demographics and Clinical Characteristics.
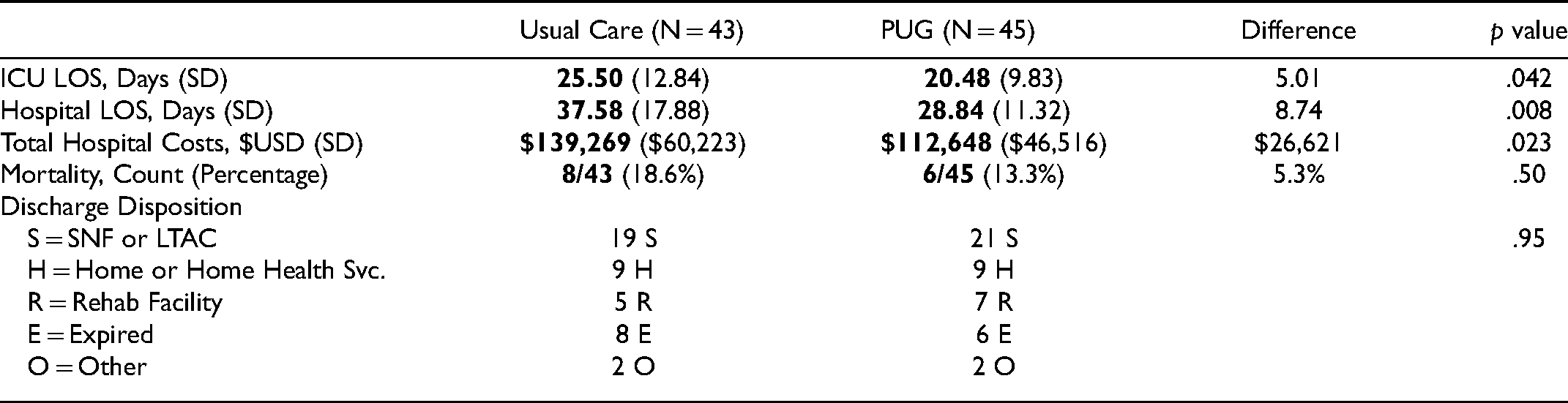
Patients who received bedside gastrostomy via PUG had a significantly shorter mean ICU LOS (20.48 vs. 25.50 days, P = .042) as well as a shorter mean hospital LOS (28.8 vs. 37.6 days, P = .008). Total hospital cost was significantly decreased in the PUG group, with a difference of US $26,621 in cost saving per patient ($112,648 vs. $139,269, P = .023). No difference in mortality was observed between PUG and usual care group (13.3% vs. 18.6%, P = .50). Discharge status also showed no difference between groups, with most patients discharged to long-term care facilities. Patient group primary and secondary outcome comparisons are shown in Table 2.
Primary and Secondary Outcomes.
No statistical difference was observed between groups comparing time from ICU admission to time of indication for gastrostomy. However, highly significant differences were observed in timing metrics post-gastrostomy indication. PUG procedures were performed 4 days earlier than usual care gastrostomies post gastrostomy indication (1.48 vs. 5.63 days, P < .0001). As expected, no patients in the usual care group could receive concomitant bedside gastrostomy and PDT, whereas 70% of the PUG group patients had concomitant PDT and PUG (“TPUG”). Time comparisons of procedure indication and completion between the PUG and usual care groups is shown in Table 3.
Gastrostomy Efficiency Metrics.
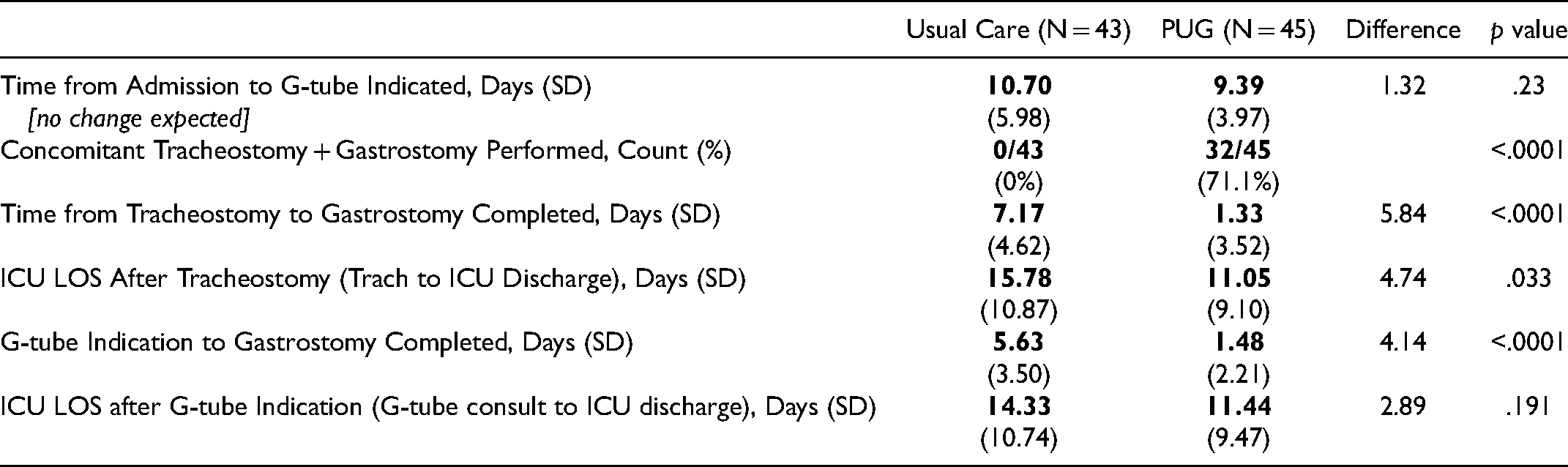
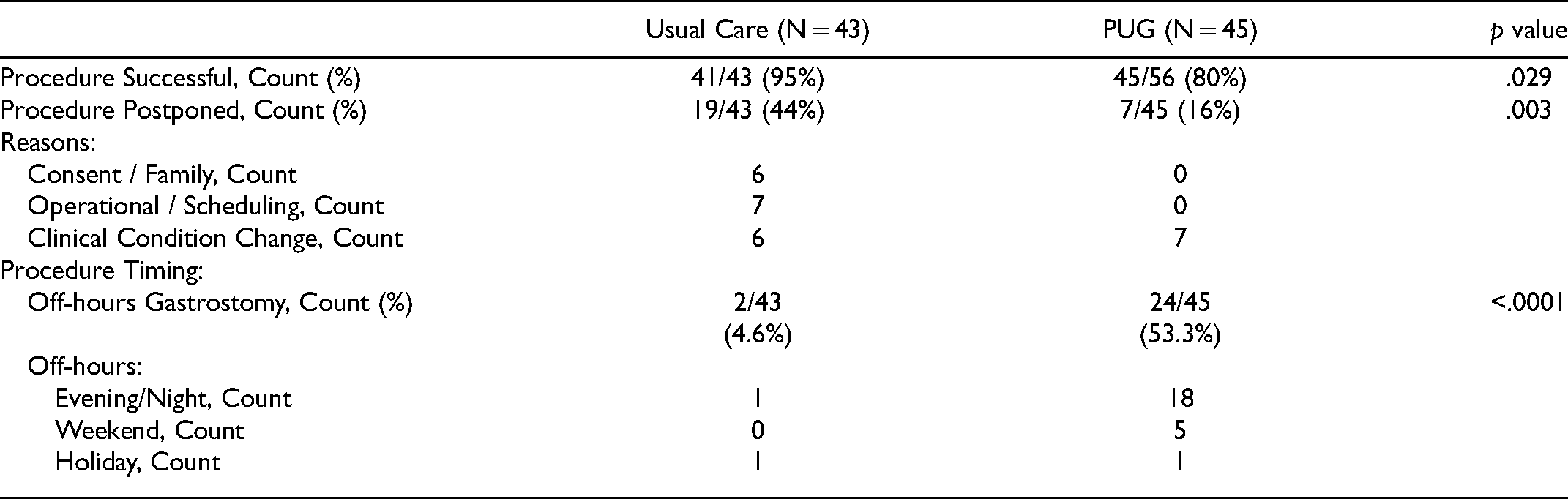
Table 4 details further analysis of gastrostomy process and delays. PUG procedures had a lower procedure success rate when compared to usual care gastrostomy placement (79% vs. 95%, P = .029). All unsuccessful PUG cases were safely aborted, without complications, and fell into categories of anatomical limitations (6), technical limitations (3), or no reasons documented (3). PUG procedures were less likely to be postponed compared to usual care gastrostomy (16% vs. 44%, P = .003) and PUG procedures were also more likely to be performed off-hours compared to usual care (54.5% vs. 4.6%, P < .0001).
Gastrostomy Delay and Feasibility Metrics.
Discussion
Our study demonstrates that PUG placement in patients with ventilator-dependent respiratory failure requiring a gastrostomy is associated with significantly decreased ICU and hospital LOS as well as total hospital costs, compared to usual care gastrostomy. The primary outcomes for this study were ICU and hospital LOS and total hospital costs, which were all found to be significantly decreased in the PUG cohort. Extrapolating the $26,600 cost savings per patient to the entire study group would translate to an annualized $2.5 Million cost reduction for the medical system that the study hospital was part of ($26,621 * 88 * 12/9 * 80%). No significant difference between groups was observed for secondary outcomes of mortality and disposition conditions, although this study was not designed or powered to detect such differences.
To our knowledge, this is the first study in a mixed medical/surgical ICU population with ventilator-dependent respiratory failure demonstrating that more timely gastrostomy, via reduced gastrostomy placement delays, leads to significantly decreased LOS and hospital costs. From a LOS perspective, a neurocritical care conference presentation on a PUG study showed a statistically significant 8-day ICU LOS reduction in patients receiving TPUG versus usual care (PDT and delayed bedside PEG). 17 Prior research from an academic Neurocritical Care Unit showed similar decreases in LOS and hospital costs when gastrostomy is performed concomitantly with PDT in ventilator-dependent critically ill patients. 7 The intervention arm in the Nobleza study had an average 6-day reduction in ICU LOS caused by an average 8-day delay in gastrostomy tube placement after indication in the usual care group, which was thought to be multifactorial.
Our analysis of procedure timing and delays in Table 4 provides insight into potential common causes of delays in usual care gastrostomy placement, which have not been widely studied. When comparing procedure timing across standard operational hours (Monday – Friday 9am – 5pm), PUG procedures were 10 times more likely than usual care gastrostomies to occur during off-hours. The ability of the primary ICU team to perform PUG during time windows when consultants were not available made a large contribution to timely gastrostomy. Furthermore, scheduling challenges with consultant teams, and consenting of patients by off-unit providers were also identified as contributors to gastrostomy postponement. As expected, no difference was found between groups for postponement associated with changes in clinical conditions.
As has been demonstrated in cost effectiveness research related to other procedures, such as central lines and PDT, transitioning to a model where procedures are performed by the primary team at the bedside alleviates the root causes of procedural delays.18,19 The term, “right line, right time,” may now be applicable to gastrostomy tube placement. Safety advantages of reducing ICU LOS have been well documented in medical literature. 19 A further advantage of bedside PUG in the COVID-19 era is the ability to perform necessary procedures without moving contagious patients or equipment throughout the hospital–reducing the risk of contaminating surgical suites and other patients. 16
Limitations in this study include the retrospective design and single center setting. Retrospective studies have potential biases in data collection and data analysis, and lack patient randomization and provider blinding. Our ICU census was cross-checked against billing data, and all admitted patients during the study period had their charts reviewed by trained research coordinators for gastrostomy indication and further clinical and outcomes data. Therefore, it is doubtful that cases or data were missed and not included in the analysis. Blinding is difficult or impossible for a surgical intervention such as gastrostomy. Since only a subset of physicians were trained in PUG, selection bias was minimized, given the random nature of the critical care physician scheduling. Whether a patient was selected for PUG or usual care gastrostomy was based on whether a PUG-trained ICU physician was attending at the time of gastrostomy indication. It is also important to note that patient crossover could occur, in both directions, and patients were grouped based on the procedure ultimately received. For example, patients which had safely aborted PUGs were then referred for usual care gastrostomy. In the inverse scenario, patients with gastrostomy indication may have had a usual care gastrostomy consult placed late in the week, but when the schedule changed to an attending with PUG privileges, that patient would receive a PUG.
Importantly, the providers performing procedures and initiating gastrostomy consults in this study did not know they were being studied, as the IRB was requested on November 2, 2020, halfway through the study period, so the Hawthorne effect could not have impacted the results of the procedures during that time period. Because the study period was during the COVID-19 pandemic, consultant responsiveness and availability may have been less than during non-COVID-19 times. However, our quality data from 2019, which was the impetus for our group to explore more timely gastrostomy options, demonstrated an average 4 day delay in gastrostomy tube placement, similar to the delay reported in this study and other studies.7,17 Our ICU is a large mixed medical/surgical ICU, but the study population includes mostly medical patients; therefore, our findings might be applicable to large medical ICU cohorts only. Medical patients are known to have the most variability in critically ill populations; therefore, a more predictable specialty ICU may see the same benefit or even greater benefits in getting their patients with ventilator dependence timely gastrostomy. For example, Nobleza and Parikh neurocritical care studies showed larger LOS reductions and Nobleza's study showed a larger cost savings of $35,000 per patient with timely gastrostomy.7,17
Future studies will be necessary to demonstrate the applicability of our findings in multicenter and more specialized ICU settings such as neuro, trauma and cardiac critical care units. Furthermore, future studies can attempt to determine if patients’ nutritional status is optimized by timely gastrostomy. These studies could also determine whether efficiencies gained in gastrostomy placement ultimately lead to decreased patient morbidity and mortality via reducing periods of malnutrition and reducing time in the ICU.
Conclusion
This study supports implementation of bedside PUG in ICUs where gastrostomy is not performed at the bedside or where typical delays exist in bedside gastrostomy placement. Timely gastrostomy is associated with significantly decreased ICU LOS and hospital LOS for patients with ventilator-dependent respiratory failure. Hospital costs were significantly reduced, a per patient savings of $26,600, specifically attributed to the significantly reduced time delay in achieving gastrostomy placement. PUG performed at the bedside by the primary ICU team also minimizes patient transport, care handoffs, and exposures to COVID-19.
Footnotes
Acknowledgments
The authors would like to thank Dana Beach, RN, and Kyra Lasko for their contribution to this research effort. We would also like to acknowledge the dedication and compassionate care provided by the clinical team at The University of Maryland Baltimore Washington Medical Center Medical Intensive Care Unit.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RGW and JM received salary support from the NIDDK grant through subawards from CoapTech Inc. The authors had control of and full access to all of the data in this study and are responsible for the integrity of the data and the accuracy of the data analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, (grant number 2R44DK115325).
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.