
Abstract
Vein line positioning represents one of the first diagnostic and therapeutic steps in Pediatric Emergency Department (PED); however, the outcome of this maneuver is frequently not as expected, especially for difficult-to-access (DIVA) patients. The standard technique (visual-palpatory) has a low success rate; hence ultrasound (US) assistance has been suggested for DIVA patients, although controversial results have been obtained. Our study compared the success rate of an intravascular (IV) access procedure at the first attempt, with and without ultrasound assistance, in pediatric DIVA patients. Secondary objectives were the global success rate, the mean procedural time, the IV device's life span, and the complications rate. We conducted an observational, prospective, monocentric, no-profit cohort study enrolling 110 patients presenting to our ED, aged 0-21 years. All the patients were considered difficult-to-access patients according to the DIVA score (≥4) or history of previous difficult intravascular access. They were randomized into two homogeneous groups: 50 patients with the standard and 60 with the US-assisted technique. We obtained a significantly higher success rate at first attempt with the US-guided technique (90% vs 18%, p ≤ .00001). Moreover, the overall success rate was higher in the US group (95% vs 46%, p < .00001). The mean procedural time resulted significantly less in the US group (2.7 ± 2.2 min vs 10 ± 6.4 min, p < .0001), as well as the overall number of attempts to obtain a stable IV line (1.09 ± 0.34 attempts vs 2.38 ± 1.09 attempts, p < .0001). We experienced some post-procedural complications without differences in the two groups, although none were severe. Our study showed that bedside ultrasound assisting implantation of peripheral venous access in pediatric DIVA patients improves first-time success rate, overall success rate, procedural time, and patient comfort, reducing the number of attempts to obtain a stable IV line.
Introduction
A peripheral intravenous catheter (PIVC) is placed in 13%-20% of children who access the pediatric emergency department (ED).1,2 Endovascular device implantation is the most commonly performed invasive procedure in hospital care, universally considered a routine practice. 3
Although PIVC represents one of the first diagnostic and therapeutic steps in the emergency approach in pediatric patients, the outcome of this maneuver may be unsuccessful, especially in difficult-to-access patients. 4 This constitutes a significant obstacle to clinical management and a source of discomfort for patients and their families.
In pediatric age, a positive outcome at first attempt in intravascular (IV) access with the visual-palpatory (standard) technique is estimated between one-third to two-thirds.5,6
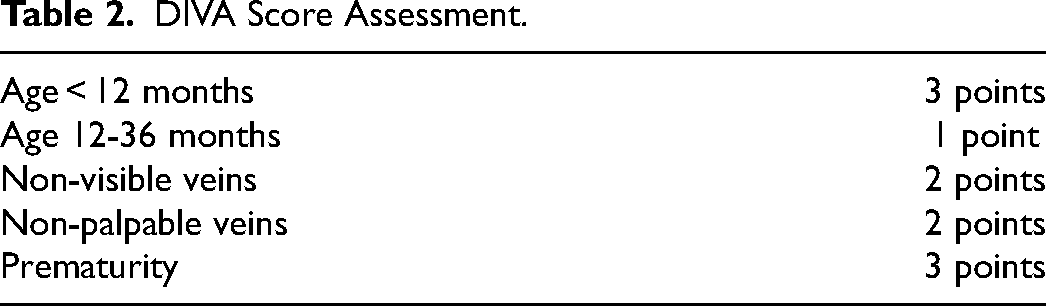
The attempts to ensure successful implantation are 2.35 on average, 7 with a global 9-min median time. 5 However, 20%-25% of the pediatric population has risk factors that may worsen this procedure outcome (Table 1); these patients are referred to as Difficult IntraVascular Access (DIVA) patients. The PIVC placement procedure for DIVA patients usually requires more skilled staff (such as anesthesiologists), several attempts, more time and cost.8-10 In 2008, Yen et al 11 developed and validated a DIVA score to recognize and classify these patients (Table 2).
Major Risk Factors for an Adverse Outcome in Vein Line Placement.
DIVA Score Assessment.
The introduction in clinical practice of alternative techniques that can increase the success rate of PIVC implantation in DIVA patients is highly desirable: for this purpose, “point-of-care” or “bedside” ultrasound (US) is making its way into the literature. Point-of-care US is a non-invasive tool that may be used as a valid aid in positioning peripheral and central intravenous devices, allowing visualization of venous vessel and surrounding anatomical structures: moreover, it helps following the needle tip during the whole procedure.
The efficacy of US-guided positioning of PIVC has been demonstrated in adults, especially in DIVA patients12,13; in the pediatric population, the advantages of its use are a matter of debate.
Aim of the Study
Our study compares the success rate of positioning PIVC access procedure at first attempt, with and without ultrasound assistance, in DIVA pediatric patients, in an ED setting.
Subsequently, we investigated the global success rate of a PIVC placement in the same populations; the mean procedural time; the survival time of the IV devices, and complication rate (during and after the procedure), comparing the two groups of patients.
Patients and Methods
We conducted an observational, prospective, monocentric, no-profit pilot study enrolling 110 pediatric patients presenting to our ED from first May to 30th November 2022. All patients met the following inclusion criteria: age between 0 and 21 years requiring a PIVC positioning in the ED due to their conditions; the procedure was considered difficult according to the DIVA score (≥4) or a history of previous difficult intravascular access (more than 3 attempts to obtain a vein line or a previous vein line placed by anesthesiologists). In addition, written or oral informed consent was obtained. We ruled out patients with coagulation disorders and those in critical conditions. Patients were randomized into two groups: the procedure was conducted with the US-guided technique in 60 patients (54.5%), whereas the rest of them (50 patients, 45.5%) were treated with the standard approach (visual-palpatory). Patients enrolled had a wide age range, from 63 days to 21 years. The DIVA score assigned ranged between 2 and 10.
The PIVC placement was performed either with the standard method (visual-palpatory) or the US-guided technique depending on the skills of the staff (US-trained and non US-trained): this approach allowed the randomization of the patients into two groups following regular staff shifts. No crossover between the two groups was permitted. The healthcare professionals engaged in the study were 25 pediatric nurses and 6 pediatricians: the US-trained staff was skilled with post-degree specific ultrasound-assisted vein-line positioning courses. The two more skilled physicians supervised the rest of the US-trained staff in at least 20 procedures before the start of the study to reach a satisfying level of technique. The staff assigned to the standard procedure had a longer length of service (mean 12.7y ± 4.9y, min 5y max 23y vs mean 5.7y ± 0.9y, min 5y max 7y; p < .0005). The US devices used are Samsung SonoAce R3 and Esaote MyLab 30 Gold, both with high-frequency linear probe. The intravascular devices are Vasofix Safety (BBraun) ranging from 20 to 24 Gauge for superficial access and Introcan Safety (BBraun) ranging from 22 to 24 Gauge for deep access. The catheter size and length were chosen according to the rule “less than 50% of the vein area occupied by the catheter and at least 2/3 of the catheter length inside the vein”. Hence the operator chose the device that closely followed this rule. All the steps of vascular access were the same in both groups (skin sanitation, care of patient and parents, fixing of the device), except for the method used to obtain the vein line (standard vs US-guided). All US-guided PIVC were placed using the single operator dynamic method in the short or long axis, in which the operator simultaneously cannulates the vessel following the needle tip into the vein (Supplementary table I).
After vein line placement, we collected data regarding the procedure and the patient, such as sex, ethnicity, weight, site of access, target vein, time to blood backflow (TBF, time between tourniquet positioning and blood backflow at the bottom of the needle), the number of attempts and intraprocedural complications (large hematoma formation, arterial or nerve lesion); these data are reported in Supplementary tables II, III and IV. When a blood backflow was obtained, we tested the vein line with 3 mL of saline flush: any sign of extravasation led to the attempt being considered failed. Moreover, we recorded data about late complications (displacement, phlebitis, occlusions) and the survival time of the device.
Descriptive statistics of the study patients were first performed and reported. Categorical variables were described in terms of absolute frequencies and percentages. Quantitative variables were described in terms of means, medians and standard deviations, with minimum and maximum values. We compared groups by nonparametric tests (Mann–Whitney U-test) for continuous variables. The association between the categorical variables was performed using the χ2 test (Chi-Square) or Fisher's exact test. All p values are estimated using a 2-tail test with statistical significance at p < .05. The software SPSS (SPSS Inc, Chicago, Illinois, USA) was used for all the statistical analysis.
This study has been previously approved by our Regional Ethic Committee (CER Liguria 141/2022 – DB id 12250)
Results
The two cohorts were homogeneous in terms of male-to-female ratio, ethnicity, age, weight-for-age centile, and DIVA score, as shown in Table 3. We obtained a significantly higher success rate on the first attempt with the US-guided technique (90% vs 18%, p < .00001). In addition, if we consider antecubital access (the only one consistently shared between the techniques), the data regarding first-attempt success rate are the same (85.7% vs 14.3%, p < .00001). Moreover, the overall success rate was higher in the US group (95% vs 46%, p < .00001). The mean procedural time resulted significantly less in the US group (2.7 ± 2.2 min vs 10 ± 6.4 min, p < .0001), as well as the overall number of attempts to obtain a stable IV line (1.09 ± 0.34 attempts vs 2.38 ± 1.09 attempts, p < .0001): these data are reported in Table 4.
Description of the Study Patients [N = 110].
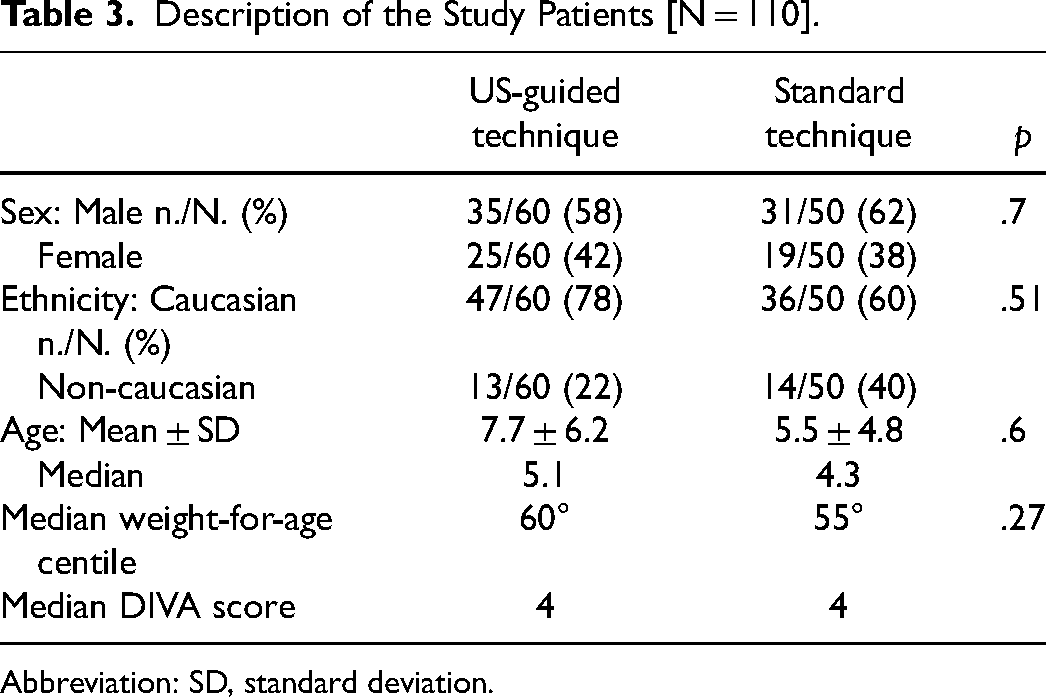
Abbreviation: SD, standard deviation.
Success Rate and Procedural Time Comparison [N = 110].
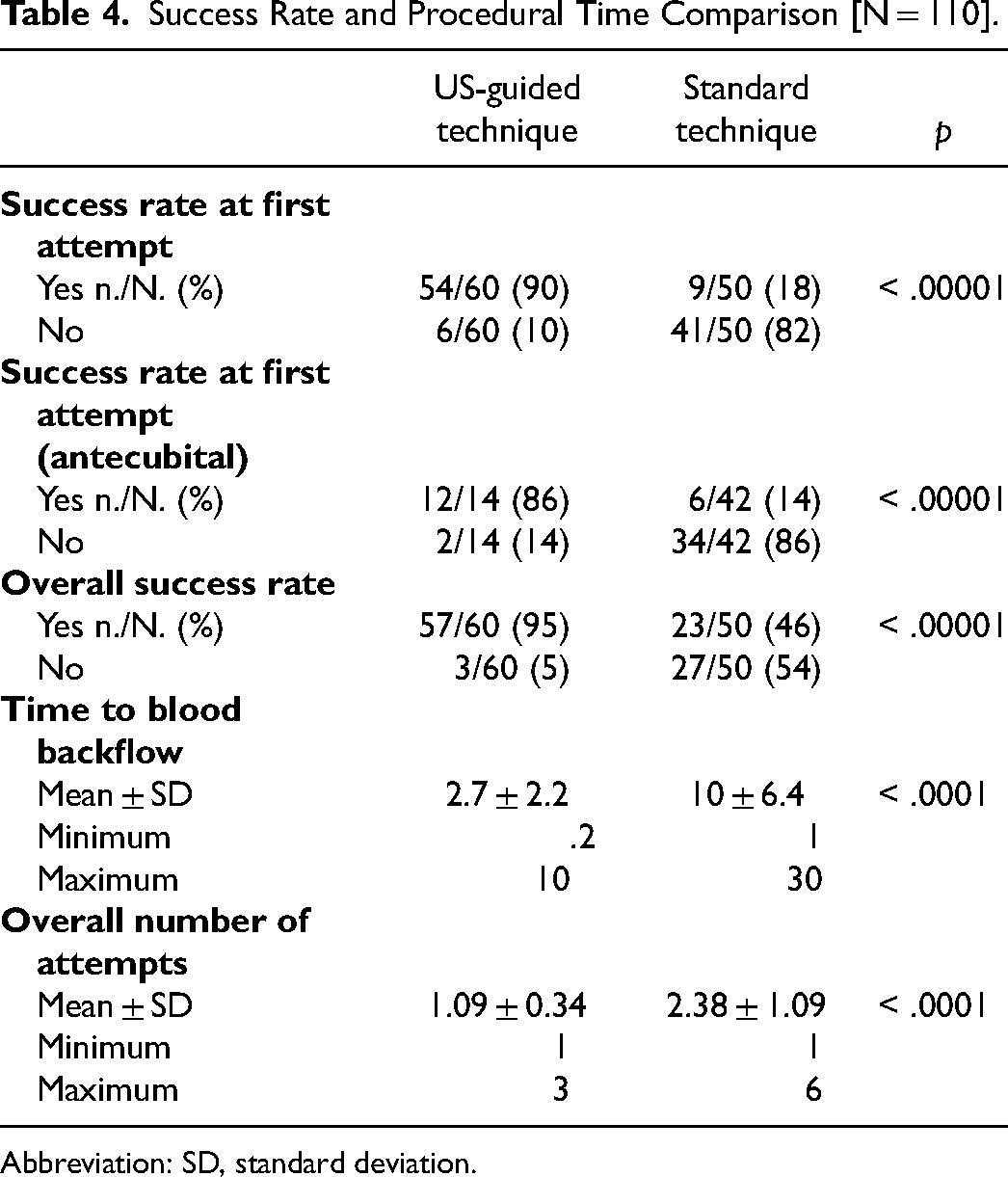
Abbreviation: SD, standard deviation.
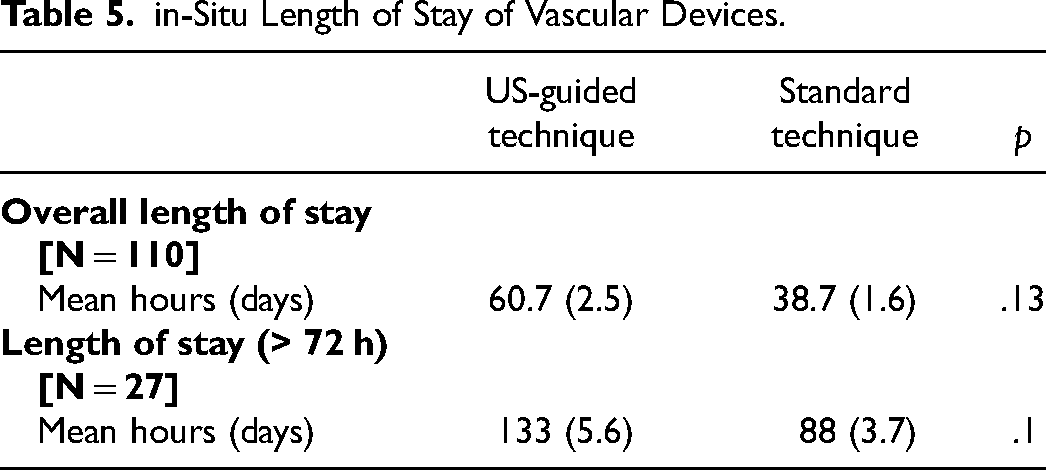
The mean in-situ duration of the PIVC was relatively short (2.5 days for the US group and 1.6 days for the standard group) because many patients were discharged directly from ED or after a brief observation period. Moreover, if we only consider devices with a survival time longer than 72 h (excluding patients with precocious discharge from ED), the difference between the two groups is wider (5.6 days vs 3.7 days). Despite this, we did not observe a statistically significant difference in the device length of stay between the US and the standard groups (p = .10, Table 5).
in-Situ Length of Stay of Vascular Devices.
No intraprocedural complications were recorded in our series, while we experienced some post-procedural complications, although none of them were classified as severe. Among 80 successful implant procedures, we recorded 28 complications (35%), as reported in Table 6. Adverse events were more frequent in the standard group (43.5% vs 31.6%), even though no statistical significance was reached (p = .43). No correlation between post-procedural complications and the procedural operator was found, as well as no patients required central venous catheter implantation.
Post-Procedural Complications.
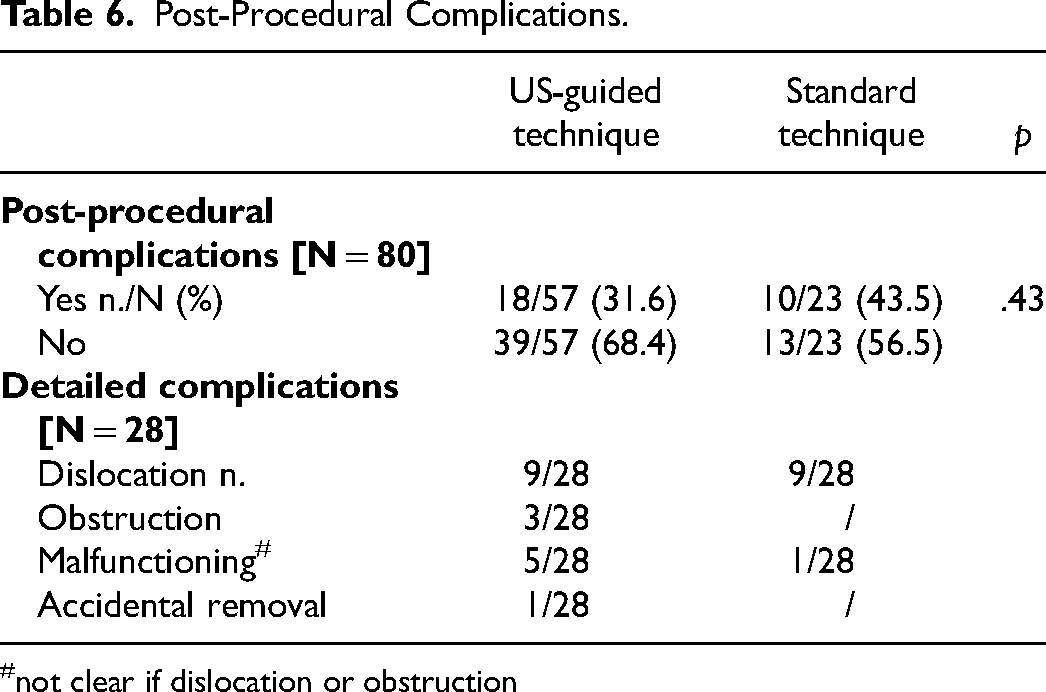
not clear if dislocation or obstruction
Discussion
The implantation of PIVC is frequently performed in pediatric ED; despite this being a routine procedure, a negative outcome is reported in up to 60% of the cases, particularly for DIVA patients. 5 In addition, many unsuccessful attempts cause discomfort for patients, parents, and operators, with delay in treatment.9,14-15
Our study compared PIVC implantation in DIVA pediatric patients in ED using the US-guided or the standard (visual-palpatory) procedure. We recorded a first-attempt and overall higher success rate in the US group (also confirmed in antecubital-access regarding data), as well as a shorter procedural time and fewer attempts to obtain a stable IV line. Moreover, we reported a slightly increased duration of intravascular devices placed with US help, albeit this data did not reach statistical significance. A similar incidence of post-procedural complications was recorded in the two cohorts; no intra-procedural complications occurred.
The US assistance has already been investigated in the literature, with different outcomes: Vinograd et al 16 conducted a prospective, randomized, controlled trial in a pediatric ED in which 167 DIVA patients were enrolled to receive either a US-guided or a standard PIVC placement; their results were comparable to our first-attempt success rate (85.4% vs 45.5%), median survival time (2.6 vs 4.5 days) and procedural complications (48% vs 40%). Benkhadra et al 17 also obtained a similar result with a smaller and younger group of patients: the median time to cannulation (1 vs 7 min) and median number of attempts (1 vs 2.5) were favorable in the US group.
However, several Authors came across different conclusions. Although Bair et al 18 used a static US-assisted (not dynamic US-guided) technique and Curtis et al 19 investigated pediatric non-DIVA patients, they did not find a statistically significant difference between the US and standard technique or even a negative effect of the US. More recently, a systematic review published in Pediatrics in May 2022 clearly demonstrated that using the US during implantation of peripheral venous access improves the first-time success rate and the overall success rate in DIVA patients. 20
Conclusions
In conclusion, our study showed that the use of bedside US-guided implantation of PIVC in pediatric DIVA patients in an ED setting improves first-time success rate, overall success rate, procedural time, and patient comfort, reducing the number of attempts to obtain a stable IV line. Moreover, it can be considered a safe procedure since we did not record intra-procedural complications, and the number of post-procedural complications was equal in both the US and standard groups.
As strengths, this study provides further evidence to support the routine use of US guidance for PIVC implantation in pediatric ED. Therefore, we suggest implementing this technique as a standard of care for pediatric DIVA patients. Weak points of our study are a small sample size, the monocentric feature and the randomization process based on staff shift.
Supplemental Material
sj-docx-1-jic-10.1177_08850666231199050 - Supplemental material for Difficult Intravascular Access in Pediatric Emergency Department: The Ultrasound-Assisted Strategy (DIAPEDUS Study)
Supplemental material, sj-docx-1-jic-10.1177_08850666231199050 for Difficult Intravascular Access in Pediatric Emergency Department: The Ultrasound-Assisted Strategy (DIAPEDUS Study) by Matteo D’Alessandro, Margherita Ricci, Tommaso Bellini, Benedetta Chianucci, Maria Grazia Calevo, Emanuela Piccotti and Andrea Moscatelli in Journal of Intensive Care Medicine
Footnotes
Acknowledgment
We are grateful to BBraun© company for providing all the devices to complete this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.