
Abstract
Objectives:
Patients with connective tissue diseases (CTD) such as systemic lupus erythematosus (SLE) have an increased risk for infections. This study investigated the outcome and characteristics of CTD patients under intensive care unit (ICU) treatment for sepsis.
Methods:
A single-center retrospective analysis was conducted and reviewed all patients with a CTD diagnosis admitted to the ICU of a university hospital for sepsis between 2006 and 2019. Mortality was computed and multivariate logistic regression was used to detect independent risk factors for sepsis mortality. Furthermore, the positive predictive value of ICU scores such as Sequential Organ Failure Assessment (SOFA) score was evaluated.
Results:
This study included 44 patients with CTD (mean age 59.8 ± 16.1 years, 68.2% females), most of them with a diagnosed SLE (61.4%) followed by systemic sclerosis (15.9%). 56.8% (n = 25) were treated with immunosuppressives and 81.8% (n = 36) received glucocorticoids. Rituximab was used in 3 patients (6.8%). The hospital mortality of septic CTD patients was high with 40.9%. It was highest among systemic sclerosis (SSc) patients (85.7%). SOFA score and diagnosis of SSc were independently associated with mortality in multivariate logistic regression (P = 0.004 and 0.03, respectively). The Simplified Acute Physiology Score II (SAPS II), SOFA and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were good predictors of sepsis mortality in the investigated cohort (SAPS II AUC 0.772, P = 0.002; SOFA AUC 0.756, P = 0.004; APACHE II AUC 0.741, P = 0.007).
Conclusions:
In-hospital sepsis mortality is high in CTD patients. SSc diagnoses and SOFA were independently associated with mortality. Additionally, common ICU scores were good predictors for mortality.
Keywords
Introduction
Connective tissue diseases are a heterogenous group of inflammatory rheumatic diseases consisting of systemic lupus erythematosus (SLE), systemic sclerosis (SSc), dermato- or polymyositis, Sjögren’s syndrome, and mixed connective tissue disease (MCTD). Since immunosuppressive therapy is usually needed, risk of infections is increased. The significant burden of infections in SLE patients for example is well known and highly contributes to mortality. 1 –7 While immunosuppressive therapy (particularly glucocorticoids) bears a dose-dependent risk for infections, 8 –10 use of antimalarials such as hydroxychloroquine reduces the likelihood of major infections due to their antibacterial, antiviral and antifungal properties. 1,10,11 Besides the negative impact of the immunosuppressive therapy, the disease itself increases the risk for infections, e.g., for pneumococcal disease due to the common complement deficiency in SLE. 12 General sepsis mortality in SLE patients without considering ICU stays shows a great variability, ranging from 0 to 60% (median 11.1%) according to a population-based study from the US. 13 The 2 major causes for ICU admission are infections (36%) and flares (24%). More than 55% of septic SLE patients are admitted to an ICU. 6 ICU-related mortality in SLE depends on the cause of admission. 14 Sepsis is the most common cause of premature death among female SLE patients < 50 years. 15
Most other CTDs are scarcely investigated regarding risk for infections and infection-associated mortality, probably due to their low incidence. In SSc, disease-related complications (40%) and infections (30%) are the most common reasons for ICU admission. 14 For patients with dermatomyositis (DM), respiratory failure was shown to be the main reason for ICU admission. 16 Nevertheless, DM significantly increases the risk for serious infections (OR 2.2, 95% CI 2.1-2.3). 17 This risk is further increased by the use of glucocorticoids and mycophenolate-mofetil in a dose-dependent manner. 18
While national and international guidelines clearly recommend vaccination against common preventable pathogens such as Streptococcus pneumoniae and influenza for patients with rheumatic diseases and under immunosuppressive therapy in general, 19,20 vaccination rates among these patient cohorts remain low. 5,21 –23
Despite the need for more data, investigations on CTDs and intensive care treatment for sepsis are rare or address ICU treatment in general without focusing on sepsis in particular. 14,16,24 –29 Consequently, this investigation was carried out to determine the in-hospital mortality of septic CTD patients requiring ICU treatment.
Methods and Study Design
All CTD patients ≥18 years admitted to the medical ICU of our University Hospital for sepsis between 2006 and 2019 have been retrospectively studied. We searched the hospital records using the International Classification of Diseases-10-German modification 2019 codes of patients admitted to the medical ICU (A39.x-A41.x for sepsis and M32.x-M35.x for the different CTDs). The diagnosis integrity was checked independently by 2 of the authors (MK and CB) reviewing the medical records and discharge letters. All diagnoses were found to be appropriate. Some of the patients were referred from other hospitals directly to our ICU for sepsis treatment only.
On ICU admission, sepsis severity is assessed and digitally documented regularly using SOFA, APACHE II, and SAPS II scores. Patient demographics, clinical and laboratory parameters were obtained at the time of ICU admission from the electronic chart.
The ethics committee of the Medical Faculty of the University of Leipzig has approved the design of this study (Reg-No. 352/19-ek).
Biostatistical Analysis
Continuous data were described using either median and interquartile range (IQR) or mean and standard deviation (SD). Categorical data were described with absolute or relative frequencies. Chi-square tests were performed to compare frequencies of categorical variables. For continuous data, Student’s t test or Mann-Whitney U test, as appropriate, was used after Shapiro-Wilk normality test. Age and sex-adjusted logistic regression was performed to identify independent risk factors for non-survival. The final regression model consisted of all significant variables. To further determine the power of ICU scores (e.g., APACHE II) in predicting mortality, receiver operating characteristic (ROC) analysis was conducted. P values <0.05 were regarded as statistically significant. All results were computed using SPSS Version 24 for Mac (IBM, Chicago, IL, USA). The figure was drawn using Prism 8 for Mac (GraphPad Software, San Diego, CA, USA).
Results
During the study period, 44 CTD patients (61.4% SLE) were admitted to the ICU for sepsis (mean age at admission 59.8 ± 16.1 years, 68.2% female). Prior to admission, 56.8% (n = 25) were treated with immunosuppressives (azathioprine, n = 7 and mycophenolate-mofetil, n = 7) and 81.8% (n = 36) received glucocorticoids. Biologic therapy was used in 6.8% (rituximab, n = 3) of the patients. Among the patients with SLE, 25.9% (n = 7) had a renal involvement. Of the SSc patients, 71.4% (n = 5) had a known interstitial lung disease (ILD), the mean forced vital capacity (FVC) of the SSc patients was 2.9 ± 1.3 l. The mean ICU length of stay was 7.1 ± 9 days.
During intensive care treatment, mechanical ventilation was required in 47.7% (n = 21), vasopressor support in 54.5% (n = 24) and renal replacement therapy (RRT) in 36.4% (n = 16) of cases. Clinical data are presented in Table 1. For details on the immunosuppressive medication, see Table 2. The most frequent site of infection was the lung (50%), followed by the urinary tract (20.5%).
Clinical and Laboratory Data of the Septic CTD Patients.a
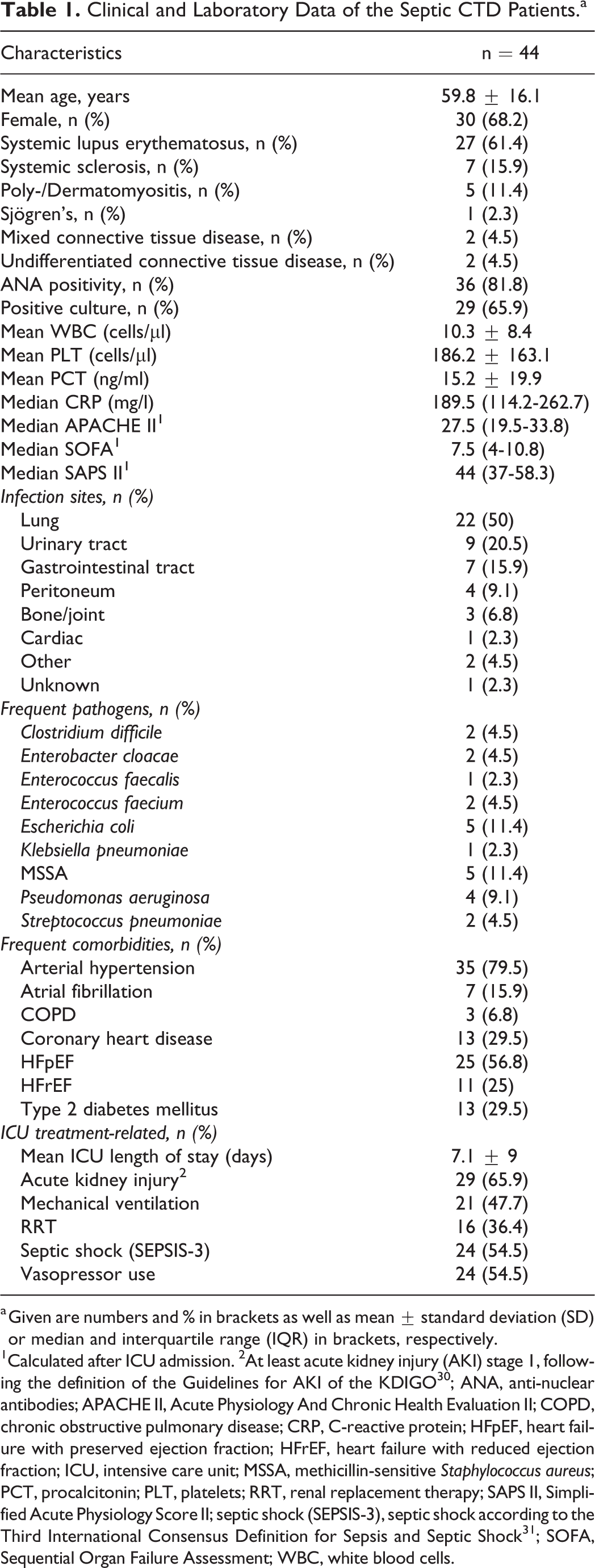
a Given are numbers and % in brackets as well as mean ± standard deviation (SD) or median and interquartile range (IQR) in brackets, respectively.
1 Calculated after ICU admission. 2 At least acute kidney injury (AKI) stage 1, following the definition of the Guidelines for AKI of the KDIGO 30 ; ANA, anti-nuclear antibodies; APACHE II, Acute Physiology And Chronic Health Evaluation II; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; ICU, intensive care unit; MSSA, methicillin-sensitive Staphylococcus aureus; PCT, procalcitonin; PLT, platelets; RRT, renal replacement therapy; SAPS II, Simplified Acute Physiology Score II; septic shock (SEPSIS-3), septic shock according to the Third International Consensus Definition for Sepsis and Septic Shock 31 ; SOFA, Sequential Organ Failure Assessment; WBC, white blood cells.
Immunosuppressive Medication Prior to ICU Admission.a
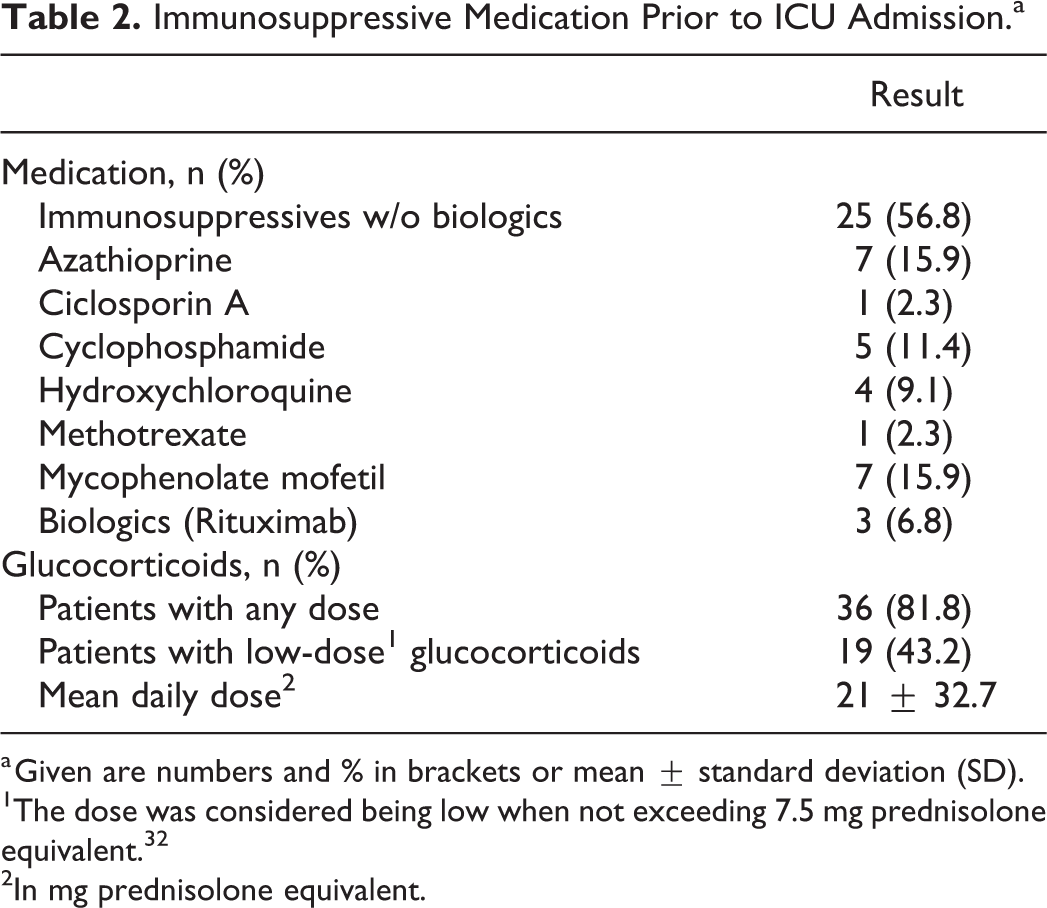
a Given are numbers and % in brackets or mean ± standard deviation (SD).
2 In mg prednisolone equivalent.
Eighteen out of 44 patients died, resulting in an in-hospital mortality of 40.9%. While we did not find a significant difference in mortality regarding the individual medication (only a trend for a higher mortality under Cyclophosphamide, P = 0.059, Table 3), the daily glucocorticoid dose was associated with mortality with significantly higher doses among non-survivors (P = 0.032). There was no association between mortality and the site of infection or the cultured pathogen (data not shown).
Bivariate Analysis of Risk Factors for Mortality in Vasculitis Patients.a
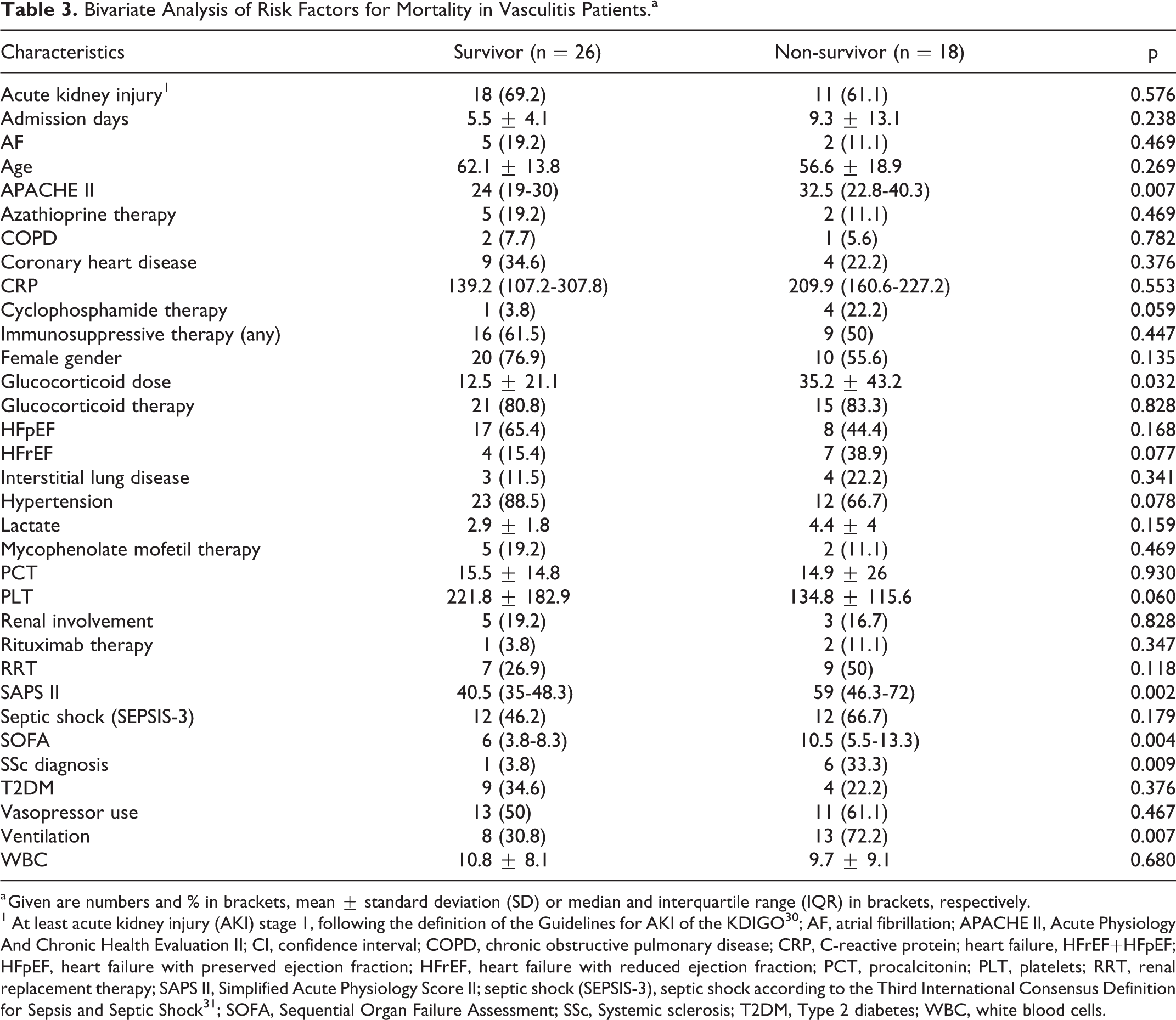
a Given are numbers and % in brackets, mean ± standard deviation (SD) or median and interquartile range (IQR) in brackets, respectively.
1 At least acute kidney injury (AKI) stage 1, following the definition of the Guidelines for AKI of the KDIGO 30 ; AF, atrial fibrillation; APACHE II, Acute Physiology And Chronic Health Evaluation II; CI, confidence interval; COPD, chronic obstructive pulmonary disease; CRP, C-reactive protein; heart failure, HFrEF+HFpEF; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; PCT, procalcitonin; PLT, platelets; RRT, renal replacement therapy; SAPS II, Simplified Acute Physiology Score II; septic shock (SEPSIS-3), septic shock according to the Third International Consensus Definition for Sepsis and Septic Shock 31 ; SOFA, Sequential Organ Failure Assessment; SSc, Systemic sclerosis; T2DM, Type 2 diabetes; WBC, white blood cells.
Importantly, the diagnosis of SSc was associated with an increased mortality (P = 0.009), which was also true for patients with the need of invasive ventilation (P = 0.007). Among the patients with SSc, overall mortality was very high with 85.7%. The majority of the deceased SSc patients (66.7%) had an ILD. Mortality among SLE patients was lower with 29.6%. Mortality was not calculated separately for the other CTD entities since numbers were too low (Table 1). PCT levels differed among the distinct entities and were highest in SLE patients without reaching significance: 17.1 ng/ml ± 22.8 in SLE, 11.6 ng/ml ± 8.1 in Myositis and 9.6 ng/ml ± 16 in SSc.
Of particular interest, there was no significant difference regarding septic shock when comparing survivors to non-survivors (P = 0.179, Table 3). There was a trend toward a lower platelet count in non-survivors, however this did not reach a statistical significance (P = 0.060). Significantly higher SOFA, SAPS II and APACHE II scores were found in non-survivors (P = 0.004, P = 0.002, P = 0.007, respectively).
In our logistic regression model, adjusted for age and gender, only SOFA (Odds ratio [OR] 1.481, 95% confidence interval [CI] 1.131-1.940, P = 0.004) and SSc diagnosis (OR 20.347, 95% CI 1.331-311.15, P = 0.03) remained independently associated with non-survival.
ROC analysis (Figure 1) revealed a good predictive power of SOFA, SAPS II and APACHE II for sepsis mortality in our CTD cohort, with the area under the curve (AUC) being the highest for SAPS II (AUC 0.772 ± 0.084, 95% CI 0.608-0.937, P = 0.002). Analyzing the ROC curves further, cut off values with a high probability for mortality have been determined for each score (Figure 1).
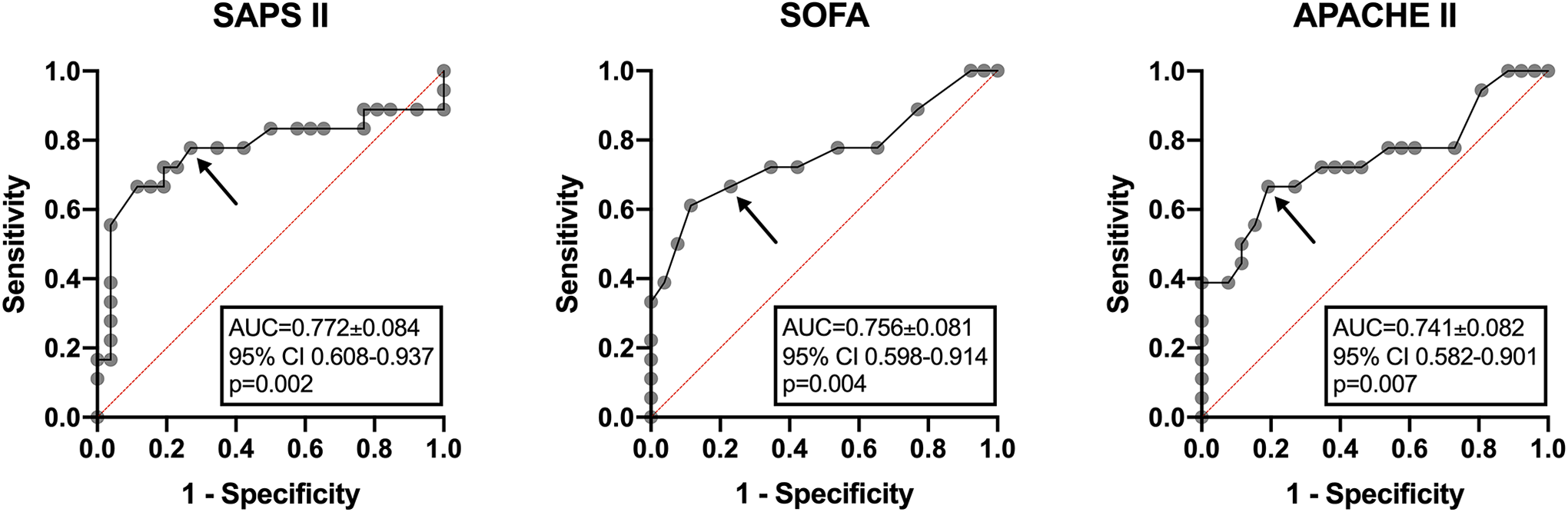
Receiver operating characteristic (ROC) analysis of the value of the SOFA, SAPS II and APACHE II score in predicting in-hospital mortality. The area under the curve (AUC) is shown with standard error (±SE), 95% confidence interval (CI) and p value. The arrows show reasonable cut off values for predicting mortality with high probability as follows: SAPS II = 47 (specificity 73%, sensitivity 78%), SOFA = 9 (specificity 77%, sensitivity 67%), APACHE II = 31 (specificity 81%, sensitivity 67%). APACHE II, Acute Physiology and Chronic Health Evaluation II; AUC, area under the curve; CI, confidence interval; SAPS II, Simplified Acute Physiology Score II; SOFA, Sequential Organ Failure Assessment.
Discussion
The aim of this study was to evaluate the in-hospital sepsis mortality among CTD patients requiring intensive care. With 40.9%, sepsis mortality was high, although septic shock was not found to be more prevalent among non-survivors. Importantly, more than 80% of the patients received glucocorticoids in a mean daily dose of 21 mg prednisolone equivalent. The contribution of glucocorticoid (GC) use of >5 mg prednisolone equivalent to mortality of rheumatic patients in intensive care treatment has been discussed before. 26 Consistent with that assumption, significantly higher GC doses were found among the non-survivors of our cohort. High doses of GC in the year before ICU admission or dose escalation during ICU stay have been shown to be associated with a reduced survival in patients with rheumatoid diseases. 33 Additionally, the tertiary character of our hospital could contribute to the high mortality. Of interest, mortality is slightly lower than in RA 34 as well as systemic vasculitis patients. 35
A literature search for patients with CTDs and admission to ICU mostly showed mixed cohorts (i.e. different rheumatic diseases including CTDs, rheumatoid arthritis and Spondylarthritis) and heterogenic reasons for ICU admission. The reported mortality showed a very wide range of 16 to 89%, mainly depending on the investigated diseases and the reason for ICU admission. 14,16,25 –29,33,36 –40 Therefore, most of the publications are difficult to compare to our well-defined group of septic CTD patients. A study by Heijnen et al (n = 86), for example, consisted of only 18.6% patients with a CTD and 60% were admitted to the ICU for infection. 38 The small proportion of CTD patients limits the meaningfulness of the reported in-hospital mortality of 39%. Brünnler et al 36 (n = 48) reported a mortality rate of only 16%, but the studied cohort consisted of patients with different rheumatic diseases (also including rheumatoid arthritis and spondylarthritis). Main reasons for admission were infections and cardiovascular complications (31 and 20%, respectively). The median APACHE II score of 12 in that cohort was considerably lower than the 27.5 (19.5-33.8) among our patients, emphasizing the exceeding severity and worse prognosis of our cohort. The results of Nihtyanova et al. (n = 51 SSc patients) show an ICU mortality of 39%, 39 while sepsis accounted for 39% of ICU admissions only. Rütter et al. (n = 50) found a mortality of 38% in a cohort of patients with very different rheumatic diseases being admitted to an ICU. 27 That cohort consisted of 20% CTD patients only and sepsis was the reason of admission in less than a third of patients. Zamir et al. investigated 27 SLE patients under intensive care and found a 30-day mortality of 29.6%, 40 with most of their patients admitted to the ICU for infections (66.7%). However, there has been no stratification whether they were septic or not. Pène et al. focused on SSc (n = 41) and reported a mortality of 31.8%. 25 Admission to ICU was predominantly caused by acute respiratory failure (65.8%), followed by renal failure (14.6%) and other unspecified reasons (19.5%). Since the number of patients admitted to ICU for sepsis was not specified, the calculated mortality is difficult to compare to our results. A case series (n = 14) from Naranjo-Escobar et al. reported an ICU mortality of 43% in SSc patients, while the main causes of ICU admission were non-SSc-related (71.4%). 28 Shalev et al. reviewed a small cohort of SSc patients (n = 9) and found a high in-hospital mortality of 89%. 29 In this small group, sepsis was the main reason for ICU admission and death, with 62.5% of the deceased patients having a pulmonary involvement of the CTD.
According to the literature, the highest mortality was seen in SSc patients. 25,28,29 Multivariate logistic regression in our CTD cohort showed SSc diagnosis (and a high SOFA score) to be independent risk factors for non-survival. Most of the diseased SSc patients had a known pulmonary involvement. A large-scaled cohort study (5860 SSc patients) found infections to be the major reason of death among non-SSc-related causes. 41 Additional ROC analysis confirmed a good and comparable predictive power of all 3 investigated ICU scores (SAPS II, SOFA and APACHE II) in our cohort. SOFA score has been shown to be associated with mortality in patients with systemic vasculitis as well as rheumatoid arthritis before. 34,35,42 –44 Contrary to our results, the study of Zamir et al. found the APACHE II score to be a stronger predictor of mortality (AUC 0.82). 40 The determined cut off values for each score (see Figure 1 for details) might be helpful for clinical decisions in septic patients with CTDs.
No distinct immunosuppressive medication was associated with mortality, although we have found a trend toward a higher mortality associated with cyclophosphamide therapy. Rituximab treatment was not linked to mortality in our cohort.
This study has certain limitations. The sample size might be relatively small, but it is quite comparable to other investigations regarding ICU treatment of CTD patients. Furthermore, we have focused on septic CTD patients requiring ICU treatment resulting in a rather homogenous cohort. Since the study is retrospective, there might be a misclassification risk due to faulty ICD-10 coding. This risk has been reduced to a large extent by double-checking the diagnoses using the present records. Since the investigation was performed at a tertiary care hospital, there may also be a bias in disease severity. Eventually, due to the rareness of some of the entities, different CTDs have been summarized in this study. Nevertheless, we believe that the results contribute to the understanding of septic CTD patients under ICU treatment.
Conclusions
To our knowledge, this is the first investigation to exclusively determine the mortality of ICU treatment requiring sepsis in patients with connective tissue diseases. The overall mortality is high and mainly driven by the increased mortality among patients with SSc. The diagnosis of SSc and the SOFA score are independently associated with sepsis mortality. Common ICU scores demonstrated a good power in predicting sepsis mortality.
Footnotes
Authors’ Note
Marco Krasselt conceived the project, collected and interpreted the data, performed the statistical analysis, and drafted the manuscript. Christoph Baerwald contributed to data collection, interpretation and was involved in manuscript drafting. Sirak Petros was responsible for ICU patient care and contributed important intellectual content to the manuscript. Olga Seifert was involved in the statistical analysis as well as manuscript preparation. All authors read and approved the final manuscript. All procedures performed in this survey were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Data obtained in this study did not interfere with the course of treatment for patients included.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Professor Baerwald received lecture fees from Merck, MSD, Mundipharma and Pfizer.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.