
Abstract
Introduction/Background:
Vasculitis patients have a high risk for infections that may require intensive care unit (ICU) treatment in case of resulting sepsis. Since data on sepsis mortality in this patient group is limited, the present study investigated the clinical characteristics and outcomes of vasculitis patients admitted to the ICU for sepsis.
Methods:
The medical records of all necrotizing vasculitis patients admitted to the ICU of a tertiary hospital for sepsis in a 13-year period have been reviewed. Mortality was calculated and multivariate logistic regression was used to determine independent risk factors for sepsis mortality. Moreover, the predictive power of common ICU scores was further evaluated.
Results:
The study included 34 patients with necrotizing vasculitis (mean age 69 ± 9.9 years, 35.3% females). 47.1% (n = 16) were treated with immunosuppressives (mostly cyclophosphamide, n = 35.3%) and 76.5% (n = 26) received glucocorticoids. Rituximab was used in 4 patients (11.8%).The in-hospital mortality of septic vasculitis patients was 41.2%. The Sequential Organ Failure Assessment (SOFA) score (p = 0.003) was independently associated with mortality in multivariate logistic regression. Acute Physiology And Chronic Health Evaluation II (APACHE II), Simplified Acute Physiology Score II (SAPS II) and SOFA scores were good predictors of sepsis mortality in the investigated vasculitis patients (APACHE II AUC 0.73, p = 0.02; SAPS II AUC 0.81, p < 0.01; SOFA AUC 0.898, p < 0.0001).
Conclusions:
Sepsis mortality was high in vasculitis patients. SOFA was independently associated with mortality in a logistic regression model. SOFA and other well-established ICU scores were good mortality predictors.
Key Points
Mortality in vasculitis patients with sepsis is high with 41.2%.
SOFA is independently associated with sepsis mortality.
APACHE II, SAPS II and SOFA have a good predictive power in septic vasculitis patients.
Introduction
Systemic vasculitides are rare conditions causing blood vessel inflammation and, potentially, consecutive organ damage. They are a heterogenous group of diseases and differ not only in size of the affected vessels but also in etiology, clinic and prognosis. 1 While ANCA [antineutrophil-cytoplasmic antibodies]-associated vasculitides (AAV) mainly involve small vessels, giant cell arteritis (GCA) typically affects medium- and large-sized vessels. 1 Due to their systemic character, vasculitides may lead to life-threatening complications such as aortic dissection, rapid-progressive glomerulonephritis and lung as well as cerebral involvement. 2 Vasculitis patients are known to have a high risk for infections, particularly due to the required immunosuppressive treatment. 3 One of the main reasons for Intensive Care Unit (ICU) admission are infections and sepsis. 4 –10 In patients with GCA, the risk for infections is increased up to 55% in the first 2 years of treatment. 11 As we know from AAV, infections during immunosuppressive therapy greatly contribute to mortality, 12 making major infections one of the 2 most important causes for death besides vasculitis itself. 10,13,14 The predominant infection site are the lungs. 4,7,10,12 –14
Remarkably, despite (inter-)national recommendations, 15,16 vaccination rates for preventable pathogens (e.g. Streptococcus pneumoniae, Influenza) are low among patients with inflammatory rheumatic diseases and immunosuppression in general. 17 –19
Contrary to patients with Rheumatoid Arthritis, 20 investigations on vasculitis and intensive care treatment for sepsis are scarce or address ICU treatment in general without focusing on sepsis in particular. 4 –8,10,21 –24
We therefore planned to investigate retrospectively the outcome of sepsis in necrotizing vasculitis patients requiring intensive care treatment in a university hospital in Germany.
Methods and Study Design
All adult necrotizing vasculitis patients admitted to the medical ICU of the University Hospital of Leipzig for sepsis between 2006 and 2019 were retrospectively analyzed. To extract the data, the hospital records were searched using the International Classification of Diseases (ICD)-10- codes (German modification 2019) of patients admitted to the medical ICU (A39.x-A41.x for sepsis and M31.x for the different vasculitis entities). The integrity of both diagnoses was double-checked independently by 2 of the authors (MK and CB) reviewing medical records as well as discharge letters. All diagnoses of the identified patients were found to be appropriate.
Sepsis severity is assessed and routinely documented in the electronic patient chart in the ICU using SOFA, APACHE II and SAPS II scores. Data regarding patient demographics, clinical and laboratory parameters were obtained at the time of ICU admission.
The ethics committee of the University of Leipzig has approved the design of the study (Reg-No. 352/19-ek).
Biostatistical Analysis
Continuous data were described using either mean and standard deviation (SD) or median and interquartile range (IQR). Categorical data were described by absolute or relative frequencies. To compare frequencies of categorical variables, Chi-squared tests were performed. To compare continuous data, student’s t test or Mann-Whitney U test, as appropriate, was used after performing Shapiro-Wilk normality test. Logistic regression, adjusted for age and sex, was used to identify independent risk factors for non-survival. All significant variables were included into the final regression model. To further investigate the power of ICU scores such as APACHE II in predicting mortality, receiver operating characteristic (ROC) analysis was conducted. A significant statistical difference was assumed when the p value was less than 0.05. All analyses were conducted by using SPSS Version 24 for Mac (IBM, Chicago, IL, USA).
Results
Thirty-four patients with necrotizing vasculitis were admitted to the ICU for sepsis (mean age at admission 69.0 ± 9.9 years, 35.3% female) during the studied period. Prior to ICU admission, 47.1% (n = 16) were treated with immunosuppressives (mostly cyclophosphamide, 35.3%) and 76.5% (n = 26) received glucocorticoids. Biologic therapy was used in 11.8% (rituximab, n = 4) of the patients (Table 1). The mean ICU length of stay was 12.1±17.2 days.
Immunosuppressive Medication at ICU Admission. Given are Numbers and % in Brackets or Mean ± Standard Deviation (SD).
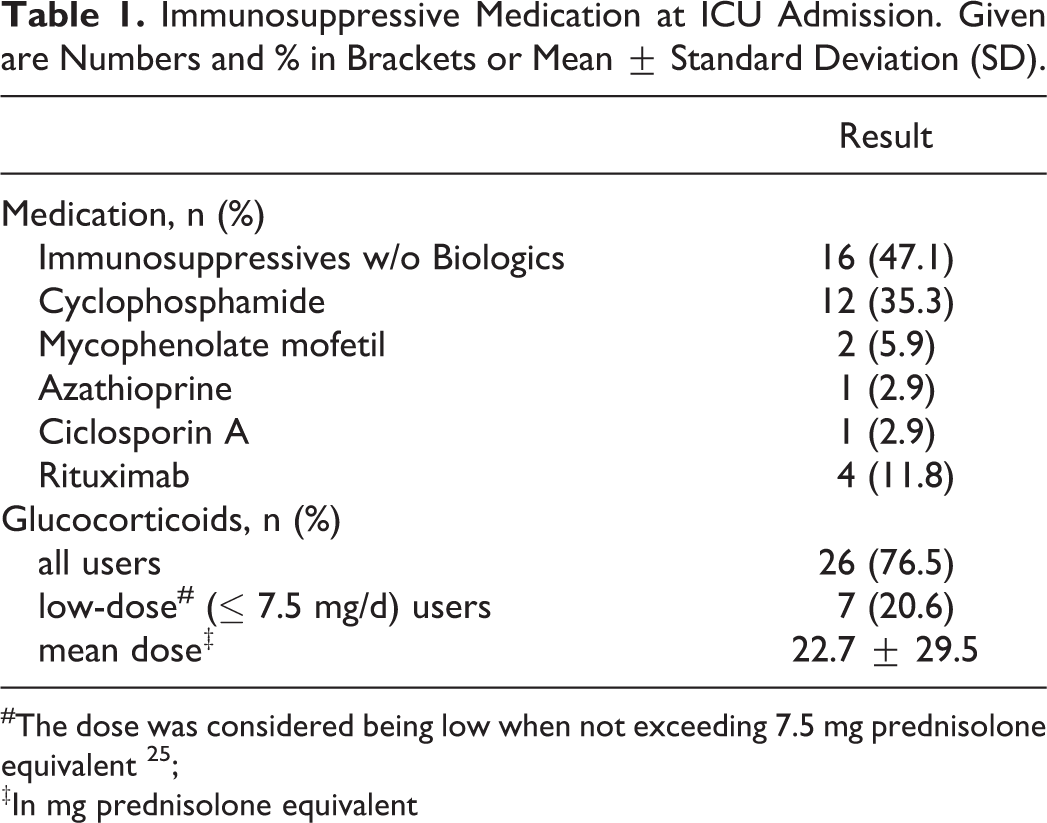
#The dose was considered being low when not exceeding 7.5 mg prednisolone equivalent 25 ;
‡In mg prednisolone equivalent
During intensive care treatment, 27 patients (79.4%) required mechanic ventilation, 26 patients (76.5%) were on vasopressor support and 21 patients (61.8%) on renal replacement therapy (RRT). Clinical data are presented in Table 2 , and details on the immunosuppressive medication in Table 1. More than two third of the patients (70.6%) had an infection of the lower respiratory tract.
Clinical and Laboratory Data of the Septic Vasculitis Patients. Given are Numbers and % in Brackets or Mean ± Standard Deviation (SD).
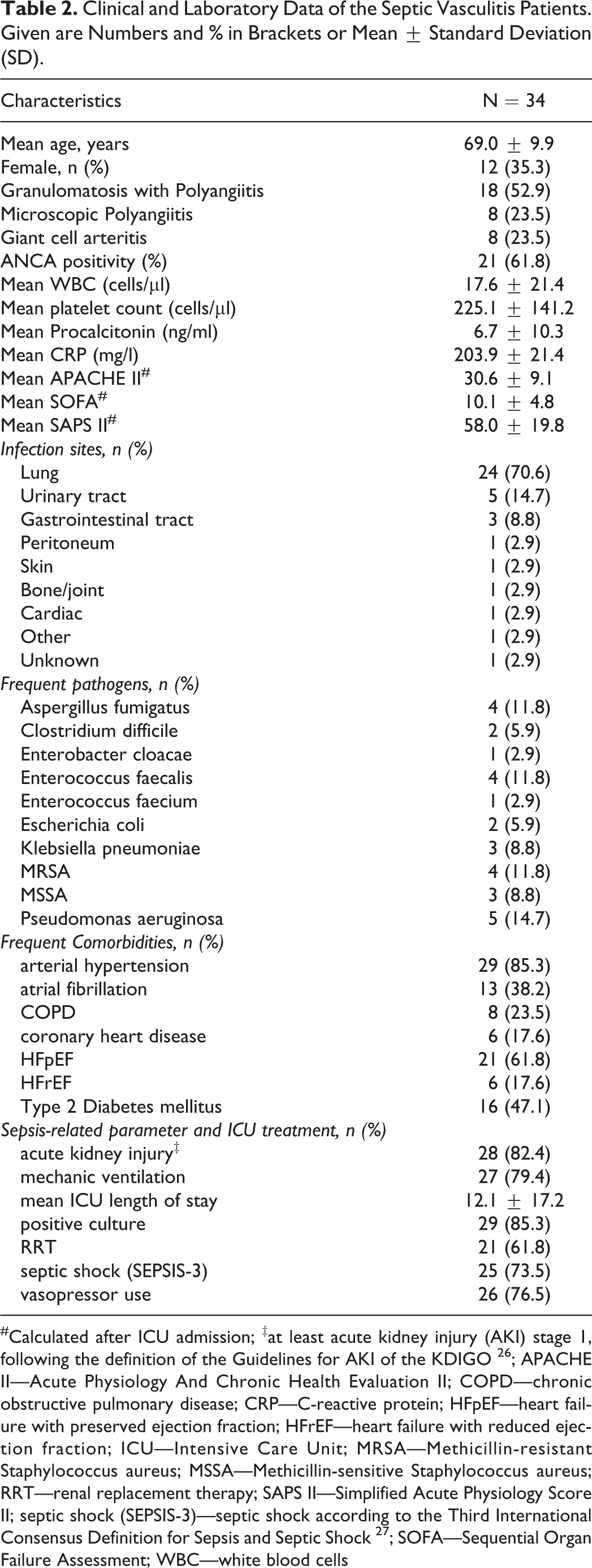
#Calculated after ICU admission; ‡at least acute kidney injury (AKI) stage 1, following the definition of the Guidelines for AKI of the KDIGO 26 ; APACHE II—Acute Physiology And Chronic Health Evaluation II; COPD—chronic obstructive pulmonary disease; CRP—C-reactive protein; HFpEF—heart failure with preserved ejection fraction; HFrEF—heart failure with reduced ejection fraction; ICU—Intensive Care Unit; MRSA—Methicillin-resistant Staphylococcus aureus; MSSA—Methicillin-sensitive Staphylococcus aureus; RRT—renal replacement therapy; SAPS II—Simplified Acute Physiology Score II; septic shock (SEPSIS-3)—septic shock according to the Third International Consensus Definition for Sepsis and Septic Shock 27 ; SOFA—Sequential Organ Failure Assessment; WBC—white blood cells
Fourteen out of 34 patients died, resulting in an in-hospital mortality of 41.2%. Of the deceased patients, 12 suffered from AAV and 2 of GCA. Mortality within those 2 groups was therefore 46.1 and 25%, respectively. All deceased GCA patients suffered from a septic shock. The mean glucocorticoid dose was 22.7 mg ± 29.5 prednisolone equivalent (27.1 mg ± 32.9 for AAV and 9.6 mg ± 6.2 for GCA). Regarding the individual medication, including glucocorticoids, no significant difference in mortality was found, with a trend for a higher mortality under Mycophenolate mofetil (MMF) (p = 0.081, Table 3). Stratification for disease entity did not change this result. Furthermore, no association between sepsis mortality and the site of infection was found (data not shown). A positive culture for methicillin-sensitive staphylococcus aureus (MSSA) was significantly associated with mortality (p = 0.03), while a positive Pseudomonas aeruginosa culture did not reach significance in that regard (p = 0.056). Interestingly, all positive MSSA as well as MRSA cultures were obtained from GPA patients (p = 0.04 for MRSA, n.s. for MSSA).
Bivariate Analysis of Comorbidities and other Potential Risk Factors for Mortality. Given are Numbers and % in Brackets, Mean ± Standard Deviation (SD) or Median and Interquartile Range (IQR) in Brackets, Respectively.
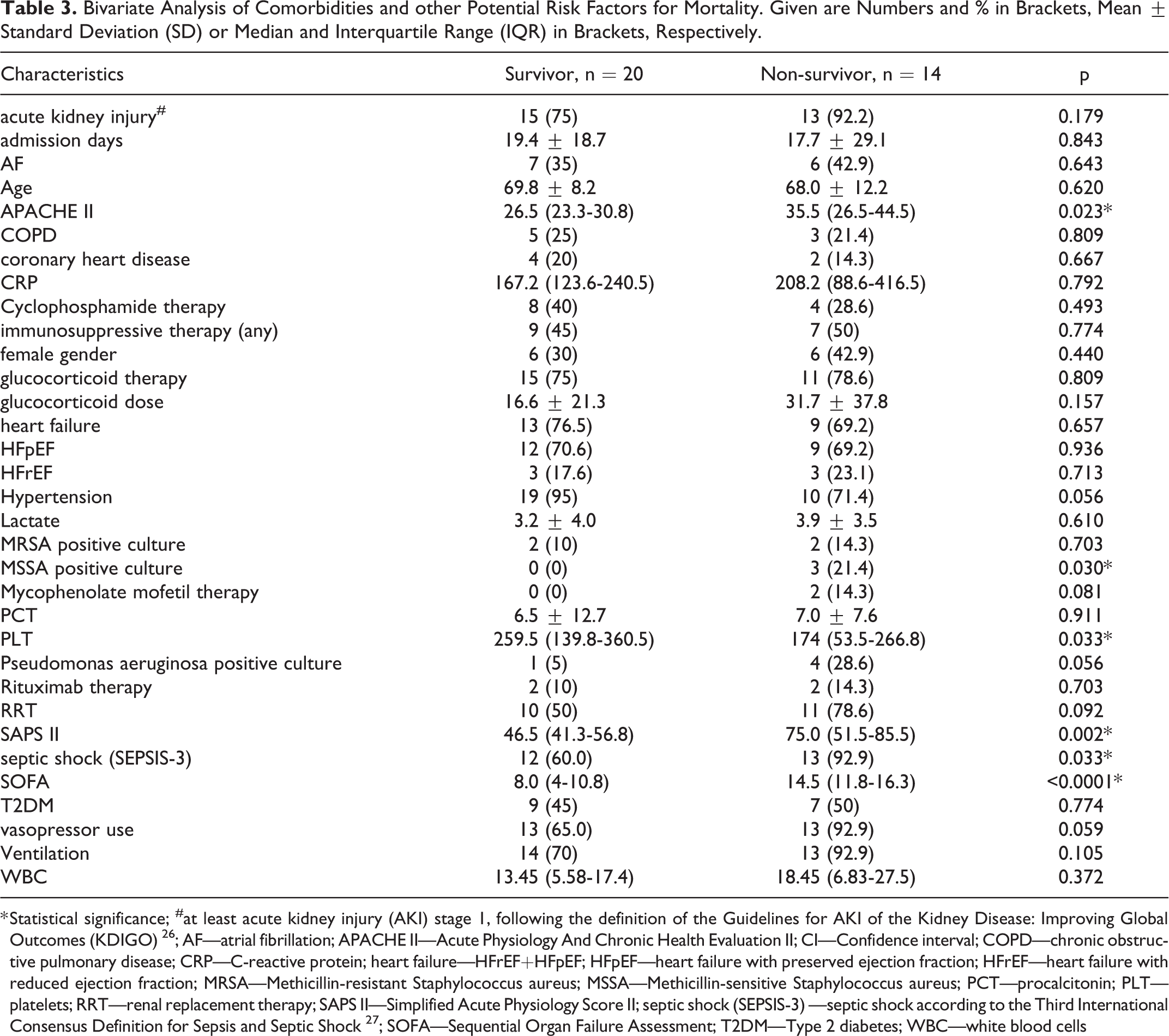
* Statistical significance; #at least acute kidney injury (AKI) stage 1, following the definition of the Guidelines for AKI of the Kidney Disease: Improving Global Outcomes (KDIGO) 26 ; AF—atrial fibrillation; APACHE II—Acute Physiology And Chronic Health Evaluation II; CI—Confidence interval; COPD—chronic obstructive pulmonary disease; CRP—C-reactive protein; heart failure—HFrEF+HFpEF; HFpEF—heart failure with preserved ejection fraction; HFrEF—heart failure with reduced ejection fraction; MRSA—Methicillin-resistant Staphylococcus aureus; MSSA—Methicillin-sensitive Staphylococcus aureus; PCT—procalcitonin; PLT—platelets; RRT—renal replacement therapy; SAPS II—Simplified Acute Physiology Score II; septic shock (SEPSIS-3) —septic shock according to the Third International Consensus Definition for Sepsis and Septic Shock 27 ; SOFA—Sequential Organ Failure Assessment; T2DM—Type 2 diabetes; WBC—white blood cells
In a bivariate analysis, septic shock was diagnosed more often in non-survivors (p = 0.033, Table 3). Moreover, higher SOFA, SAPS II and APACHE II scores were found in non-survivors (p < 0.0001, p = 0.002, p = 0.023, respectively). Platelets were significantly lower among non-survivors (p = 0.033).
In a multivariate analysis, only the SOFA score (Odds ratio 1.711, 95% confidence interval 1.19-2.45, p = 0.003) remained independently associated with non-survival.
ROC analysis (Figure 1) demonstrated a good predictive power of SOFA, SAPS II and APACHE II scores for sepsis mortality in vasculitis patients. Area under the curve (AUC) and predictive power were found to be the highest for SOFA score (AUC 0.898 ± 0.06, 95% CI 0.780 -1.000, p < 0.0001).
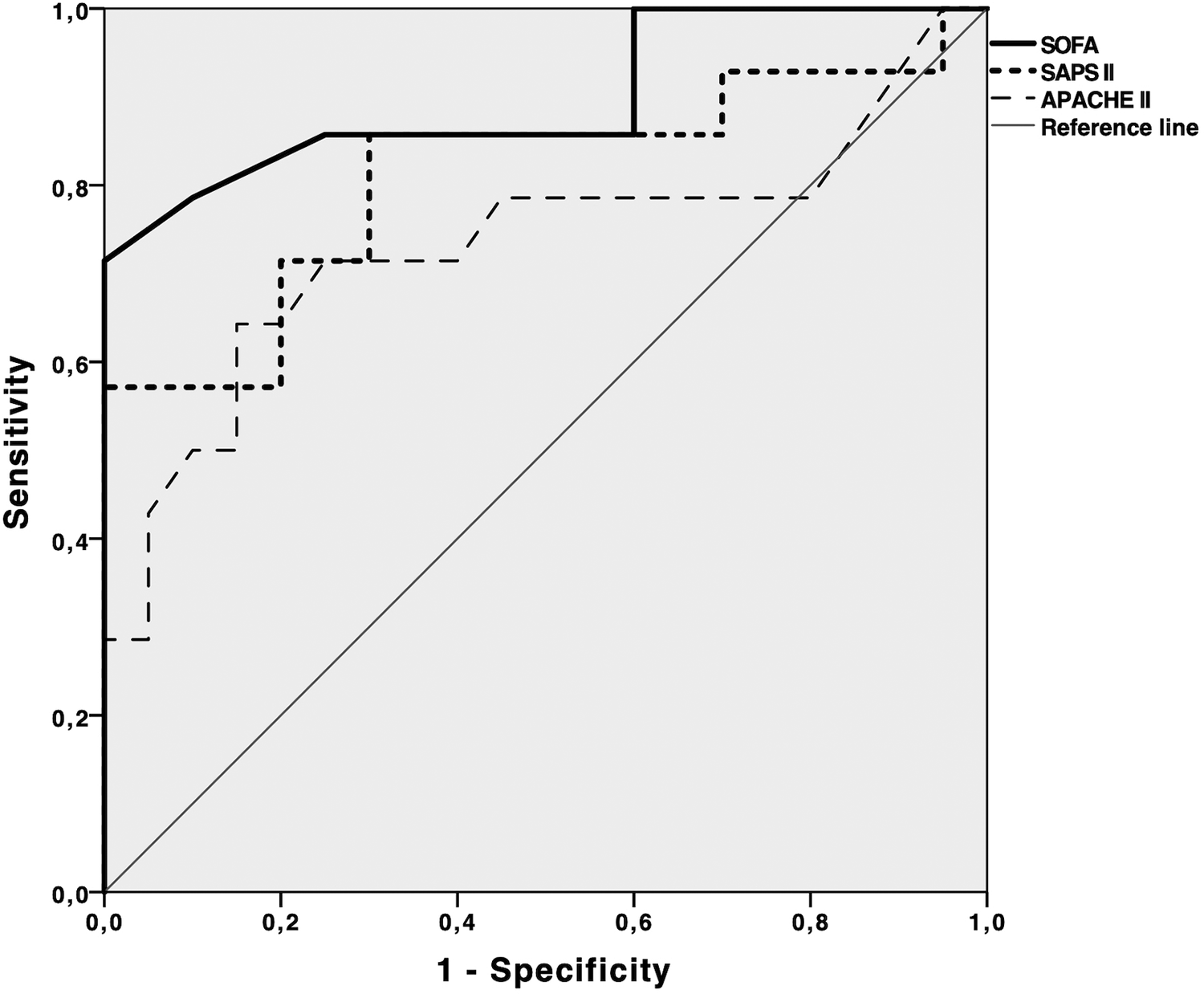
Receiver operating characteristic (ROC) analysis of the value of the SOFA, SAPS II and APACHE II score in predicting in-hospital mortality. Area under the curve (AUC) is given with standard error (±SE), 95% confidence interval (CI) and p value.
Discussion
The aim of this study was to evaluate the in-hospital sepsis mortality of necrotizing vasculitis patients requiring intensive care. With 41.2%, sepsis mortality was found to be high, which might be partly explained by the high prevalence of septic shock in our cohort (almost three-fourth). While septic shock was significantly more prevalent among non-survivors, multivariate analysis did not show septic shock to be independently associated with non-survival in our logistic regression model. This finding can be explained by the strong association of shock with other variables in the model (e.g., SOFA). Septic shock highly contributes to sepsis mortality. 7,28 On the other hand, the tertiary character of our hospital (admission of predominantly severely ill patients, also transferred directly from other hospitals) could be another reason for the high mortality. Additionally, more than three-fourth of the patients received glucocorticoids at a mean daily dose of >20 mg prednisolone equivalent. The contribution of glucocorticoid use >5 mg prednisolone equivalent to mortality of rheumatic patients in intensive care treatment is well known. 29 In this context, high glucocorticoid doses in the year before ICU admission as well as dose increasing of glucocorticoids during ICU stay are associated with a reduced survival too. 30 Nevertheless, bivariate analysis did neither find the mere use of glucocorticoids nor glucocorticoid dose to be associated with mortality, although the mean dose of glucocorticoids was almost twice as high in non-survivors compared to survivors. The dose of glucocorticoids in both groups is spread widely and the high standard deviation (survivors and non-survivors) exceeds the mere difference between the groups. The difference could therefore not reach statistical significance. Mortality was higher among patients with AAV than patients with GCA. This difference can be readily explained by the more likely involvement of organs such lungs or kidneys in AAV and the higher GC doses in this patients. With 25%, sepsis mortality in GCA alone was comparable to the general population. While it could be reduced in the last decades, mortality still reaches almost 30% for severe sepsis in the general population in the United States. 31 In Germany, general sepsis mortality (including severe sepsis and septic shock) was calculated 24.3%. 28
A literature search on mortality of vasculitis patients under intensive care only brought up studies on ICU treatment in general. 4 –8,10,21 –24 Investigations on ICU treatment for sepsis in particular are missing. We have found differing results while comparing our mortality to that in the literature. While some investigators showed a comparable mortality, (46.7-48%), 4,7 others reported both, substantially higher (55.6-60.9% 5,23 ) and lower (16-21% 6,8,10,24 ) mortality. These differences are mainly the result of differences in either the study cohort or the primary endpoint. Biscetti et al., 5 for instance, investigated a small group of vasculitis patients (n = 18), mainly suffering from AAV (77%). Mortality was high with 55.6%. Vasculitis patients admitted to the ICU for any reason were included, of whom 50% suffered from sepsis. The high mortality might be explained by the use of glucocorticoids in all the studied patients (100%) and a high proportion of additional use of immunosuppressants (66.7%). 5 A study from Poland found a high mortality of 60.9% in 23 patients with small-vessel vasculitis under intensive care. 23 Since ICU admission was not exclusively caused by sepsis, this finding is difficult to compare to ours. The investigation by Heijnen et al. included only 36% patients with a systemic vasculitis (64% were other, non-vasculitis systemic diseases such as sarcoidosis and systemic sclerosis), 60% were admitted to the ICU for infection. 6 The small proportion of vasculitis patients limits the meaningfulness of the reported mortality of 19 and 39% (ICU and in-hospital mortality) and makes it hardly comparable to our finding. Similarly, the study conducted by Dumas et al. consisted of only 26.2% vasculitis patients and also found a rather low mortality of 21%. 10 39.9% of patients were admitted to the ICU for infection. Khan reported a 28-day mortality of only 11% in a cohort of AAV patients, with only 18% of patients being admitted to ICU for infection and only 33% of patients who were in need of RRT. 8 Brünnler et al. 24 reported a mortality rate of only 16%, but the studied cohort consisted of patients with very different rheumatic diseases (including Rheumatoid Arthritis, Spondylarthritis and Connective Tissue Diseases). Vasculitides accounted for 13% only, the main reasons for admission were cardiovascular complications and infections (20 and 31% respectively). The median APACHE II score was low with 12 (2-33) compared to 26.3 (23.25-30.75) in survivors and 35.5 (26.5-44.5) in non-survivors in our cohort, emphasizing the exceeding severity and worse prognosis in our cohort.
Using multivariate logistic regression, the SOFA score could be identified as the only independent risk factor for mortality among our vasculitis cohort. Further ROC analysis confirmed a good predictive power of all investigated scores, but the SOFA score outperformed both SAPS II and APACHE II. The SOFA score has been shown to be associated with mortality in vasculitis patients before. 4,7,8,10 However, the predictive power of this score was higher in our cohort compared to the result of Haviv et al. (AUC 0.898 vs. 0.761). 4 In contrast to our study, Haviv et al. investigated any vasculitis ICU admissions, and both glucocorticoid use as well as RRT were more prevalent among their patients, probably reflecting severely ill patients with a higher mortality. Surprisingly, this assumption is not supported by either SOFA or APACHE II score, which were both lower than in our cohort. Contrary to the results of Haviv and Biscetti et al., 4,5 APACHE II score was significantly higher among non-survivors in our cohort and showed a good power in predicting mortality. Our findings are basically supported by the results of others, 6,22,24 who found significantly higher APACHE II scores among non-survivors. Nevertheless, comparing those studies to the results of our investigation seems difficult (the cohorts either consisted only partly of vasculitis patients or the cause of admission differed widely). Since we focused on septic vasculitis patients, the prognostic power of the APACHE II score might be better in this distinct condition. Our literature search only brought up 2 studies that also investigated SAPS II score in vasculitis patients. Cruz et al. reported significantly higher SAPS II scores among non-surviving vasculitis patients under intensive care, 22 being in line with our findings. Befort and colleagues similarly reported a higher SAPS II score in non-survivor vasculitis patients under ICU treatment. 21 In the cohort of Befort et al., SAPS II was also independently associated with mortality. Again, this fact is difficult to compare since main admission reason in that study was the vasculitis itself.
The fact that all MSSA and MRSA cultures in our cohort were obtained from GPA patients emphasizes the likely involvement of Staphylococcus aureus in the pathogenesis of GPA. 32,33
Rituximab (RTX) was not associated with increased mortality in our cohort, which is contrary to the results of Haviv et al. 4 Since the number of patients under RTX is low (n = 4 in both studies), the finding of a significant association by Haviv et al. is difficult to interpret.
Our study has several limitations. Due to the rarity of the vasculitides, the sample size is relatively small, but comparable to other investigations regarding ICU treatment of vasculitis patients. Since the study is retrospective, there may be the risk of misclassification due to incorrect ICD-10 coding. This risk has been reduced as far as possible by double-checking the diagnoses using the medical records. As a single-centre study at a university hospital, there may also be a bias in disease severity. Additionally, treatment of vasculitides has changed during the years. While conventional immunosuppressives such as cyclophosphamide or MMF were the cornerstones of induction and maintenance therapy in AAV for several decades (including a large amount of patients in this investigation), RTX was established as a suitable and effective replacement for both induction and maintenance therapy during the last years. 34 –37 As for GCA, the interleukin-6 receptor antagonist Tocilizumab is increasingly used as a steroid-sparing agent lately. 38,39 How these changing treatment regimens will affect the risk of infections and therefore sepsis mortality remains the subject of further investigations. Nevertheless, we believe that our results may contribute to the understanding of patients with necrotizing vasculitis suffering from sepsis and requiring ICU treatment.
Conclusions
To our best knowledge, this is the first study that exclusively investigated the mortality of sepsis in necrotizing vasculitis patients requiring ICU management. Mortality in those severely ill patients has been found to be high. The SOFA score was identified as the only parameter independently associated with sepsis mortality. All commonly used ICU scores (APACHE II, SAPS II and SOFA) demonstrated a good power in predicting sepsis mortality of vasculitis patients. Since the SOFA score showed the best predictive power, it might be the most appropriate prediction tool in septic vasculitis patients.
Footnotes
Authors’ Note
MK conceived the project, collected and interpreted the data, performed the statistical analysis, and drafted the manuscript. CB contributed to data collection, interpretation and was involved in manuscript drafting. SP was responsible for ICU patient care and contributed important intellectual content to the manuscript. OS was involved in the statistical analysis as well as manuscript preparation. All authors read and approved the final manuscript. All procedures performed in this survey were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Data obtained in this study did not interfere with the course of treatment for patients included.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. Professor Baerwald received lecture fees from Merck, MSD, Mundipharma and Pfizer.