
Abstract
Background:
MRI often requires general anesthesia in children, which carries risks, increases costs, and prolongs scan wait times.
Purpose:
Our study aimed to evaluate whether virtual reality (VR) simulations could familiarize children with the MRI experience to enable awake scans without anesthesia. Secondary objectives included assessing child anxiety and determining whether movement during the simulation correlated with scan quality.
Materials and Methods:
In this prospective study, 18 participants underwent a 10-minute VR simulation of an MRI procedure presented as an avatar-led game before their head MRI scan. Child and caregiver anxiety surveys were completed before the simulation and after the MRI. The VR software recorded head motion during the simulation, which was correlated with MRI scan quality.
Results:
All participants (n = 18) successfully completed an awake MRI after the simulation session, aiding clinical diagnoses. The average participant age was 5.0 years (±1.3 years). MRI quality assessments indicated 44.4% excellent, 27.8% high-acceptable, 22.2% acceptable, and 5.6% low-acceptable scan quality. No statistically significant changes in anxiety levels were observed. 94.1% of legal guardians reported the VR simulation was effective at preparing their child for the MRI scan.
Conclusion:
VR sessions were associated with a significant improvement in caregiver perceptions and enabled successful completion of MRI scans without the need for sedation in all children initially considered to require anesthesia. While no statistically significant reduction in anxiety was observed, the intervention resulted in diagnostic-quality imaging with minimal motion artifacts, supporting its utility as a strategy to facilitate pediatric MRI without anesthesia.
Introduction
Magnetic resonance imaging (MRI) has become increasingly popular in the pediatric population due to its excellent soft tissue resolution and lack of ionizing radiation. According to the National Health Services, 162 745 children, aged 0 to 14 years, had an MRI scan in 2022 to 2023 in England, a 4.6% increase from 155 215 in 2021 to 2022.1,2 With its growing use, ensuring children have a satisfactory experience while remaining still for optimal image acquisition is essential. MRI’s loud noises and confined space can cause anxiety and claustrophobia, making it challenging to endure a 30 to 45 minute scan.3,4 Tyc et al identified loud noises, head coil placement, and small space as distressing factors. 5 While anesthesia ensures stillness, it requires significant resources and costs. A Canadian study found that sedated MRIs are 9.56 times more costly to hospitals than awake scans. 6
To address these challenges, various age-based non-sedative techniques are used to enhance compliance, comfort, and reduce anxiety and motion artifacts. Swaddle-sleep method, mock scanners, MR-compatible video goggles, and play therapy have proven to be effective techniques.7-9 An emerging approach is virtual reality (VR), which creates a 3D simulated environment for user interaction.10,11 VR is increasingly applied in healthcare as a distraction and preparation tool.11,12 Stunden et al compared different preparation methods, including VR simulation, manuals, and child-life programs, and found caregivers expressed highest satisfaction with VR and child-life programs. 13
VR systems used to prepare children for MRI can vary widely in their design and implementation. Immersive, headset-based VR provides a highly engaging experience closely simulating the MRI environment but may be difficult for very young children who cannot tolerate wearing a headset, and can cause motion sickness and discomfort. By contrast, tablet-based VR is more accessible and flexible, and allows caregivers to participate, though it may be less representative of a true MRI simulation, limiting its desensitization impact to the MRI environment.
Building on these advancements, our study introduced a VR platform simulating a head MRI experience, from donning the head coil to entering the gantry, to desensitize children to noises and confined space. We hypothesized that after VR, children aged 3 to 7 would be sufficiently prepared and comfortable for a non-sedated scan. We also aimed to assess whether VR reduces anxiety and whether movement during simulation correlates with awake MRI quality.
Methods
Study Setting
We conducted a prospective study at the Children’s Hospital of Eastern Ontario, Canada following REB approval (#22/85X). Written informed consent was obtained from all participants’ caregivers.
Patient Population
Eighteen eligible pediatric patients were selected from a sedated head-MRI waitlist or referred by a pediatric neurologist. Their sedated MRI order remained active until a successful non-sedated MRI was confirmed, ensuring their position on the waitlist was maintained. Inclusion criteria were children aged 3 years and above, requiring a non-contrast head MRI under general anesthetic (GA). Exclusion criteria included severe cognitive impairments, deafness or blindness, active migraine, or active earaches (as per manufacturer’s guidelines), 14 or a previous successful awake MRI.
Virtual Reality Session
During the 30-minute scheduled VR sessions, children donned VR goggles (HP Reverb VR Headset; HP Development Company) and followed a 10-minute avatar-led MRI simulation by EmmaRye. 15 Sessions occurred 1 to 2 hours before the MRI, except for participant 8 (VR session occured 6 days before the scan). The VR simulations took place outside of the MRI suite in an adjacent room, to familiarize the child to the MRI environment. All sessions were conducted by the same research assistant to ensure consistency. The simulation began with a 5-minute avatar-guided breathing technique introduction, followed by a 5-minute simulated MRI scan, which included entering the scanner, head coil placement, and the scanner’s noises. To successfully complete the simulation, children had to remain still for a cumulative of 5 minutes, which was tracked by an avatar collecting magical dust (Figure 1). Movement was monitored, and corrective feedback was provided through the VR headset.

Image portraying the fairy avatar and magical dust collection used in the VR simulation. During the VR simulation, children are given the option to choose either a robot or a fairy to guide them through the simulation. Once they enter the virtual MR simulation session, a visual representation of the time remaining is shown next to the avatar.
Children were informed that they could pause or end the simulation at any time if they experienced discomfort. Participants were reassured that withdrawing from the study would not affect their position on the sedated-MRI waitlist.
Data Collection
Various separate datasets were collected during the study, including patient demographics, caregiver and perceived child anxiety levels, perceived VR effectiveness, movement during VR simulation, and MRI scan quality.
Caregivers were provided with 2 bilingual (French and English) questionnaires to complete before the VR simulation. The first questionnaire gathered demographic data, while the second utilized a Likert scale (ranging from strongly agree to strongly disagree) to assess their anxiety levels, the child’s perceived anxiety toward the MRI, and caregivers’ beliefs regarding the effectiveness of the VR sessions. Categories on the Likert scale were combined into agree, disagree, and neutral categories due to the small sample size and similarity between responses.
Within 2 days of their MRI scan, an identical questionnaire was sent to the caregivers to evaluate changes in anxiety and gather feedback.
MRI Scan
Following the simulation, participants underwent the MRI scan according to routine departmental policy. Scan durations varied based on the clinical requirements, with all participants receiving a rapid-MRI sequence (5-minute protocol) for baseline imaging. If the child remained still, additional sequences were added by the radiologist based on clinical requirements. If the child was unable to remain still for a full-length scan, we ensured key sequences were acquired to maximize diagnostic information. All participants used MR-safe video goggles to watch a movie during the scan as per hospital protocols, and caregivers were welcome to accompany the participant into the MRI unit upon request.
Once the scans were completed, 2 pediatric radiologists (NG, EM; years of experience 14, 24 respectively) independently and blindly to patient information, completed surveys to categorize scans based on their quality and motion artifact. The radiologists determined whether the scans were diagnostic or not, and whether a sedated-MRI was still required. Scans were ranked as “poor”, “acceptable”, and “excellent” for quality of scans and “poor”, “acceptable”, and “none” for motion artifact.
Statistical Analysis
Survey results were analyzed using a Stuart-Maxwell Marginal Homogeneity Test to compare dependent samples with categorical data. A P-value of <.05 was considered statistically significant. Throughout the simulation, the VR software automatically collected motion data including head position and head rotation. Mean distances for head position and rotation were calculated using the respective formula: sqrt(x2 + y2 + z2) for head position coordinates (x, y, z), and sqrt(alpha2 + beta2 + gamma2) for head rotation coordinates (alpha, beta, gamma).
Results
Participants Demographics and Adverse Effects
Eighteen pediatric participants were included, of a mean age of 5.0 years (±1.3 years). Eleven were male (61.1%) and 44.4% of the participants had previous imaging studies done (3 participants had previous sedated MRIs; Table 1). Of the 18 participants, 16 completed the VR training traditionally. One participant (participant 4) reported being unable to see through the VR goggles, and another participant (participant 8) experienced dizziness. These 2 children completed the session using a computer screen.
Demographic Characteristics of Study Participants.
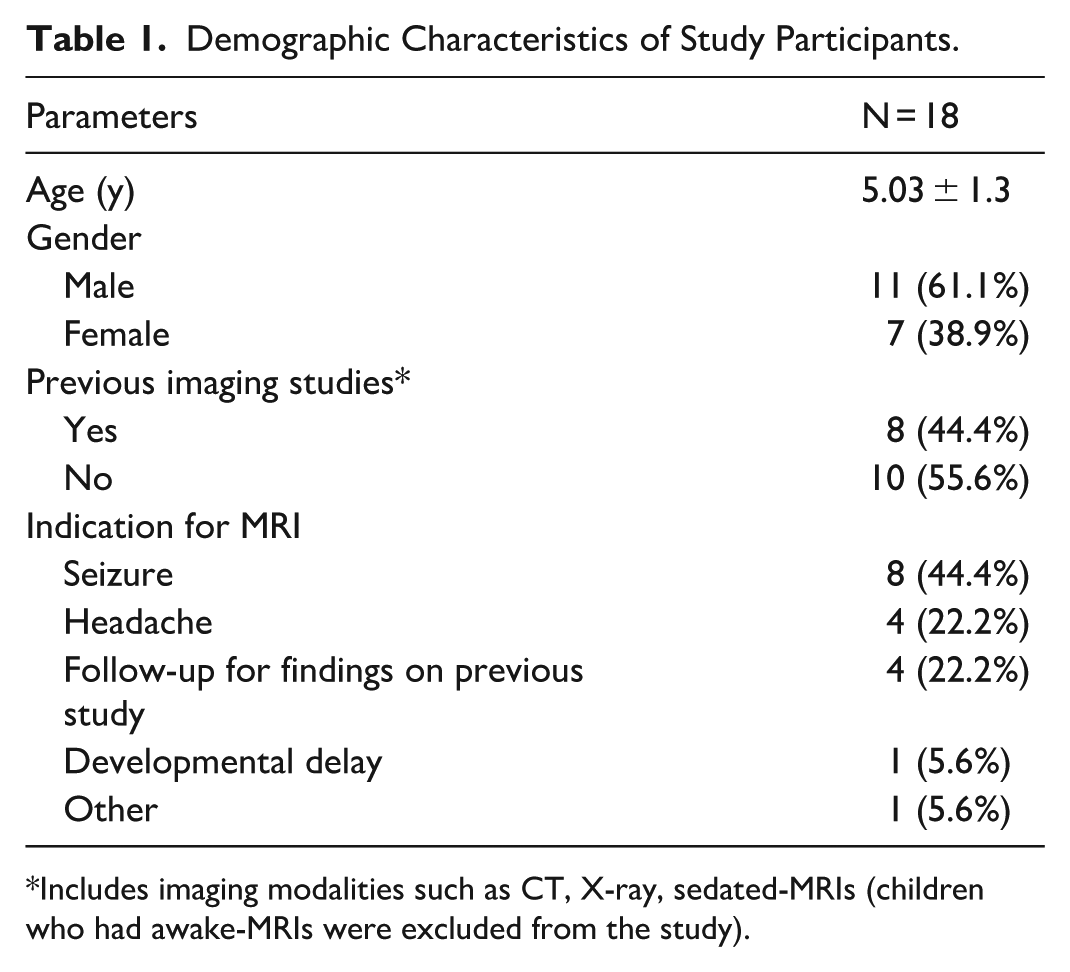
Includes imaging modalities such as CT, X-ray, sedated-MRIs (children who had awake-MRIs were excluded from the study).
VR Session
The per minute mean change in head position (Figure 2) and in head rotational movement (Figure 3) were analyzed throughout 17 participants’ sessions (data from participant 3 is incomplete due to data retrieval error). The data reveals significant individual variability in movement patterns. Several children (1, 6, 7, 9, 10, 11, 13, 15, 17) demonstrated minimal movement throughout the session, with their mean position change remaining close to zero. Children 4, 8, 16, and 18 exhibited notable sporadic spikes in movement, indicating periods of significant activity. Participants 16 and 18 were visibly anxious during the VR simulation, requiring pauses in the session.
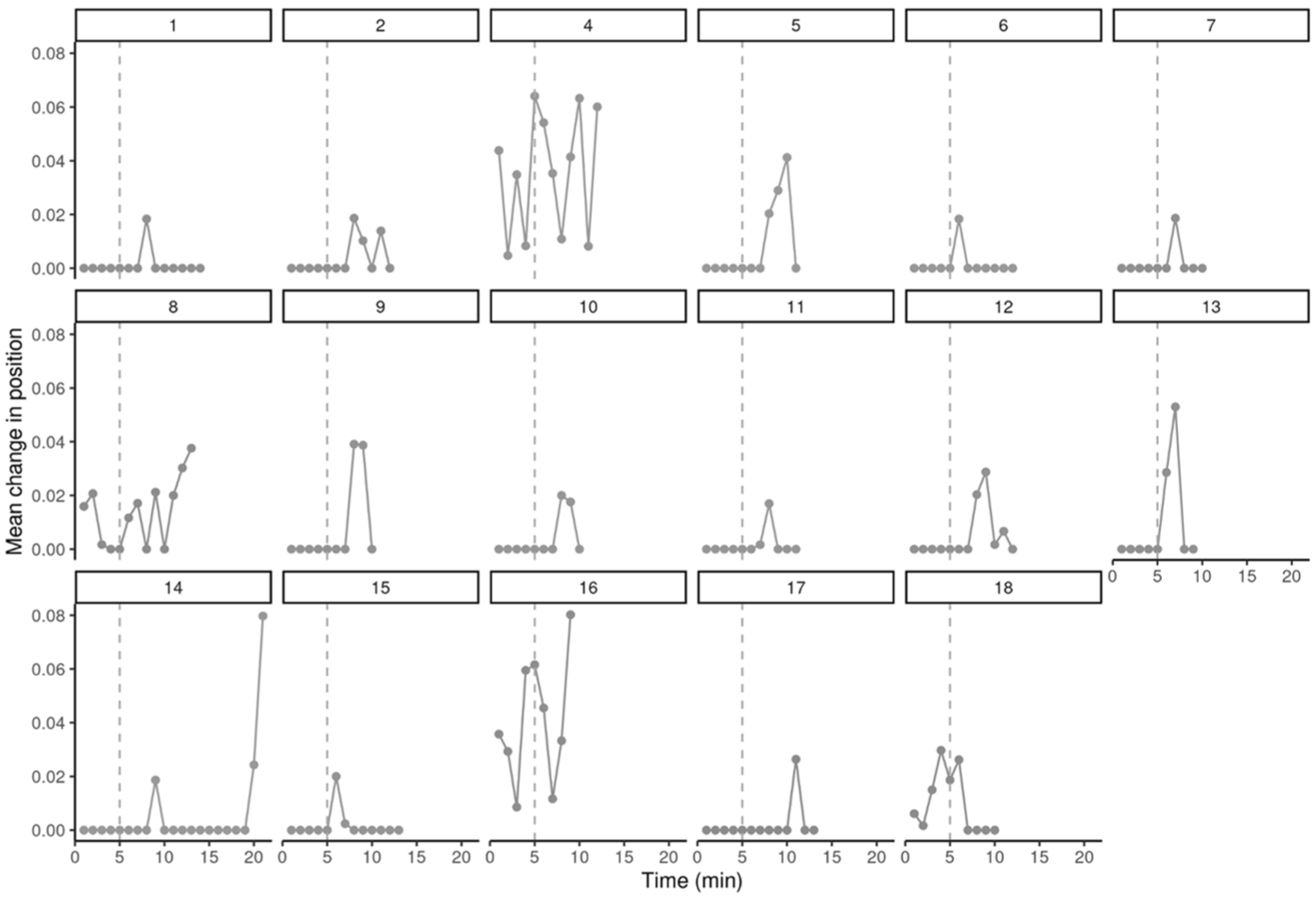
Mean change in head position by time and participant. The distance between each point was calculated using the following formula: sqrt(x2 + y2 + z2) where x, y, and z are the head position coordinates. The starting point for each measurement was the previous coordinates of the previous time point. A vertical dotted line is added to highlight the fifth minute of the training when participants virtually enter the MRI scanner. Incomplete data for participant 3.
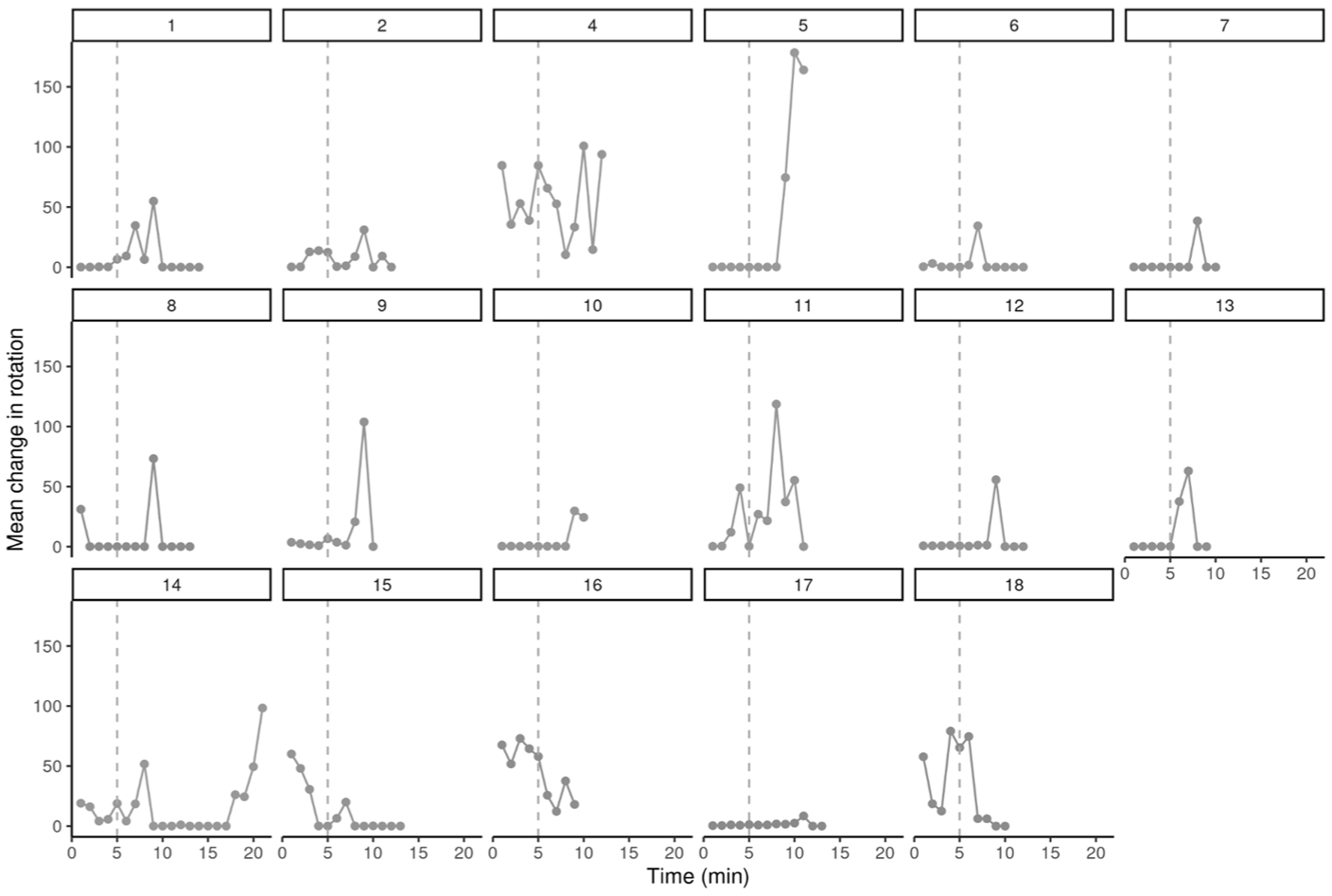
Mean change in head rotation by time and participant. The distance between each point was calculated using the following formula: sqrt(alpha2 + beta2 + gamma2) where alpha, beta, and gamma are the head rotation coordinates. The starting point for each measurement was the previous coordinates of the previous time point. A vertical dotted line is added to highlight the fifth minute of the training when participants virtually enter the MRI scanner. Incomplete data for participant 3.
Similarly, the mean change in head rotational movement for the 17 participants, showed notable individual differences in rotational pattern. Many children (eg, 1, 2, 5, 6, 7, 8, 9, 10, 12, 13, and 17) exhibited minimal rotational movement throughout their training, with occasional larger rotations. Several of them showed significant spikes (eg, 4, 11, 14, 15, 16, and 18) in rotational movement, which were irregular and varied in timing across individuals. After minute 5 of the VR training, a general increase in movement (head position or rotation) was observed across participants.
Pre-VR and Post-MRI Survey Results
The percentage of caregivers who disagreed with feeling anxious pre and post-MRI were similar (16.7% vs 23.5% respectively). Caregiver anxiety levels remained largely stable, with no significant change observed (P = .819). Similarly, no significant change was observed in reported child anxiety levels (P = .082), although a small percentage (25.0% pre-MRI vs 41.2% post-MRI) of caregivers reported that they disagree with their child feeling anxious about getting a scan. 31.3% of caregivers agreed to the statement “my child will be successful at getting a non-GA MRI before the VR session”. 56.3% of caregivers believed the VR session will be effective at helping their child succeed, compared to 94.1% who reported that the VR session was effective after their MRI scans (P = .030). Of note, one caregiver did not complete the post-MRI survey (Table 2).
Pre-VR and Post-MRI Survey Results.
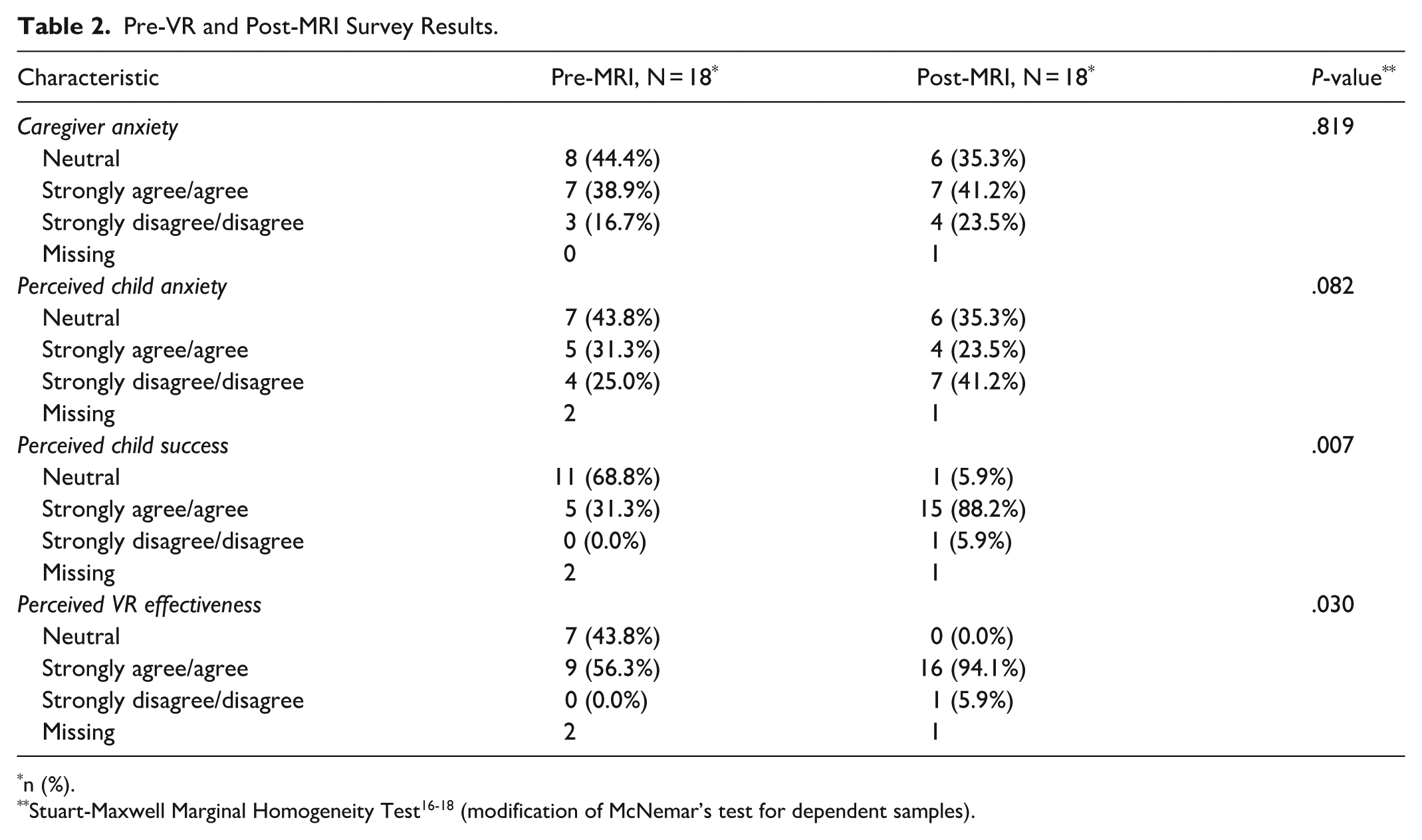
n (%).
MRI Scans
The mean scan length was 32.8 minutes (±10.5 minutes), with a total time spent per participant (VR session and MRI scan) of 44.1 minutes (±10.0 minutes). Maximum and minimum total time spent were 29 and 68 minutes, respectively. Results of the MRI scan analysis is shown in Table 3. 44.4% (n = 8) were of excellent quality with 5.6% (n = 1) having low-acceptable image quality. 44.4% (n = 8) high-acceptable motion artifact and 5.6% (n = 1) having low-acceptable motion artifact. Although no statistically significant correlation can be deduced from the data, a general trend can be seen whereby participants with less overall head movement during the VR simulation demonstrated higher quality MRI scans.
Characteristic of MRI scans. Characteristics represent a combined classification based on 2 radiologists’ expertise.
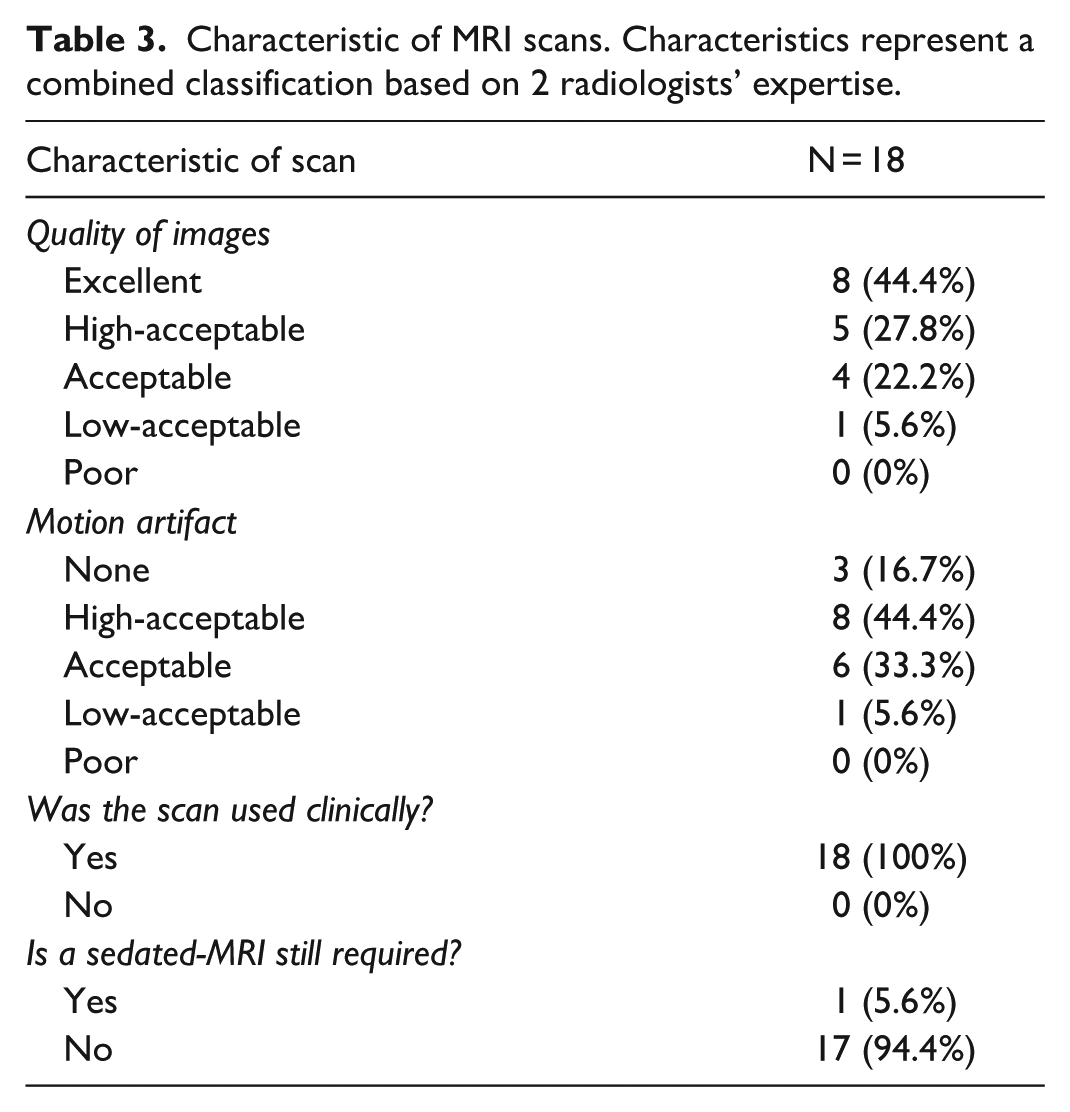
All MRI scans were used for clinical diagnosis, with one radiologist recommending a GA-MRI for one participant (participant 14), if their physician requested it. Based on their clinical findings and indication for scan, the limited images obtained were sufficient and no GA-MRI was needed.
Discussion
The purpose of this pilot study was to evaluate whether providing children with a VR simulation of an MRI scan would adequately prepare them for an awake MRI, potentially reducing the need for sedation. We also aimed to assess whether the VR intervention could reduce anxiety regarding the scan, gauge caregiver perceptions, and determine the percentage of caregivers who believed their child would successfully complete an awake MRI. Key metrics included scan success rate, image quality, and the correlation between head movement during VR and image quality.
Previous research has shown that a negative, anxiety-provoking healthcare experience can affect a child’s psychological wellbeing.19,20 Although our survey did not show statistically significant change in perceived child anxiety pre-VR and post-MRI (as scored by caregivers), a slight decrease was observed (41.2% reported as “disagree” with being anxious, compared to 25.0% pre-VR). This suggests that increased exposure through VR could help minimize the stress associated with undergoing an MRI. A recent study by Saliba et al reported similar findings, where a VR group (ages 4-14 years) showed significantly reduced anxiety post-VR compared to a control group. 21
He et al found that therapeutic play interventions reduced negative emotional manifestations and postoperative pain in children. 22 Similarly, our study suggests that VR simulations can familiarize children with the MRI environment, potentially reducing pre-procedural anxiety and improving the overall experience. Caregiver feedback indicated high perceived benefit of the VR simulation, noting its usefulness in preparing children, and willingness to repeat the experience. They appreciated testing their child’s ability to stay still in a controlled environment. As with many pediatric interventions, caregiver engagement is a key determinant of success. When carers believe in and feel comfortable with an intervention, such as shown with the VR simulation, their positive attitude can facilitate greater child participation and improve the intervention’s effectiveness.
Our data indicated increased head movement after the 5-minute mark of the simulation, corresponding to the virtual entry into the scanner, a known challenging moment for children. 5 Malisza et al used a stepwise approach to expose children to the MRI environment, estimating a 50% failure rate in those aged 2 to 5 years and 35% in children aged 6 to 7 years when entering the MRI scanner. 23 Despite this, children in our study exhibited less hesitation when entering the real MRI scanner and having the head coil placed, likely due to prior exposure through VR.
Our sample included children aged 3 years and 1 month to 7 years and 3 months. Participants under 4 years showed more movement during their VR session and were less engaged with the avatar, yet their MRI scan quality was still acceptable for clinical use. This suggests that while VR is beneficial for all ages, children over 4 years may benefit more, showing less overall movement and more patience during the simulation and scans. For children under 4 years, impatience rather than anxiety appeared to be the main reason for movement. Shorter scan durations or breaks may be necessary to accommodate their needs.24,25
Reducing the need for sedation offers significant time and cost benefits for hospitals and patients. Hayatghaibi et al found that sedated MRI lasted 158 to 224 minutes, whereas an awake MRI lasted 70 to 112 minutes. The most significant predictor of a longer turnaround time was the need for sedation. 26 Similarly, a study by Vanderby et al found that non-sedated scans took half the visit duration time, compared to sedated scans. 6 Including both the VR simulation (mean time = 11.4 minutes) and scanning time (mean time = 32.8 minutes), the average total time spent with participants was 44.12 minutes in our study, significantly less than the allocated time for a sedated MRI. Moreover, the VR simulation required fewer resources and staff compared to the extensive requirements for sedated MRIs.6,27 Reducing the need for anesthesia improves departmental flow times, and prevents children from receiving avoidable sedation. While the long-term effects of anesthesia remain unclear, studies indicate potential adverse effects. Flick et al concluded that multiple exposures to anesthetic drugs increased the risk of learning disabilities in children under the age of 2 years. 28 Additionally, known acute risks include respiratory distress, airway obstruction, hypotension, and other side effects to the medications used during sedation. 29 In all 18 of our participants who were initially scheduled for a sedated MRI, anesthesia was successfully avoided by adequately preparing these young children for their scan using a VR simulation, thereby avoiding unnecessary exposure to sedation. This highlights the potential for further studies to challenge current departmental protocols of sedating children once a swaddle-sleep technique is no longer applicable, and when they are under the age of 7 years. 30
Motion artifacts can significantly impact MRI image quality. Eichhorn et al found a significantly higher amount of head motion in non-sedated children compared to sedated children (mean displacement of 2.19 vs 1.12 mm). 31 In our study, most participants had minimal to acceptable motion artifacts post-VR sessions, and all scans were diagnostically usable. Some children required shorter MRI protocols (eg, a 5-minute fast head MRI) or repeat sequences (4 participants required 1-2 repeated sequences), emphasizing the need for tailored scanning protocols based on the child’s age, ability to remain still, and clinical question.
Although no significant correlation was found between movement during VR sessions and scan quality, a general trend suggested that children who displayed less movement in VR had higher quality scans. Children could have exhibited significant movement during VR simulation for a variety of reasons: boredom, difficulty with the size of the VR goggles and anxiousness. The peak head movement observed during the VR simulation for most participants occurs at the fifth minute, coinciding with the virtual entry of the child into the MRI scanner and the onset of the associated noises. After the simulation, the children may have become comfortable with the MRI scanner and noise and anticipated the experience, therefore increasing their ability to stay still. The use of MRI-compatible goggles to watch a movie during the MRI, as per departmental protocol, could also have contributed to improved stillness and distraction compared to the VR simulation.
Limitations of our study include timing of survey administration, lack of standardized anxiety questionnaires, and the small sample size. The post-surveys were completed after the MRI scans by most caregivers, therefore introducing a bias based on how they perceived their child performed in the MRI scanner. Moreover, given the unique characteristics of our study population and the aims of our research, we opted not to use a standardized questionnaire to assess anxiety. The children in our study were aged 3 to 7 years, and most standardized anxiety questionnaires are validated for older children. Furthermore, tools such as the preschool anxiety scale, a validated assessment for younger children, provide a generalized measure of anxiety symptoms in children aged 3 to 6 years. 32 Our study aimed to assess the perceived anxiety of the child toward a particular situation (MRI scan) rather than generalized anxiety. For this reason, we opted for caregivers to self-report their child’s anxiety. In future studies, we would opt for a visual analogue scale and have children rate how they feel at various timepoints during VR and their MRI, and we would invite caregivers to complete the surveys immediately after the VR intervention. Our study was limited by its sample size. Further research would benefit from including a larger cohort and an age-matched control group undergoing awake MRI without prior VR exposure. This would enable comparison of the VR interventions’ effectiveness, including whether it reduces the need for repeat sequences by improving stillness, and help assess differences in anxiety levels between the 2 groups.
Conclusions
This study demonstrates that the practice VR session was associated with a significant improvement in caregiver perceptions (P = .030) and enabled successful completion of MRI scans without the need for general anesthesia or sedation in all children initially considered to require GA. While no statistically significant reduction in anxiety was observed, the intervention resulted in diagnostic-quality imaging with minimal motion artifacts, supporting its utility as a strategy to facilitate pediatric MRI without anesthesia.
Footnotes
Acknowledgements
We highly appreciate Nicole Whitley and Fatima Kazoun for their assistance throughout this study. This study was conducted using an EmmaRye virtual reality system, which was provided at no cost for the duration of the research study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.