
Abstract
Patient-reported outcome measures (PROMs) are standardized, validated instruments that measure how patients feel and function, collected directly from the patient. Traditionally, key metrics in radiology include technical aspects such as image quality, radiation dose, and diagnostic accuracy. However, medical imaging and image-guided therapies shape patient experience in informational, emotional, physical, and logistical domains that are rarely measured. Failing to capture this information is an important gap in radiology research and practice today that needs to be addressed. This review synthesizes the science of PROMs through a radiology lens: what PROMs are; why PROMs are relevant to diagnostic imaging and interventional practice; how to select and interpret PROMs responsibly, with explicit attention to bias, conflicts of interest, and minimal important differences; and how to implement PROMs pragmatically using contemporary digital workflows. This article highlights radiology-specific frameworks for patient-centred outcomes of diagnostic tests, summarizes evidence on how electronic PROM (ePROM) programs can improve patient experience and clinical outcomes, and proposes a practical roadmap for department-level implementation. Throughout, this review aligns recommendations with current methodological and regulatory guidance, draws on Canadian implementation experience, and translates lessons from applied PROM programs in complex clinical services to radiology settings. Implemented thoughtfully, PROMs give radiologists a rigorous, low-burden way to document benefits radiology already provides, strengthen outcome and health-economic analyses, and co-design services around what patients value. Integrating PROMs alongside established technical and diagnostic metrics can extend radiology’s value proposition, and make radiology’s patient-centred impact visible, measurable, and improvable.
Introduction
Radiology has traditionally been considered as a specialty that operates behind the scenes, with varying levels of physician-patient interaction. Physician-patient interactions in radiology can depend on the radiological subspecialty, service models, and the impact of rising imaging volumes. However, the decisions radiologists make have a major impact on patients and their families. Recognizing this, many professional societies now emphasize the need to “put patients first in radiology,” a theme highlighted at a past Radiological Society of North America (RSNA) scientific meeting that called for stronger radiologist–patient communication.1,2 The rapid pace of technological innovation in medical imaging further underscores the importance of explaining complex procedures clearly and incorporating patient feedback into care. At the same time, workforce constraints can limit opportunities for direct interaction. This makes it essential to establish reliable communication pathways that keep patient perspectives at the centre of radiology practice. In this article, we highlight how patient-reported outcome measures (PROMs) can serve as a practical solution to strengthen communication and advance patient-centred radiology.
What PROMs Are (and Are Not)
Patient-reported outcome measures (PROMs) are standardized, validated instruments that capture information about health status directly from patients. 3 PROMs commonly measure information about symptoms, functional ability, and health-related quality of life. PROMs are distinct from patient-reported experience measures (PREMs), the latter assessing concepts related to the process of care (eg, communication and wait times) rather than outcomes. 4 International methodological guidance requires that PROMs be developed with patient input, and anchored in a clear conceptual framework, with demonstrated validity, reliability, responsiveness, and interpretability. 5 In addition to clinical and research use, rigorously developed PROMs are used in regulatory settings, such as for drug and device evaluation, and medical device labelling, where they must meet robust standards. 6
PROMs can be classified as either generic, or condition-specific. 7 Generic PROMs are designed to compare outcomes across various clinical conditions, and measure concepts like physical function, pain, fatigue, and quality of life. Examples of generic PROMs include the Short Form 36 (SF-36) and the World Health Organization Quality of Life measure (WHOQOL), which both measure quality of life.8,9 Condition-specific PROMs are developed for populations with specific health conditions, and are typically more sensitive to clinically meaningful change with these individuals. Examples include the Uterine Fibroid Symptom and Quality of Life questionnaire (UFS-QOL), 10 which measures symptoms after procedures to treat uterine fibroids; the Aberdeen Varicose Vein Questionnaire (AVVQ), 11 which measures key symptoms associated with varicose veins (eg, leg heaviness, pain, activity limitations); and the Chronic Venous Disease Quality of Life Questionnaire (CVIQ-20), 12 which measures physical and psychological symptoms associated with venous disease of the lower limb. Condition-specific PROMs can be useful in making decisions around who may benefit from an interventional procedure, follow-up to track key outcomes post-procedure, and in comparative treatment effectiveness studies. In some cases, there is benefit to pairing a brief, generic PROM (eg, one measuring quality of life), with a targeted, condition-specific PROM (eg, one measuring pain with chronic venous disease) to obtain both system-level comparability and detailed sensitivity to change.
PROMs matter in radiology because imaging tests and image-guided interventions impact patients in ways beyond what traditional radiologic metrics (eg, technical quality) can capture. Medical imaging impacts how patients understand their condition, how patients feel (eg, anxiety, reassurance), what patients can do in their daily life, and how they plan their day through balancing work and family responsibilities concerning visits to hospitals and healthcare facilities. The Patient-centred Outcomes of Diagnostic Tests (PROD) framework organizes the patient impact of radiology into 4 key domains: information/knowledge, physical effects, emotional effects, and burden of test. 13 Using PROMs to capture and measure these domains can provide radiologists and radiology departments a systematic, structured, reproducible, and evidence-based way to target, monitor, and improve patient impact of both diagnostic radiology pathways (eg, MRI-related anxiety, discomfort during mammography), 14 and interventional radiology care (eg, symptom relief, functional improvement). We cannot improve what we do not measure; PROMs can provide the measurement foundation required to make the patient-centred impact of radiology quantifiable, more visible, and sustainable.
Why PROMs Belong in Radiology
Diagnostic Imaging
Diagnostic imaging provides clear informational benefits to patients. Diagnoses are often clarified or excluded as a result of radiology exams. However, diagnostic imaging can also impact patients through emotional, physical, and logistical effects, which can impact the outcomes and experience of patients. Qualitative and mixed-methods research studies demonstrate that patients value clear explanations of results, empathetic preparation, physical comfort during diagnostic imaging tests, and minimal disruption to their daily life.15,16 These factors influence patient trust in physicians and adherence to their recommendations. Using PROMs that align with the PROD framework can make these outcomes visible, and therefore, improvable. 13
A case example is with MRI. The loud, enclosed scanning environment can contribute to claustrophobia and stress, particularly in young and senior populations, which can increase motion artifact, early exam termination, sometimes leading to rescheduling. 17 Trials and implementation studies demonstrate that interventions such as extending pre-scan information, structured preparation, and environmental adjustments can decrease distress and improve exam quality.18,19 In children, the utilization of virtual reality and goggles during long MRI scans reduces anxiety and the need for general anaesthesia and sedation procedures.20,21 Implementing brief PROMs before and after scanning quantifies these gains, and flags individuals who would benefit from additional support.22,23
Mammography provides another key example. Discomfort and anxiety are well-researched identified barriers for individuals to return for screening.24 -26 Capturing post-mammography PROMs can create a modality-specific quality signal that technologists and radiologists can take action on, through interventions such as: positioning coaching, comfort aids, or small workflow changes.27 -30 PROM implementation in this setting can add a patient-centred metric which can complement traditional metrics such as recall rates.
Image-Guided Procedures
Image-guided procedures, whether for diagnostic (eg, biopsy) or therapeutic purposes (eg, abscess drainage, embolization, ablation), are performed to answer important clinical questions, and improve symptoms while being as minimally invasive as possible. Successful outcomes in these cases are multidimensional. Technical success, diagnostic yield, safety, and time and resources used for the procedure are essential pieces of information. However, patient-reported pain, anxiety, recovery time, and return to usual activities also matter to patients and influence outcomes and satisfaction. 31 In these contexts, PROMs can be a helpful complement to traditional metrics. For biopsies, patient-reported studies demonstrate that simple and low-cost interventions, such as calming audio or structured relaxation, can reduce anxiety and pain during core needle procedures.32,33 PROMs can make the benefits of these interventions measurable, and help radiology teams target where additional support might be needed. For therapeutic procedures, symptom relief and functional improvement are typically the primary goals. For this reason, many high-quality randomized controlled trials use PROMs as primary endpoints, for example when comparing uterine-artery embolization with myomectomy. 34 A balanced approach that integrates technical and diagnostic metrics with targeted PROMs can provide a complete picture of procedural value and practical basis for service improvement and shared decision-making. The Society of Interventional Radiology (SIR) has also explicitly prioritized PROMs. 35 Overall, these efforts demonstrate PROMs as key to demonstrating a full picture of the value and outcomes of image-guided interventions.
Evidence From Adjacent Fields
In oncology, randomized trials demonstrate that electronic symptom reporting through PROMs, and clinician alerts during treatment reduces emergency department visits, improves quality of life, and also improves survival.36 -38 The reason for these benefits is in part thought to be related to enabling early recognition and management of adverse effects.39,40 These trials demonstrate what can be possible with PROM implementation in routine clinical practice. Brief, regular check-ins and targeted measurement can be adapted to radiological services, including interventional oncology follow-up.
Choosing the “Right” PROM: Validity, Interpretability, and Practicality
Selecting the right PROM should begin with the goal a radiology team is trying to achieve. It is important to begin by specifying whether the aim is to evaluate the experience and tolerability of a diagnostic imaging study (eg, anxiety, discomfort), to capture a change in symptoms and functional status after an image-guided therapeutic procedure, or to generate data for cost-effectiveness and comparative treatment effectiveness analyses. By beginning with clear identification of the goal, the available PROM options can be narrowed, and it can become easier to decide on the choice between a generic versus condition-specific PROM (or a combination of both). It can also become easier to decide on timing, and mode of PROM administration. Not all PROMs are created equal, and it is important to appraise the quality of a PROM intended for use, in line with the COSMIN methodology, which is a consensus-based framework for choosing PROMs by systematically appraising their measurement properties. 41 The most important criteria to ensure when selecting a PROM is demonstration of content validity, which means that the items in the PROM comprehensively and meaningfully cover what matters most to patients in your setting. 42 Next, key measurement properties that an acceptable PROM should demonstrate include: structural validity, internal consistency, test-retest reliability, measurement error, cross-cultural validity, responsiveness, and interpretability. In order to have clinically useful scoring, it is important to use pre-specified thresholds anchored in credible minimal important differences. Minimal important difference (MID) estimates the smallest change in PROM score that patients perceive as beneficial. 43 However, MID’s are calculated heterogeneously, with varied methods and credibility. 43 Radiology teams should prioritize MID’s derived from anchor-based methods with strong anchors, adequate sample size, and reproducibility. It is important to also note that MID’s are frequently related to clinical parameters, therefore the interaction among a multidisciplinary team is key for obtaining clinically meaningful MID’s. Patient Acceptable Symptom State (PASS) defines a symptom level beyond which patients consider themselves “well enough,” complementing change-based metrics with a target state. 44 This can be helpful for interventional radiology follow-up clinics. It is also important to have a plan for how missing data will be handled. For example, planning for feasibility of implementing and completing PROMs, and factors such as reading level, completion time, language translations available for PROMs, licencing constraints, and the fit with electronic workflows.45,46 When considering PROMs for research and quality improvement use, PROM selection and analysis plans should align with SPIRIT-PRO guidelines and reported according to CONSORT-PRO guidelines to ensure transparency, reproducibility, and interpretability.47,48 While the SPIRIT-PRO guidelines specify what is needed to be specified in study protocols that use PROM’s (eg, objectives, measures, timing, missing data handling, analyses), the CONSORT-PRO guidelines provide reporting standards for presenting PROM results and interpretation. In routine radiology practice, a generic PROM can be used to capture systems-level data across patient conditions, which can be used for comparative and economic analyses. A condition-specific PROM can be used to generate data which is more sensitive to change for specific patient populations. Canadian experience with standardized PROMs programs demonstrates how shared instruments and timing enable fair comparison and system-level learning. 49
Ethics, Equity, and Conflicts of Interest in PROM Selection
PROM selection has ethical and equity implications. Licencing restrictions, proprietary scoring, and vendor lock-in can shift choices toward options which are not fit-for-purpose, and exclude patients if PROMs are limited in translation, burdensome due to length, or unavailable. It is important to select a PROM which is accessible, has transparent development without conflicts of interest, and clear licencing pathways. For example, the PROMIS measures are publicly available for many clinical and research uses, and the EQ-5D can be used free of charge and is helpful for health economic analyses.50,51 Selection of PROMs should also explicitly address measurement bias by confirming the involvement of diverse patient involvement in the development, validation of measurement tools, and examining for differential item functioning across languages and cultural groups. It is also important to select a PROM with open documentation and independent validation. PROMs closely tied to a manufacturer’s commercial strategy, or where development and validation studies are performed by individuals with direct conflicts of interest (eg, collection of royalty fees, collection of pharmaceutical or medical device funding for PROM validation studies) should be avoided.52,53 At minimum, independent validation by unaffiliated investigators and transparent reporting of conflicts of interest are important before clinical adoption of PROMs. When a radiology department selects PROMs to evaluate its own services, declaring relevant interests and including patients and external stakeholders in governance can aid in reducing bias and preserving credibility.
Implementation: From Pilot to Routine Care
Workflow Integration
PROMs demonstrate the most effectiveness when they are a part of the routine clinical workflow.54 -58 Short, purposeful PROMs collected at natural checkpoints (eg, before the imaging study via a patient portal, at a check-in via a tablet or kiosk, immediately after a key milestone like post-biopsy recovery) can be helpful in reducing patient burden and improving PROM response rate. PROM scores should appear in the same systems that radiologists/technologists already use (eg, PACS/EMR), and be available in time to guide the encounter. Standardizing timing of PROMs and a standardized dataset of responses can enable comparison between sites and over time. PROM implementation can then be scaled across institutions, and has been demonstrated in other clinical areas.59,60 Standardizing PROM processes across departments and institutions would enable comparable data, pooled analyses, and smoother implementation. To achieve this, regional, national, and international multidisciplinary working groups should co-develop and validate culturally adaptable PROMs (with translation and measurement-invariance testing) so tools are reliable and meaningful across countries.
Digital Infrastructure (FHIR, SMART, and EMR’s)
Electronic PROM implementation should follow open, internationally recognized standards to ensure data remains portable across systems and that data can be sustainably collected over a longitudinal period of time. Electronic PROM implementation may also confer key implementation benefits such as improved integration into existing information technology systems, automatic scoring, and flagging for key results. 61 Health Level Seven (HL7) Fast Healthcare Interoperability Resources (FHIR) provides relevant data models and application programming interfaces (API’s): the PROM should be represented as a FHIR Questionnaire, with each completed survey as a “Questionnaire Response” and scores as an “Observation,” using appropriate codes and metadata.62,63 Electronic PROMS should be integrated to existing operational systems available in the institutions including AI platforms. For Canadian settings, individuals leading PROM implementation may also seek to review the Canadian Baseline (CA Baseline), and if applicable, Pan-Canadian Patient Summary (PS-CA) implementation Guide to ensure the PROM data aligns with national vocabulary and exchange conventions while ensuring full interoperability.64,65 SMART-on-FHIR allows for secure applications to present questionnaires in patient portals and for structured results for clinician-facing views in electronic medical records, for example flowsheets. 66 A vendor-neutral build can help protect against lock-in, simplify governance and version control, and can help facilitate interoperability and participation in registries. When considering digital deployments, instrument licencing and official materials should be used for licencing and scoring.
Governance, Privacy, and Consent
PROM data should be governed as clinical data. Clinical use requires a clear purpose statement, role-based access, secure storage and data management, and transparent communication with patients about how their information will be used. For research purposes, appropriate research ethics review and consent, with data retention and de-identification procedures should be specific in advance. In Canada, programs such as Ontario Health/Cancer Care Ontario have implemented ePROMs at scale, and also provide lessons on clinician training, clinic-flow integration, and score interpretation.67,68 These resources can be helpful for radiologists to have an overview on the impact of clear governance, privacy safeguards, and key information that is important for sustaining ePROM implementation and realizing clinical benefit.
Learning From Implementation Science
High-quality implementation studies underscore a common set of considerations. Barriers to PROM implementation include limited digital literacy, language barriers, and limited time in busy clinical workflows. Effective PROM implementation programs address these concerns through co-design with patients counting with the assistance of interdisciplinary healthcare professionals, allowing for patients to identify how they prefer to complete PROMs and when, and implementing shorter PROMs where possible.69 -71 When PROM implementation strategies are tested for local feasibility, refined iteratively, and aligned with clinical workflow, the likelihood of implementation success and relevance and usefulness of the PROM is greater.72,73
Practical Roadmap for a Radiology Department
Define the initial purpose and goals of PROM implementation: Beginning in a goal-oriented manner and with one high-value radiology pathway, with a small, explicit set of patient-centred outcomes from the PROD framework 15 is an ideal starting point. Examples of starting points include: MRI (pre-scan anxiety and comfort), CT colonography (preparation tolerability), breast imaging (discomfort and anxiety related to the testing process), or focused image-guided interventions such as uterine artery embolization or transarterial chemoembolization.74,75 Leverage transformational leadership strategies to effectively work in a team to advance on PROM implementation (Figure 1).76,77
Select the right PROMs for the intended purpose, with a transparent rationale: It is worth considering pairing a brief generic measure (eg, PROMIS short form), with a condition-specific PROM specific to the pathway of interest. Review the PROM and assess for its measurement properties in accordance to the COSMIN criteria, 78 and ensure the PROM offers translated versions, is free from conflicts of interest, and free from financial ties to for-profit corporations, which may skew and bias the performance and scoring of the PROM.
Embed the PROM into the electronic workflow: Integrate the PROM through existing patient portals, or through a tablet when patients check-in. Include the option for a post-imaging study survey when immediate feedback is important. Use guidance from FHIR 62 to ensure the data is present in clinician workflows and relevant dashboards.
Ensure PROM scores are interpretable and actionable: Pre-emptively establish thresholds that radiologists can use in real-time, utilizing anchor-based MIDs, and PASS cut-offs when available. Display scores with prompts which can indicate the intervention needed (eg, elevated pre-scan anxiety identified with a set of interventions such as scheduling the patient to use a short-bore scanner, offering headphones, and/or presenting a coaching script; or a score being flagged to indicate symptoms of bleeding after an interventional radiology procedure, along with recommended next steps for clinical decision-making, measuring anxiety scores of young children prior to undergoing an MRI scan without general anaesthesia or sedation and comparing these scores by using tools to reduce anxiety such as pre-MRI scan virtual reality training). It is important to assign clear ownership for reviewing red flags and closing the loop with patients who complete PROMs with their scores being flagged.
Institute governance, equity safeguards, and feedback: Use PROM data as if it is clinical data in terms of ensuring role-based access, and secure storage. For research purposes, ensure ethics committee oversight. Review response rates and missing data, and offer alternative language versions for PROMs where available for patients who need them. Sharing score summaries with patients when appropriate, and displaying aggregate results at regular departmental meetings can also facilitate health system performance improvements.
Evaluate and scale carefully: After determining feasibility and value of PROM implementation in one pathway, extend it to another radiology pathway creating alignment between PROM strategies across different imaging modalities, and between diagnostic and interventional pathways. Aim to maintain similar instruments for implementation pathways where possible so that data trends are interpretable and cross-site benchmarking remains valid.
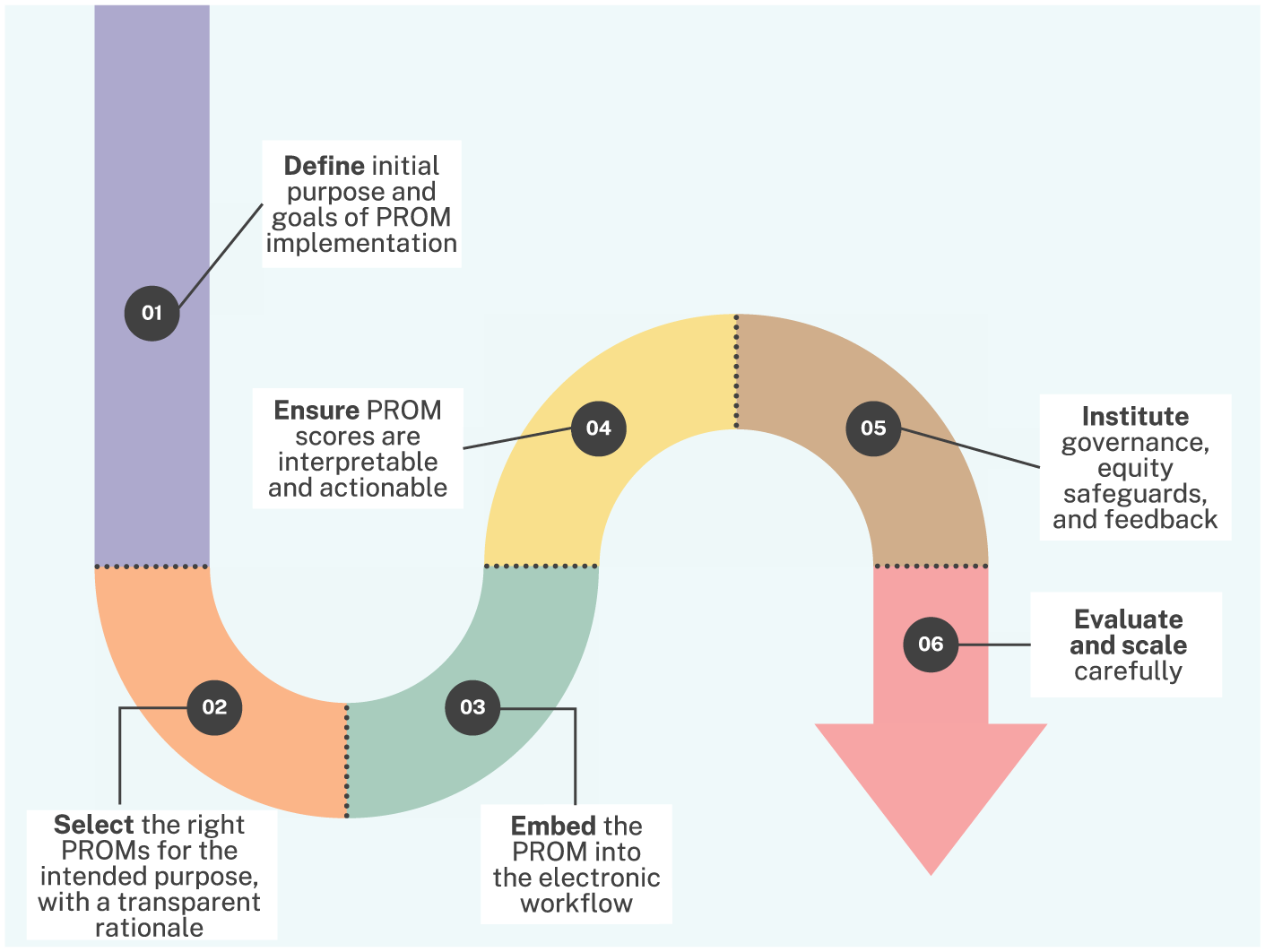
Practical roadmap for PROM implementation in radiology.
Common Concerns, and Solutions
Will this add time?: Short, ePROMs completed before an encounter with the healthcare system, or in the waiting room can have minimal impact on throughput, with several implementation studies demonstrating that ePROMs can streamline encounters by focusing efforts targeted on what patients need. Purposeful workflows that deliver brief PROMs via patient portals or digital kiosks with digital structured scores returned have been shown to be feasible and efficient in routine healthcare environments. 79
Will we be judged on factors that we cannot control?: Early PROM implementation should be used for local improvement versus external benchmarking. When comparative data analyses are sought, analyses should adjust for case-mix and social risk, and emphasize domains that radiology services can influence directly, such as preparation, comfort, communication of results, timeliness, and post-procedure care.
Isn’t diagnostic accuracy enough?: Diagnostic accuracy is an important metric in radiology. However, in today’s age, this is not sufficient for a comprehensive health measurement strategy for any clinical field. For example, two imaging studies/reports with identical accuracy can impose very different patient burdens, different emotional responses, and different downstream outcomes and healthcare utilization. For interventional procedures, two different image-guided interventions used to treat a certain health condition, however, can impose major differences in side effects to patients, aftercare, or return time to their usual activities. These concepts are best measured directly from patients through the use of PROMs, and can help identify the right imaging tests or procedures to select, the right interventions to implement, and provide quantitative data to demonstrate the direct impact radiology has on patients. 80 This data can also be used to strengthen value discussions with referrers and health system partners to advance radiology as a specialty.
Looking Forward: Building Patient-Centred Radiology Workflows
Radiology can utilize PROM-informed imaging protocols, where pre-imaging study PROMs can collect data to better triage patients to open or short-bore scanners, music or headphone interventions, enhanced communication, or anxiolysis where appropriate. By tracking completion rate, motion artifact, and patient experience, these domains can be used as joint outcomes to improve the experience, impact, and efficiency of radiology clinical workflows, and be applied as composite outcome measures in multicentric clinical trials comparing effectiveness of drugs that use imaging as an outcome measure. Second, PROM-anchored follow-up can be used for image-guided interventions, which can treat patient-reported symptoms and functions as a “vital sign,” with automated flags for critical PROM values indicating outcomes that require follow-up or intervention, with simple and pre-defined recommended actions. Third, radiologists can lead electronic PROM collaborations with clinical teams to embed imaging specific questionnaires within broader symptom-monitoring programs. Radiology can contribute to the informatics and workflow expertise to make PROM integration across clinical specialties seamless. In the long-term, the field of radiology can develop and validate imaging-specific PROM modules with professional societies working together to coordinate item banks, translations, and reference values. Progress in these fronts can accelerate when radiology departments begin collecting structured, comparable data, and share key implementation lessons.
Conclusion
The value of radiology goes beyond diagnostic clarity to what patients feel and can do after imaging studies and image guided interventions. PROMs provide a structured, systematic, and valid way to capture and measure these patient impacts, making them visible, and actionable. Radiology embodies the essentials needed to proceed based on the information in this article: clear frameworks to guide outcome measurement in radiology, examples of validated PROMs for general and condition-specific uses, reference-standard measurement and reporting guidance, and an overview of open data standards allowing for routine electronic collection. Implementation of PROMs will need to be iterative and incremental, starting with one high-value pathway in radiology, defining a set of outcomes that matter most to patients, embedding brief PROMs at natural clinical checkpoints, and closing the loop with timely, thoughtful review and action. Success in early, focused pilots can create the foundation to scale across services and departments. Implementation of PROMs in this way should allow us to quantify the direct impact of radiology on patients, helping to provide better care for patients as they move through the medical imaging department in different diagnostic and therapeutic pipelines, and strengthen radiology’s value proposition.
Footnotes
Author Contributions
RK was involved with conceptualizing the study. RK led the writing of the manuscript. RK, AD, and MP were involved with critical revision of the manuscript. All co-authors approve the submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.S.D.: Conflicts of interest unrelated to the current manuscript: Technical Advisory Board(s) of OMERACT (not for profit); Research Support of Novo Nordisk (Research Grant); Terry Fox Foundation (Research Grant); PSI Foundation (Research Grant); Society of Pediatric Radiology (Research Grant); Radiological Society of North America (Educational Grant).