
Abstract
Introduction
Breast imaging is a critical component of breast cancer screening, diagnosis, and treatment in Canada. As technology progresses, the pivotal role of medical imaging in detecting, diagnosing, and treating breast cancer evolves alongside it. As the most common cancer to affect women, breast imaging also presents numerous medico-legal challenges, and particularly in terms of the standard of care, informed consent, and potential legal liabilities. The medico-legal aspects of breast imaging can have significant implications for health care providers, patients, and their families. In this context, it is crucial to understand the medico-legal issues arising in breast imaging in Canada and the responsibilities and obligations of health care providers in this field. To our knowledge, there have been no prior studies reporting on the medico-legal landscape for breast imaging in Canada.
Errors and discrepancies in radiology practice are generally accepted to be in the range of 3%-5% of radiologists’ interpretations, with much higher rates also reported. 1,2 The literature of medico-legal aspects of breast imaging comes mainly from the USA, although European and UK reports are available. 3-7 Most often, malpractice cases include an allegation of a delay in the diagnosis of breast cancer, related to breast imaging and other reasons. In 1 large American study, imaging findings related to the breast (4.13 claims per 1000 person-years) were the most common cause of organ-related misdiagnosis subject to malpractice suits. 3
It is well recognized that screening mammography is a challenging exam to interpret with a sensitivity in the order of 80%. Breast cancers may be present but not be detectable or missed at mammography, or they may develop as interval cancers, that is, diagnosed after a normal screening mammogram and before the next screening study. It is recognized that many of these interval cancers may in fact occur because of the “masking effect” of breast tissue density, which obscures cancers. 8 In practice, this does not frequently lead to malpractice suits. More frequently, other issues such as poor positioning, errors in perception and interpretation, incorrect adherence to guidelines, and poor communication lead to malpractice issues in breast imaging. 7 While screening mammography is the most common breast imaging test, breast imaging also commonly includes diagnostic mammography, breast ultrasound, breast MRI and biopsies, with a growing contribution recently for contrast-enhanced mammography.
Understanding factors contributing to medico-legal risk for radiologists interpreting breast imaging may help identify opportunities to improve patient safety and outcomes. Breast imaging is subject to routine auditing to evaluate the performance of radiologists and medical centers to ensure excellence in the modality of mammography, in Canada and other countries. 9 Like other fields of diagnostic radiology, it is recognized that the breast imaging workforce has decreased in the USA. 10 One issue that may negatively impact the workforce and future entry into breast imaging practice is the fear of lawsuits, as shown in a survey of radiology residents in Canada and the USA. 11
This study aims to provide an overview of the key medico-legal issues of breast imaging in Canada and their implications for health care providers and the safety of patients.
Methods
Information for this work was obtained through a collaboration with the Canadian Medical Protective Association (CMPA). The CMPA is a national, not-for-profit mutual defense organization offering assistance to eligible physicians with medico-legal matters, including civil legal cases, complaints to medical regulatory authorities (Colleges) and hospitals. In 2023, the CMPA represented over 107,000 physician members. The Association maintains a medico-legal repository to conduct safe medical care research. The repository relies on physician members to voluntarily contact the CMPA and submit materials when seeking advice or support for medico-legal matters.
Medical analysts, who are experienced specially trained nurses, abstract and code medico-legal records based on CMPA procedures. Peer experts are individuals (most often physicians with similar training and experience as those named) retained in the case to review and comment on the allegations related to the patient’s care. Coding is guided by a previously published medical coding methodology, the CMPA Contributing Factor Framework 12 (CFF). Clinical information is coded using the International Statistical Classification of Diseases and Related Health Problems, 10th revision, Canada (ICD-10-CA) and the Canadian Classification of Health Interventions (CCI), as well as in-house CMPA coding. To reduce the effect of misclassification, regular coding quality assurance (QA) reviews are conducted to assure consistency.
For this study, CMPA medical analyst researchers (registered nurses with training in medico-legal research) and a statistician extracted data by searching for cases where a radiologist was named in a complaint and with an occurrence date between January 1, 2002 and December 31, 2021. Case types included civil-legal actions (class action legal cases were excluded) and both medical regulatory authority (College) and hospital complaints. Cases were then identified using CCI codes for breast imaging and breast biopsy. Trend analysis was done comparing cases involving breast imaging/biopsy to all cases where a radiologist was named.
A descriptive analysis of breast imaging cases included an analysis of the contributing factors identified by peer experts. Contributing factors were categorized as provider, team, and system factors using the CMPA’s CFF. In addition, patient age, allegations, and patient harm were analyzed. Interventions, geographical location of care and physician specialties were reviewed. Prior to analysis, all cases were de-identified and reported at the aggregate level to ensure confidentiality for patients and health care providers. The Advarra Institutional Review Board (Pro00020829) provided ethical approval for this portion of the study.
Results
Between 2002 and 2021, radiologists were named in a total of 3108 medico-legal cases. Figure 1 illustrates the trends for radiologists in case occurrence for this study period. Of the medicolegal cases involving radiologists, 188 of these cases (6%, 188/3108) were coded with a CCI code for breast imaging or breast biopsy. In this dataset, there was equal representation of male and female radiologists (IRR = 1.22; 95% CI: .89, 1.56). Comparison of trends in case occurrence, radiologists, breast imaging and biopsy, event occurrence year 2002-2021.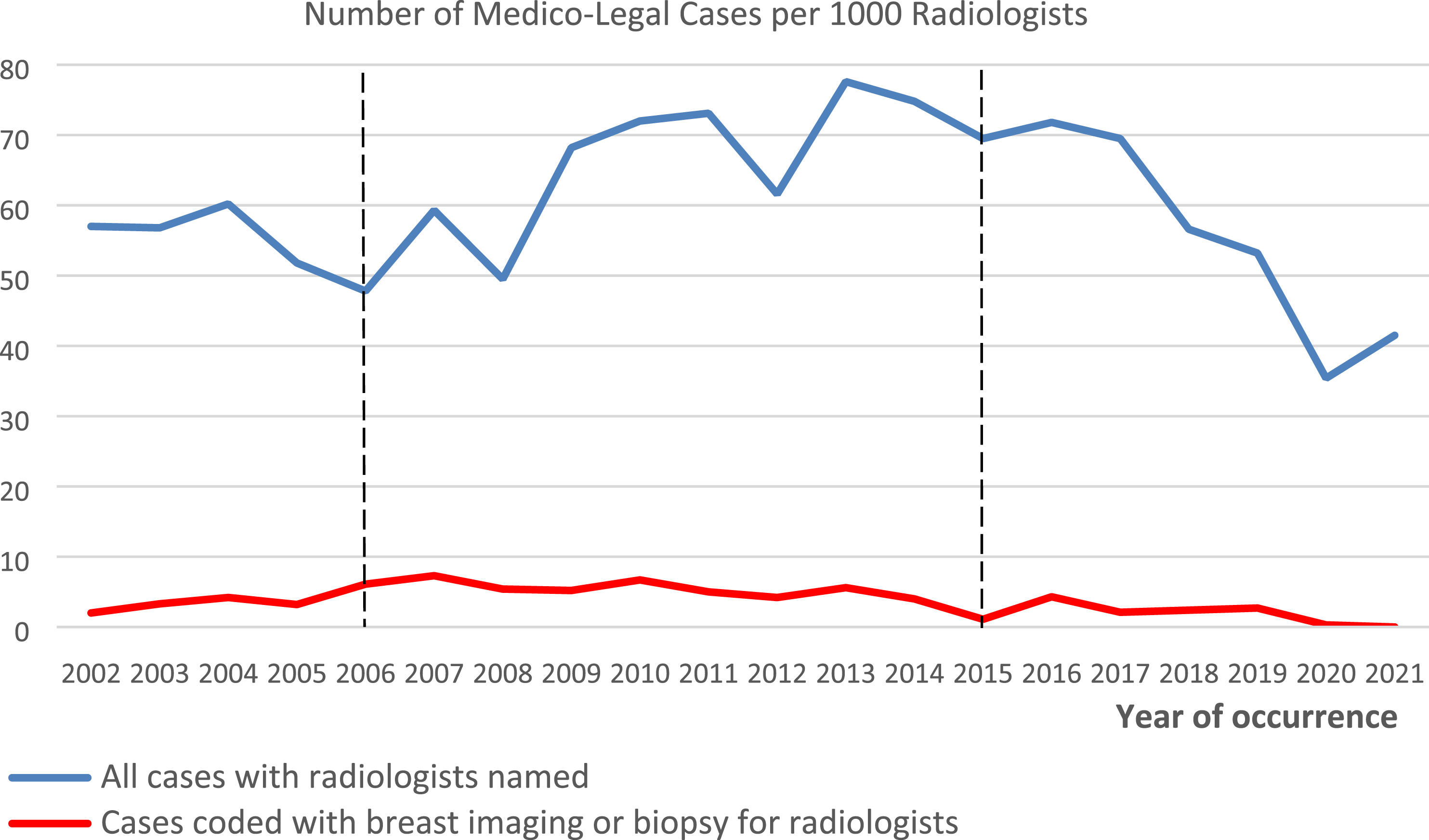
The median time lag between case occurrence and file closure at the CMPA is 4 years, with 90% of cases closed within 8 years. To account for this lag time, we adjusted the test window for statistical significance back 8 years from the data extraction date (January 5, 2023) and thus obtained a 10-year test window from 2006 to 2015 (Figure 1, dotted lines). In this time frame, analyses identified a significantly increasing trend for all cases where a radiologist was named (blue line, P-value = .0128 for a positive estimate) but a significantly decreasing trend for those cases coded with breast imaging or biopsy (red line, P-value = .0099 for a negative estimate).
Of the 188 breast imaging or biopsy cases, almost all were civil-legal actions (48.9%, 92/188) or College complaints (43.6%, 82/188) (Supplementary Appendix A). Nearly half (49.5%, 93/188) of all cases occurred in Quebec.
Patient ages ranged from 26 to 85 years. Seventy-nine percent (79%) were between 30 and 64 years of age with a median age of 57 years. There were 231 physician members named in these cases. All cases involved at least 1 radiologist and some cases named more than 1 physician or physician specialty for example: another radiologist, family practitioners, general surgeons, obstetrician gynecologists, gynecologists, and pathologists.
The overall rate of unfavourable medicolegal outcomes for Canadian physician(s) in this dataset, including civil-legal actions settled or won by the plaintiff, College and hospital cases where there were criticisms of the physician(s)] was 62% (117/188). The most common allegation in these cases was diagnostic error (81.9%, 154/188) and misinterpretation of a diagnostic test (67.0%, 126/188). A diagnostic error is defined as a misdiagnosis, a failure to make the correct diagnosis or a delay in diagnosis. Diagnostic error could occur when: a patient’s symptoms were incorrectly assessed, test results were misinterpreted or overlooked, further diagnostic testing was not done, there was a lack of follow up with the patient or miscommunication with the patient or other physicians. A misinterpretation (included in diagnostic error) refers to a failure to correctly interpret the images or recognize the abnormality potentially resulting in a missed or delayed diagnosis of breast cancer or other breast-related condition. In some cases, there was more than 1 allegation.
There were 199 radiologists involved in the 188 cases. The breakdown of the radiologists’ years of experience was 71 (36%) with greater than 30 years, 62 (31%) with 21-30 years, 31 (16%) with 11-20 years, 15 (7%) with 6-10 years, and 20 (10%) with 5 years or less experience. There was no information about the volume of breast imaging read by each radiologist or if they were fellowship-trained or not. It was of note that the risk of the radiologist being named in a case increased with years of practice. For example, in the group of radiologists with more than 20 years’ experience, 13% were named in more than 1 case and cases dated back to 2002.
Among the 188 patients, 73.4% (138/188) experienced health care related harm that were claimed to have had a negative effect on their health, psycho-emotional status, or quality of life. For 93.5% (129/138) of those patients, peer experts concluded the care fell below the standard expected in the circumstances.
Diagnostic Errors
In the CMPA data, a diagnostic error is considered a Patient Safety Indicator (PSI) which is defined as a health care event or circumstance which could have resulted or did result in harm to the patient. Note that not all cases have a patient safety indicator. Of the 132 cases that were identified with a PSI, 126 cases involved a diagnostic error. These included an incorrect diagnosis (eg, radiologist interpreted a benign lesion of the breast, eg, cysts, fibroadenoma in patients later diagnosed with malignant neoplasms), missed diagnosis or delay in diagnosis.
Criticisms or contributing factors were noted in 70% (138/188) of cases and were categorized as provider, team, and system factors. The remaining 50 cases had no criticism of the clinical care provided. Some cases had more than 1 contributing factor. In terms of provider factors, data revealed the most common clinical concern resulted from errors in radiologists’ clinical decision making which resulted not only from misinterpretation of the imaging but also resulted from a lack of (1) a thorough patient evaluation that included reviewing the patient’s clinical and family history, (2) reviewing and comparing previous images, and (3) performing a breast exam. In some cases, these deficiencies contributed to the radiologist’s incorrect decision not to investigate further or an incorrect recommendation of whether follow-up was required. A failure to perform further investigations was found in 34 cases and these included ultrasounds, mammograms (with or without magnified views), MRI/CT and breast exams.
Delays in further investigation in turn contributed to delays in the diagnosis of breast cancer and in some cases, affected the patients’ prognosis and management of care. Of the 126 diagnostic error cases, the reason imaging was ordered included: 65 for diagnostic purposes (eg, presenting with a palpable nodule), 58 for screening (eg, Provincial/Territorial Screening program or patients with a history of cancer or family history of cancer routinely being screened) and 3 for unknown reasons. Of these, there were 86 with a contributing factor of a misinterpretation. The remaining 40 cases were the result of other contributing factors.
The top 5 contributing factors for cases with diagnostic error were: • Misinterpretation of imaging (eg, benign neoplasm vs malignant neoplasm; no abnormal masses or calcifications to suggest malignancy however retrospective review noted the area of density and distortion was evident) • Failure to perform test/intervention (eg, magnified views for microcalcifications) • Inadequate documentation (eg, wording of mammogram report was vague and failed to provide clear recommendations as to the urgency of next steps) • Inadequate monitoring or follow-up (eg, lack of follow-up when pathology results did not correlate with clinical findings) • Deficient assessment (eg, failing to perform a breast exam in order to correlate clinical findings with imaging)
Provider, Team and System Factors for Cases With Peer Expert Criticism and an Event Occurrence Year 2002-2021, Radiologists, Breast Imaging and Biopsy, (n = 138 Cases).
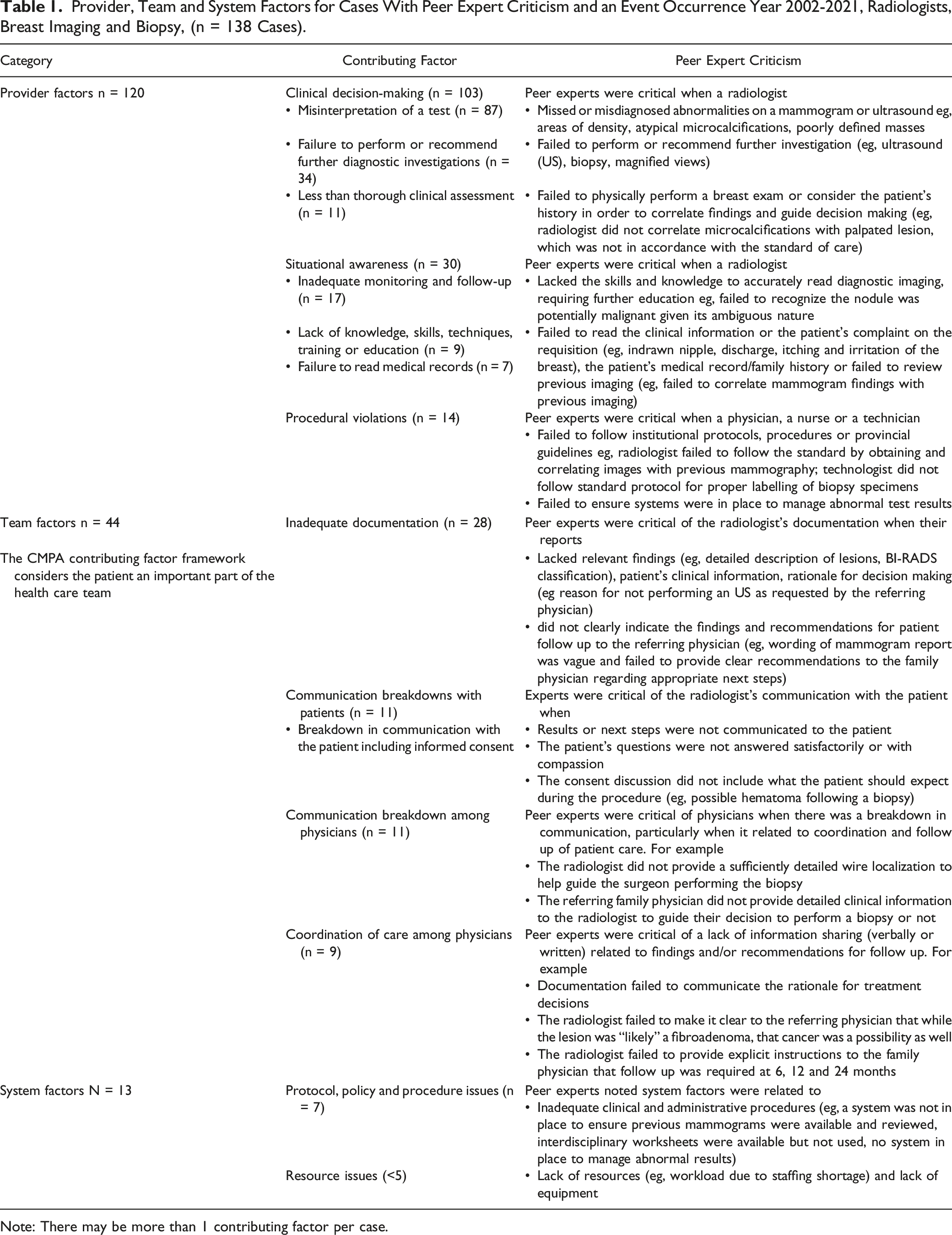
Note: There may be more than 1 contributing factor per case.
Some examples of diagnostic errors included: • A review of the patient’s previous mammograms determined the abnormality – later confirmed to be a cancer - was not visible on prior films and this was correctly reported by the radiologist. An ultrasound was indicated for work-up, but the radiologist’s report did not include this ultrasound recommendation. • In a patient with dense breast tissue at mammography, a radiologist failed to note the presence of a breast mass. Because the patient complained of palpable nodules, the radiologist should have recommended an ultrasound. • In a patient with a palpable lesion, a radiologist reported benign calcifications with no abnormality to correspond with the palpable abnormality. Expert review of the films revealed a mass with possible associated neoplastic microcalcifications. • A radiologist failed to follow the correct process by failing to correlate the mammogram and ultrasound images as well as correlate the images with clinical findings.
In this dataset, errors associated with misinterpretation of imaging included cases with mammography (n = 81) and/or ultrasound (n = 21). Some cases could have both a mammogram and an ultrasound that were misread). Some cases lacked information. Breast density subtypes are not captured. Only 8 cases had expert comments related to breast density as potentially obscuring underlying masses or creating limitations in sensitivity of the interpretation. However, in several cases, the patient was known to have dense breast tissue.
Some examples of incorrect management included: • A patient with a mass that appeared probably benign at mammogram (eg, BI-RADS 3) should have had a follow-up mammogram recommended in 6 months but was not • A radiologist diagnosed a benign fibroadenoma and recommended routine mammogram screening for a patient older than 50 years presenting with a palpable nodule. The Expert noted the mass did not have the classic appearance of either a breast cancer or a benign fibroadenoma and the standard of care required the radiologist raise the possibility of breast cancer and recommend a biopsy.
Other factors contributing to a diagnostic error on the provider’s side included a lack of situational awareness, predominantly related to inadequate patient monitoring or follow-up and insufficient physician knowledge or skill and a failure to read medical records. For example, a radiologist was required by the College to enroll in an intensive breast imaging course for missing microcalcifications which were clearly evident.
Team factors were mostly related to concerns with communication. Communication breakdowns among physicians primarily resulted from poor documentation that lacked detail and clarity by either the referring physician or by the radiologist in their report back to the referring physician. Communication breakdowns between the radiologist and patient also resulted from a lack of a thorough consent discussion, a failure to speak directly to the patient or clearly communicate follow-up recommendations. The CMPA CFF considers the patient an important part of the health care team. System factors were noted in 13 cases and were often related to inadequate clinical and administrative procedures or a lack of resources. However, this number for system factors is likely an underestimate, as until very recently the CMPA data coding focused on provider factors and captured a limited number of system factors.
Table 1 illustrates some of the peer expert comments associated with the most common contributing factors for all cases with peer expert criticism.
Discussion
From 2006-2015, there was a significant decrease in medico-legal cases involving breast imaging (P = .0099), with breast imaging cases comprising only 6% of all cases involving radiologists, a very low proportion of cases. This differs from the USA, where missed breast cancer diagnosis is the most frequently missed diagnosis. 3 This is a positive finding for radiologists practicing breast imaging in Canada, showing that the Canadian medico-legal landscape differs markedly from the USA, and radiologists practicing breast imaging in Canada are subject to a lower risk of medico-legal cases.
The rates of missed breast cancer on mammograms have been reported in the range from 10%-33%. 13,14 Of the 188 Canadian breast medico-legal cases in 10 years, the most common allegation was a diagnostic error (82%, 154/188) or a misinterpretation of a diagnostic test (67%, 126/188). The recommendations reported in 2003 by Majid et al 15 of being “alert to subtle features of breast cancers and using multiple prior studies to look for subtle increases in lesion size, looking for other lesions when 1 abnormality is seen and judging a lesion by its most malignant features” still holds true today. In our study, the most common errors occurred during interpretation. Peer experts were critical when a radiologist missed or misdiagnosed abnormalities on a mammogram or ultrasound eg areas of density, atypical microcalcifications, poorly defined masses, failed to perform or recommend further investigation (eg, ultrasound (US), biopsy, magnified views), poor documentation, failed to monitor or follow up with the patient, or failed to physically perform a breast exam to correlate with the patient’s complaint and/or consider the patient’s history, indicating that there is still room for improvement in the education of radiologists to avoid missing breast cancer diagnoses.
It is not clear what are the reasons for the lower number of lawsuits in Canada for breast imaging compared to the USA. In the USA, between 1995 and 2010, of 8265 radiologists (84.9% men and 15.1% women), male radiologists had a higher rate of being sued than female radiologists (IRR = 1.37; 95% CI: 1.20, 1.56). 16 In Canada, a larger proportion of breast radiology is thought to be done by women radiologists although data on the actual numbers of radiologists practicing breast imaging according to gender are lacking and we found no gender difference in the rates of medico-legal cases involving breast imaging. Further, in the context of universal health care coverage, the payouts in Canada may not be as necessary as in the USA where medical coverage is more variable. However, other medico-legal cases in radiology increased while breast imaging cases decreased suggesting that it was not the major reason for the low rate.
One other potential reason for the decreasing low rate of medico-legal breast imaging cases is that many breast radiologists communicate directly with patients with more “face-to-face” interactions than in other aspects of radiology. In a 2011 study of screened women in the Netherlands, 20.9% (308/1475) of screen detected cancers and 24.3% (163/670) of interval cancers were considered missed at a previous screen. Of these, only 19 women contacted the screening program radiologist about a delay or missed cancer diagnosis but did not initiate litigation, while 3 women who did not communicate with the radiologist filed a claim for financial compensation. 7 The open communication with the responsible radiologist was found probably to have prevented subsequent litigation. As an additional benefit, it has been shown that direct communication between radiologists and patients improves the quality of Imaging reports. 17 We believe direct communication with patients by breast radiologists may have contributed heavily to this improvement.
Limitations
The cases reported may not represent a complete picture of all such cases in Canada. The CMPA provides medico-legal support to physicians, and therefore cases related to an incident that did not involve a physician would not be reported to the CMPA. Results reflect only diagnostic breast imaging and biopsy issues reported to the CMPA. CMPA physician-members seek assistance for nearly all civil legal cases but do not always seek assistance for College and hospital matters. Despite rigorous quality assurance processes in place and case-by-case verification by medical analysts to assess the quality of the medical coding of cases, CMPA does not calculate and thus cannot report formal measures of inter-coder reliability, such as a Kappa statistic. The clinical information associated with these cases may be limited. Therefore, this report does not represent a comprehensive analysis of all Canadian medico-legal cases on this topic. Information on the level of radiologists’ training, volume of cases read, and the patient’s breast tissue density were not captured. In addition, medico-legal cases are influenced by recall bias, and analyses of these cases are prone to hindsight bias and outcome bias. Finally, medico-legal cases often take years to resolve so that cases that occurred in recent years are not captured in this report.
In summary, a very low number of medico-legal cases involving breast imaging was found in Canada in the past 19 years. A significant decrease in cases involving breast imaging were found from 2006-2015, accounting for 6% of the medico-legal cases. This is positive news for radiologists performing breast imaging in Canada. This study may help to encourage more radiologists to consider breast imaging, not only rewarding as a career, but with a lower medico-legal risk than was previously considered.
Supplemental Material
Medico-Legal Cases in Breast Imaging in Canada: A Trend Analysis
Supplemental Material for Medico-Legal Cases in Breast Imaging in Canada: A Trend Analysis by Jean M. Seely, Laura Payant, Cathy Zhang, Rana Aslanova, Sharon Chothia, Anna MacIntyre, Isabelle Trop, Qian Yang, Gary Garber, and Michael Patlas in Canadian Association of Radiologists Journal
Footnotes
Acknowledgments
Casey Hurrell and Courtney Green for their help in research and manuscript submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.