
Abstract
Purpose:
In pelvic MRI, Turbo Spin Echo (TSE) pulse sequences are used for T2-weighted imaging. However, its lengthy acquisition time increases the potential for artifacts. Deep learning (DL) reconstruction achieves reduced scan times without the degradation in image quality associated with other accelerated techniques. Unfortunately, a comprehensive assessment of DL-reconstruction in pelvic MRI has not been performed. The objective of this prospective study was to compare the performance of DL-TSE and conventional TSE pulse sequences in a broad spectrum of pelvic MRI indications.
Methods:
Fifty-five subjects (33 females and 22 males) were scanned at 3 T using DL-TSE and conventional TSE sequences in axial and/or oblique acquisition planes. Two radiologists independently assessed image quality in 6 categories: edge definition, vessel margin sharpness, T2 Contrast Dynamic Range, artifacts, overall image quality, and lesion features. The contrast ratio was calculated for quantitative assessment. A two-tailed sign test was used for assessment.
Results:
The 2 readers found DL-TSE to deliver equal or superior image quality than conventional TSE in most cases. There were only 3 instances out of 24 where conventional TSE was scored as providing better image quality. Readers agreed on DL-TSE superiority/inferiority/equivalence in 67% of categories in the axial plane and 75% in the oblique plane. DL-TSE also demonstrated a better contrast ratio in 75% of cases. DL-TSE reduced scan time by approximately 50%.
Conclusion:
DL-accelerated TSE sequences generally provide equal or better image quality in pelvic MRI than standard TSE with significantly reduced acquisition times.
Introduction
MRI is used widely to assess anatomy, pathology, and treatment response in pelvic diseases.1-15 A critical component of pelvic MRI exams is the acquisition of T2-weighted images.2,4,7,8,16-19 These provide high tissue contrast that enables the delineation of anatomy and pathology in a broad range of pelvic diseases.2-4,18,20,21 T2-weighted images are typically acquired with a Turbo Spin Echo (TSE) or Fast Spin Echo (FSE) pulse sequence. However, a major drawback of diagnostic-quality TSE scans is the long acquisition time. This leads to longer overall patient examination times, as well as an increased likelihood of artifacts.20,21
The long acquisition time of TSE has motivated the use of acceleration techniques such as parallel imaging (PI) and compressed sensing (CS).22-28 While these techniques decrease scan time, they can result in reduced signal-to-noise ratio (SNR) or additional artifacts.22,29 As an alternative, deep learning (DL) reconstruction has been used to achieve highly reduced scan times, but without the degradation in image quality associated with other accelerated techniques.14,16,17,24,30-32 Previously, there have been some promising studies demonstrating the potential of the DL-accelerated TSE sequence for evaluation of targeted pelvic malignancy protocols (eg, prostate and rectal cancer). However, a comprehensive comparison to standard TSE pulse sequences for broad applications across general pelvic anatomy has not been performed.14,16,17,24,30-34 Therefore, the objective of this study was to compare the performance of a DL-accelerated TSE pulse sequence to a standard TSE pulse sequence for a broad spectrum of pelvic MRI indications. Demonstration of the superiority of DL-TSE over standard TSE sequences can support replacement of the latter in wide ranging pelvic MRI applications with great potential for enhancing clinical efficiency and improved utilization of MRI resources.
Materials and Methods
Study Population
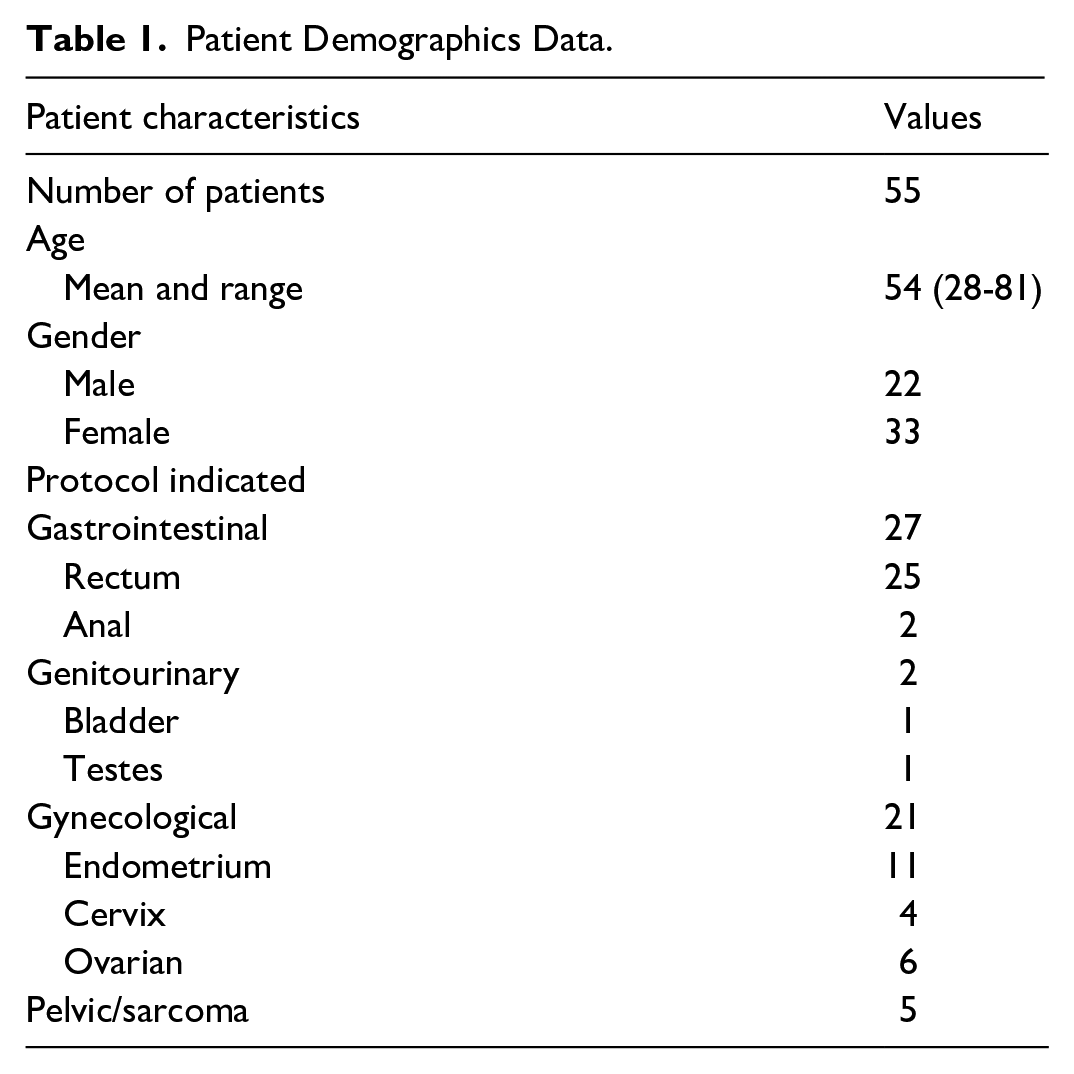
Study approval was obtained from the institutional research ethics board, and written informed consent was secured from all patients. This prospective study enrolled 55 patients undergoing pelvic MRI scans from January to September 2023. The patient cohort was comprised of 33 females and 22 males, with a mean age of 54 years (range of 21-81). Patients were referred for a pelvic MRI for clinical indications that included gastrointestinal pathology (29 patients), gynecological conditions (21 patients), pelvic sarcoma (5 patients), and a genitourinary condition (1 patient). Patients referred for prostate MRI were not included in this study, since it would have required a different TSE protocol. Table 1 summarizes the age, gender, and clinical protocol for the study cohort.
Patient Demographics Data.
Imaging Protocol
MRI exams were performed on a 3 Tesla system (MAGNETOM Verio, Siemens Healthineers, Erlangen, Germany), employing a 32-channel body coil with the compatibility of parallel imaging. All patients were scanned with both a standard 2D TSE sequence as well as an investigational DL-accelerated 2D TSE pulse sequence (Siemens Healthineers, Erlangen, Germany). Both scans were performed during the same imaging session. Depending on the clinical indication, scans were performed in either an axial plane (45 patients), an oblique plane (25 patients), or both planes (15 patients). Representative scan parameters for the standard and DL-accelerated TSE sequences are listed in Table 2. However, the exact FOV, number of slices, and scan angles deviated slightly from these values depending on the patient and clinical indication. The conventional TSE parameters reflect current clinical practice at our institution. The DL-TSE parameters were selected to assess the increased performance capabilities of the pulse sequence specifically with regards to resolution and shorter scan time versus the conventional TSE sequence.
Sample Imaging Protocol (Subject to Minor Changes Based on Variations Due to Patient Body Habitus and Clinical Indication).
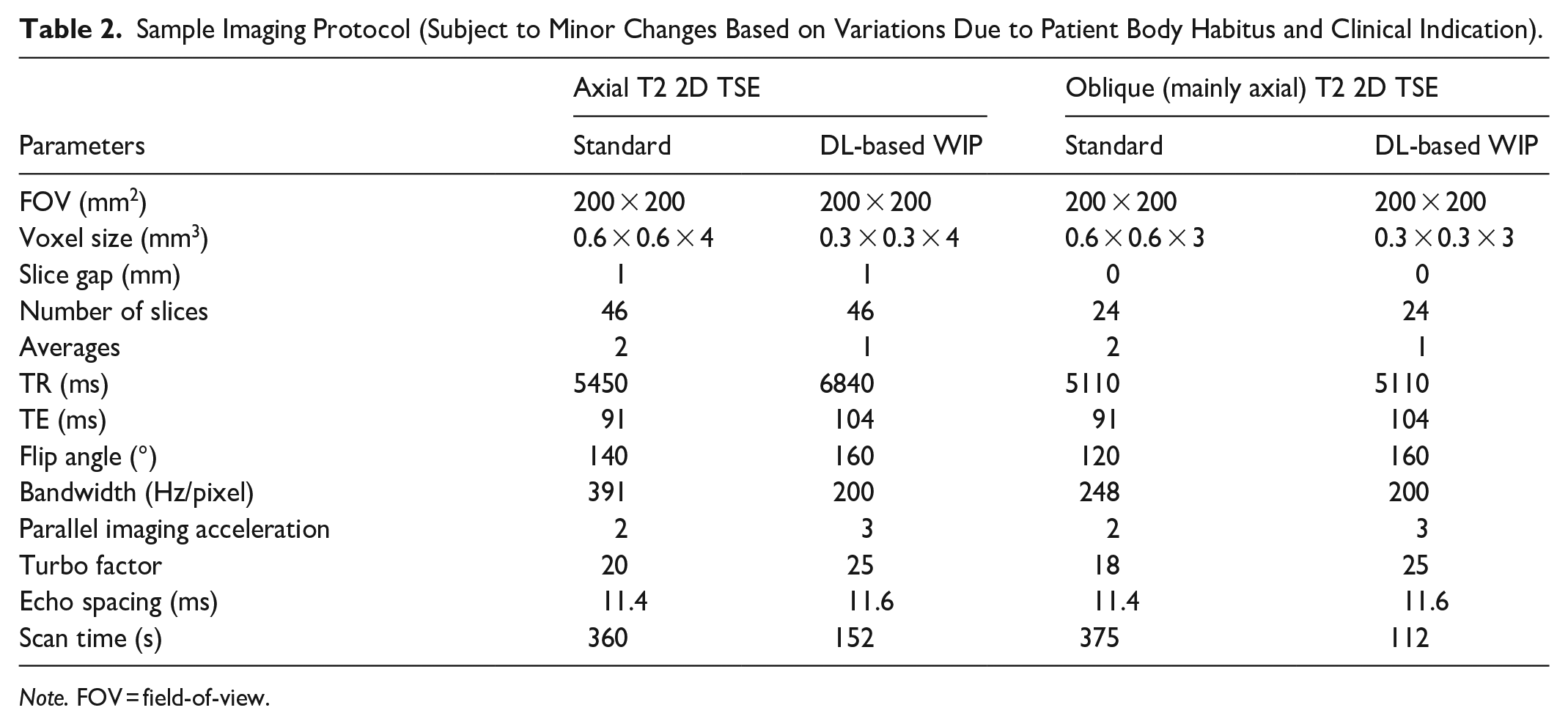
Note. FOV = field-of-view.
Deep Learning Reconstruction
The DL-based image reconstruction employs a variational neural network that receives under-sampled k-space data as well as pre-calculated coil sensitivity maps as input and generates the image through a fixed number of iterations that alternate between a parallel imaging-based data consistency and a neural network-based image enhancement. 35 The parameters of the neural networks as well as step sizes for the data consistency are considered as trainable and determined through end-to-end supervised training of the unrolled architecture. Trainings pairs were derived from fully sampled acquisitions providing target images and retrospectively under-sampled k-space data as input. About 25 000 fully sampled slices from healthy volunteers acquired on 1.5 and 3 T scanners (MAGNETOM scanners, Siemens Healthineers, Erlangen, Germany) in different body regions using a broad range of image contrasts were used as training data. Implemented in PyTorch, the model was trained on an Nvidia Tesla V100-SXM2 GPU cluster and exported for prospective use in the scanner reconstruction pipeline. The reconstruction was provided by Siemens Healthineers as a research application and has been previously evaluated for different clinical applications.30,32
Image Quality Analyses
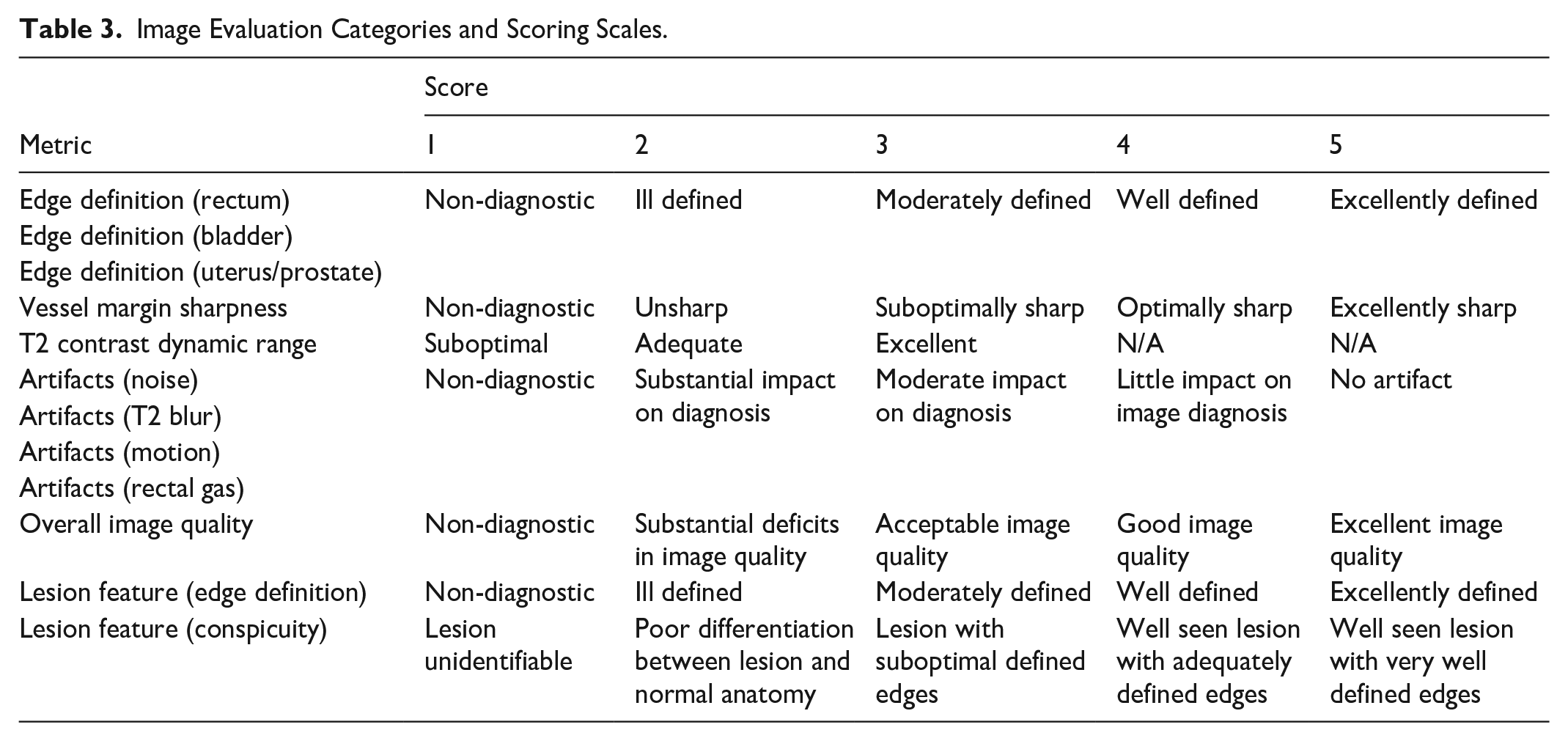
All images were anonymized and reviewed by 2 abdominal radiologists (with 2 and 24 years of MRI experience) using the institutional PACS system (Coral PACS, Version: 2.5.0.0). Both radiologists were blinded to all sequence information, and pulse sequence order was randomized for presentation to the radiologists. Each radiologist independently scored image quality on a 5-point scale in the following categories (including subcategories), except for the T2 Contrast Dynamic Range, which used a 3-point scale:
(1) Edge definition (rectum, bladder, prostate/uterus)
(2) Vessel margin sharpness
(3) T2 Contrast Dynamic Range (T2CDR)
(4) Artifacts (noise, T2 blur, motion, rectal gas)
(5) Overall image quality
(6) Lesion features (edge definition and conspicuity)
The definitions of the above categories are self-explanatory, except for T2CDR. This was defined as the ability of the sequence to provide qualitative (visual) contrast differences in T2 signal intensity between pelvic soft tissue structural elements, such as that of smooth muscle (eg, bowel wall, uterus, etc.) against pelvic fat, skeletal muscle, and or fluid signal intensity. High T2 contrast differences between these pelvic structures are critical for characterization of pelvic pathology as well as cancer detection and staging. Since this variable involved an overall visual qualitative assessment by the readers, a 3-point scale was deemed adequate for comparison of the 2 TSE sequences.
Including subcategories, there were a total of 12 different scores for each patient. Table 3 lists the scoring scales used for each of these 12 categories. As an additional quantitative measure of image quality, the contrast ratio (CR) was assessed for each pulse sequence. This was defined as the difference in signal between ischiorectal fat pads and the gluteus medius muscle, divided by the signal in the ischiorectal fat pads:

Image Evaluation Categories and Scoring Scales.
Signal was calculated as the mean value over a circular region-of-interest (ROI) in each of the regions. Measurements were taken on both left and right sides.
Acquisition Time
The acquisition times for the DL-TSE and standard TSE sequences in axial and oblique planes (when performed) were recorded in all patients for direct examination time comparisons.
Statistical Analyses
The null hypothesis tested in this study was:
H0: There is no difference in image quality (ie, categories listed in Table 3) or CR (equation (1)) between DL- and conventional-TSE pulse sequences
This hypothesis was tested with a two-tailed Sign Test using Matlab (MathWorks, R2013b). Statistical significance was set at the 95% confidence level. All tests were performed separately for axial and oblique orientations. For the image quality tests, a Bonferroni correction was applied to account for the multiple test categories under investigation. For each image quality category (Table 3), scoring was performed separately for each of the 2 readers. Reader agreement was defined as the fraction of image quality categories where both readers agreed on the superiority, inferiority, or equivalence of DL-TSE compared to conventional TSE.
Results
Image Results
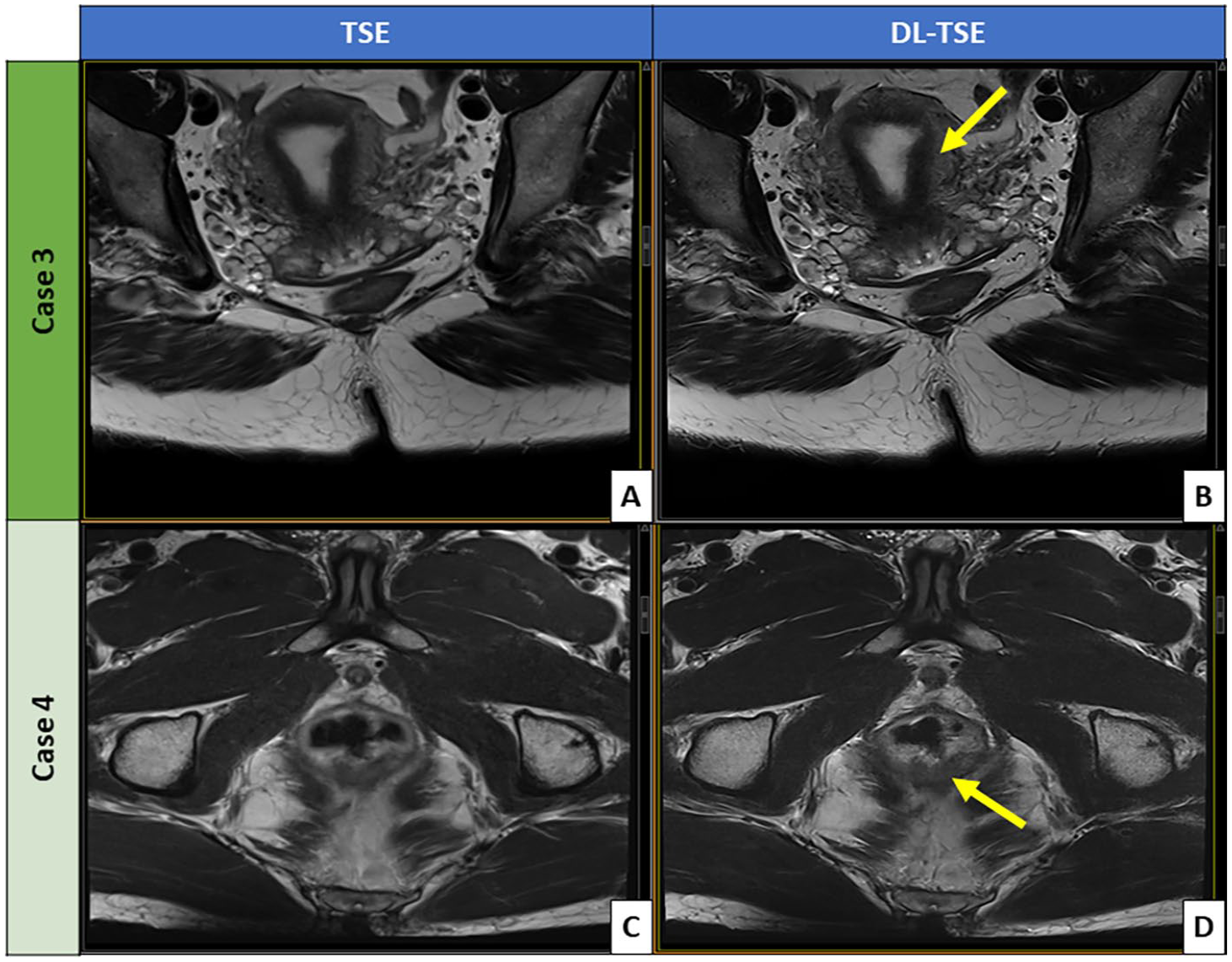
Figures 1 and 2 illustrate some example DL- and conventional TSE images. Figure 1 shows the comparison of axial T2-weighted images acquired with the standard-TSE against the DL-TSE. Overall, the axial DL-TSE renders sharper anatomical edge definition than the axial standard-TSE without introducing artifacts. Lesion-wise, the axial DL-TSE provides sharper delineation of the uterine mass than the axial standard-TSE, although both sequences were deemed diagnostic (Figure 1A and B). In another patient, Figure 1C and D, the axial DL-TSE shows significantly reduced motion artifacts and superior delineation of the low rectal cancer within its posterior wall. Figure 2 compares the oblique T2-weighted images between the standard-TSE and DL-TSE. Like Figure 1, more definitive tissue delineations are observed generally for the oblique DL-TSE compared to the oblique standard-TSE – for example of the uterine junctional zone (Figure 2A and B). As shown in another patient in Figure 2C and D, the oblique DL-TSE provides clearly superior diagnostic details of a rectal tumor than the oblique standard-TSE, with significantly reduced motion blur and precise rectal tumor delineation. This is especially critical for optimal rectal cancer staging and management.
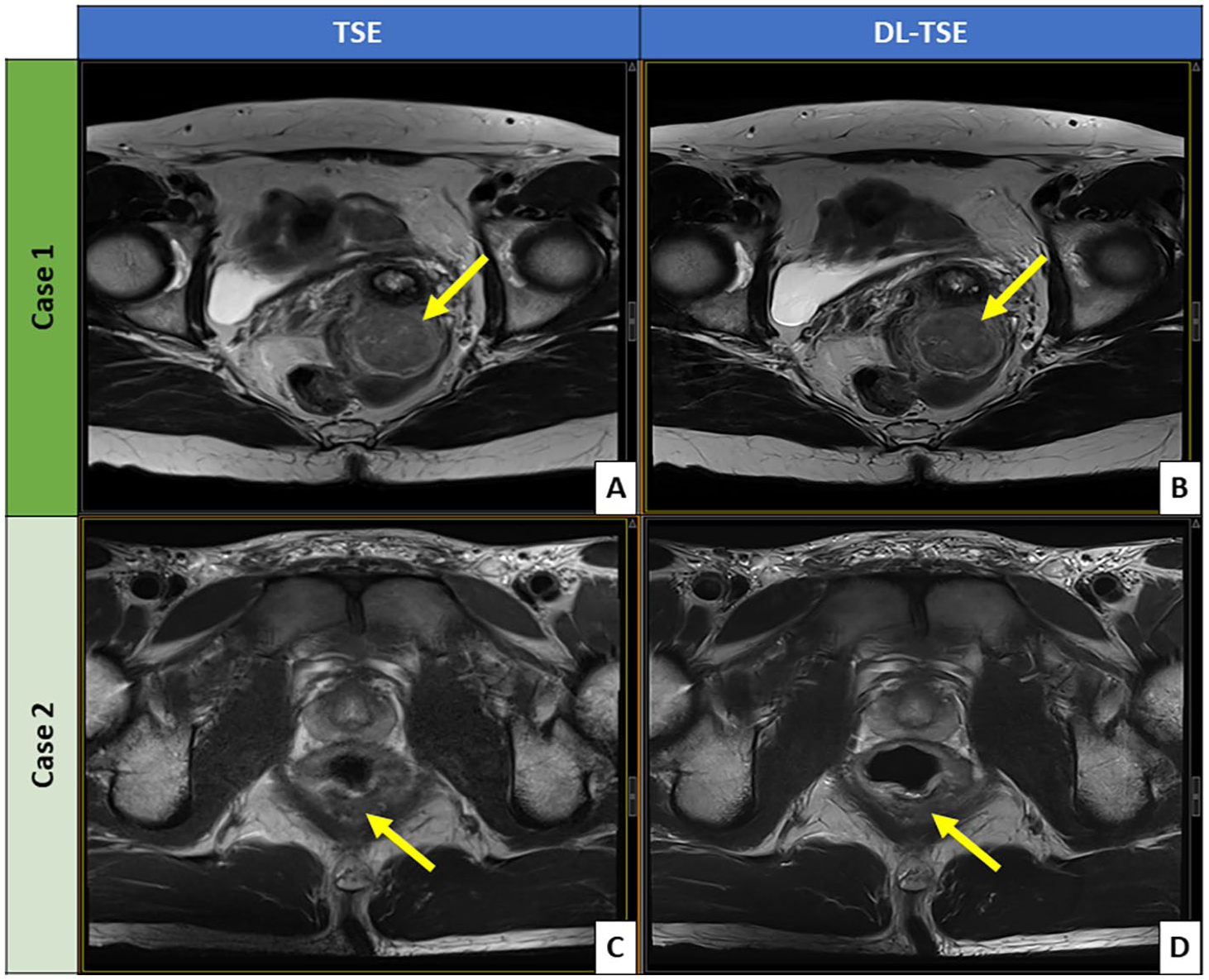
Comparison of axial T2-weighted images acquired with standard TSE versus DL-TSE. The images include: (A) standard TSE and (B) DL-TSE of a patient being evaluated for a uterine mass (indicated by the arrows), and (C) standard TSE and (D) DL-T-TSE of a patient with rectal cancer (indicated by the arrows).
Comparison of oblique T2-weighted images acquired with standard TSE versus DL-TSE. The images include: (A) standard TSE and (B) DL-TSE demonstrating comparative delineation of uterine junctional zone and zonal anatomy (indicated by the arrow), and (C) standard TSE and (D) DL-TSE in a patient with rectal cancer (indicated by the arrow).
Qualitative Evaluation
Tables 4 and 5 list the results for the image quality comparison in axial and oblique scan planes respectively. Overall, in 10 out of 12 categories in the axial plane, and 11 out of 12 categories in the oblique orientation, both readers independently found DL-TSE to provide image quality with either no significant difference or better image quality than conventional TSE. Going into more detail for the individual categories, both readers found significantly better image quality for DL-TSE in 6 out of 12 categories in both scan planes: edge definition (rectum, bladder, and uterus/prostate), vessel margin sharpness, overall image quality, and edge definition), while neither reader found a significant difference in T2CDR and rectal gas artifacts in either of the scan planes. For the remaining 4 categories: artifacts (noise, T2 blur, motion) and lesion conspicuity, there was disagreement between the readers in one or both orientations. There were 2 cases within these latter categories (T2 blur and motion artifacts in the axial orientation) where reader #2 found conventional TSE was better than DL-TSE. However, reader #1 disagreed and found the obverse. There was one case (noise in the oblique orientation) where reader #1 found conventional TSE to be better than DL-TSE, while reader #2 found no difference. Overall, the 2 readers agreed on superiority/inferiority/equivalence of DL-TSE compared to conventional TSE in 8/12 (=67%) of the categories in the axial plane, and 9/12 (=75%) of the categories in the oblique plane.
Image Quality Results of the Two-Tailed Sign Test for the Standard TSE Sequence and the DL-TSE Sequence in the Axial Orientation.
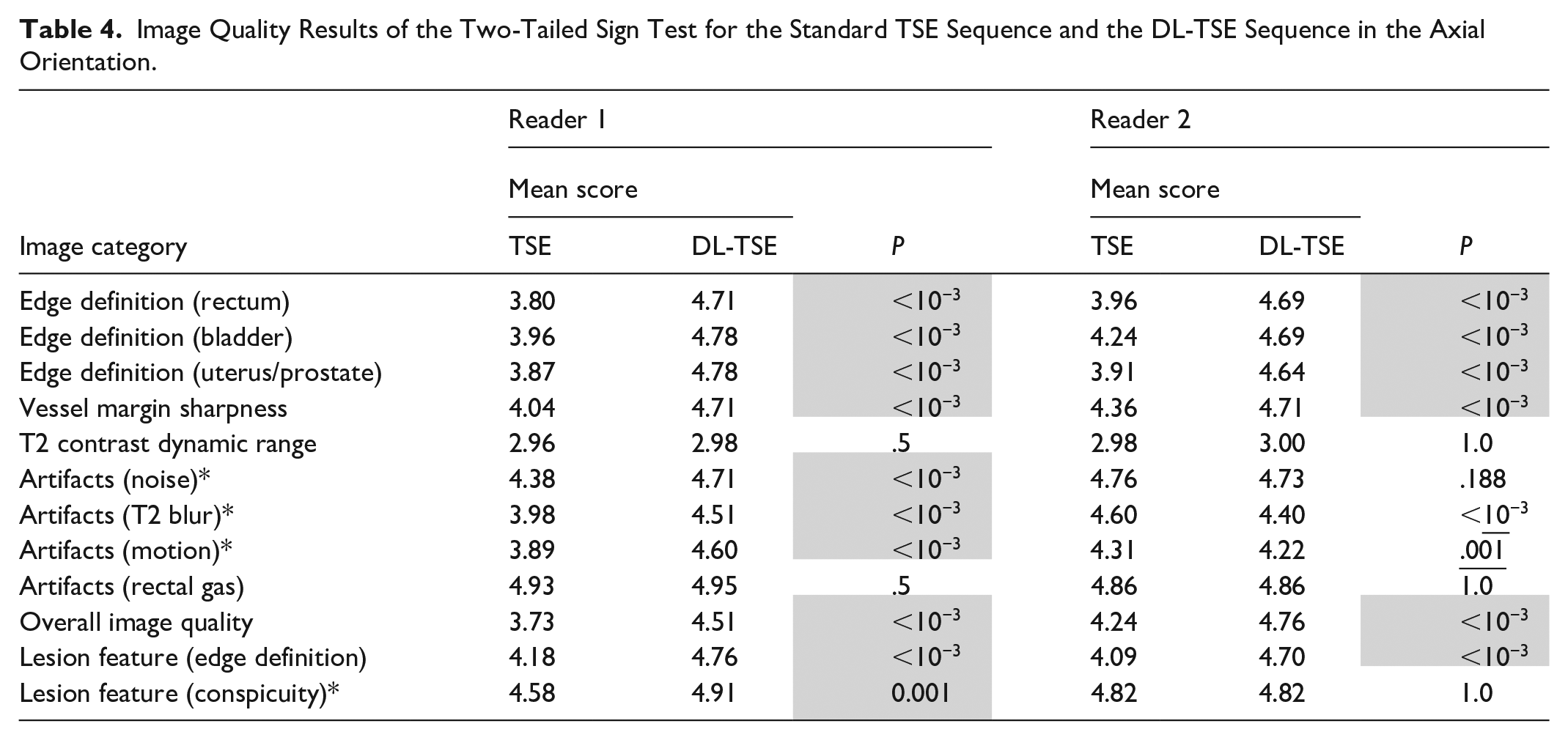
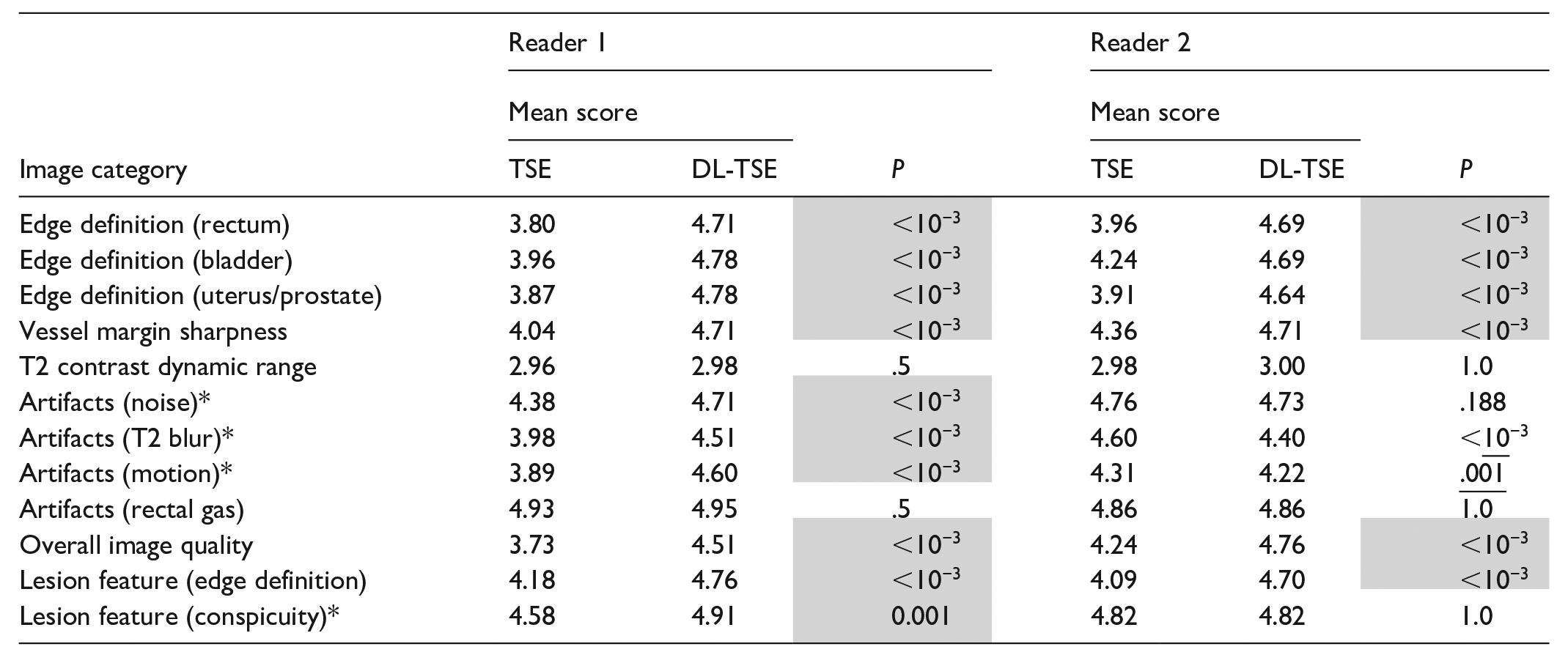
Image Quality Results of the Two-Tailed Sign Test for the Standard TSE Sequence and the DL-TSE Sequence in the Oblique Orientation.
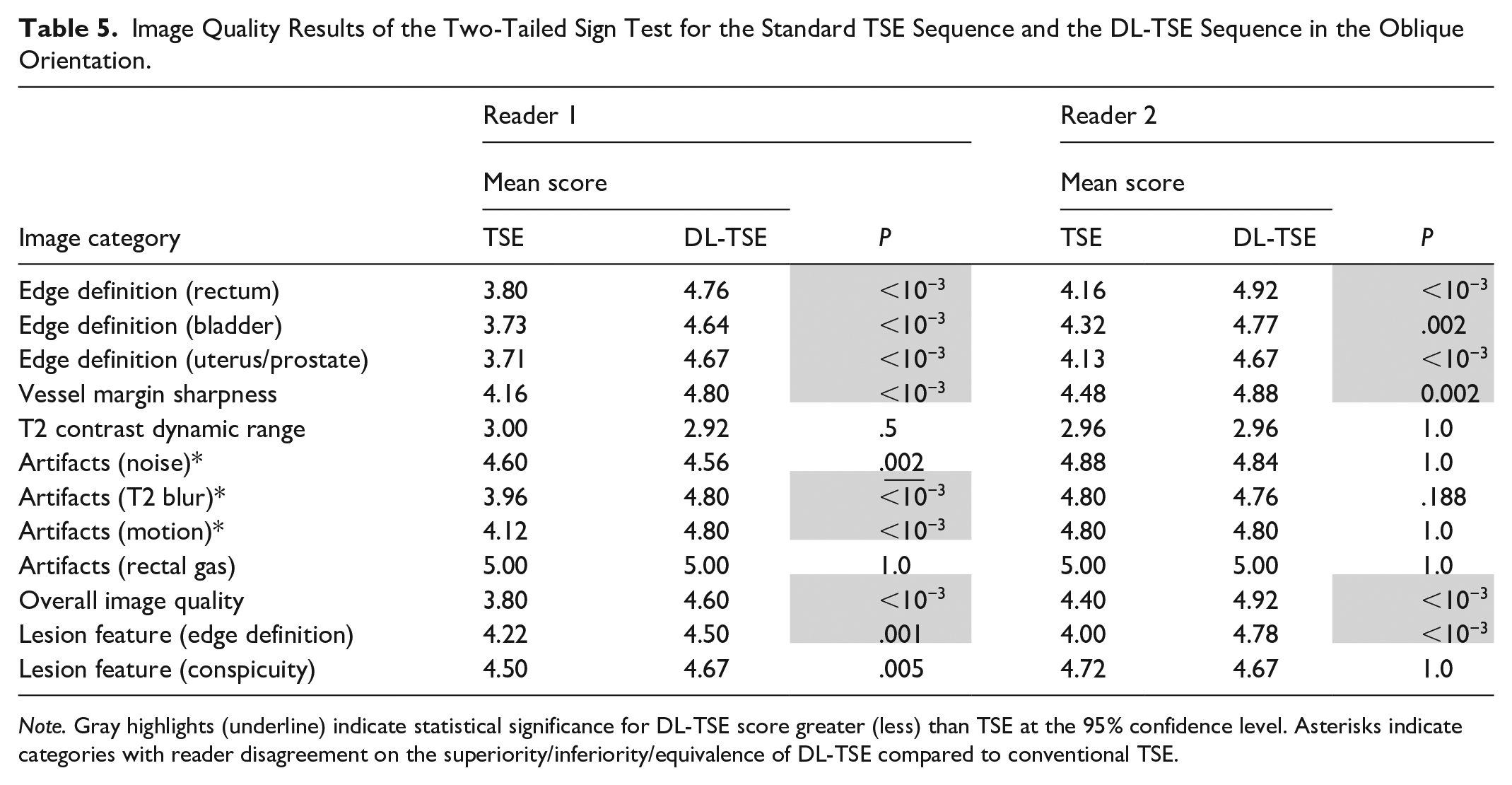
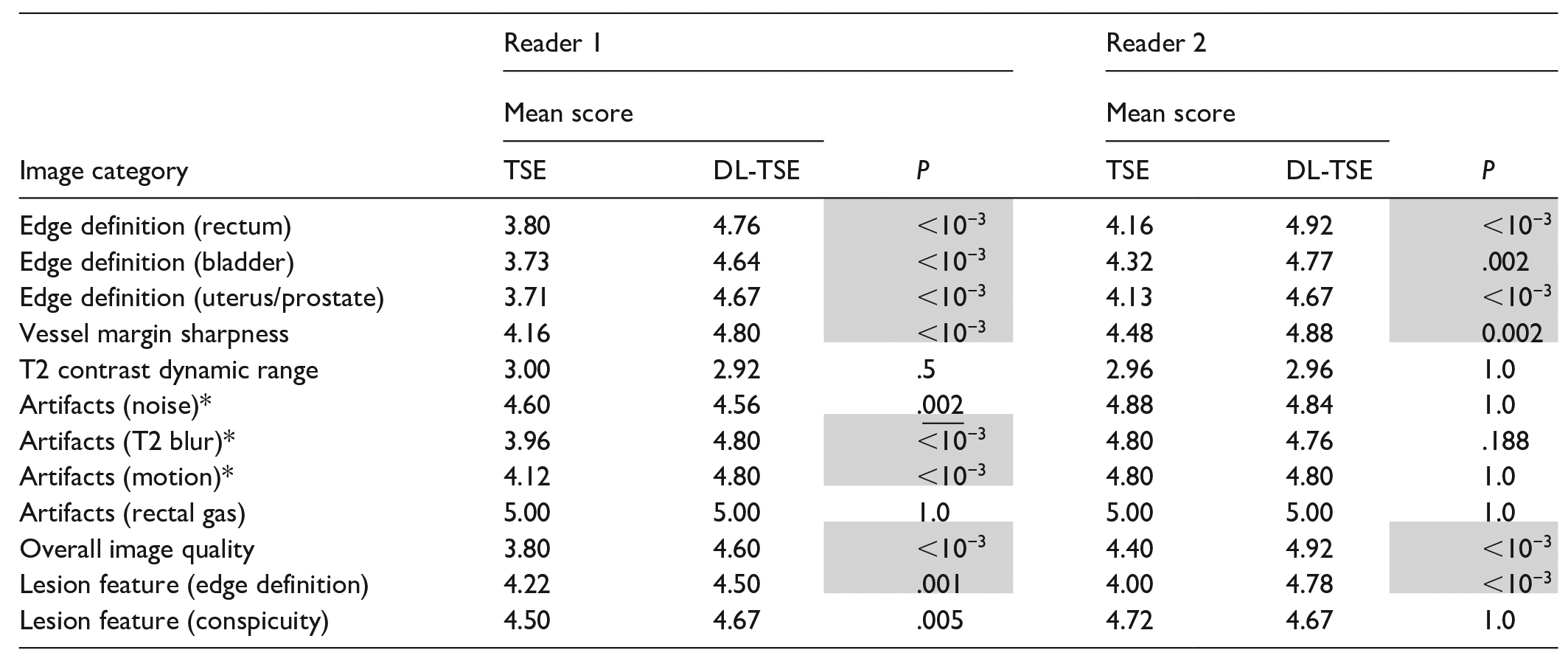
Note. Gray highlights (underline) indicate statistical significance for DL-TSE score greater (less) than TSE at the 95% confidence level. Asterisks indicate categories with reader disagreement on the superiority/inferiority/equivalence of DL-TSE compared to conventional TSE.
Quantitative Evaluation
Table 6 summarize the CR analyses. The DL-TSE CR is significantly higher than conventional TSE in all cases except for the left sided oblique CR. In the latter case, conventional TSE CR was higher. Although all results were statistically significant, the differences in CR only amounted to a few percent in absolute terms.
Contrast Ratio (CR) Results of the Two-Tailed Sign Rank Test for the Standard TSE Sequence and the DL-Based TSE Sequence.
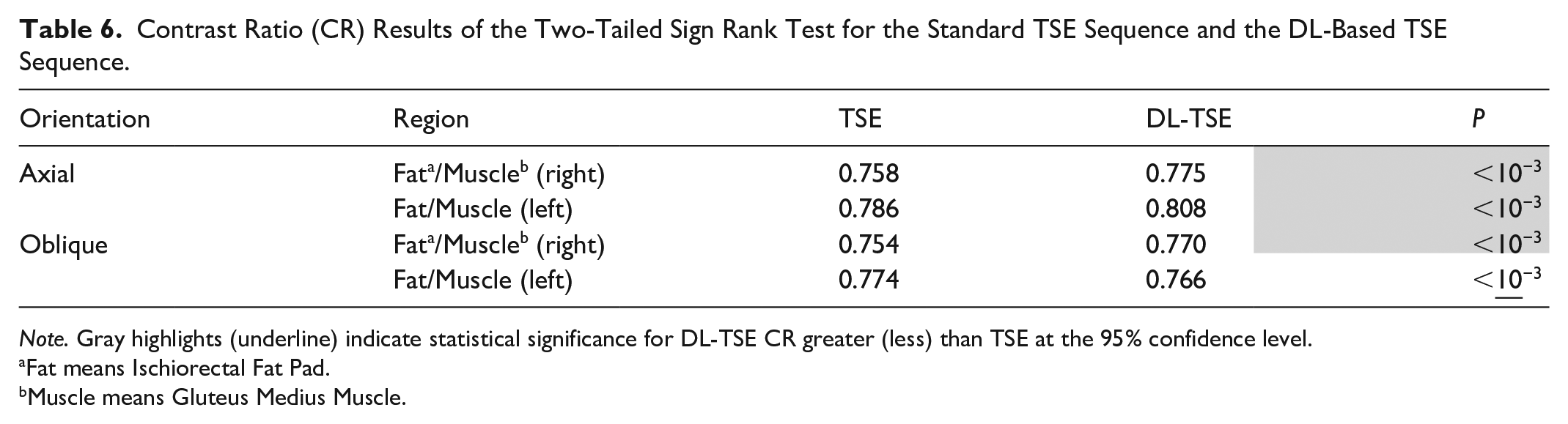

Note. Gray highlights (underline) indicate statistical significance for DL-TSE CR greater (less) than TSE at the 95% confidence level.
Fat means Ischiorectal Fat Pad.
Muscle means Gluteus Medius Muscle.
Acceleration Improvement
DLR-accelerated sequences enabled a significant reduction in scan acquisition times. On average, the axial DL-TSE accelerated the scan to 152.0 ± 10.4 seconds from 360.0 ± 17.7 seconds rendered by the axial standard-TSE. Similarly, the oblique DL-TSE achieved a scan time reduction to 112.0 ± 0.9, compared to 375.0 ± 22.5 seconds of the oblique standard-TSE.
Discussion
This prospective study compared a DL-accelerated T2 2D TSE sequence to a standard T2 2D TSE sequence in the context of pelvic MRI. In 10 out of 12 categories in the axial plane, and 11 out of 12 categories in the oblique orientation, DL-TSE provided image quality with either no significant difference or improved image quality compared to conventional TSE. In half of the image quality assessment categories, both readers scored the DL-TSE sequence as significantly better than the conventional TSE sequence. In 2 of the categories, T2CDR and rectal gas artifacts, both readers did not detect any significant difference in image quality. In the case of T2CDR, no significant difference is expected, since it should depend primarily on the TE value, rather than the reconstruction technique. Based on the reader scores, rectal gas artifacts were absent in this patient data set for both pulse sequences. For the remaining categories (artifacts and conspicuity), there was a discrepancy between the 2 readers on the superiority/inferiority/equivalence of DL-TSE compared to conventional TSE. Discrepancies also arose between axial and oblique orientations in these categories. A potential explanation for the observed discordance could be that these categories represent more subtle aspects of image quality and or differences in readers’ experience. On the other hand, given that DL-TSE has approximately half the scan time compared to the conventional TSE, it was somewhat surprising that DL-TSE was not clearly superior to conventional TSE in the motion artifact category. This may be due to the source of the motion artifacts. Artifacts arising from motion that occurs sporadically (eg, gross patient movement) are expected to be reduced with the use of a shorter scan time; those arising from rhythmic physiological motion (eg, peristalsis or breathing) would likely remain (unless scan times were much shorter – on the order of a few seconds). Unfortunately, the nature of the motion artifacts was not captured in the scoring system used in this study (Table 3).
The quantitative results of this study indicated that the CR of DL-TSE was superior to those of conventional TSE images in 3 out of 4 cases and worse in one. However, although statistically significant, the difference in CR values was relatively small (a few percent) in all cases. This small difference is likely an additional reason why neither reader noted a significant difference in the T2 contrast dynamic range image quality category. It is important to emphasize that the equivalent or better image quality provided by DL-TSE was obtained in about half the scan time of conventional TSE. Thus, it can be concluded that DL-TSE provides a viable clinical alternative to TSE for routine pelvic MRI examinations.
There are several recent studies which are in accordance with the present results –specifically, that DL-accelerated sequences provide equal or better image quality to their standard equivalents.16,17,30-34 It should be emphasized, though, that most previous studies focused on a narrow range of pelvic anatomy – primarily the prostate or female pelvis. The present study more generally included all consenting patients scheduled for non-prostatic pelvic MRI. Additionally, this study evaluated a broader range of image quality categories than these previous studies. For example, none of the previously mentioned studies has explicitly evaluated motion artifacts, T2CDR, or rectal gas artifacts.
Limitations
One limitation of this study was the number of patients. This study included consenting patients for any type of non-prostate pelvic MRI exam. Therefore, although the total study enrollment was 55, the numbers of patients scanned for any one specific clinical indication was lower (Table 1). As a result, no sub-analysis of the results by clinical indication was performed. Related to this limitation, some anatomy is not well represented in our patient group (eg, anus, bladder, and testes). However, since we were non-selective in patient recruitment, the mix of indications is representative of our clinical practice. Also note that since this study was designed as an assessment of image quality only, there was no direct assessment of diagnostic performance.
A second limitation was the modest reader agreement (~70%) on the superiority/inferiority/equivalence of DL-TSE compared to conventional TSE. For example, in some cases, one reader would score DL-TSE as significantly better than conventional TSE, while the other reader would find no significant difference. However, despite discordant reader agreement in ~30% of the cases, there were only 3 instances out of 24 (=12 categories × 2 readers) where either reader scored the conventional TSE superior to DL-TSE. Even in these cases, the other reader did not agree with the result. In all the rest of the cases, DL-TSE was scored equal to or better than conventional TSE. A related limitation is that only 2 readers were used to assess image quality in this study. Additional reader(s) may have helped resolve some of the cases of reader disagreement. However, due to the relatively few cases where conventional TSE was scored better than DL-TSE by either reviewer, it is unlikely that additional reviewers would have changed the overall conclusions of this study.
One factor that potentially confounded the comparison between conventional and DL-TSE was the fact that the scan parameters were not exactly the same (see Table 2). In particular, note that the DL-TSE sequence had a finer resolution and shorter scan time. Indeed, these parameter differences may well have been the reason for some of the better image quality scores achieved by DL-TSE in Tables 4 and 5. The reason that identical parameters were not used was because this wouldn’t have provided a realistic clinical assessment of the improved capabilities offered by the DL-TSE pulse sequence – the entire motivation for using this sequence in the first place. Conversely, improving the resolution of the conventional TSE sequence to match that of DL-TSE would have resulted in clinically unsuitable long scan times. Therefore, the parameters chosen for this study represent a fair assessment of each pulse sequence as it would be implemented clinically.
Finally, although both the DL-accelerated and standard TSE sequences provided convincing depictions of pelvis pathology, the correlation between the image results and pathological results, were outside the scope of this study.
Conclusions
This study demonstrated that DL-TSE overall provides equivalent or improved image quality than conventional TSE for most pelvic MRI examinations. Moreover, it achieves this in approximately half the acquisition time, while providing better CR in most cases. This could be used to enhance clinical efficiency, optimize imaging resource allocation in pelvic MRI, enhancing patient experience while maintaining or improving image quality. DL-TSE is therefore a viable option for replacement of conventional TSE in pelvic MRI.
Footnotes
Acknowledgements
The authors would like to thank Dr. Gerald Moran, Research Collaborations Manager at Siemens Healthcare Limited, Oakville, ON, Canada.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Lumeng Cui and Dominik Nickel report financial support was provided by Siemens Healthineers AG. Other authors report no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Lumeng Cui and Dominik Nickel are employees of Siemens.