
Abstract
Introduction
Medical imaging is a dynamic specialty. Its ever-evolving nature can make it challenging for medical professionals to determine which imaging test offers the greatest clinical value for their patients. This challenge is reflected in the fact that up to a quarter of medical imaging studies are considered low value or fail to meet appropriateness criteria.1,2 Not ordering the most clinically valuable test first can lead to patient harm, including unnecessary exposure to ionizing radiation and contrast material, needless inconvenience, discomfort or anxiety, and the identification of incidental findings that may trigger a cascade of unwarranted tests and interventions.1,3 Furthermore, it also overburdens a healthcare workforce already struggling with short staffing and burnout, strains an overstretched healthcare system, drives up healthcare spending, and harms the environment.1,3 There is an urgent need to optimize the use of limited medical imaging resources. To improve the appropriateness of imaging use, developing and maintaining up-to-date, evidence-based diagnostic referral guidelines is essential.2,4
As the voice of medical imaging in Canada, the Canadian Association of Radiologists (CAR) recently updated a series of 13 diagnostic imaging referral guidelines. 5 The guideline on the musculoskeletal (MSK) system 6 is ready for knowledge translation activities. This guideline supports the development of new Choosing Wisely Canada (CWC) recommendations. Launched in 2014, CWC is a physician-led initiative designed to foster conversations between doctors and patients about unnecessary tests, treatments, and procedures. 3 CWC collaborates with professional clinical societies to develop recommendations aimed at reducing healthcare overuse. 7 The campaign aims to prevent potential harm to patients, preserve healthcare resources, and reduce environmental impact by eliminating practices that add no clinical value to patient care. The objective of our project is to create new CWC recommendations for the imaging of the MSK system based on the latest CAR MSK referral guideline.
Methods
The study received ethics approval from the McGill University Institutional Review Board.
A Steering Committee of clinical MSK experts was formed to guide the development of recommendations aimed at reducing unnecessary imaging in Canada. Relevant professional associations—including the Canadian Academy of Sport and Exercise Medicine, Canadian Association of Emergency Physicians, Canadian Association of Radiologists, Canadian Orthopaedic Association, Canadian Rheumatology Association, and The College of Family Physicians of Canada—were invited to participate and to recommend a delegate from their organization for committee membership. Physicians affiliated with these associations frequently manage patients with musculoskeletal conditions and could be impacted by these recommendations. Members from various provinces and members from community practices as well as from urban academic centres were selected.
The Committee held an initial full-group meeting during which the process for selecting clinical scenarios and drafting recommendations from the CAR MSK System Diagnostic Imaging Referral Guideline 6 was agreed upon by consensus. The process of development of the recommendations is illustrated in Figure 1.
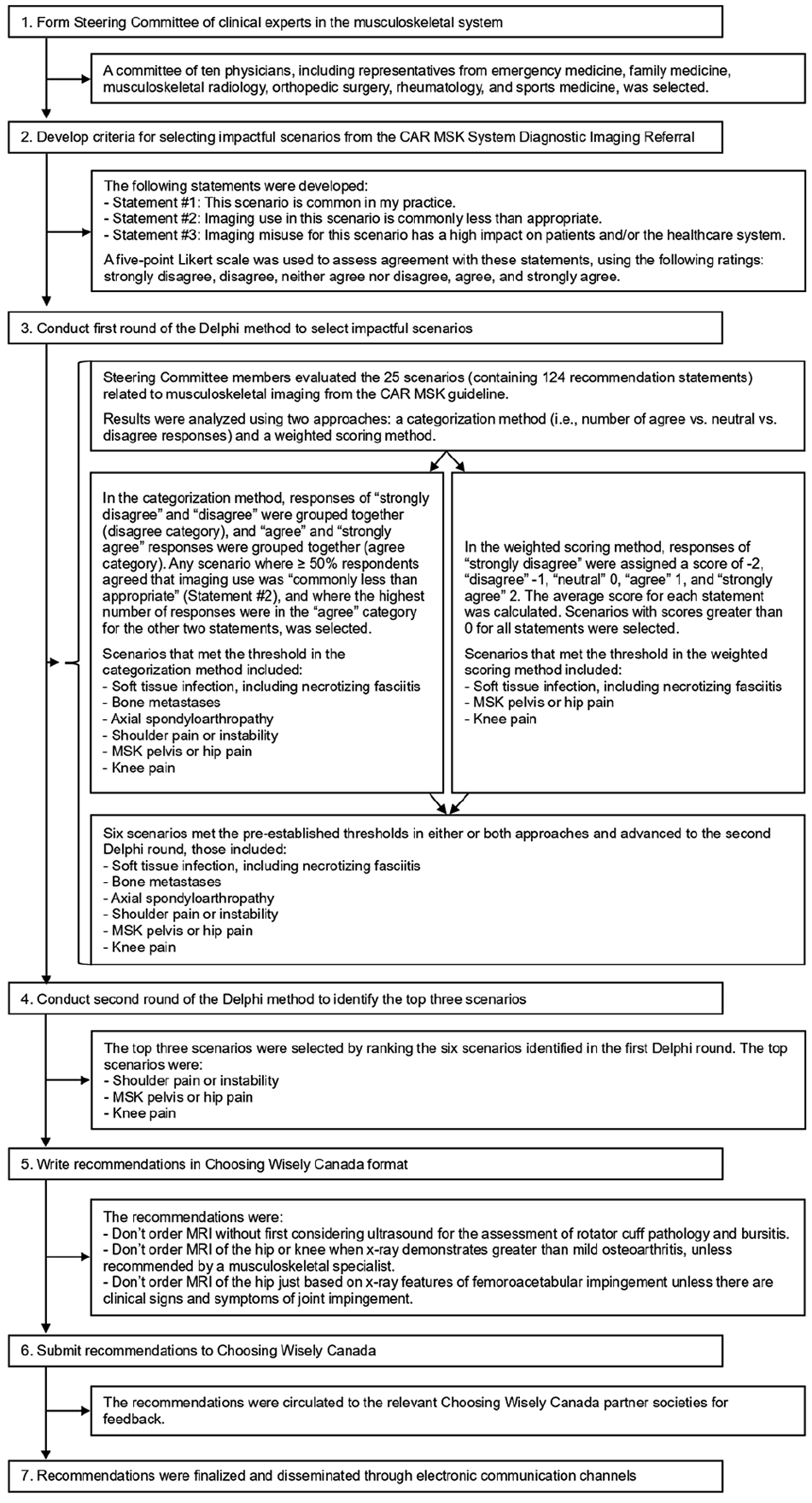
Flow diagram illustrating the process of development Choosing Wisely Canada recommendations for musculoskeletal imaging, informed by the 2024 Canadian Association of Radiologists (CAR) Musculoskeletal (MSK) System Diagnostic Imaging Referral Guideline.
For the first round of the Delphi method study, a survey was sent to Committee members listing all 25 clinical diagnostic scenarios, including 124 recommendation statements from the referral guideline, 6 with instructions to evaluate their level of agreement across 3 statements:
Statement #1: This scenario is common in my practice.
Statement #2: Imaging use in this scenario is commonly less than appropriate.
Statement #3: Imaging misuse for this scenario has a high impact on patients and/or the healthcare system.
In the latter statement, “high impact” refers to substantial consequences, such as patient inconvenience, discomfort or complications, and/or increased costs to the healthcare system.
A 5-point Likert rating scale was used, with the following options: strongly disagree, disagree, neither agree nor disagree, agree, and strongly agree. An additional option of “not applicable” was provided for scenarios that were outside the scope of a committee member’s specialty practice.
Two approaches were then used to analyze the data: a categorization method and a weighted scoring method:
The categorization method grouped responses of “strongly disagree” and “disagree” together (disagree category), and “agree” and “strongly agree” responses together (agree category). Any scenario where ≥50% respondents agreed that imaging use was “commonly less than appropriate” (Statement #2), and where the highest number of responses were in the “agree” category for the other 2 statements, was selected. The rationale for prioritizing Statement #2 over Statements #1 and #3 is that the purpose of CWC is to reduce unnecessary tests in Canada.
In the weighted scoring method, responses of “strongly disagree” were assigned a score of −2, “disagree” −1, “neutral” 0, “agree” 1, and “strongly agree” 2. The average score for each statement was calculated. Scenarios with scores greater than 0 for all statements were selected.
Scenarios that met the threshold in either or both approaches advanced to the second round of the Delphi study.
In the second Delphi round, Committee members were asked to rank the scenarios retained from Round 1 according to their perceived impact on addressing overuse and their relevance to the CWC campaign. The top 3 scenarios ranked as most relevant were selected.
Choosing Wisely recommendations were drafted by the Committee Co-Chairs (NG, KR) during a virtual meeting, using the methodology outlined in the CWC Medical Professional Society Handbook, 7 ensuring that each statement began with “Don’t.” We opted to focus on imaging modalities, without providing protocol details. Feedback on the recommendations was then sought from all the Committee members. Once consensus was reached, the recommendations were circulated to CWC, who sent them to their list of societies for feedback (as per their process) and were subsequently finalized and distributed through electronic communication channels.
Results
The Steering Committee consisted of 10 experts, including an emergency physician, one family physician, 3 musculoskeletal radiologists, one orthopaedic surgeon, one rheumatologist, and 3 primary care sports medicine physicians. Members represented various provinces and territories—British Columbia (1), Ontario (6), Quebec (1), Saskatchewan (1), and Yukon (1)—and came from both academic (8) and community (2) practice settings.
Attendance was 100% at the initial consensus meeting and response rate was 100% for both rounds of the Delphi study.
Following the first round of the Delphi study (results presented in Supplemental Material 1 and 2), the following 6 clinical scenarios were retained:
Scenario 3: Soft Tissue Infection, including Necrotizing Fasciitis
Scenario 5: Bone Tumour—Metastases
Scenario 11: Spondyloarthropathy (Axial)
Scenario 16: Shoulder Pain or Instability
Scenario 19: MSK Pelvis or Hip Pain
Scenario 20: Knee Pain
All these scenarios met the threshold in the categorization method, while 3 (Scenarios 3, 19, and 20) also met the threshold in the weighted scoring method.
Following the second round of the Delphi study (results presented in Supplemental Material 3), the following 3 scenarios were retained:
Scenario #16: Shoulder Pain or Instability
Scenario #19: MSK Pelvis or Hip Pain
Scenario #20: Knee Pain
The final recommendations were:
Recommendation #1: Don’t order MRI without first considering ultrasound for the assessment of rotator cuff pathology and bursitis.
Recommendation #2: Don’t order MRI of the hip or knee when x-ray demonstrates greater than mild osteoarthritis, unless recommended by a musculoskeletal specialist.
Recommendation #3: Don’t order MRI of the hip just based on x-ray features of femoroacetabular impingement unless there are clinical signs and symptoms of joint impingement.
Explanations and references for the final recommendations are presented in Supplemental Material 4.
Discussion
This article documents the process of developing CWC recommendations based on the CAR MSK referral guideline. 6 It provides a framework for developing future CWC recommendations for the remaining 12 CAR referral guidelines. 5 As expected, the MSK imaging referral scenarios identified through multidisciplinary consensus as priorities for reducing overuse include commonly imaged large joints (shoulder, hip, knee) and prevalent conditions such as rotator cuff pathology, shoulder bursitis, femoroacetabular impingement, and osteoarthritis. 8 The literature suggests a high frequency of inappropriate MRI use for the hip, knee, and shoulder, with reported rates ranging from 15% to 56%.9-11 Some of these rates are based on studies conducted in other countries and may not reflect patterns of MRI use in Canada. A common instance of inappropriate MRI use is in the setting of moderate or greater osteoarthritis.9,11 MRI is generally unwarranted at these stages of degenerative arthropathy because it does not alter patient management. 12 Nevertheless, Choosing Wisely campaign recommendations are intended to provide guidance for appropriate utilization, not rigid rules. It is recognized that each patient’s situation is unique, and there may be critical signs or symptoms for which MRI may still be indicated, even in the setting of advanced OA on radiographs.
An additional example of MRI misuse is in the evaluation of femoroacetabular impingement. MRI of the hip should not be ordered based solely on radiographic findings of femoroacetabular impingement morphology without clinical features of the syndrome, as these anatomical findings may represent asymptomatic variants.13,14 Even when impingement symptoms are present, history and physical examination, along with radiographic imaging—sometimes supplemented by diagnostic injection—are often sufficient for diagnosing femoroacetabular impingement syndrome. 15 Advanced imaging with MRI may be unnecessary and is best reserved for complex diagnostic cases or preoperative planning.14,15
Another imaging practice that deviates from published appropriateness criteria is the frequent ordering of shoulder MRI without preceding radiographs and instead of ultrasound.8,16 For evaluating soft tissues such as the rotator cuff, MRI and ultrasound have comparable effectiveness, with MRI rarely providing additional management-relevant information beyond ultrasound, which is also less expensive. MRI is more useful than ultrasound for intra-articular concerns. However, a review of shoulder MRI examinations at a Veterans Affairs tertiary care hospital suggested that ultrasound could have effectively replaced MRI in 66% of cases. 16 Therefore, a combination of radiographs and ultrasound should be considered before ordering a shoulder MRI. In some parts of Canada where musculoskeletal ultrasound expertise is not readily available—for example, in certain rural areas—MRI may be used as an alternative.
Over the past decades, medical imaging has revolutionized medicine by enabling earlier and more precise diagnoses, as well as minimally invasive therapies that improve patient outcomes. 1 It has enhanced disease management and contributed to better population health through screening. Due to its considerable impact, imaging has become an essential tool in many areas of healthcare. When the appropriate imaging test is used at the right time, it adds substantial value to patient care. 17 It is not surprising, therefore, that the use of medical imaging has increased significantly. For example, in musculoskeletal imaging in the U.S., MRI usage rates rose by 615%, CT by 758%, and ultrasound by 500% between 1994 and 2013. 18 The rising demand for imaging has been partly attributed to expanding evidence-based clinical indications, a growing elderly population, and an increasing burden of chronic conditions like cancer. 1 However, with the increased use of imaging, there is also a growing concern about overutilization. 1 Overutilization refers to the use of tests and treatments that provide little to no benefit to patients, or those with a risk of harm that outweighs the potential gain, thereby failing to improve overall patient outcomes.17,19
Overutilization exposes patients to potential harm, wastes limited human and material healthcare resources, and unnecessarily increases the environmental footprint of medical imaging.1,3,19,20 In a healthcare system already struggling with resource constraints—such as limited and aging medical imaging equipment and staffing shortages that reduce radiology service hours—growing demand exceeds capacity.1,21 This leads to excessive wait times for imaging and bottlenecks in healthcare delivery.11,17 The inability to obtain timely imaging delays diagnosis and treatment, potentially resulting in poorer health outcomes. 17 When limited resources are allocated to low-value imaging, access to high-value studies—and ultimately, patient care—is compromised. It is, therefore, imperative to use imaging wisely. As CAR advocates, we must ensure that patients receive the right test at the right time. 21 A shift toward value-based radiology is urgently needed to maintain quality, safety, efficiency, and sustainability in imaging services.19,22
Addressing overutilization requires understanding its causes and identifying the most effective solutions. There are many factors driving the overuse of medical imaging, including patient expectations, physician education and experience, regional practice patterns, a culture of defensive medicine driven by medico-legal concerns, financial incentives such as self-referral, and the duplication of imaging studies.4,23 Primary care physicians, who serve as gatekeepers of the Canadian healthcare system and stewards of its limited resources, also face the challenge of managing a wide range of clinical presentations. 4
Transforming deeply entrenched healthcare practices is challenging. Passive dissemination of guidelines to raise public awareness may be insufficient to drive sustained practice change in reducing low-value care. 24 To address the various factors contributing to overuse, interventions that are active, engage multiple stakeholders, and consist of multiple components are typically the most effective.24,25 There has been debate about whether the Choosing Wisely campaign has successfully influenced physician practices, as extensive healthcare overuse persists a decade after its launch and system-level change remains limited. 26 Some critiques of the campaign include that creating and publishing lists of recommendations on low-value care is insufficient to significantly reduce such care, particularly considering strong financial incentives, high concerns about malpractice, and patient preferences. Furthermore, Choosing Wisely leaves it to specialty societies to determine which healthcare practices are included in their recommendations, without a standardized methodological approach, which may lead to inconsistencies and call into question the strength of the scientific evidence supporting these selections. Measuring the impact of the Choosing Wisely campaign is difficult, especially since most datasets lack sufficient relevant data to assess meaningful outcomes.19,26 Nevertheless, the literature suggests that initiatives driven by CWC have contributed to reductions in overuse. 27 For example, a quality improvement initiative based on the CWC campaign’s recommendation for head injuries led to a 13.9% decrease in CT rates at 3 months, with a sustained reduction of 8% at 16 months. 28 Strategies that involve organizational change to implement Choosing Wisely recommendations have shown particularly high success rates. 24 Given that the Choosing Wisely initiative is relatively recent, and like many public health campaigns that require years to demonstrate broad impact, these small grassroots quality improvement projects, with sustained effort and investment, have the potential to contribute to system-wide change over time.
A strategy that has shown promise in reducing imaging overutilization is the use of clinical decision-support (CDS) tools.25,29 For example, one study reported a 23.4% reduction in MRI use for low back pain following the implementation of a CDS-based intervention. 30 Overall, the evidence on the effectiveness of CDS for appropriate medical imaging remains mixed, with limited high-quality studies. 29 CDS tools can be particularly helpful for providing primary care physicians with immediate access to the latest evidence-based clinical practice guidelines, embedded into their workflow, across the full range of possible presentations encountered at the point of care. 4 These tools must, nevertheless, be designed in a way that does not overstep physician autonomy or restrict access in a manner that hinders clinicians from adequately addressing individual patient circumstances. 19 The referral guidelines created by the CAR 5 are being integrated into CDS systems 31 to improve adherence and enhance the appropriateness of imaging investigations. This initiative aims to help guide referring physicians in determining what imaging referral is likely to impact patient management and to ensure the most appropriate modality is selected as the first choice.
Additional approaches to improving appropriate healthcare resource utilization include fostering a culture that promotes value-based care, aided by system-level enablers. Integrating resource stewardship and cost-effective care into the medical school curriculum can help develop a philosophy of high-value healthcare practice in the next generation of physicians. 32 If supervising attending physicians embrace these concepts as part of their role in modelling behaviour, it can further strengthen this cultural shift. 32 Furthermore, individualized feedback reports that allow ordering physicians to assess their adherence to guidelines can encourage continuous improvement in value-based care and serve as reinforcement. 25 Ultimately, stimulating intrinsic motivation through the innate human desire to feel competent and effective, along with a sense of professional accomplishment, positive peer recognition, and a well-regarded reputation, may encourage behavioural change and maintain it over time. 33 On the part of radiologists, careful screening of imaging orders—including rectification or rejection of those that appear unindicated—along with enhanced communication with referrers through readily available consultations, can help reduce low-value examinations.1,2,34 Patient education—whether provided by radiology departments or referring physicians—is also important, as patient attitudes considerably influence medical imaging utilization. 34 Finally, system-wide changes are required to support value-based radiology, including a centralized imaging ordering system and easy access to imaging records across the province or even the country.2,33
This study has several limitations. First, the selection of scenarios and development of recommendations were based on expert consensus, which, while rigorous, is inherently subjective and shaped by the personal perspectives of the participants. The Steering Committee was comprised of a relatively small number of experts, which may limit the diversity of perspectives. Although the Steering Committee was multidisciplinary and geographically diverse, it may not fully represent all practice settings in Canada, potentially limiting generalizability. Additionally, the Delphi method, which relies on self-reported assessments of imaging use, is based on personal knowledge and experience and may not accurately reflect true national imaging utilization patterns. However, the selected recommendations address areas of frequent overuse reported in the literature. Lastly, the statistical analysis focused on basic evaluation using categorization and weighted scoring methods. While advanced techniques for assessing consensus strength could have been applied, the chosen methods were deemed appropriate for the study’s scope and data.
In conclusion, this study outlines the process of developing new CWC recommendations for MSK imaging, grounded in the latest CAR referral guideline. It provides a roadmap for the development of additional CWC imaging recommendations derived from the other 12 updated CAR referral guidelines. Through a structured, consensus-driven approach, 3 key recommendations were identified to reduce unnecessary MRI use for rotator cuff pathology, shoulder bursitis, femoroacetabular impingement, and osteoarthritis. These recommendations align with existing literature on imaging overuse and aim to improve imaging appropriateness in musculoskeletal care. This project strengthens the relationship between CWC and CAR and contributes solution-oriented approaches to the current healthcare crisis. The next steps will involve implementation strategies to enhance the integration of these recommendations into clinical practice. Measuring the impact of these initiatives will then guide our efforts toward value-based radiology. For example, these new CWC recommendations could be integrated into the CDS tools increasingly used in Canada, with rates of appropriate imaging utilization monitored to evaluate the success of this initiative.
Supplemental Material
sj-docx-1-caj-10.1177_08465371251339389 – Supplemental material for Optimizing Musculoskeletal Imaging Referrals: Making Wise Choices a Knee-Jerk Reaction
Supplemental material, sj-docx-1-caj-10.1177_08465371251339389 for Optimizing Musculoskeletal Imaging Referrals: Making Wise Choices a Knee-Jerk Reaction by Natalia Gorelik, Courtney R. Green, Candyce Hamel, Anne-Marie LeBlanc, Bheeshma Ravi, Danielle R. Frost, Hugue Ouellette, Kuan-chin Jean Chen, Lisa Y. Liang, Nitai Gelber, Reza Mirza and Kawan S. Rakhra in Canadian Association of Radiologists Journal
Footnotes
Acknowledgements
We would like to thank Choosing Wisely Canada for collaborating with us on this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by a Canadian Radiological Foundation (CRF) and Canadian Heads of Academic Radiology (CHAR) Research Grant. Dr. Natalia Gorelik’s research work is supported by a Clinical Research Scholars - Junior 1 Award from the Fonds de Recherche du Québec - Santé (FRQS).
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.