
Abstract
The Canadian Association of Radiologists (CAR) Musculoskeletal System Expert Panel consists of musculoskeletal radiologists, a family physician, a sports and exercise medicine physician, emergency medicine physicians, a patient advisor, and an epidemiologist/guideline methodologist. After developing a list of 25 musculoskeletal clinical/diagnostic scenarios, a systematic rapid scoping review was undertaken to identify systematically produced referral guidelines that provide recommendations for 1 or more of these clinical/diagnostic scenarios. Recommendations from 41 guidelines (50 publications) and contextualization criteria in the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) for guidelines framework were used to develop 124 recommendation statements across the 25 scenarios related to the evaluation of the musculoskeletal system. This guideline presents the methods of development and the recommendations for imaging in the context of musculoskeletal pain, infection, tumors, arthropathies, metabolic bone disease, stress injuries, orthopedic hardware, avascular necrosis/bone infarction, and complex regional pain syndrome.
Introduction
Beginning in May 2021, an Expert Panel (EP) comprised of musculoskeletal radiologists, a family physician, a sports and exercise medicine physician, emergency medicine physicians, a patient advisor, and an epidemiologist/guideline methodologist met to develop a new set of recommendations specific to referral pathways for the musculoskeletal system. Through discussions (via virtual meetings) and offline communication, the EP developed a list of 25 clinical/diagnostic scenarios to be covered by this guideline. These recommendations are intended primarily for referring clinicians (eg, family physicians, emergency physicians, advanced care practitioners, other allied musculoskeletal specialities); however, they may also be used by radiologists, patients, and patient representatives.
Recommendation Text, Symbol, and Interpretation.
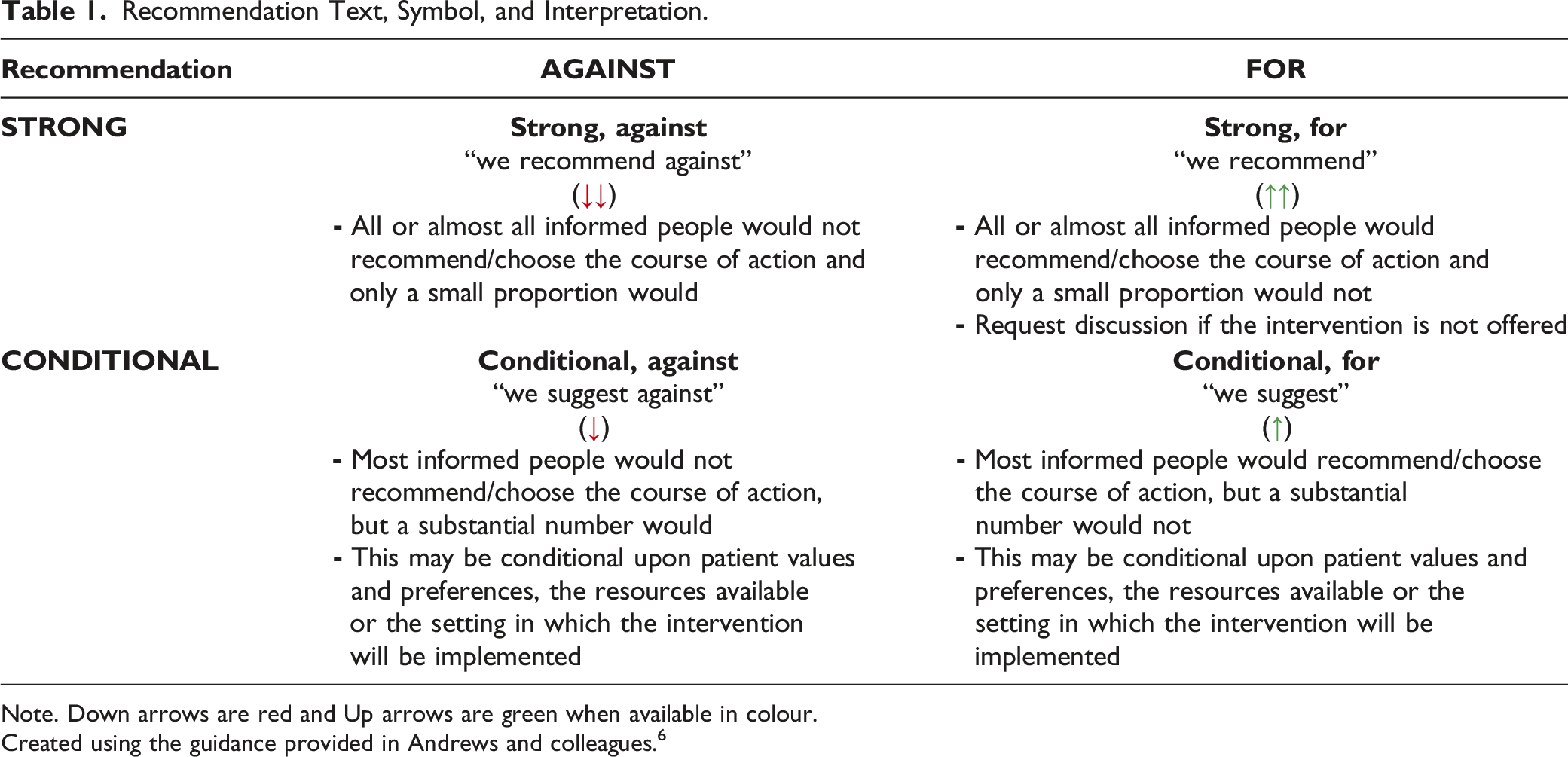
Note. Down arrows are red and Up arrows are green when available in colour.
Created using the guidance provided in Andrews and colleagues. 6
A systematic search for guidelines (with an a priori defined inclusion criteria) was run in Medline and Embase on July 22nd, 2021. The search was limited to publications from 2016 onward (Supplementary file Appendix 1). Supplemental searching included the following national radiology and/or guideline groups: the American College of Radiology (ACR), the National Institute for Health and Care Excellence (NICE), and the Royal College of Radiologists (RCR) 8th Edition (2017). Recommendations for each clinical scenario were formulated over 7 virtual meetings from September 2021 to February 2022. External review and feedback were obtained from radiologists, emergency physicians, a family physician, a nurse practitioner, an orthopaedic surgeon, a rheumatologist, and a nuclear medicine specialist. The full guideline can be found on the CAR website (www.car.ca).
Results
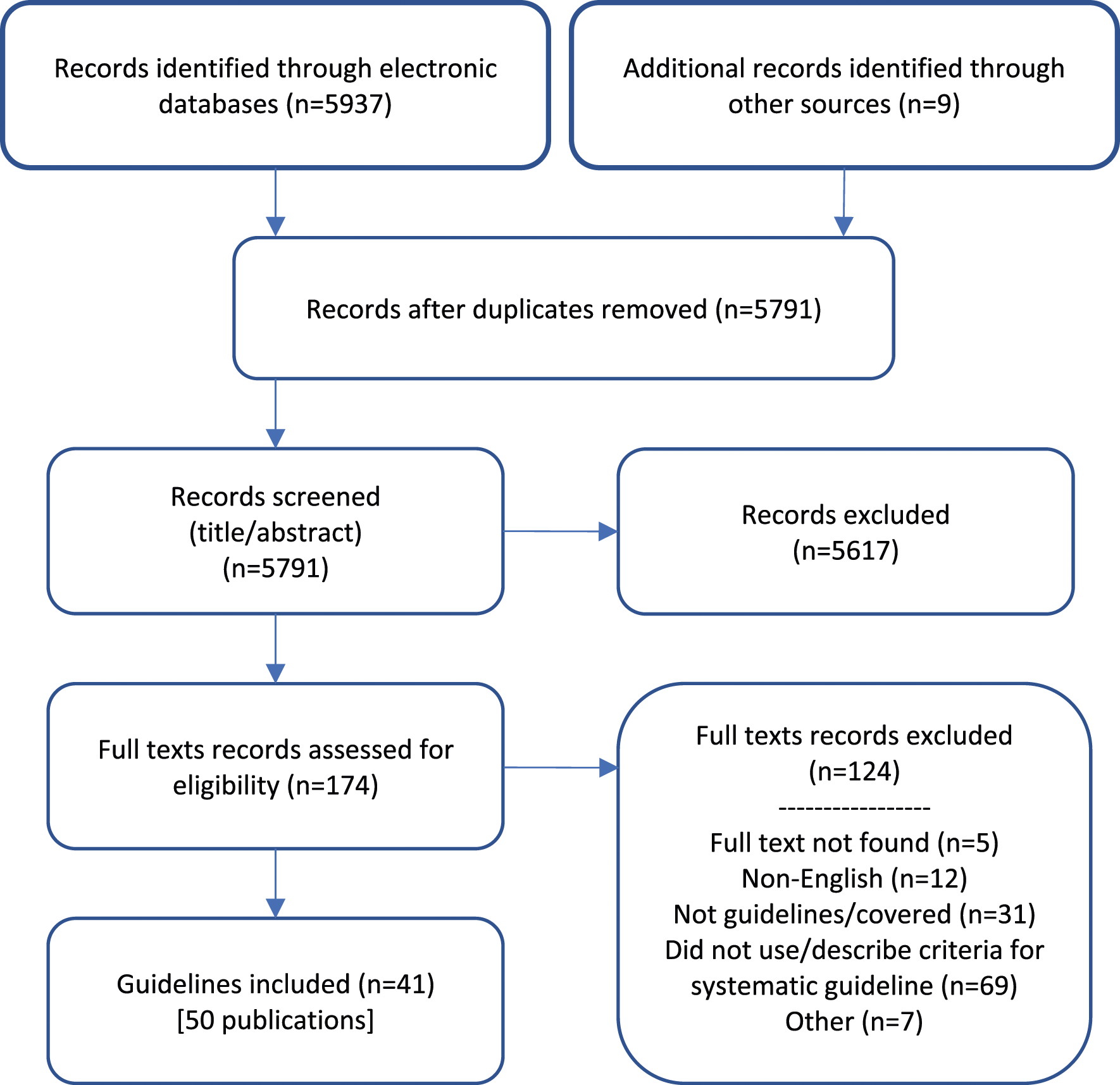
Systematic Scoping Review
A total of 5937 records were identified through the electronic database and 7 additional records were added from the supplemental search. A total of 41 guidelines, plus 9 companion papers, were included (Figure 1). Potentially relevant guidelines published in languages other than English can be found in Supplementary file Appendix 2. A list of excluded records including justifications for exclusion is available upon request. Most guidelines were rated as moderate or high quality, using the modified AGREE-II checklist (Supplementary file Appendix 3). The number of guidelines included per clinical/diagnostic scenario ranged from zero to 8, with a median of 4 guidelines per clinical scenario. PRISMA flow diagram.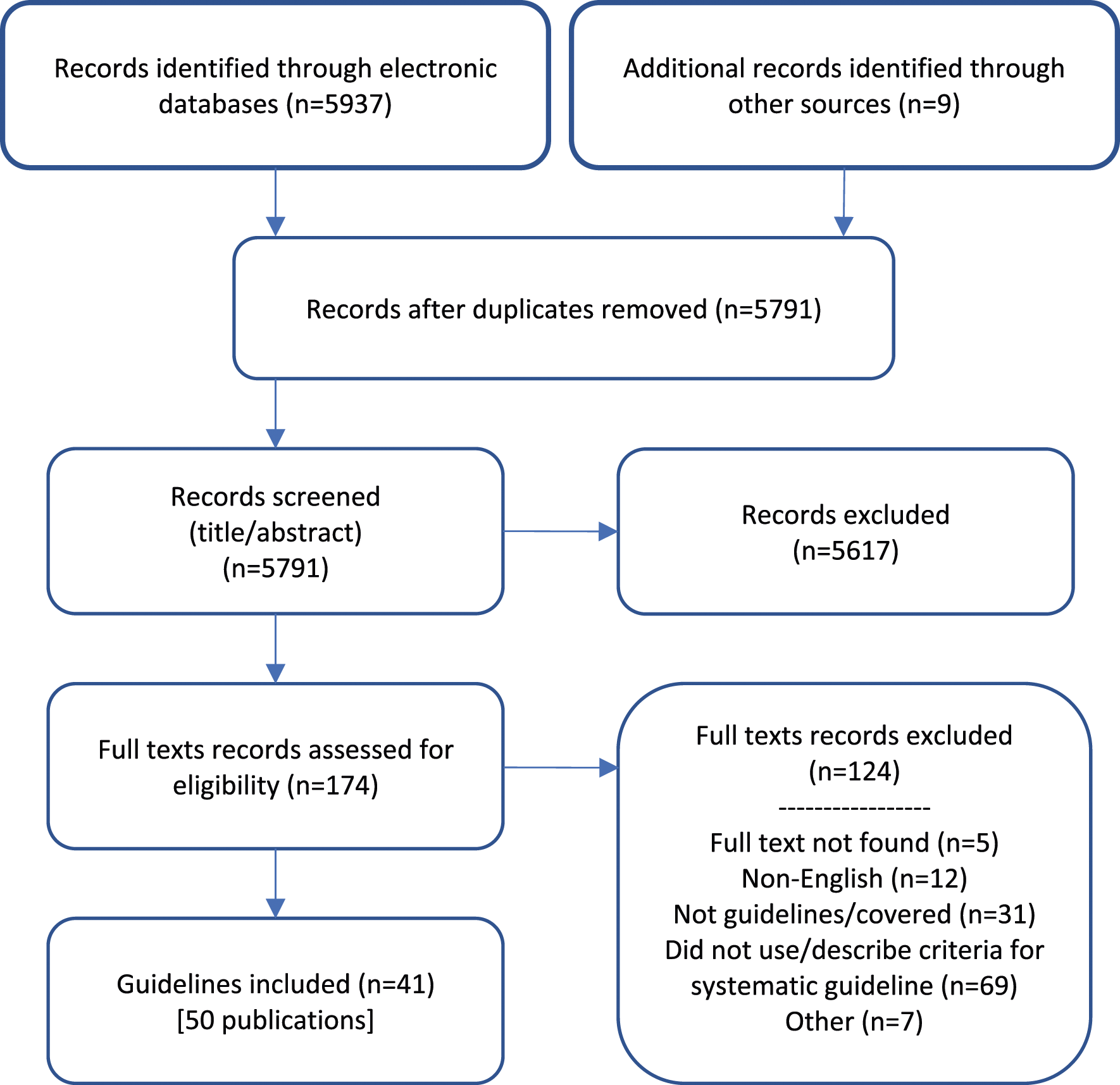
Recommendations
Additional details of the included guidelines, including which imaging modalities (ie, computed tomography [CT], computed tomography arthrography, dual-energy X-ray absorptiometry [DEXA], fluoroscopy, magnetic resonance arthrography, magnetic resonance imaging [MRI], nuclear medicine [NM], positron emission tomography [PET], radiograph [XR], ultrasound [US]) that were discussed can be found in Supplementary file Appendix 4.
A guideline is intended to guide and not be an absolute rule. Medical care is complex and should be based on evidence, a clinician’s expert judgment, the patient’s circumstances, values, preferences, and resource availability. Not all imaging modalities are available in all clinical environments, particularly in rural or remote areas of Canada. Decisions about patient transfer, use of alternative imaging or serial clinical examination and observation can be difficult. Therefore, the expected benefits of recommended imaging, risks of travel, patient preference, and other factors must be considered. The guideline recommendations address choice of imaging modality, not the management of individual patients in contexts where modalities are not available. Imaging should not delay definitive management.
We reviewed relevant recommendations related to the 25 clinical/diagnostic scenarios previously published by radiology and specialty societies, including: the Canadian Association of Radiologists, 9 the American Academy of Orthopaedic Surgeons, 10,11 the American College of Physicians (ACP), 12 the American College of Radiology (ACR), 13-30 the Brazilian Society of Rheumatology, 31 the combined guideline by the European Association of Nuclear Medicine, the European Bone and Joint Infection Society, and the European Society of Radiology, 32-34 the European League Against Rheumatism (EULAR), 35,36 the European Society of Musculoskeletal Radiology, 37 the European Society for Medical Oncology, 38 the German S-3 (the German Society for Orthopaedics and Traumatology [DGOOC] and the German Societies of Radiology [DRG], of Physical Therapy and Rehabilitation [DGPMR] and Osteology [DVO]), 39 the International Consensus on Orthopedic Infections, 40 the International Hip-related Pain Research Network, 41 the Lisbon Agreement, 42-44 the National Institute for Health and Care Excellence, 45-52 the Paget’s Association, 53 the Royal College of Radiologists (RCR), 54 the Society for Vascular Surgery in collaboration with the American Podiatric Medical Association and the Society for Vascular Medicine, 55 the Spanish Society of Rheumatology, 56 and the United States Preventive Services Task Force (USPSTF). 57,58
Although the ACR Appropriateness Criteria® Chronic Elbow Pain 59 did not meet the inclusion criteria for this guideline, as it was published in 2015, due to the lack of recommendations around other imaging modalities for the elbow pain scenario, it was referenced to provide additional support to the CAR discussions and recommendations.
Soft Tissue and Bone Infection, Bone Tumour, Soft Tissue Mass, and Soft Tissue Pain Recommendations.
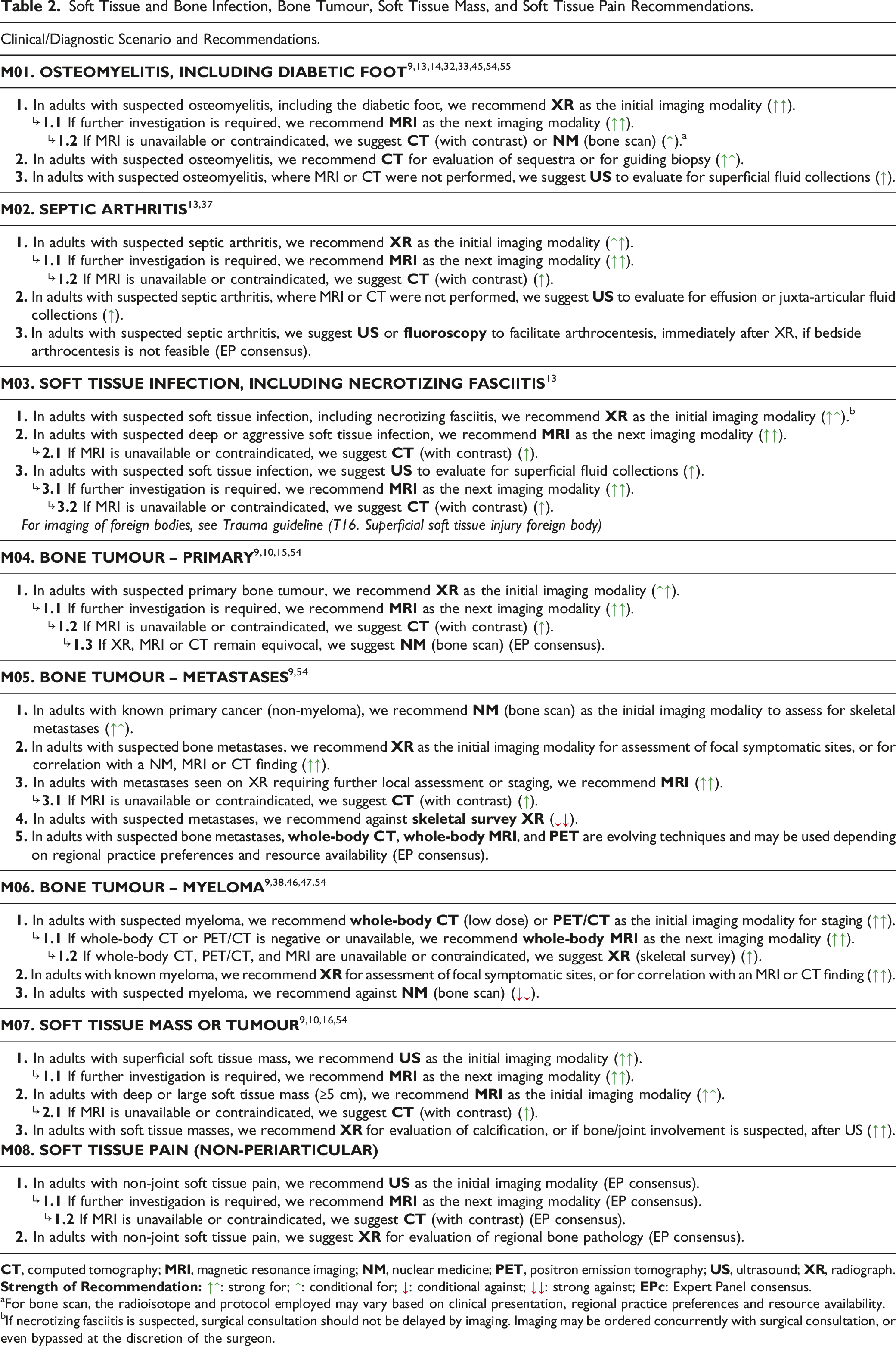
aFor bone scan, the radioisotope and protocol employed may vary based on clinical presentation, regional practice preferences and resource availability.
bIf necrotizing fasciitis is suspected, surgical consultation should not be delayed by imaging. Imaging may be ordered concurrently with surgical consultation, or even bypassed at the discretion of the surgeon.
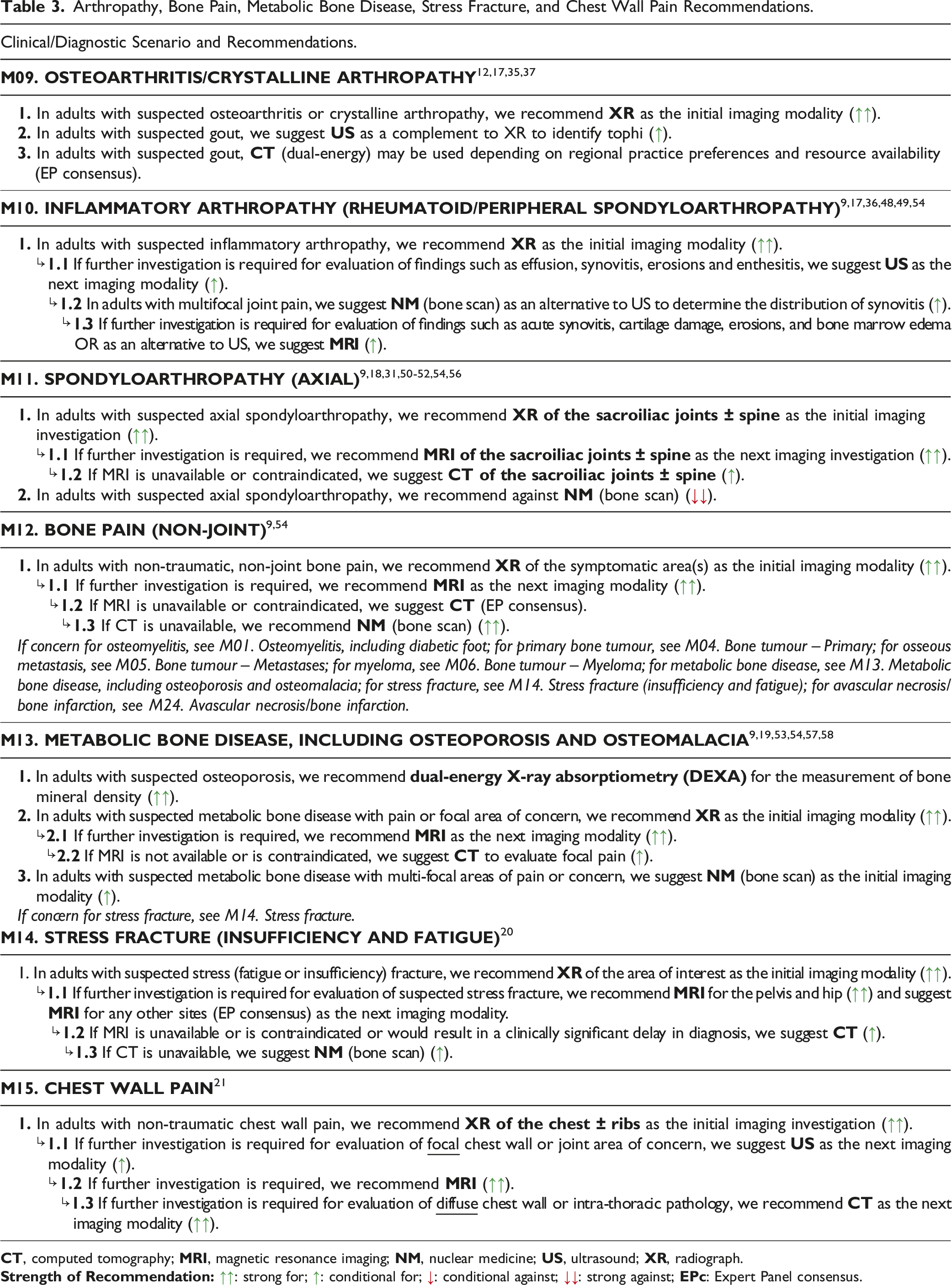
Arthropathy, Bone Pain, Metabolic Bone Disease, Stress Fracture, and Chest Wall Pain Recommendations.
Shoulder, Elbow, Hand/Wrist, MSK Pelvis or Hip, Knee, Ankle, Foot, and Orthopedic Hardware/Arthroplasty Pain, Avascular Necrosis/Bone Infarction, and Complex Regional Pain Syndrome Recommendations.
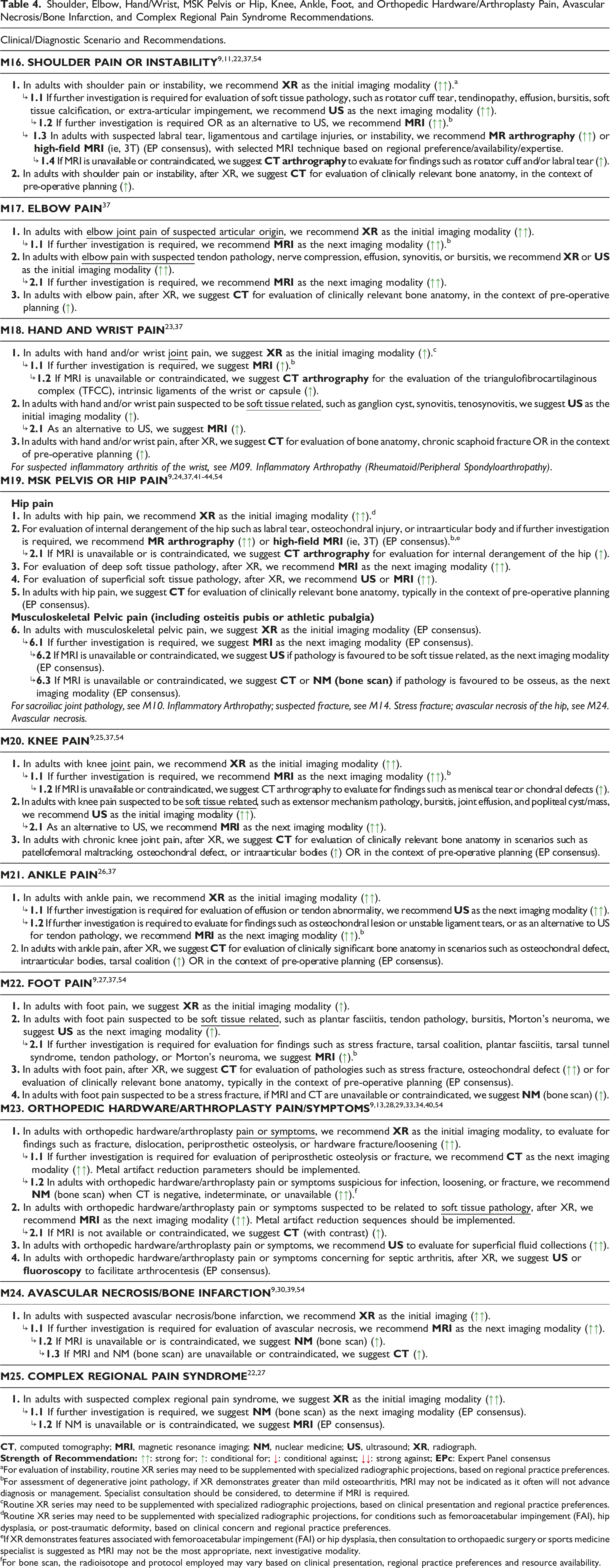
aFor evaluation of instability, routine XR series may need to be supplemented with specialized radiographic projections, based on regional practice preferences.
bFor assessment of degenerative joint pathology, if XR demonstrates greater than mild osteoarthritis, MRI may not be indicated as it often will not advance diagnosis or management. Specialist consultation should be considered, to determine if MRI is required.
cRoutine XR series may need to be supplemented with specialized radiographic projections, based on clinical presentation and regional practice preferences.
dRoutine XR series may need to be supplemented with specialized radiographic projections, for conditions such as femoroacetabular impingement (FAI), hip dysplasia, or post-traumatic deformity, based on clinical concern and regional practice preferences.
eIf XR demonstrates features associated with femoroacetabular impingement (FAI) or hip dysplasia, then consultation to orthopaedic surgery or sports medicine specialist is suggested as MRI may not be the most appropriate, next investigative modality.
fFor bone scan, the radioisotope and protocol employed may vary based on clinical presentation, regional practice preferences and resource availability.
Supplemental Material
Supplemental Material - Canadian Association of Radiologists Musculoskeletal System Diagnostic Imaging Referral Guideline
Supplemental Material for Canadian Association of Radiologists Musculoskeletal System Diagnostic Imaging Referral Guideline by Candyce Hamel, Barb Avard, Natalia Gorelik, Martin Heroux, David Mai, Adnan Sheikh, Anthony Vo, Mary-Lynn Watson and Kawan Rakhra in Canadian Association of Radiologists Journal
Footnotes
Acknowledgments
We would like to thank: Becky Skidmore for creating the search strategies for the systematic scoping review, Leila Esmaeilisaraji for her role as a reviewer on the scoping review, and the following individuals on the Diagnostic Imaging Referral Guidelines Working Group and external stakeholders for providing feedback on the guideline (listed alphabetically): Sibel Aydin, Samuel Campbell, Noel Corser, Nicolas Dea, Bruce Foster, George Grammatopoulos, Michel Leblanc, Ryan Margau (WG co-chair), Paul Pageau (WG co-chair), Charlotte Yong-Hing, Kaitlin Zaki-Metias
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Medical Association.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.