
Abstract
Neurosonography (NSG) is pivotal for rapid, point-of-care neonatal brain assessment. This review elucidates the comprehensive applications of NSG in pediatric care, emphasizing its role in early diagnosis and management of pathologies affecting the pediatric head—such as scalp lesions, misshapen calvarium, ventricular distortions, and cerebrovascular abnormalities, and its specific role in conditions like hypoxic-ischaemic encephalopathy (HIE) across different neonatal gestational ages. We explore its diagnostic advantage in critical care settings, particularly for infants with stroke risk in sickle cell disease, ECMO-related complications, screening for therapeutic hypothermia, and routine neonatal intensive care unit monitoring. This review discusses the recommendations based on the timing of brain injury (preterm and term) and describes technical considerations that enhance diagnostic accuracy. Ultimately, this article advocates for its incorporation into routine neonatal screening to improve neurodevelopmental outcomes, underscoring its importance in clinical decision-making and long-term management of pediatric brain disorders.
Introduction
Neurosonography (NSG) is an initial imaging modality for assessing the neonatal brain. NSG can be performed bedside in the intensive care unit with no radiation exposure. It has several advantages as it is readily available, cost-effective, real-time, and portable compared to MRI. The NSG aims to detect brain injury, structural abnormalities, and understand the timing and evolution of parenchymal injury. It also aids in making accurate diagnoses to facilitate clinical decision-making and monitor the growth and brain maturation in the neonatal period.
With technological innovation, improved image resolution, and faster processing, NSG is reliable in the early diagnosis of brain injury in infants at risk of neurodevelopmental impairment, allowing timely initiation of optimal therapy and eventually improving neurological outcomes. In this review, we highlight the indications of NSG and emphasize the technique and sonographic anatomy with a systematic approach to the diverse spectrum of pathologies affecting the head, including neonatal haemorrhages, sutural abnormalities, hypoxic-ischaemic encephalopathy, congenital masses and malformations, and cerebrovascular abnormalities.
Indications
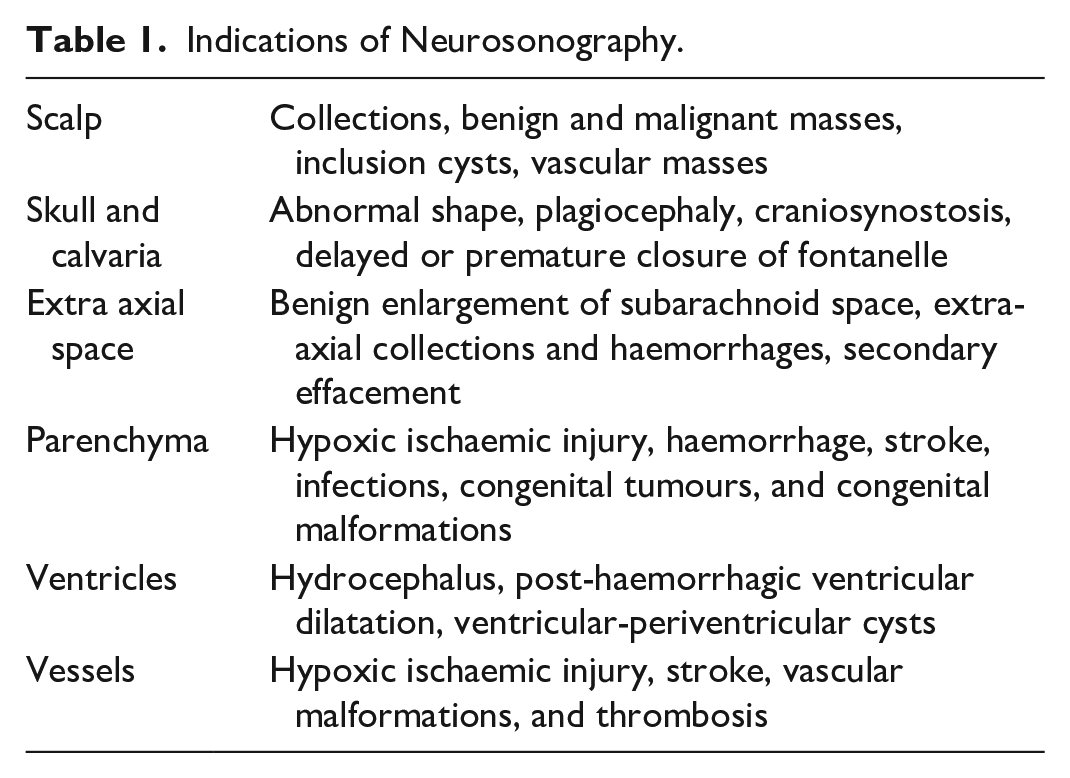
NSG plays a critical, multifaceted role in evaluating pediatric brain abnormalities, primarily indicated for screening all newborns with suspicion and risk of brain injury. The American Institute of Ultrasound in Medicine practice parameters outline the specific indications for NSG in neonates and infants.1,2 This article presents an anatomically based framework, beginning with the outermost scalp, followed by skull and sutures, extra-axial spaces, brain parenchyma, ventricles, and intracranial vessels, as described in Table 1.
Indications of Neurosonography.
Timing of Neurosonography in Neonates
Preterm Infants (<31 + 6 Weeks Gestational Age)
For preterm infants born at ≤31 + 6 weeks, the position statement by the Canadian Pediatric Society recommends NSG for routine surveillance at 4 to 7 days to detect germinal matrix haemorrhage (GMH), intraventricular haemorrhage (IVH), and early ventricular dilatation. 3
In infants with Grade 2 or higher IVH or white matter injury, a follow-up NSG should be performed every 7 to 10 days. If ventricular dilatation or worsening post-haemorrhagic ventricular dilatation (PHVD) occurs, the imaging frequency should be intensified, at least weekly initially and as clinically indicated later. 3
Term-corrected NSG is recommended for preterm infants born before 26 weeks’ gestation and for infants born between 26 + 0 and 31 + 6 weeks gestational age in case of additional risk factors or previous moderate-to-severe abnormality, including grade 3 or higher IVH, PHVD, or cystic periventricular leukomalacia (PVL). 3
Preterm infants (32 + 0 to 36 + 6 Weeks Gestational Age)
For the late and moderately preterm infant (32 + 0 to 36 + 6 GA) with additional risk factors, an NSG is recommended 4 to 7 days after birth, followed by repeat imaging at 4 to 6 weeks in case of imaging abnormality on initial NSG. Term-corrected NSG is not routinely recommended for late and moderately preterm infants. 3
Technique and Settings
NSG is preferably done through the cranial incubator in the NICU and at the bedside or in the ultrasound room during infancy and childhood. During the examination, adequate care should be taken to avoid moving the infant and causing any disturbance to the incubator temperature and pressure over the anterior fontanelle for optimal Doppler assessment.
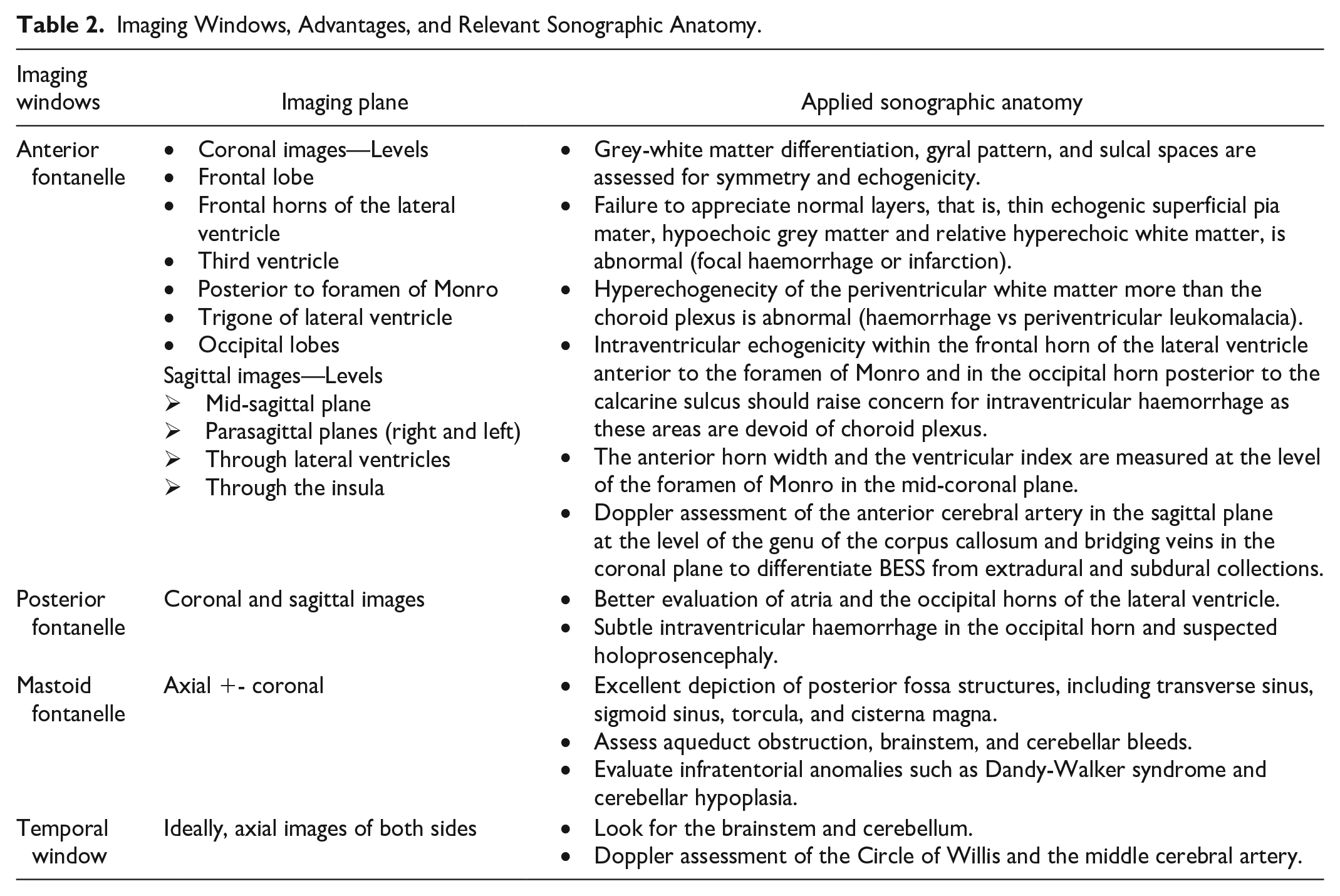
NSG starts with grey-scale imaging performed through the anterior fontanelle in coronal and sagittal planes using the multifrequency phased array, curved array, and linear array transducers (5-18 MHz). The choice of transducer frequency is a compromise between resolution and penetration with the optimal near-field resolution of higher frequencies and better penetration depth of lower frequencies. The focus point is centred on ventricular areas and can be altered based on the region of interest. Appropriate gain adjustment helps interpret the imaging findings reliably, and adequate depth of view is necessary for better assessment of the posterior part of the brain. Coronal planes are acquired through the anterior fontanelle with anterior-to-posterior angulation with the transducer marker pointing to the right side (7 standard planes).2,4 Sagittal imaging uses a mid-sagittal view with the transducer pointing anteriorly, and left and right parasagittal views extend from the midline through the caudothalamic grooves, deep white matter, insula, Sylvian fissures, and peripheral cortex on both sides (7 standard planes)2,4 (Figure 1A and B). Cine loops may also be obtained to supplement the coronal and sagittal images. Additional images are acquired through the posterior and mastoid fontanelles. The primary and supplemental imaging windows, their advantages, and relevant sonographic anatomy are described in Table 2, Supplemental Videos 1 to 3.
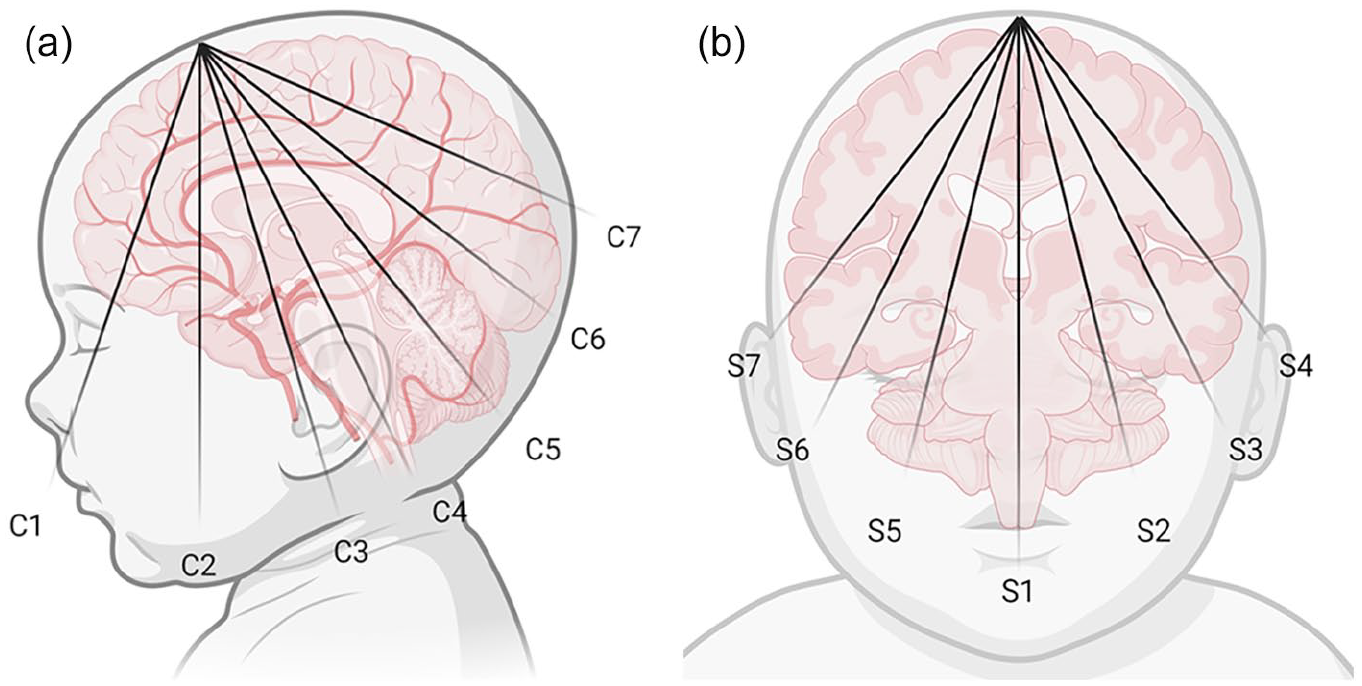
(A) Sagittal graphic representation showing standard coronal planes performed through the anterior fontanelle, at the level of frontal lobes (C1); frontal horns of the lateral ventricle (C2); lateral ventricles at the level of foramina of Monro (C3); lateral ventricles posterior to the foramina of Monro (C4); quadrigeminal plate cistern and cerebellum (C5); echogenic glomi of the choroid plexus (C6); and posterior to the occipital horns including parietal and occipital lobes (C7). (B)
Imaging Windows, Advantages, and Relevant Sonographic Anatomy.
Colour Doppler images are mandatory when screening arterial and venous structures. Doppler imaging assessment of the anterior cerebral artery (ACA) at the genu and the region of the superior sagittal sinus (SSS) and vein of Galen are an integral part of the assessment. Spectral tracing with peak systolic velocity (PSV), end-diastolic velocity (EDV), and resistive index (RI) is essential to evaluate hypoperfusion, ischaemia, and cerebral oedema in post-haemorrhagic ventricular dilatation and underlying cardiac abnormalities. Power Doppler and B-flow imaging help assess hyper- and hypoperfused areas.
Finally, high-resolution linear array transducer images are obtained to assess the convexity subarachnoid spaces, peripheral cortex, and deeper brain structures. Linear images are also used to assess the scalp, sutures, extra-axial spaces, and vascular structures.
Teaching Points
In preterm neonates, to ascertain periventricular leukomalacia, the findings must be confirmed on 2 orthogonal planes as prominent periventricular echogenicity could be due to the anisotropic effect caused by the perpendicular ultrasound beam striking the peri-atrial white matter tracts.
In preterm neonates, the RI tends to be elevated (up to 0.90) due to low intracerebral diastolic flow velocities. In term infants, it can be as low as 0.65, reflecting improved diastolic flow due to physiologic transition. 4
The ACA RI has to be carefully evaluated in cardiac disease, primarily due to variability in the end-diastolic flow. The intracranial arteriovenous malformations demonstrate irregular and biphasic spectral patterns.
Normal Variants of the Brain on Neurosonography
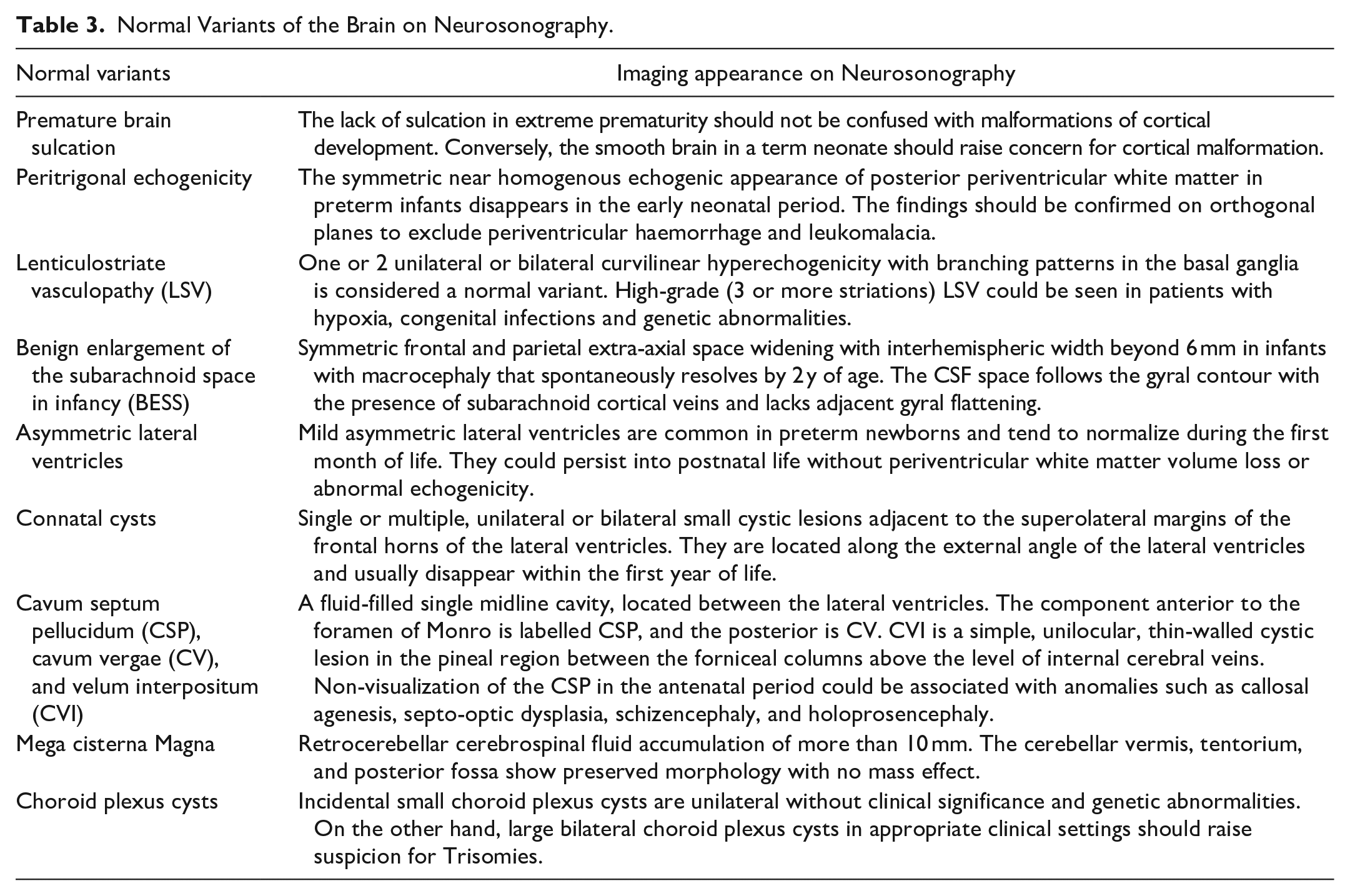
Adequate awareness of the imaging appearances on neurosonography is necessary to avoid potential misdiagnosis, and the normal variants are described in Table 3.
Normal Variants of the Brain on Neurosonography.
Pathologies
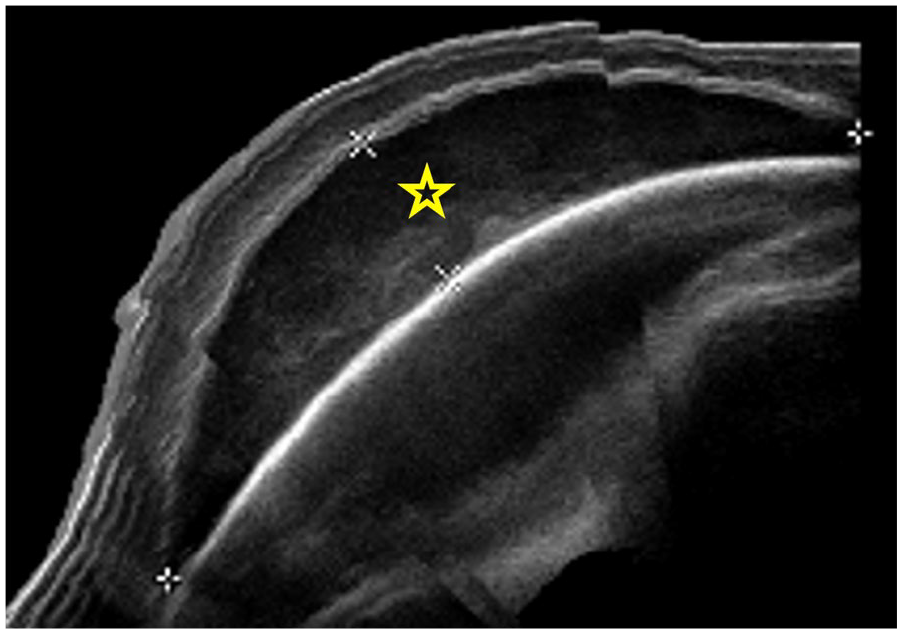
Newborn following vacuum-assisted delivery. The panoramic ultrasound image reveals the right parietal heterogeneous echogenic collection, suggesting cephalohaematoma (star), which does not cross the midline or sutures.
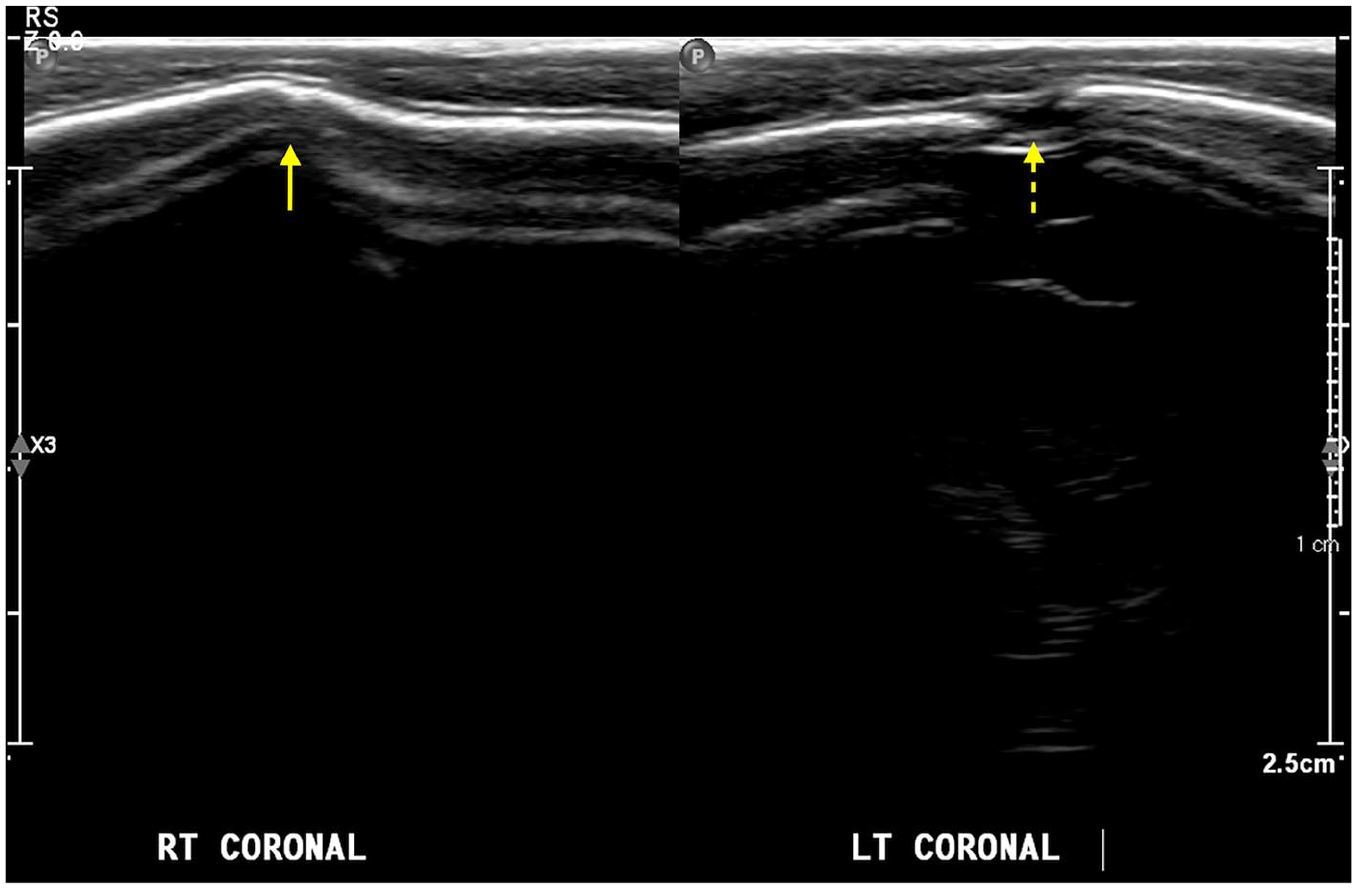
Three-month-old female with anterior plagiocephaly. Coronal ultrasound image with linear array transducer shows fusion of the right coronal suture, in keeping with coronal craniosynostosis (arrow) compared to the patent coronal suture on the normal left side (dashed arrow).
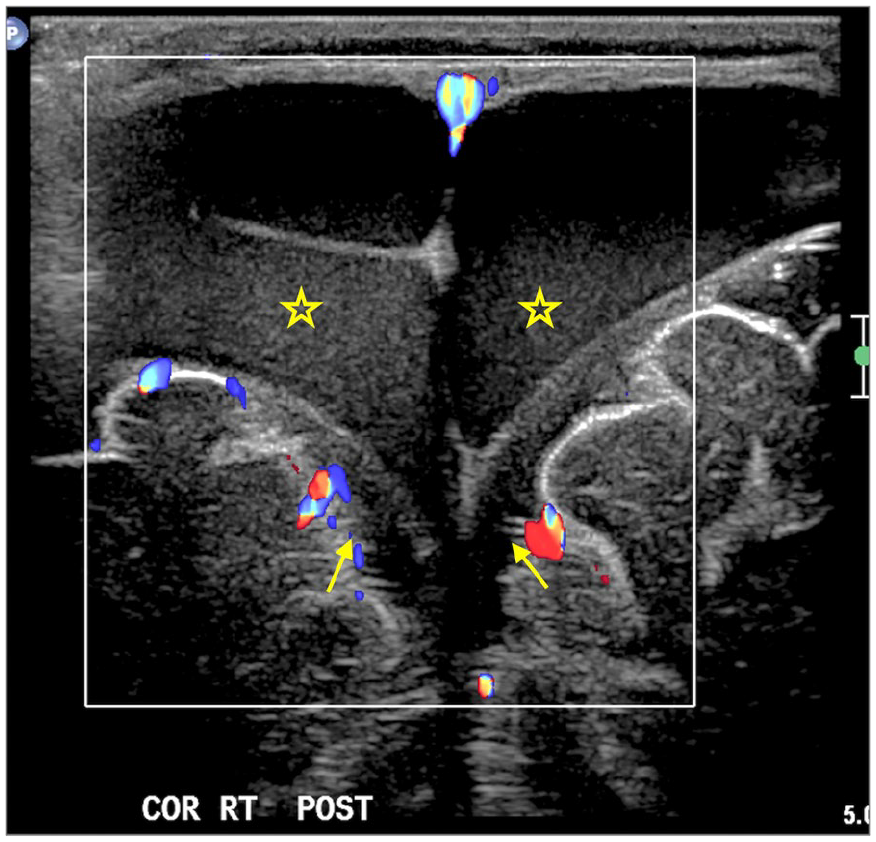
Five-month-old patient with increasing head circumference. Coronal ultrasound image with a linear array transducer shows bilateral subdural collections (stars) with internal echoes in the medial parietal parafalcine region, causing mildly effaced underlying subarachnoid spaces (arrows).
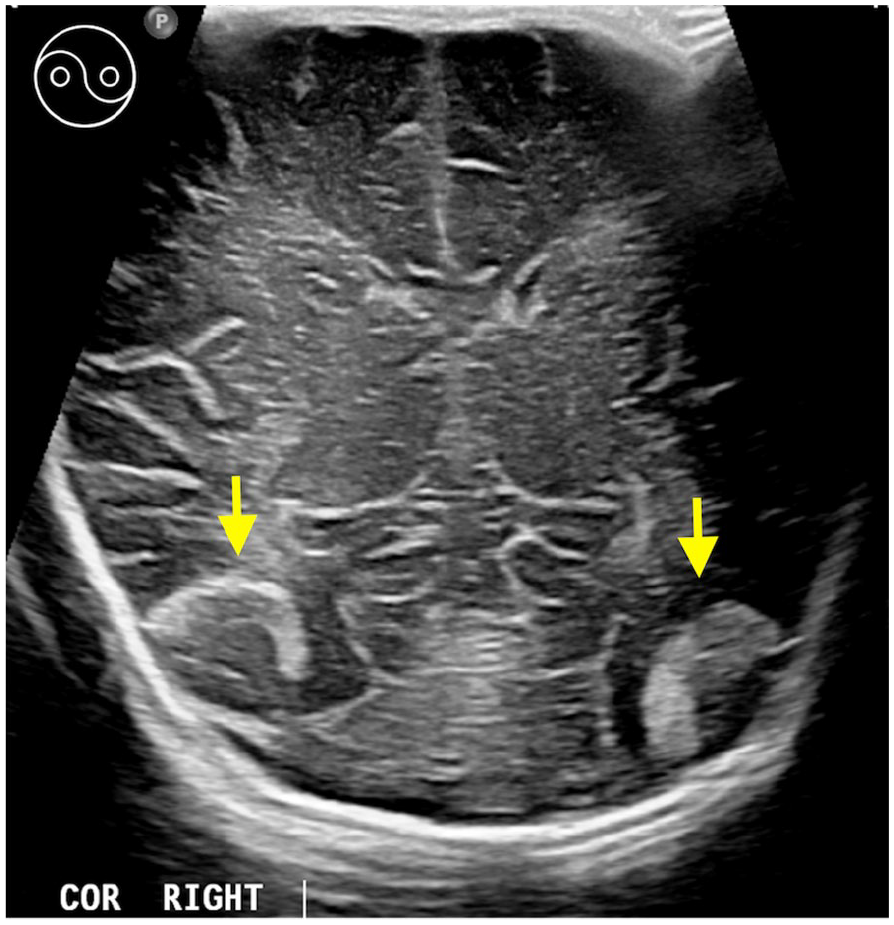
Two-day-old with premature baby for screening. Coronal ultrasound image with a linear array transducer reveals bilateral inferior temporal extra-axial gyriform mixed echogenicity causing sulcal widening (arrows). The larger subpial haemorrhage along the right inferior temporal region shows a Yin-Yang appearance (inset image in left upper corner).
Six-month-old male with a head circumference above 97th percentile for age and sex-matched controls. Coronal ultrasound image with a linear array transducer demonstrates enlarged extra-axial CSF spaces with normal traversing vessels, suggesting benign enlargement of the subarachnoid sulcal spaces (BESS).
Parenchyma
Key Imaging Findings in Hypoxic-Ischaemic Encephalopathy.
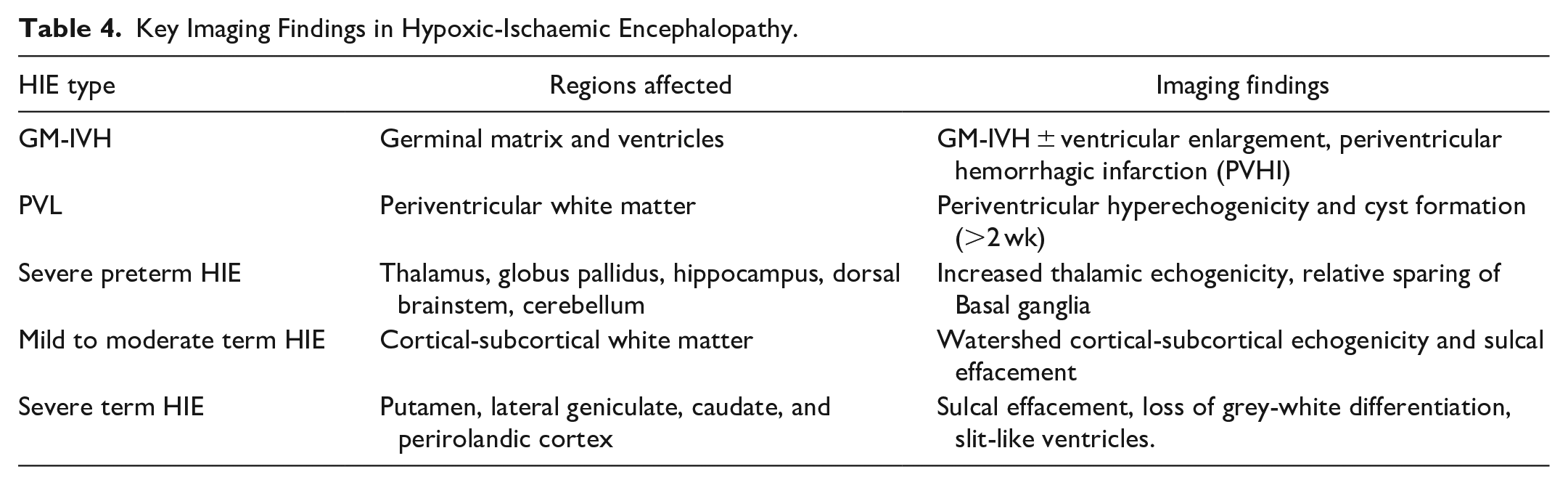
Germinal Matrix-Intraventricular Haemorrhage (GM-IVH): The germinal matrix containing fragile blood vessels is susceptible to fluctuations in systemic blood pressure and oxygen levels.26,29 Most haemorrhages happen within the first 3 to 4 days of life (critical window).30,31 NSG is essential for monitoring high-risk infants, especially those born before 30 weeks and extremely low birth weight and for the grading of GM-IVH.20,28,32
Grade 1: Confined to the germinal matrix (Figure 7A). Grade 2: Extends into the lateral ventricle without dilatation (Figure 7B). Grade 3: Grade 2 with ventricular dilatation in early/initial scan with AHW measuring >6 mm (Figure 7C). Periventricular Haemorrhagic Infarction (PVHI): Rare ischaemic injury affects brain tissue adjacent to a GM-IVH (5% of cases), often resulting from damage to terminal subependymal veins (Figure 7D). PVHI has a high risk of long-term neurological impairment.21,31,33 It is critical to assess whether PVHI is unilateral or bilateral, extent of involvement and the presence of midline shift.
21
Cerebellar Haemorrhage: Haemorrhage in the external granule cell and subependymal layers (cerebellar germinal zones) haemorrhages are rare but more frequent in babies with very low birth weight (<750 g), traumatic delivery, and ECMO babies (Supplemental Figure 4).21,28,30,34
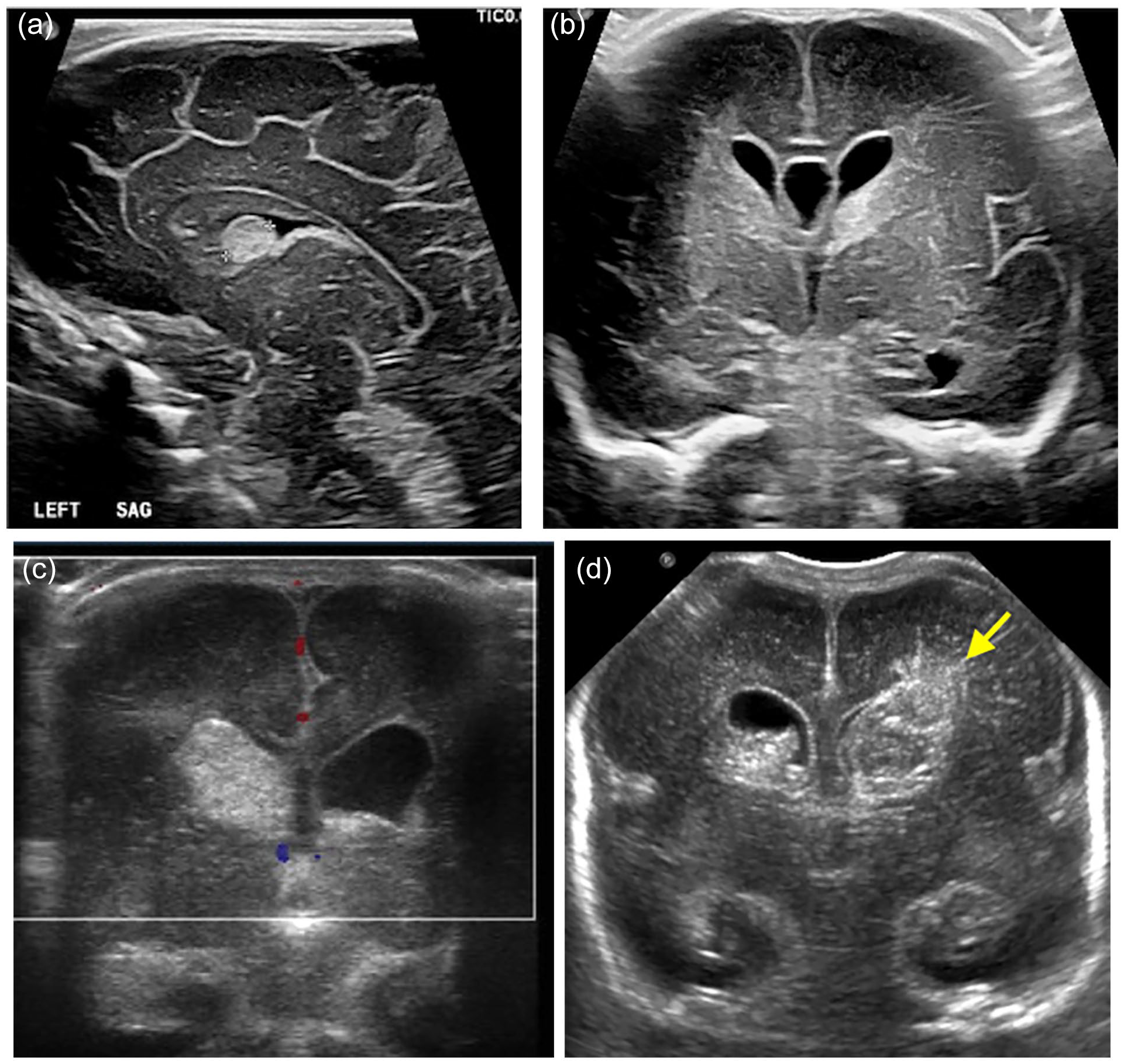
Parasagittal ultrasound image with a linear transducer array (A) shows echogenic focus in the caudothalamic groove (Grade I—GMH-IVH). Coronal images (B and C) with a linear transducer array show echogenic focus in the left caudothalamic groove and temporal horn of the right lateral ventricle in B (Grade II—GMH-IVH) and right caudothalamic groove bleed with right frontal and temporal horns extension and mild ventricular enlargement in C (Grade III—GMH-IVH). Coronal image with a curvilinear transducer array (D) shows bilateral germinal matrix haemorrhages with ventricular extension and left periventricular haemorrhagic infarction (Grade III + PVHI) (arrow).
A 5-day-old preterm boy with mild HIE. Coronal ultrasound image with a linear array transducer demonstrates the asymmetric increased echogenicity in the bilateral periventricular white matter confirmed in a follow-up MRI study (not shown).

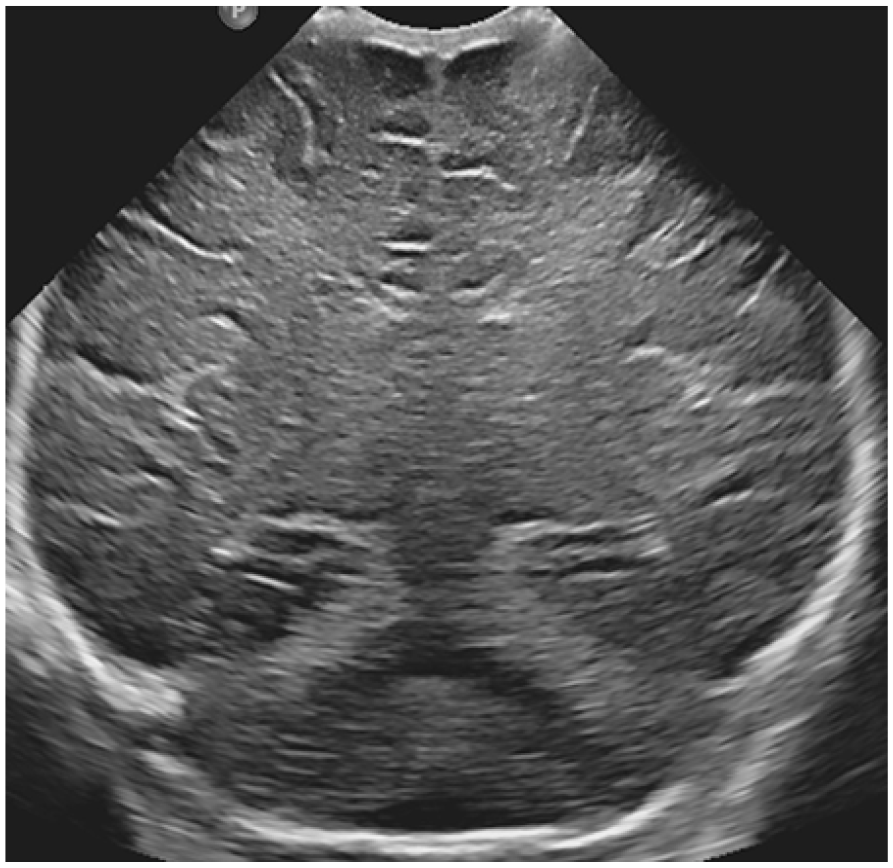
Newborn with prolonged labour and severe preterm HIE. Coronal ultrasound image with a linear array transducer demonstrates diffusely increased echogenicity of the deep and periventricular white matter and bilateral gangliothalamic region (stars) with effacement of the sulci and ventricles.
Mild to Moderate HIE: Involves peripheral watershed regions, showing increased echogenicity in the subcortical white matter with accentuated grey-white matter differentiation of the parasagittal frontal and parietal regions.20,21,26,39 Prolonged hypoxia may involve basal ganglia and often cause widespread echogenicity with cerebral oedema, slit-like ventricles, effaced extra-axial CSF spaces, and low RI in the Doppler study.21,26,39
Severe HIE: Targets more advanced myelinated areas, including the caudate nucleus, putamen, perirolandic cortex, ventrolateral thalamus, hippocampus, and dorsal brainstem.20,21,26,28,39 In severe cases, cortical and subcortical injury may lead to sulcal effacement, loss of grey-white matter differentiation, and slit-like ventricles (Figure 10). ACA RI below 0.55 correlates with poor neurodevelopmental outcomes (Supplemental Figure 6).32,41
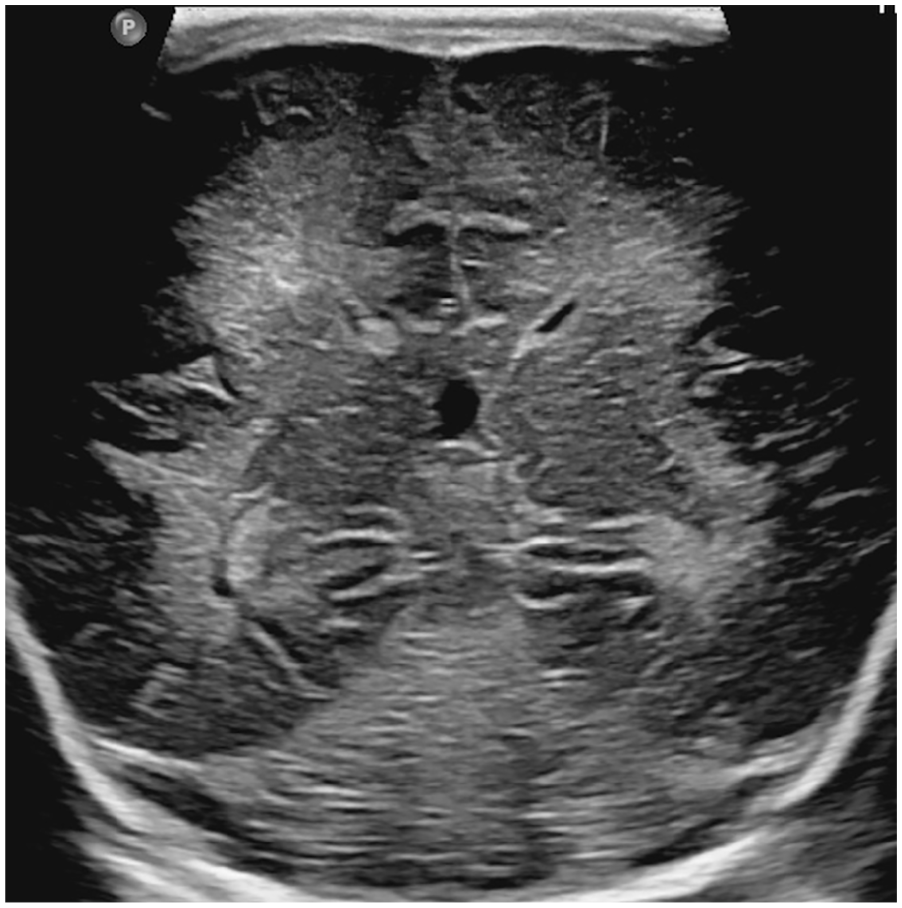
Term baby with severe HIE. Coronal ultrasound image with a curvilinear array transducer reveals diffuse increased echogenicity involving the visualized brain parenchyma with slit-like ventricles, effaced sulcal spaces, and low resistive index (not shown).
Neonatal Stroke
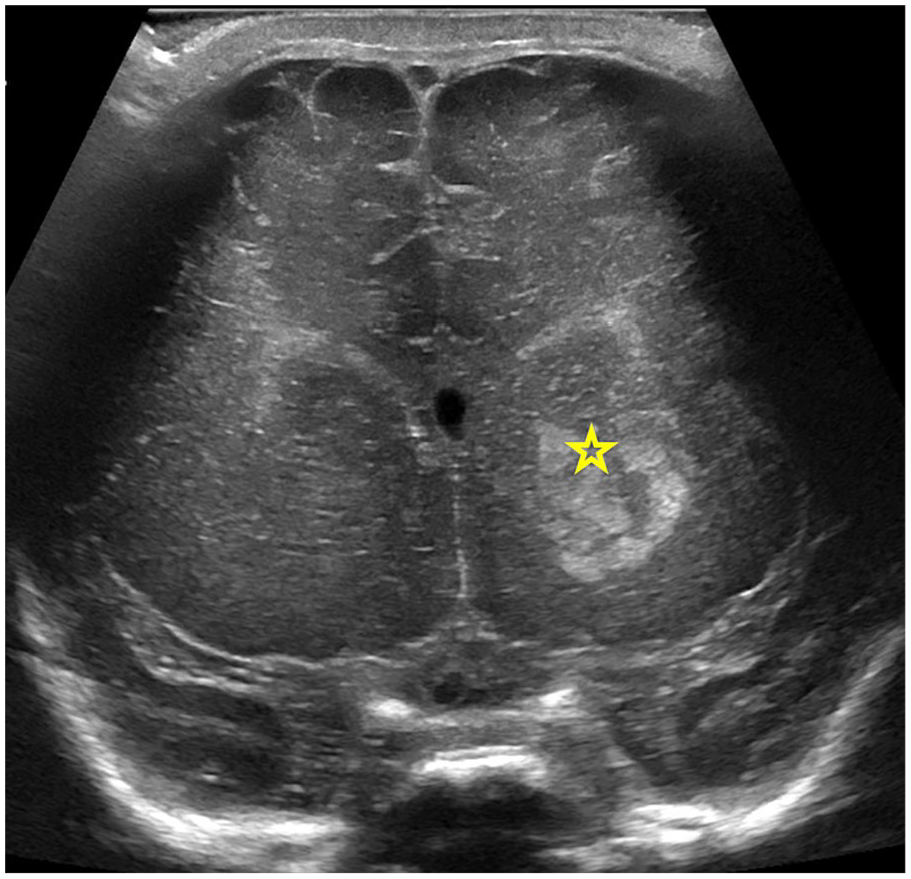
Two-day-old term baby with left upper extremity arterial clot for screening US head before initiation of heparin. Coronal ultrasound image with a linear array transducer reveals a hyperechoic and bulky left basal ganglia (star), concerning for neonatal ischaemic infarction, confirmed on MRI (not shown).
Neonatal Infections
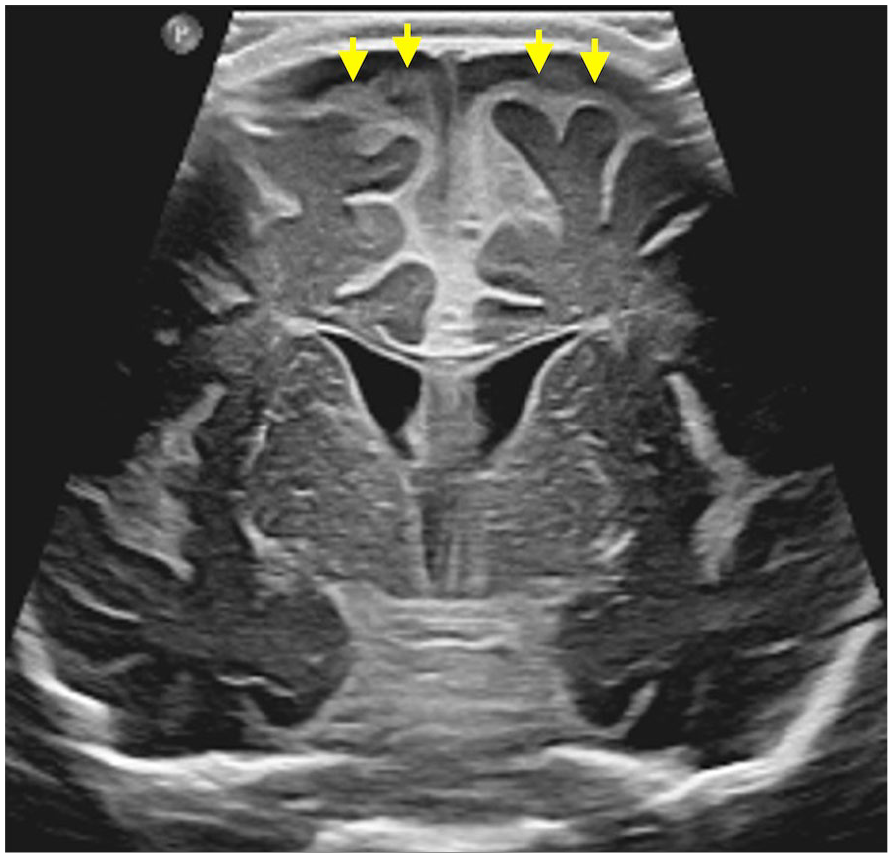
Seven-day-old girl, serology positive for congenital CMV infection. Coronal ultrasound image with a linear array transducer shows tiny periventricular echogenic foci (circle), from suspected calcifications, left germinolytic cysts (not shown), and abnormal sulcation (arrows), suggesting polymicrogyria.
Two-month-old female admitted for H Influenza meningitis. Coronal ultrasound image with a linear array transducer reveals diffuse echogenic thickening of the leptomeninges and prominent extra-axial spaces with internal echoes (arrows). Mildly increased echogenicity of the ventricular wall is concerning for ventriculitis. Findings were confirmed on contrast MRI (not shown).
Supratentorial Malformations
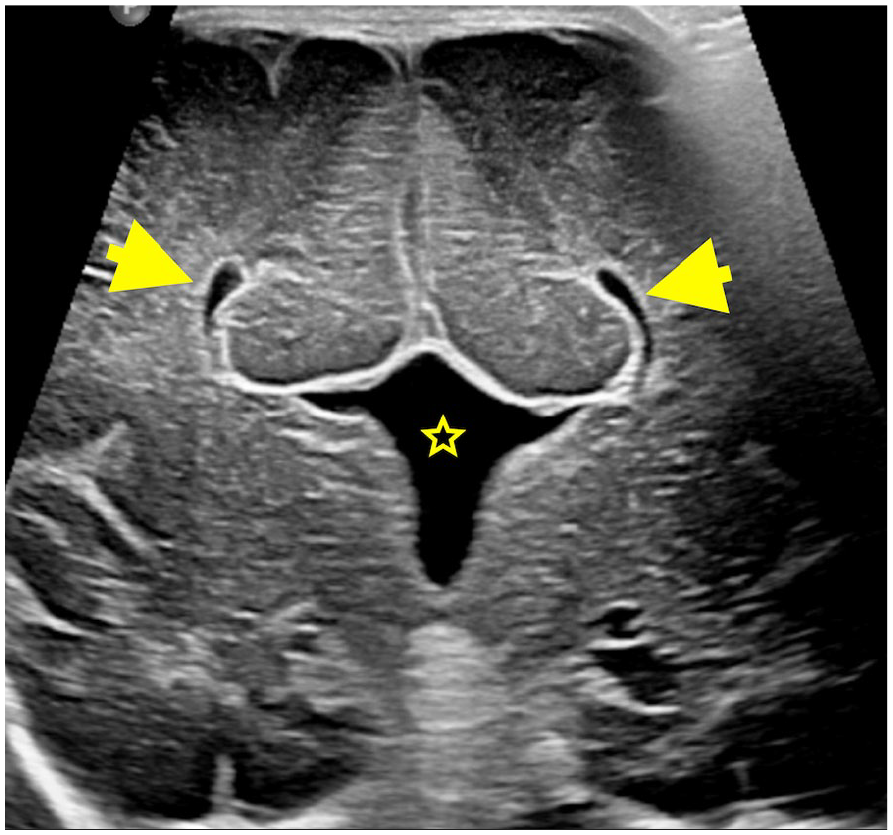
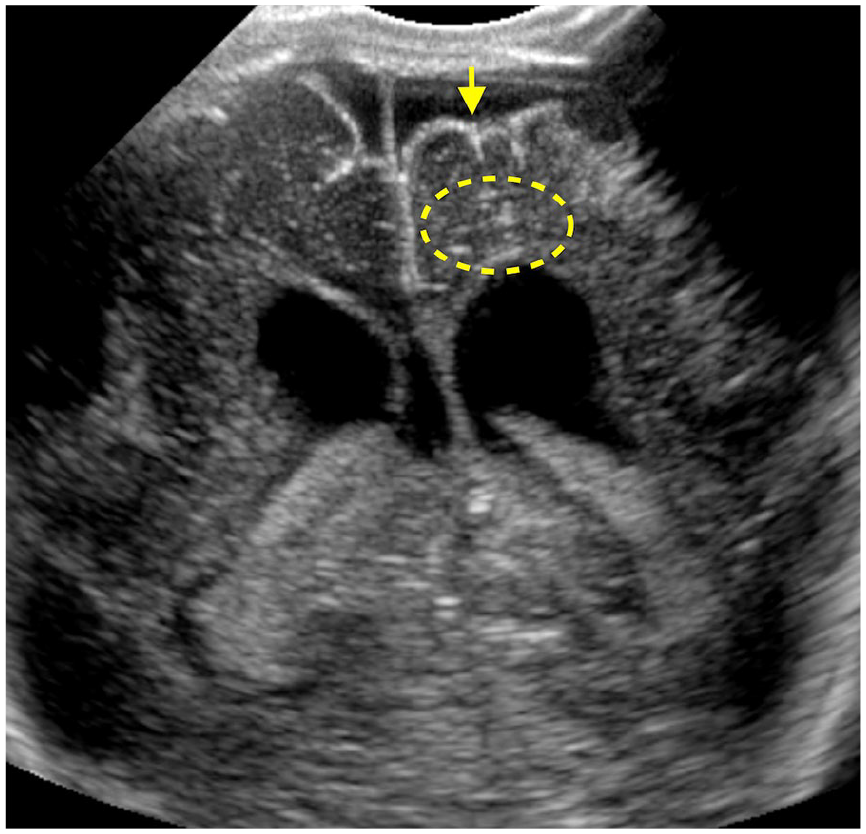
Coronal ultrasound image with a linear array transducer demonstrates the absence of septum pellucidum and agenesis of the corpus callosum with parallel oriented lateral ventricles, “Viking horn” appearance (arrows) and a prominent and high-riding third ventricle (star).
Infratentorial Malformations
Ventricles
Vessels
Doppler ultrasound is essential in evaluating various neonatal brain conditions, including ischaemia, thrombosis, and cardiac- and ECMO-related complications. It also helps distinguish subdural fluid collections from BESS and assess intracranial vascular masses.
a.
b.
c.
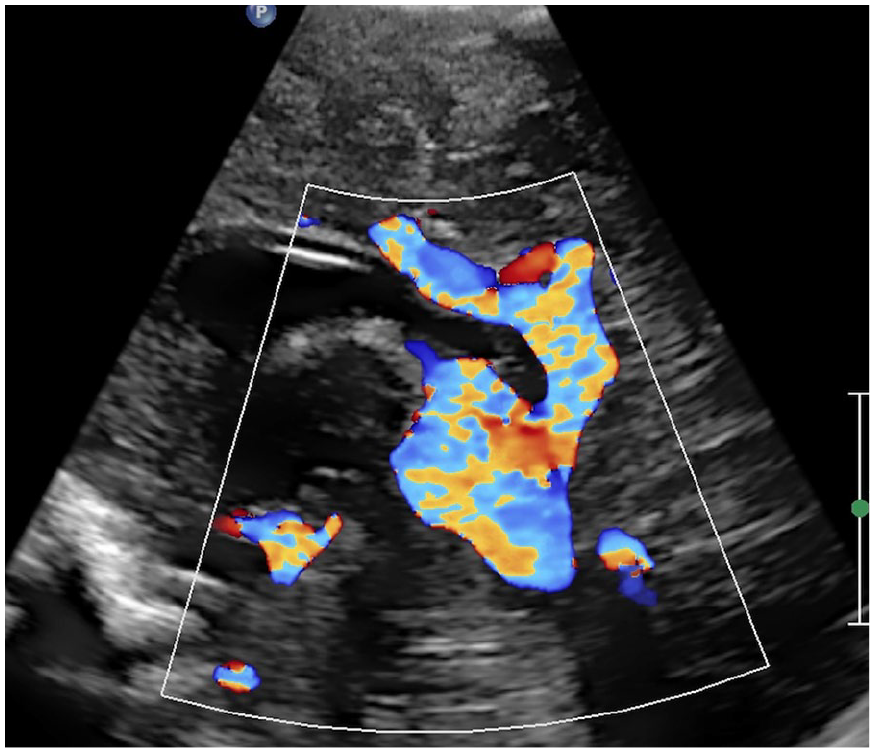
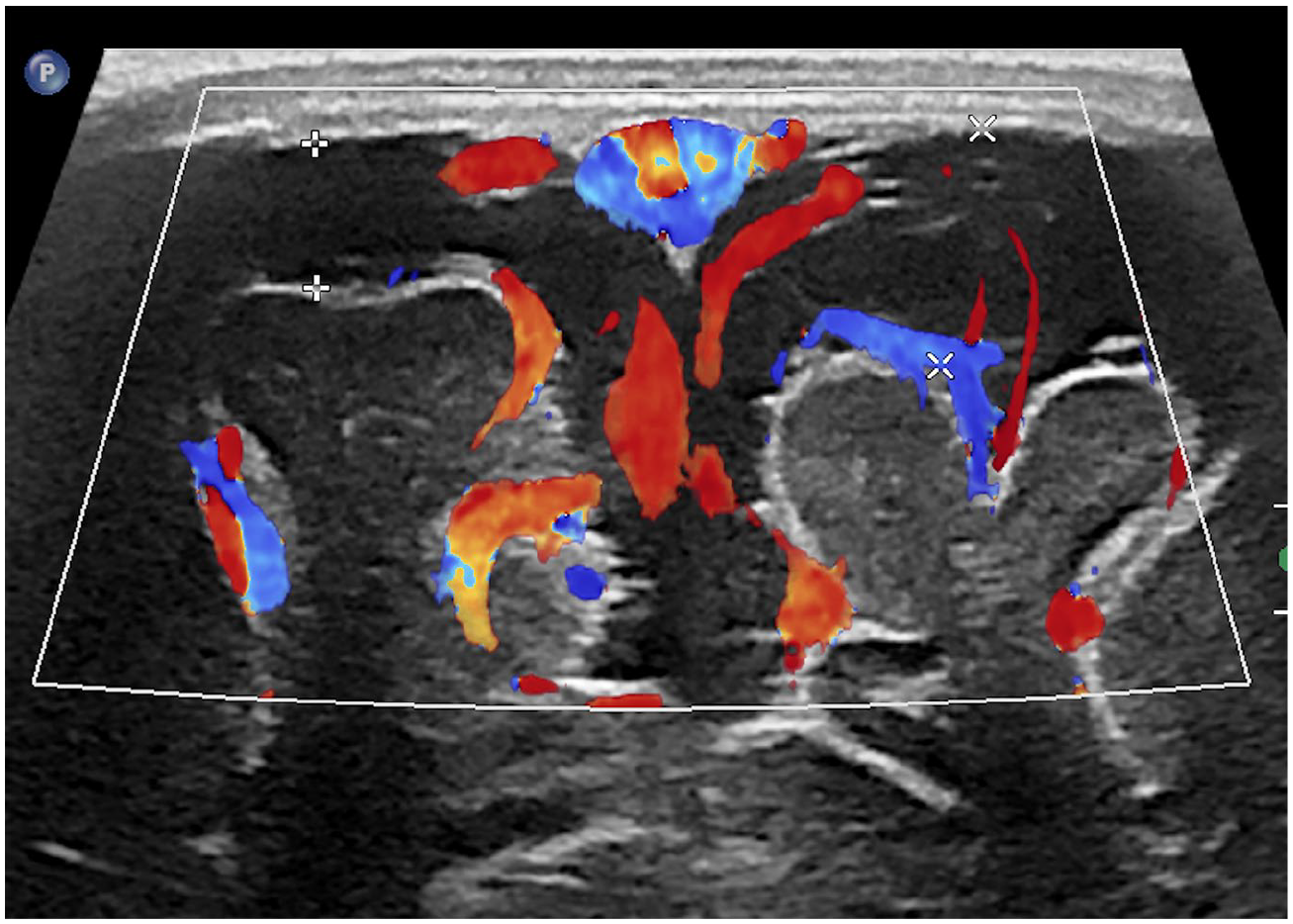
A 1-day-old female, born at 30 + 6 weeks of gestational age, with a vein of Galen malformation. Sagittal ultrasound image with a linear array transducer shows an enlarged vein of Galen, in keeping with aneurysmal malformation of the vein of Galen.
Specific Conditions
Summary
This article provides an in-depth evaluation of the role of neonatal neurosonography in diagnosing and managing brain pathologies. NSG is indispensable in the early diagnosis, treatment planning, and prognosis of neurological conditions in neonates and infants, especially in the NICU setting. Doppler ultrasound further enhances diagnostic capabilities by providing crucial insights into cerebral blood flow dynamics and guiding interventions in HIE, hydrocephalus, and other cerebrovascular disorders. Additionally, the use of transcranial Doppler for stroke risk assessment in children with sickle cell disease underscores the broader application of neurosonography in pediatric neuroimaging.
Supplemental Material
sj-tiff-1-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-1-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-10-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-10-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-11-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-11-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-12-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-12-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-13-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-13-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-14-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-14-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-15-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-15-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-16-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-16-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-2-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-2-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-3-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-3-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-4-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-4-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-5-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-5-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-6-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-6-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-7-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-7-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-8-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-8-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Supplemental Material
sj-tiff-9-caj-10.1177_08465371241308849 – Supplemental material for Pediatric Neurosonography: Comprehensive Review and Systematic Approach
Supplemental material, sj-tiff-9-caj-10.1177_08465371241308849 for Pediatric Neurosonography: Comprehensive Review and Systematic Approach by Neetika Gupta, Shivaprakash B. Hiremath, Isabelle Gauthier, Nagwa Wilson and Elka Miller in Canadian Association of Radiologists Journal
Footnotes
Acknowledgements
To the CAR-ASM 2024 team for inviting our work for submission in the CARJ.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.