
Abstract
Radiology is increasingly defined by interdependence: imaging value is created through tightly coupled relationships among radiologists, technologists, nurses, physicists, administrators, and referring clinicians, under escalating expectations for access, safety, quality, and timeliness. In this context, leadership is a department-wide capability that must be deliberately designed, taught, and sustained. Drawing on distributive leadership and servant leadership literatures, we propose a radiology-specific synthesis, that decentralizes problem-solving while maintaining accountability, and positions leaders as multipliers who build others’ competence, agency, and voice. We review why “heroic” leadership models predictably fail in complex adaptive clinical environments; summarize the empirical foundations of distributive and servant leadership; and translate these concepts into operational practices for radiology departments. This includes decision-rights design, meeting architecture, psychological safety, inclusive leadership, mentorship and sponsorship systems, and leadership development pathways for trainees and early-career faculty. We then examine 2 contemporary leadership stress tests: workforce sustainability (burnout, boreout, moral distress, hybrid work) and digital transformation (AI governance), arguing that both are best understood as organizational design challenges rather than individual resilience deficits or technology procurement exercises. Finally, we outline pragmatic metrics and evaluation approaches that align leadership behaviours with departmental outcomes (quality, access, safety culture, retention, and patient-centred value). A distributive servant leadership model offers a coherent, evidence-informed approach to building radiology departments that are adaptable, humane, and performance-oriented.
Introduction
Radiology’s clinical authority is grounded in interpretive expertise, and is delivered through coordinated systems and teamwork; including imaging pathways, protocols, safety processes, communication loops, and downstream clinical decisions that depend on collaboration across teams and disciplines.1,2 Accordingly, radiologists shape care through consultation, prioritization, escalation, quality oversight, and service design, activities that function as everyday leadership work.1-4 At the same time, radiology departments are navigating persistent demand growth, workforce constraints, and post-pandemic workflow redesign.5-9 These pressures create a predictable leadership risk: an understandable drift toward command-and-control problem-solving, where a small number of leaders absorb more decisions, crises, and emotional labour, while others become passive implementers.10-12 Over time, this pattern is associated with slower learning cycles, fragile morale, and “single points of failure” in governance and succession.10,12,13 The alternative is intentional distribution of leadership activities, supported by structures that make accountability explicit.10-13 This article advances a radiology-specific model, distributive servant leadership, that integrates: (i) distributive leadership’s emphasis on leadership as an emergent property of systems and teams, focused on “agile” goal-directed tasks, projects and programs, and (ii) servant leadership’s emphasis on leaders who elevate others’ growth, agency, and well-being as a route to sustained performance by enabling the development of each individual’s best self.10-17 The integration of distributive and servant leadership styles offers a practical and ethically coherent approach to modern radiology leadership, particularly when departments must deliver high performance without normalizing burnout.14-16,18-23
Leadership Versus Management in Radiology
Radiology departments require both management and leadership: operational reliability (staffing, scheduling, modality uptime, reporting queues) must coexist with adaptive change (redesigning pathways, addressing inequities, implementing new technology, building culture).1,2,24 Leadership literature distinguishes management as maintaining order and predictability, while leadership aligns people around purpose, enables sense-making, and mobilizes change in uncertain environments.25-27 In radiology, this distinction matters because many departmental challenges are adaptive rather than technical: they cannot be “solved” by expertise alone, and instead require new norms, shared ownership, and iterative learning.28-31 A practical implication is that radiology leaders should be evaluated not only on “snapshot” throughput metrics, budget adherence, or turnaround time, but also on their ability to build collective capacity over time, demonstrating consistent psychological safety, mentorship, cross-disciplinary collaboration, and distributed decision-making.32-36 These “soft” skills determine whether a department can learn and improve without exhausting its people.18-22,33-36
Leadership in Complex Clinical Systems: The Limits of the “Heroic” Model
Radiology departments behave as complex adaptive systems: multiple interacting agents adapt to changing constraints, and local decisions can produce unintended consequences across the system.28-31 In these environments, leadership is less about controlling outcomes and more about shaping conditions, such as information flow, feedback loops, decision rights, and learning mechanisms, so that teams can adapt safely and coherently.28-31,37
Distributive leadership literature critiques the “heroic leader” assumption, the “genius with a thousand helpers” myth that describes a leadership model where a department or organization depends heavily on one exceptionally talented leader (the “genius”), while everyone else mainly implements the genius’s ideas. 38 Empirically, complex organizations rarely function this way; leadership work is distributed across roles and situations, and outcomes depend on how leadership is enacted collectively.10-13 For radiology departments, the “heroic” framing is especially hazardous because it concentrates responsibility for systemic problems (access, staffing, burnout, technology change) onto a few people, limiting sustainability and often normalizing unsustainable work patterns.18-22 Servant leadership, on the other hand, offers a reframing, treating leadership as an obligation to build others’ capacity, which is simultaneously a performance strategy and a well-being strategy.14-17 Distributive and servant leadership models also contrast transactional leadership, which focuses on exchanges of reward or punishment, or authoritarian leadership, which consolidates power to a single individual. Unlike these frameworks, distributive and servant leadership foster inclusivity, sustainability, and creativity, qualities that align closely with the mission of radiology to provide compassionate care, innovate academically, and sustain collaborative cultures.12,15 Because the servant leadership model builds a strong leadership bench, engaging people at many levels to contribute ideas, departments of radiology aligning with this leadership framework continue thriving after leadership transitions.
Distributive Leadership: Evidence Base and Relevance to Radiology
Distributive leadership is not synonymous with position. It encompasses a set of activities: sense-making, direction-setting, coordinating, and enabling, that can be enacted by multiple people across a system.10-13 Harris’ synthesis of evidence highlights distributive leadership as particularly relevant in knowledge-intensive environments where expertise is dispersed, tasks are interdependent, and outcomes depend on coordinated professional judgement. 11 Bolden’s review similarly describes distributive leadership as an approach that foregrounds collective agency, emergent coordination, and context-specific leadership practices rather than universal leader traits. 12
Radiology matches these conditions closely. Subspecialty expertise is distributed (eg, neuroradiology, musculoskeletal, body, breast, pediatrics, interventional radiology), operational expertise is distributed (Picture Archiving and Communication Systems [PACS], informatics, modality operations), and safety expertise is distributed (MR safety, radiation safety, contrast safety).1-3,24,39,40 When leadership is centralized, decisions often lag behind frontline reality; when leadership is distributed without structure, accountability becomes ambiguous.10-13 Therefore, distributive leadership in radiology must be paired with explicit design of decision rights, escalation pathways, and performance feedback.1,2,4,10-13,39,40 In radiology, distributive leadership may mean residents leading teaching rounds, technologists shaping workflow protocols, or subspecialists taking responsibility for strategic initiatives such as artificial intelligence, or equity, diversity, and inclusion. By redistributing leadership functions, departments can benefit from diverse expertise and cultivate cultures of trust and innovation.
Distributive leadership also has implications for training. Radiology residency historically emphasizes interpretive mastery; leadership capacity (meeting facilitation, negotiation, improvement science, conflict management) is often implicit rather than taught.41-43 Reviews of leadership development offerings across radiology residencies show variability in formal leadership education programs, and an opportunity to formalize curricula and experiential pathways to enable the development of leadership traits as part of required non-interpretative skills. 42
Servant Leadership: Empirical Foundations and Radiology-Specific Value
Servant leadership originates from Greenleaf’s proposition that leaders should first seek to serve, prioritizing others’ growth, autonomy, and well-being, while maintaining high standards and organizational purpose. 17 Contemporary empirical work operationalizes servant leadership as a measurable construct associated with trust, engagement, and team performance.14-16 Liden et al developed and validated a multidimensional servant leadership measure, anchoring the model in observable behaviours. 16 Subsequent systematic reviews and meta-analytic syntheses describe servant leadership as associated with employee well-being, organizational commitment, and performance outcomes, while also acknowledging heterogeneity across contexts and measurement approaches.14,15
For radiology, servant leadership is a strategy for building sustainable performance under constraints.18-22 A servant leader in radiology mentors junior staff, advocates for work-life balance among allied professionals (including technologists, nurses, and clerks) and ensures all radiologists have the tools they need to provide excellent patient care. Servant leaders also model humility by crediting others for success, taking responsibility for setbacks, and protecting junior faculty during difficult reviews, while simultaneously promoting their work in national and international forums. Radiology departments also depend on discretionary effort from all radiologists for teaching, protocol optimization, peer learning, quality improvement, and collaboration, which are not fully captured by productivity metrics, yet they determine clinical value.1-3,24,33-36 Servant leadership supports these “invisible” contributions by making capability building an explicit leadership responsibility.14-16 Servant leadership also aligns with patient-centred professionalism. When leaders cultivate environments where everyone in the department can raise safety concerns, where trainees, technologists, nurses, and radiologists feel comfortable disclosing uncertainty and challenging unsafe workflows without fear of reprisals, patient outcomes tend to improve through earlier detection of system risks.33-36,39,40
Meeting the Needs of Radiologists
In service-oriented specialties, such as radiology, addressing the spectrum of employee needs is critical for engagement and retention. Basic needs include fair compensation, predictable schedules, career security, and psychological safety. Once these are met, higher-order needs such as meaningfulness, personal growth, belonging, achievement, and recognition become central motivators. 44 Servant leadership supports these higher-order needs through empathy and mentorship, while distributive leadership provides opportunities for team members to contribute meaningfully to decisions and innovations. Together, these models create environments where individuals are both supported, and empowered.
Integrating the Models: Defining “Distributive Servant Leadership” in Radiology
Distributive leadership provides the structural logic (“leadership is shared and enacted across the system”), while servant leadership provides the ethical and developmental logic (“leaders exist to grow others and create conditions for excellence”).10-17 We define distributive servant leadership in radiology as:
Shared leadership activity across roles and levels, deliberately designed rather than informally assumed
High-accountability decentralization, where decision rights are explicit and aligned with expertise
Multiplying capability, where leaders systematically build others’ competence, confidence, and voice
Culture as infrastructure, emphasizing psychological safety, inclusion, and learning as performance prerequisites
This synthesis also clarifies a common misconception: distributive leadership does not always mean equal influence, it means leadership is situationally allocated to those with the most relevant expertise and proximity to the problem, within governance structures that maintain coherence and accountability.10-13 Similarly, servant leadership does not mean avoidance of conflict or lowered standards; it means standards are pursued through developing people rather than extracting unsustainable effort.14-17
Operationalizing Distributive Servant Leadership: Structures, Processes, and Behaviours
Decision-Rights Design: Who Decides What, and How Escalation Works
Radiology departments often rely on informal influence networks: certain individuals become default decision-makers for protocol disputes, workflow issues, or quality concerns. This is efficient in the short-term, but creates fragility over time. A distributive servant approach makes decision rights explicit: routine operational decisions should sit close to the work (eg, protocol optimization led by modality and subspecialty experts), while strategic decisions require structured deliberation and transparent rationale.1,2,4,33-36,39,40 Pragmatically, this can be implemented through “decision maps” that distinguish decisions that are delegated, decisions that require consultation, decisions reserved for leadership, and decisions that require formal committee approval. In radiology, this reduces ambiguity in common friction points: add-on imaging requests, protocol deviations, contrast policy exceptions, and communication standards.
Meeting Architecture as Leadership Infrastructure
Many radiology departments treat meetings as information broadcasts. A distributive servant model treats meetings as a key mechanism for distributed sense-making and learning. High-performing meeting systems include cognitively diverse stakeholders, clarify purpose of tasks (decision, coordination, learning), define pre-read expectations, and document decisions and follow-up owners. 45 This model also mitigates the common leadership failure mode where decisions are repeatedly revisited because rationales were never recorded, or because diverse knowledgeable stakeholders were not included, which emphasizes the importance of cognitive diversity in team meetings.
Communication and “Visibility Work” in Radiology
Radiologists can have limited operational visibility when reporting work is physically and cognitively separated from clinical teams, a challenge magnified by remote and hybrid models.6-9 Leadership therefore includes “visibility work”: structured consult pathways, multidisciplinary rounds, and reliable critical results’ processes that make radiology’s clinical contributions legible to patients and colleagues. Remote work guidance in academic radiology emphasizes that hybrid arrangements require intentional design to preserve teaching, mentorship, collaboration, and clinician relationships.6-9
Conflict as Data: Building Capacity for Respectful Disagreement
Radiology leadership routinely involves conflicts about appropriateness, resource allocation, and clinical uncertainty.46-48 Treating conflict as personal failure leads to avoidance, whereas treating it as information enables improvement. Servant leadership supports conflict competence by coaching people in structured disagreement (clarifying shared goals, separating interests from positions, using data where possible, and documenting decisions). 49 Distributive leadership strengthens this by ensuring conflicts are resolved at the appropriate level; close enough to the work to be informed, but within escalation structures that prevent unsafe local variation.
Psychological Safety and Inclusive Leadership as Performance Prerequisites
Psychological safety, the shared belief that a team is safe for interpersonal risk-taking, is strongly associated with improved learning behaviours, reduced reporting error, improved quality of delivery of services, and promotion of innovation.36,50,51 In healthcare teams, leader inclusiveness fosters psychological safety and strengthens improvement efforts, particularly in environments where status differences might otherwise silence junior team members or non-physician voices. 35 Radiology-specific guidance on inclusive leadership emphasizes concrete behaviours: inviting participation, crediting others’ contributions, addressing bias and microaggressions, and building structures that support belonging and retention.33,34 Inclusive leadership is therefore a mechanism that improves diagnostic and operational reliability by ensuring that concerns surface early and that diverse expertise is heard. This is especially relevant in radiology, where technologists and nurses often detect workflow hazards (eg, patient identity mismatch, contrast contraindications, MRI safety risks) before radiologists do.39,40
Building the Leadership Pipeline: Mentorship, Sponsorship, and Formal Development
Radiology leadership cannot always depend on “finding” natural leaders; departments must build leadership capacity systematically. Mentorship literature in academic medicine shows benefits for career satisfaction, productivity, and retention, while also emphasizing that mentorship quality and access are uneven.52,53 Radiology-specific mentorship literature describes mentorship as both a career development mechanism and a departmental strategy for succession planning. 53 However, mentorship alone cannot overcome structural barriers to career advancement. Sponsorship and active advocacy from senior leaders for junior radiologists and trainees are also critical, particularly in promoting equity and inclusion.54,55 In radiology, this includes ensuring equitable access to professional visibility opportunities (committee roles, invited talks, leadership development programs) and making selection processes transparent.32-34
Leadership development programs within radiology have been described at multiple levels, including residency-focused curricula and executive development initiatives.41-43 Reviews of radiology residency leadership training highlight variability and support the argument for a more deliberate approach that integrates didactics with experiential leadership practice, the “mind and hand” concept, which expresses the concept that knowledge (mind) should be combined with practical application (hand). 56 This concept is applicable to project leadership, committee chairing, and negotiated change.42,57 Radiology leadership scholarship also underscores that leadership development is most effective when tied to real departmental priorities (quality improvement initiatives, access redesign, patient safety) rather than generic leadership content.41,43
Leaders can maximize the potential of their workforce by fostering continuous professional improvement, ensuring emotional and moral safety through inclusive policies, and sponsoring colleagues for new opportunities. An important concept here is the “multiplier,” a leader who amplifies the talents of others, encouraging creativity, trust, and innovation. 58 In radiology, multipliers create teams that think broadly, act collaboratively, and generate solutions that extend beyond the abilities of any single individual. Servant and distributive leadership naturally embody this approach by creating conditions where all voices are heard and all contributions are valued.
Leading Change in Radiology: From Frameworks to Execution
Radiology departments change constantly. These continuous changes relate to protocols, technology, staffing models, reporting standards, and cross-departmental pathways. However, change efforts often fail for predictable reasons: unclear urgency, insufficient coalition building, lack of communication, and failure to consolidate gains.27,59 Kotter’s classic change framework remains relevant as a heuristic for these failure modes. 27 Implementation science offers additional tools for healthcare change. 60 The Consolidated Framework for Implementation Research (CFIR) supports structured assessment of intervention characteristics, inner and outer setting influences, individual characteristics, and process factors that shape implementation. 30 The Knowledge-to-Action (KTA) framework similarly provides a pragmatic map from evidence to sustained practice. 29 For radiology leaders, these frameworks can prevent a common error: assuming that selecting the “right” intervention is equivalent to implementing it.29,30,60
Quality improvement (QI) scholarship in radiology provides concrete examples of how leadership, measurement, and iterative learning produce system gains. Radiographics and AJR primers describe how radiology departments can establish comprehensive QI programs, apply Lean methods, and use process improvement tools in routine operational redesign.1,2,4,39,40,61-67 Systematic reviews of Lean and Six Sigma in radiology suggest potential benefits while calling for methodological rigour and context-sensitive implementation, an argument consistent with CFIR/KTA insights. 61 In practice, distributive servant leadership aligns with QI because it treats frontline expertise as central, builds shared ownership, and creates learning loops rather than compliance rituals.
Workforce Sustainability as a Leadership Mandate: Burnout, Boreout, Moral Distress, and Hybrid Work
Burnout is Not an Individual Weakness Problem
Physician burnout is prevalent and associated with adverse outcomes for clinicians and systems.21,23 Meta-analytic work estimates substantial burnout prevalence among physicians, with heterogeneity by specialty and setting. 23 Interventions exist, but organizational strategies tend to have larger, and more durable effects than individual-focused approaches alone. 21 Importantly, executive and local leadership behaviours are strongly implicated in clinician well-being; leadership is therefore causally relevant for burnout. 22
Radiology-specific scholarship has explicitly argued that leaders can both cause and cure burnout, particularly through controllable drivers such as workload design, autonomy, fairness, recognition, and the integrity of professional values. 18 This framing is important because departments sometimes respond to distress with resilience programming while leaving structural drivers unchanged.18-22 A distributive servant model instead emphasizes structural prevention: designing work so that excellence is achievable without chronic depletion. Another concerning effect of hierarchical non-distributive leadership is “boreout,” which relates to demotivation, disengagement, and reduced well-being caused by lack of meaningful work and under-utilization of the individual’s talents and skills.68,69 In radiology departments, boreout is observed when trainees or physicians at different career levels are not empowered to contribute ideas, or present their own work to senior leadership of the healthcare institution, technologists or nurses are excluded from decision-making, and highly trained professionals perform low-complexity tasks, without discussions about career path and promotions.
Moral Distress and Moral Injury in Radiology
Burnout frameworks alone can miss an increasingly salient phenomenon: moral distress, when clinicians know the ethically appropriate action, but feel constrained from taking it; and moral injury, when clinicians feel they have participated in, witnessed, or been unable to prevent actions that violate deeply held values.19,20 Radiology has unique moral distress triggers, including pressure for throughput over deliberation, resource rationing affecting access, and misalignment between operational targets and patient-centred care.20,70,71 Several radiology commentaries have argued for institutional and departmental countermeasures, including governance reforms, staffing strategies, and deliberate ethics-informed leadership practices.67,70 A distributive servant leadership approach addresses moral distress by changing the system conditions that generate it: improving voice and escalation pathways, clarifying accountability for unsafe constraints, and building forums where clinicians can name and resolve value conflicts rather than privately absorbing them.
Hybrid and Remote Work: A Leadership Design Problem, Not a Perk Negotiation
Remote and hybrid radiology work is now part of the workforce landscape, with both benefits and risks.6-9 Academic radiology guidance describes advantages (flexibility, recruitment, autonomy) and disadvantages (reduced visibility, weakened mentoring, decreased informal collaboration), emphasizing that hybrid success depends on intentional departmental design. 6 Expert panel guidance for remote academic radiologists similarly highlights the need for governance, communication norms, equitable policies, and protected teaching/mentorship structures. 7 Survey work in academic radiology suggests that remote and flexible work options are common and perceived to improve well-being, with implications for retention and diversity. 8 Distributive servant leadership is well matched to hybrid work because it explicitly invests in relational infrastructure: it builds predictable touchpoints, preserves teaching as a departmental commitment, and avoids creating “two-tier” cultures in which on-site work is equated with commitment and recognition, while remote work is equated with disengagement and less valuable contribution.
Level 5 and 4-CAP+: A Practical Radiology Leadership Toolkit
Collin’s hierarchy of leadership emphasizes Level 5 leaders, who combine humility with determination, and channel ambition into organizational success, rather than personal success. 38 Such leaders resonate with servant leadership’s ethos of service and sustainability, as they build strong teams of capable leaders and create systems and culture that endure. The 4-CAP+ model developed at MIT further outlines essential skills for leadership today: sensemaking, visioning, relating, and inventing. 72 For radiology leaders, sensemaking requires interpreting challenges such as the COVID-19 pandemic with clarity, and prioritizing safety. Relating involves active listening and building trust across professional groups. Visioning means developing collective goals rooted in shared values, while inventing entails designing new processes and structures to achieve those goals. These skills must be combined with agility to adapt to rapidly changing imaging technologies, openness to collaboration, and the discipline to execute plans effectively. Together, they offer a practical framework for how distributive and servant leadership can be enacted in daily departmental practice.
Digital Transformation as a Leadership Stress Test: AI Governance as an Organizational Capability
AI governance illustrates why distributive servant leadership is increasingly necessary. AI implementation is a socio-technical change that affects workflow, accountability, risk, equity, and professional identity.73-75 Radiology societies have emphasized the need for clear frameworks and standards for AI evaluation, validation, monitoring, and regulation.73,76 The 2018 Canadian Association of Radiologists’ white paper on AI articulated early governance priorities relevant to Canadian practice, including safety, ethics, and workforce implications. 76 Broader radiology guidance outlines infrastructure and governance requirements for clinical AI implementation and emphasizes monitoring and lifecycle management rather than one-time deployment. 73 AI governance also demands multi-stakeholder participation: radiologists, technologists, informaticians, physicists, data scientists, administrators, and equity and ethics expertise. 77 This requirement is structurally aligned with distributive leadership: expertise is dispersed, and safe adoption depends on coordinated action across the system. Servant leadership adds a necessary ethical anchor: leaders must ensure that AI integration does not externalize risk onto frontline clinicians, worsen inequities, or increase cognitive burden through poorly designed workflow integration. AI governance also intersects directly with burnout and moral distress. Poorly governed tools can increase alert fatigue, undermine trust, and create new liability anxieties; well-governed tools can reduce friction and support clinical decision-making. Leadership therefore determines whether AI becomes a net burden or a net benefit, less through technical sophistication than through governance maturity.
Measuring Leadership: Aligning Behaviours With Radiology Outcomes
The performance metrics of a leader in a department of radiology is directly related to departmental outcomes’ metrics. Radiology QI literature provides an example of effective measurement approaches: it demonstrates how structured measurement supports sustained improvement in safety, communication, efficiency, and patient experience.1,2,4,39,40,61-63,78 Leadership evaluation can borrow this orientation by defining a small set of metrics aligned with distributive servant priorities, such as:
Safety culture indicators (incident reporting volume and closure quality; psychological safety climate measures)
Workforce accrual and sustainability (recruitment and retention of best talent, sick time, engagement, moral distress screening)
Learning system performance (QI project throughput, time-to-implementation, adherence to feedback loops)
Equity and inclusion (leadership pipeline diversity, sponsorship access, differential attrition)
Clinical performance (critical results communication reliability, appropriateness and protocol adherence, turnaround time without sacrificing quality of services)
Leadership should be treated as a clinical-quality capability: it should be designed, taught, measured, and improved according to Plan, Do, Study, Act (PDSA) frameworks that use specific methods for quality improvement and continuous learning in complex systems.37,79 PDSA frameworks are central to quality improvement in a department of radiology because they encourage small, rapid tests of change; promote data-driven decisions; reduce risk before large-scale implementation, and supports learning organizations.
Practical Synthesis: What Distributive Servant Leadership is About on the Daily Routine of a Radiologist
A recurring barrier to leadership scholarship in radiology is translation: readers may agree with principles, yet struggle to see what changes on the next Monday morning. In practical terms, distributive servant leadership changes 4 things. First, it reallocates decision-making closer to expertise and to the end-user which includes multidisciplinary teams and patients, with explicit escalation rules, reducing bottlenecks and protecting leaders from becoming single points of failure. Second, it invests in people development as a performance strategy; mentorship, sponsorship, leadership training, and meaningful roles for trainees and early-career faculty. Third, it treats culture as part of a multi-lens approach which includes strategy, culture, and politics, using inclusive leadership and psychological safety practices to improve learning, safety, and retention. Fourth, it recognizes that modern radiology leadership must actively design for inclusivity and sustainability, addressing burnout, boreout, and moral distress through structural interventions, assessed on a periodic basis, and designing hybrid work models that preserve collaboration and teaching. Notably, this is compatible with high standards. Servant leadership requires making excellence achievable through systems that develop capability rather than extracting sacrifice.
Reflection and Career Alignment
Reflection exercises help professionals clarify their values, strengths, and transferrable skills, while career planning ensures that personal goals remain aligned with institutional missions. The model depicted in Figure 1, adapted from career alignment frameworks integrating strengths, interests, and organizational needs, 80 can be used by leaders to guide colleagues toward sustainable career pathways, integrating servant leadership’s attentiveness to individual development with distributive leadership’s commitment to shared responsibility.81,82
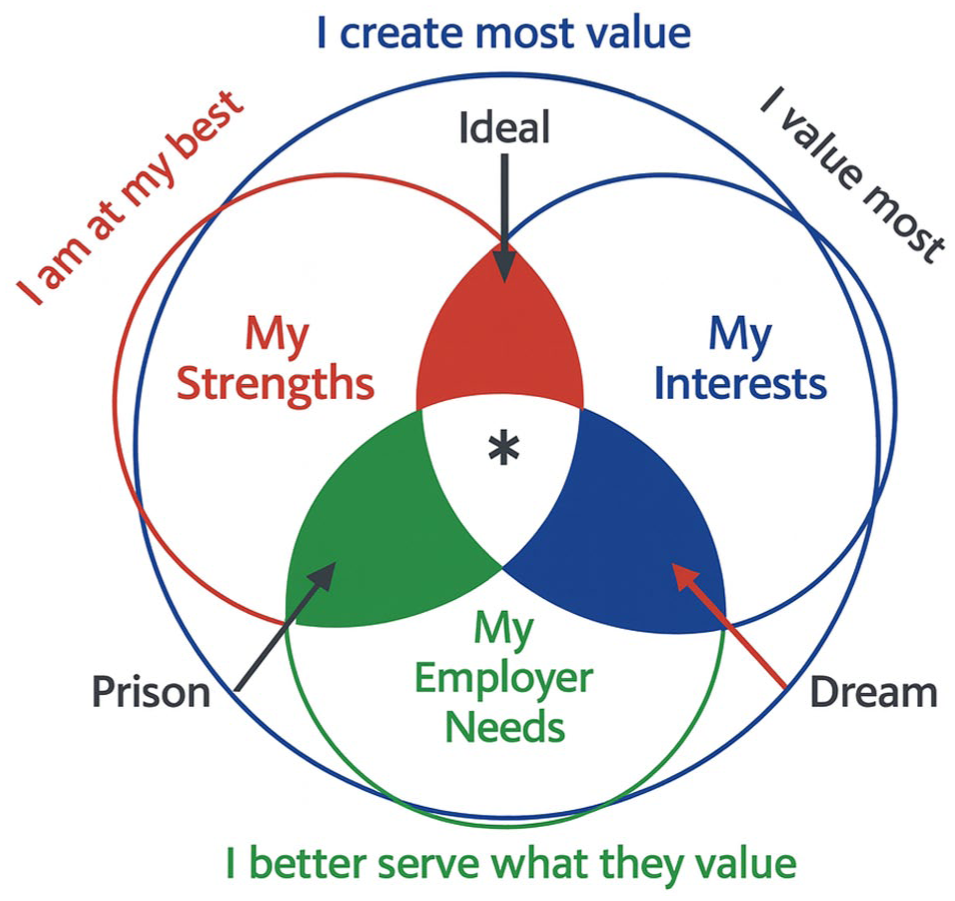
Conceptual model of career alignment at the intersection of strengths, interests, and organizational needs.
Leadership and Legacy
Strong leadership in radiology requires the ability to inspire, empower, and to sustain. Servant and distributive leadership combines visionary thinking with empathy and freedom of verbalization of innovative thoughts that challenge the “status quo” of the organization, humility with courage and determination, and service with inclusivity and accountability. This fosters cultures of innovation and continuous improvement, ensuring that teams feel supported and that departments remain resilient in the face of change. A leader everyone values is one who cultivates learning, balances individual satisfaction with organizational performance, and creates an environment where future leaders can thrive. This legacy, rooted in servant and distributive leadership, has the potential to transform radiology into a specialty defined by clinical and scientific excellence on top of the strength and sustainability of its leadership culture.
Conclusion
Radiology departments face a leadership challenge that is both practical and moral: to deliver reliable, high-quality imaging under real constraints without normalizing harm to the workforce. Distributive leadership offers a structurally realistic view of how leadership actually operates in complex organizations, while servant leadership provides an ethically coherent and empirically supported approach to building sustainable performance through developing others. A distributive servant leadership model integrates these traditions into a radiology-specific strategy: decentralize leadership activities with accountability, multiply capability through mentorship and sponsorship, build inclusive psychologically safe cultures, and approach burnout, boreout, moral distress, hybrid work, and AI governance as organizational design problems. For radiology, leadership is a core clinical competency that determines whether departments remain adaptable, humane, and excellent.
Footnotes
Author Contributions
RK and ASD were involved with conceptualizing the study. ASD wrote the initial draft of the manuscript. RK wrote further iterations of the manuscript. RK, MP, MC, and ASD were involved with critical revision of the manuscript. All authors approved the submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Doria is the Principal Investigator of research grants unrelated to the current study, respectively from Terry Fox Foundation, PSI Foundation, Society of Pediatric Radiology, Radiological Society of North America, CARRA Foundation, and Novonordisk Access to Insight Grant.