
Abstract
Radiology departments are increasingly tasked with managing growing demands on services including long waitlists for scanning and interventional procedures, human health resource shortages, equipment needs, and challenges incorporating advanced imaging solutions. The burden of system inefficiencies and the overuse of “low-value” imaging causes downstream impact on patients at the individual level, the economy and healthcare system at the societal level, and planetary health at an overarching level. Low value imaging includes those performed for an inappropriate clinical indication, with little to no value to the management of the patient, and resulting in healthcare resource waste; it is estimated that up to a quarter of advanced imaging studies in Canada meet this criterion. Strategies to reduce low-value imaging include the development and use of referral guidelines, use of appropriateness criteria, optimization of existing protocols, and integration of clinical decision support tools into the ordering provider’s workflow. Additional means of optimizing system efficiency such as centralized intake models, improved access to electronic medical records and outside imaging, enhanced communication with patients and referrers, and the utilization of artificial intelligence will further increase the value of radiology provided to patients and care providers.
This is a visual representation of the abstract.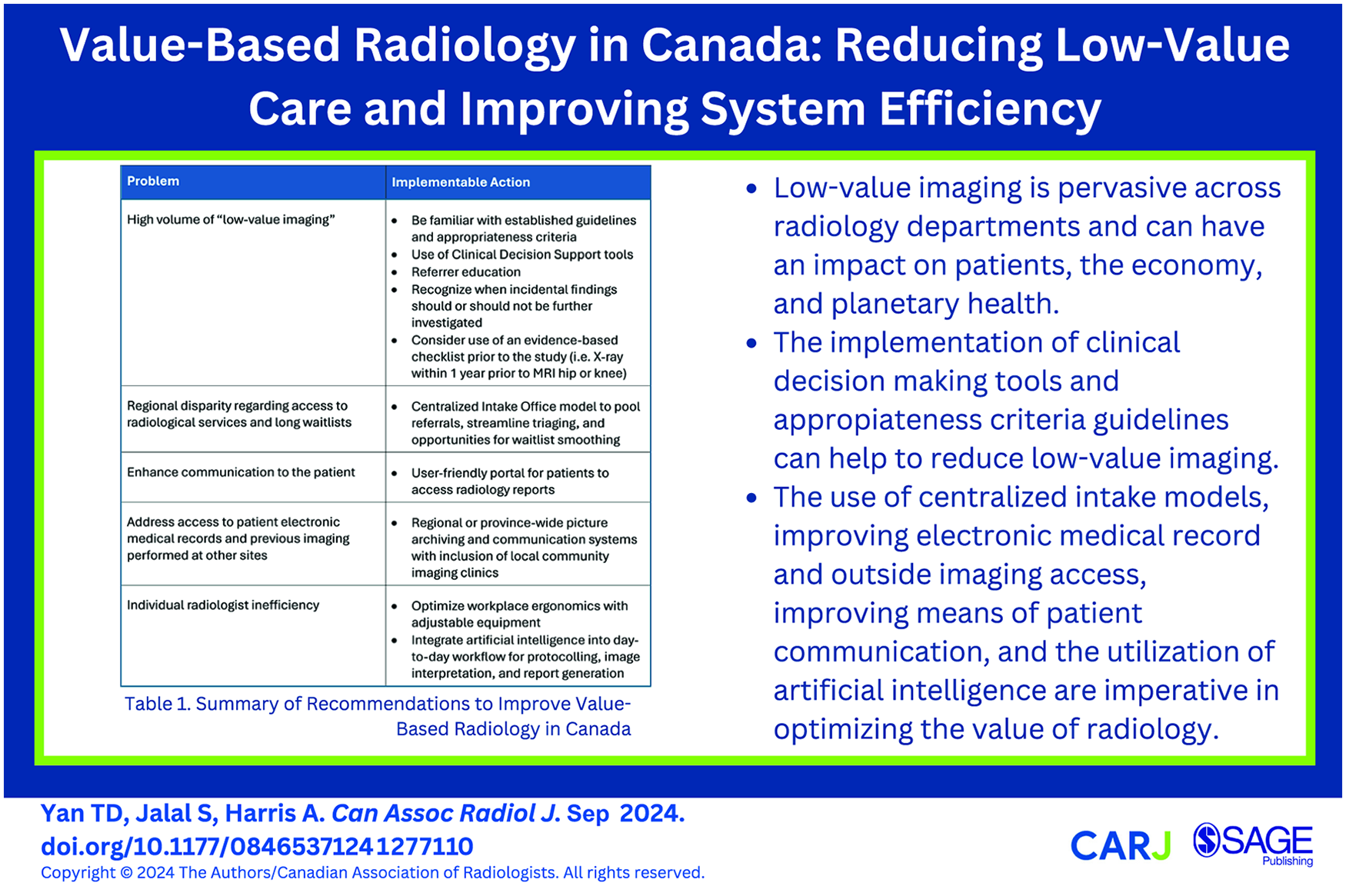
Introduction
The concept of Value-Based Radiology (VBR) has emerged as a shift in the perspective of radiology departments toward delivering high-value care centric to the patient, rather than the historical focus primarily on volume. 1 First described in 2010, economist Michael Porter introduced the notion of Value-Based Healthcare in which value is determined by patient health outcomes per unit of expenditure. 2 As highlighted in a recent multi-society expert statement, the provision of radiology services has the potential to be a significant driver of patient value, rather than the extreme interpretation of radiology as a “cost center.” 3 It is critical to note that medical imaging brings value to all facets of healthcare delivery, from prevention and detection, to diagnosis, delivery and monitoring of therapy, and prognosis, amongst other areas. 4 In 2017, the Conference Board of Canada published their first report on the Value of Radiology, underscoring the pivotal role played by Canada’s radiology sector—for example, in screening and early detection—and its contributions to Canada’s broader healthcare system and economy. 5 In the case of screening, the early detection of breast cancer through mammography decreases the cost of treatment and productivity losses as the economic burden of disease is greater in later-stage disease. 5 For instance, for Stage IV breast cancer the average cumulative cost in Canada (accounting for inflation at the time of 2016) was $53 419 compared to $34 214 for Stage I disease. 6 Recent Canadian research presented at a 2024 Breast Cancer conference found that if screening for breast cancer was made earlier starting at age 40 years, the Canadian healthcare system would save $459.6 million with 3499 breast cancer deaths averted. 7
Consequently, when components of the radiology system are delayed or falter, the resulting impact is detrimental to individuals, their families, and at a societal level. In their subsequent 2019 report, The Value of Radiology Part II, the Conference Board of Canada outlined the economic impact of excessive wait times for cross-sectional imaging including computed tomography (CT) and magnetic resonance imaging (MRI). 8 In 2017 alone, the excessive wait times for CT and MRI examinations were estimated to cost the Canadian economy $3.54 billion. By analyzing historical trends, as well as considering the aging population and evolving medical practices, this issue is expected to be further exacerbated by the projected increased imaging volume in future years: the number of CT examinations are forecasted to more than double from 5.6 million in 2017 to 11.9 million in 2040, coupled with an even further growth in MRI examinations from 1.9 million to 5.3 million in the same time frame. As such, it is vitally important for radiology to explore initiatives to mitigate the growing strain on our system. This paper aims to review the current landscape of VBR in Canada, with a particular focus on reducing low-value imaging and highlighting other means of optimizing system efficiencies. The need for research ethics board review was waived as the manuscript reviews existing literature without the direct involvement of human or animal subjects.
Reducing Low-Value Imaging
A discussion of value—and by virtue, imaging deemed to be “low-value”—must first be preceded by how value is measured. Traditional metrics have focused on process or volume-based measurements, however, there is now a paradigm shift toward outcome measures that show value. 9 For example, in the case of a liver biopsy, traditional process metrics would pertain to the number of biopsy passes, room turnover time, or needle size. Alternatively, outcome and value measures would include customer (patient) satisfaction, impact on hospital length of stay and treatment, and change in diagnosis. This would align with how patients themselves identify high-value radiological care. A survey by the European Society of Radiology (ESR) of patients across 22 countries found that communication, efficiency (ie, optimizing wait times and time-to-diagnosis), diagnostic accuracy, and appropriateness of the scan performed are the hallmarks of a valuable radiology service. 10
Accordingly, assuring appropriateness of the scan performed is a critical aspect of VBR. A group from Norway has been leading this area of investigation, having conducted a scoping review of over 370 studies to identify a comprehensive list of 84 radiological examinations that would be considered “low-value.” 11 At the forefront of this list: imaging for atraumatic pain, routine imaging in minor head injury, fracture follow-up, and some cancer follow-up studies. 11 The same group has conducted a systematic review on the global economic cost of low-value imaging, unsurprisingly reporting that it could amount to billions of US dollars per year. 12 106 studies were included in their systematic review, the majority (66%) conducted in the United States, 16% conducted in European countries, and 7% conducted in Canada. 12 There was a diversity of clinical practices deemed to be “low-value” which were studied, ranging from routine post-operative radiographs to inappropriately indicated musculoskeletal MRIs. 12 The authors reported the potential annual cost savings for each low-value practice, including over $120 000 saved each year from avoiding duplicate trauma imaging, or over $204 000 saved from avoiding inappropriately indicated head CTs. 12 Another systematic review identified interventions and their outcomes in reducing low-value imaging. 13 The 2 most common interventions included clinical practice guidelines and education. 13
In the United States (US), the Choosing Wisely (CW) initiative was launched by the American Board of Internal Medicine Foundation in 2012 and developed to address the perceived over-ordering and inappropriate use of tests and treatments. The CW initiative identified 103 high-volume imaging examinations determined to be “low-value,” recognizing the potential to reduce waste and ensure appropriate testing. 14 More recently, the American College of Radiology (ACR) has spearheaded the drive to reduce low-value imaging through their Imaging 3.0 initiative. 15 Part of these efforts includes the ACR Appropriateness Criteria, a set of evidence-based clinical practice guidelines currently comprised of 239 topics geared toward the most efficient use of medical imaging. An example case study from Colorado demonstrates how the ACR Appropriateness Criteria can be successfully integrated into a point-of-care clinical decision support (CDS) tool, leading to an increase in appropriately ordered imaging from 77% to 80% over a period of just 10 months—a small but significant difference. 16 In the short implementation period, they also found that there was a decrease in change orders (changing the original order to another imaging study). 16
Similarly, CW Canada aims to reduce unnecessary tests and treatments in Canada. The Canadian Association of Radiologists (CAR) endorses their top 5 recommendations to reduce low-value imaging for specific clinical scenarios (in the absence of red flags) including lower back pain, minor head injury, uncomplicated headache, CT as first-line for paediatric appendicitis, and ankle X-ray series in adults for minor injuries. Moreover, the CAR has created, and continues to develop, its own referral guidelines with 7 updated sections published at this time on areas such as trauma, breast disease, and obstetrics and gynaecology.17-23 Referral guidelines are developed with an interdisciplinary expert panel including radiologists, subspecialty clinicians, patient advisors, and epidemiologists/guideline methodologists to optimize high-value imaging for common clinical scenarios encountered in each body system or topic.17-23 An eventual goal for the CAR referral guidelines is for their incorporation into a CDS system and integrated at the point of ordering into electronic medical records. While not yet widely used in Canada, several hospitals in Ontario are linked to a system which provides a CDS tool for ordering physicians based on the Royal College of Radiologist’s referral guidelines. 24 Further research is needed to evaluate the impact of CDS tools on improving the utilization of CT and other imaging modalities, although these ongoing efforts and contributions highlight Canada’s commitment toward VBR. 25
Within individual provinces clinical referral guidelines may vary slightly, but the overarching theme of optimizing high-value radiological care is maintained. In British Columbia (BC), the website BCGuidelines.ca has published over 50 evidence-based guidelines on various clinical scenarios including several focused on medical imaging. 26 In the guideline “Appropriate Imaging for Common Situations in Primary and Emergency Care,” recommendations include: not performing CT for pulmonary embolism in low-risk, non-pregnant adults, and not performing MRI for hip and knee pain in adults if degenerative changes are seen on a recent X-ray. The latter recommendation stems from Canadian research showing that 21% of hip and knee MRI requisitions could be avoided by evaluating an X-ray from within a year for findings of severe osteoarthritis, which if extrapolated to all of BC at the time of study in 2020, would amount to 2419 of 11 700 MRI examinations. 27 In Saskatchewan, a combined checklist with evidence-based indications for MRI and CT of the lumbar spine for low back pain was developed for use in one of the former health regions (Five Hills) beginning in May 2018. 28 The monthly number of pre and post checklist implementation MRI and CT lumbar spine referrals were compared to a nearby former health region in which the checklist was not used. 28 A shift (decrease, −16%) was observed in the monthly number of MRI lumbar spine requisitions in Five Hills following implementation of the checklist with an increase (+7%) in the adjacent region. The combined checklist (for MRI and CT) decreased complexity associated with 2 prior checklists and facilitated ordering appropriateness. 28
When low-value imaging is reduced, the impact can be felt beyond that of the initial, more obvious economic considerations. Canadian studies have suggested that 2% to 24% of advanced imaging studies may be “inappropriate.”29,30 This can lead to consequences such as emergency departments becoming congested, waitlists for needed imaging examinations lengthening, patients incurring unnecessary radiation exposure, false positives potentially resulting in psychological and physical harm, and further testing for incidental findings.31,32 Practice guidelines set out by groups such as the CAR and ACR outline recommendations for the further work-up of incidental findings. An example is the ACR White Paper on Managing Incidental Thyroid Nodules Detected on Imaging. 33 In the ACR guidelines, incidental thyroid nodules of certain size and radiographic characteristics in differing age groups may not require further evaluation—for example, an incidental nodule found on CT or MRI without suspicious features that measures less than 1.5 cm in a patient 35 years or older does not require a thyroid ultrasound. 33 An example guideline from the CAR is the Recommendations for the Management of Incidental Musculoskeletal Findings on MRI and CT, which describe how to deal with incidental findings such as focal bone lesions, marrow changes, and soft tissue masses. 34 In the CAR recommendations, focal bone lesions with intralesional fat on MRI, or those that are blastic (greater than 885 Hounsfield units) on CT favour benign aetiologies that may not need to be further investigated in the absence of other concerning features. 34
Additionally, there is increasing importance on the impact of medical imaging on planetary health. 35 The carbon footprint of radiology includes both direct and indirect emissions during the production and use of medical imaging equipment and supplies. 35 Several strategies have been identified to improve the sustainability of radiology departments, including the implementation of decision support tools to reduce low-value imaging, and abbreviating imaging protocols when appropriate. 35 For example, by removing select sequences from a standard cardiac MRI protocol, the use of an abbreviated cardiac MRI protocol (8 minutes shorter) if implemented across the US would be equivalent in emissions savings to the average energy for 27 homes for 1 year. 36 The notion of net zero health-care emissions requires significant buy-in across all healthcare domains, and radiology departments have an opportunity to lead by example. 37 Reducing low-value imaging not only improves the value provided to patients but is an important way to improve sustainable planetary health practices.
Optimizing Access to Medical Imaging Services
There are additional levels of system inefficiencies that can be optimized to improve patient access to radiological services (Table 1). Single entry models are not a unique concept to the Canadian healthcare system. For example, improved access to surgical services under the BC Surgical Strategy and reducing wait times for lung cancer care in Newfoundland are 2 notable examples.38,39
Summary of Recommendations to Improve Value-Based Radiology in Canada.
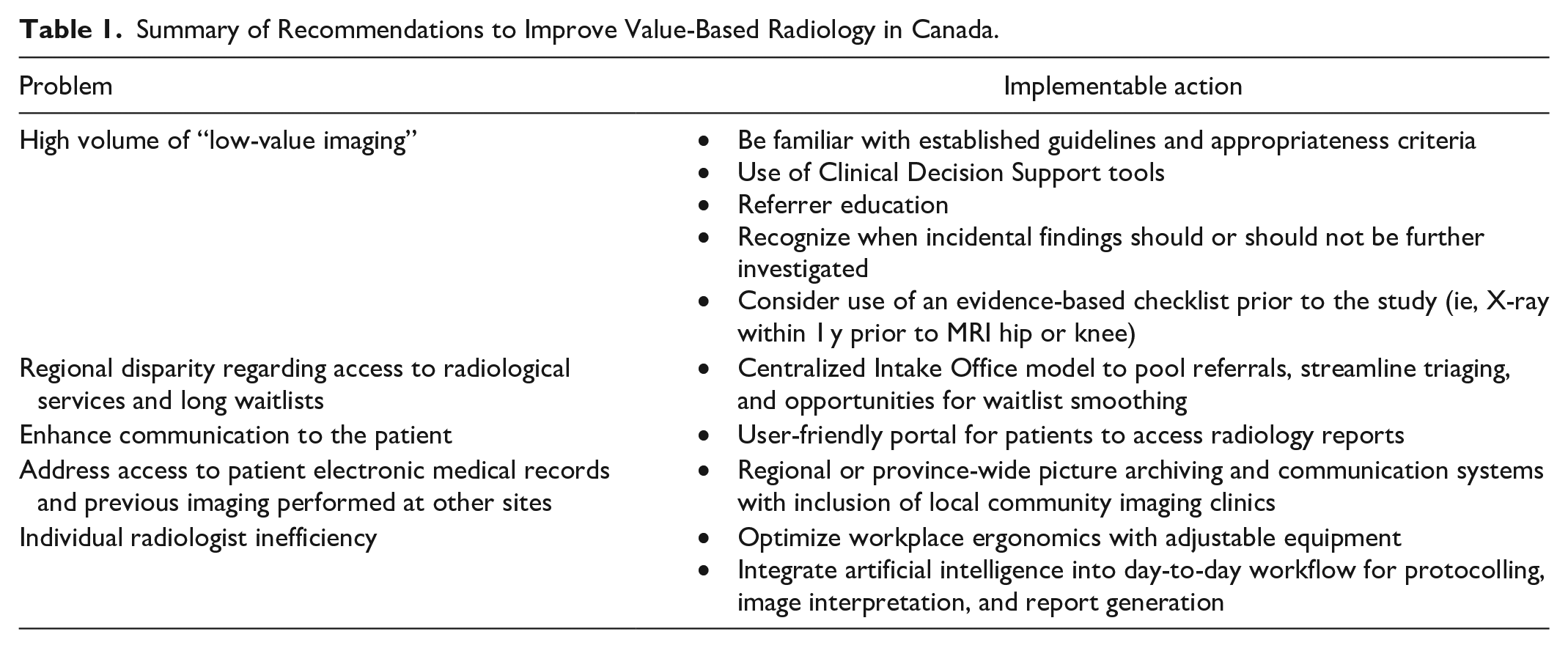
In radiology, however, centralized intake models are relatively uncommon, but pose an opportunity for significant improvements in waitlist smoothing and unnecessary imaging. Substantial variation in MRI service provision within Canadian academic imaging departments such as hours of operation, differences in request forms and prioritization scales were outlined and the need to improve consistency between institutions highlighted in the paper by Vanderby et al. 40 Moreover, the volume of MRI examinations continues to trend upward, with 50th and 90th percentile wait times of 49 and 169 days, respectively, in 2023. 41 In an effort to address anticipated increases in MRI referrals, a Central Intake Office was established in BC’s lower mainland following a provincial directive, encompassing multiple hospital facilities and utilizing a single entry model for system optimization. Through pooling of referrals and streamlined triaging for urgency, standardized pathways for care were established. This type of model can work synergistically with other interventions to reduce low-value imaging through the integration of appropriateness criteria and ensuring that clinical practice guidelines are met and has the potential for expansion into other communities, other modalities, and to incorporate artificial intelligence tools to streamline the process of referrals.
Enhancing Patient Communication
Prioritizing high-quality patient communication is a critical piece to VBR. 10 Direct radiologist-to-patient communication generally occurs at the time of an interventional radiological procedure and is integral to high-value care. However, optimizing patient communication through greater access to diagnostic reports is an area of increasing focus. In BC, the Digital Health Gateway mobile application is an initiative whereby patients can directly review their own imaging reports within a short timeframe. 42 Care is needed to ensure report clarity and the use of patient-sensitive terminology to decrease the potential for receiver anxiety or misinterpretation.
Enhancing Radiologist Workflow
System efficiency can also be impacted at level of the individual radiologist. In a survey of 191 CAR members, 79% reported the presence of musculoskeletal discomfort, and 93% reported that these symptoms affected their work productivity. 43 Ergonomic parameters such as adjustable desks and chairs, correct posture, and appropriate monitor height are easily implementable strategies to improve workplace efficiency. 43
Realtime integration of image archives and relevant information from the patient’s electronic medical record at the radiologist’s workstation can greatly enhance efficiency and reduce symptoms of burnout. The ability of a radiologist to access patient clinical information and to view prior imaging from outside centres is fundamental to a complete and accurate interpretation. Province-wide picture archiving and communication system integration, with the inclusion of community imaging clinics, would substantially reduce repeated examinations and improve the value and timeliness of care provided. 44 A recent statement by the ESR similarly calls attention to the desire for central archives to improve the availability of imaging from outside institutions. 45
Lastly, the use of artificial intelligence (AI) is increasingly viewed as a means of improving efficiency across all system levels. A major focus has been on AI’s potential utility in improving image interpretation and large language models to construct text. 46 In the area of image interpretation, the detection of acute findings can help a radiologist’s workflow by increasing confidence in diagnostic accuracy and ensuring timely communication of results for prompt management. For the detection of intracranial haemorrhage on head CT scans in an emergency department in Switzerland, the implementation of an AI-based tool demonstrated a negative predictive value of 98% with improved workflow metrics including shorter times to communication of positive and negative findings as well as shorter emergency department turnaround times. 47 Within Canada, anecdotally there are radiology groups which have employed similar AI tools for the detection of intracranial haemorrhage, though data on its performance and workflow benefits have yet to be published. Beyond interpretation, AI is predicted to have a role throughout the entire workflow: from organizing imaging requisitions, to triaging protocols, acquiring images, improving image quality, and generating reports. 48 At the image acquisition and post-processing stage, AI can be employed to improve image quality by enhancing spatial resolution, reducing noise, and removing motion and other artifacts. 49 AI has already been integrated into the post-processing of CT images among major vendors such as GE Healthcare, Canon Medical Systems, and Philips Healthcare which have developed US Food and Drug Administration approved deep learning reconstruction (DLR) algorithms that are being increasingly used clinically. 50 DLR algorithms allow for high-quality images with lower radiation doses and removal of metal and other artifacts. 50 Similarly, DLR algorithms can be used in the reconstruction of MRI scans, with notable applications in prostate MRIs allowing for accelerated acquisition times of T2-weighted turbo spin-echo sequences with improved image quality. 51 Anecdotally, these DLR algorithms are being increasingly used among Canadian radiology departments. At the report generation stage, natural language processing is a subset of AI that can be seamlessly integrated into the clinical workflow with the potential to transform the efficiency of both standardized and non-standardized reporting. 52
Conclusion
High-value radiological care requires optimization of system inefficiencies across multiple levels. The implementation of practice guidelines and clinical decision support tools can improve the appropriateness of requested imaging and thereby reduce low-value care. Standardized processes for requisition ingestion (eg, utilizing a centralized intake model), robust systems to communicate reports to patients, improvements in radiologist ergonomics, centralized imaging archives and electronic medical records, and the integration of artificial intelligence will all be integral in maintaining and improving Canada’s commitment to Value-Based Radiology. The measures outlined will also serve to reduce waste in the health care system and improve the ability of medical imaging to provide sustainable solutions into the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Alison Harris currently serves as Vice-President of the Canadian Association of Radiologists.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.