
Abstract
This is a visual representation of the abstract.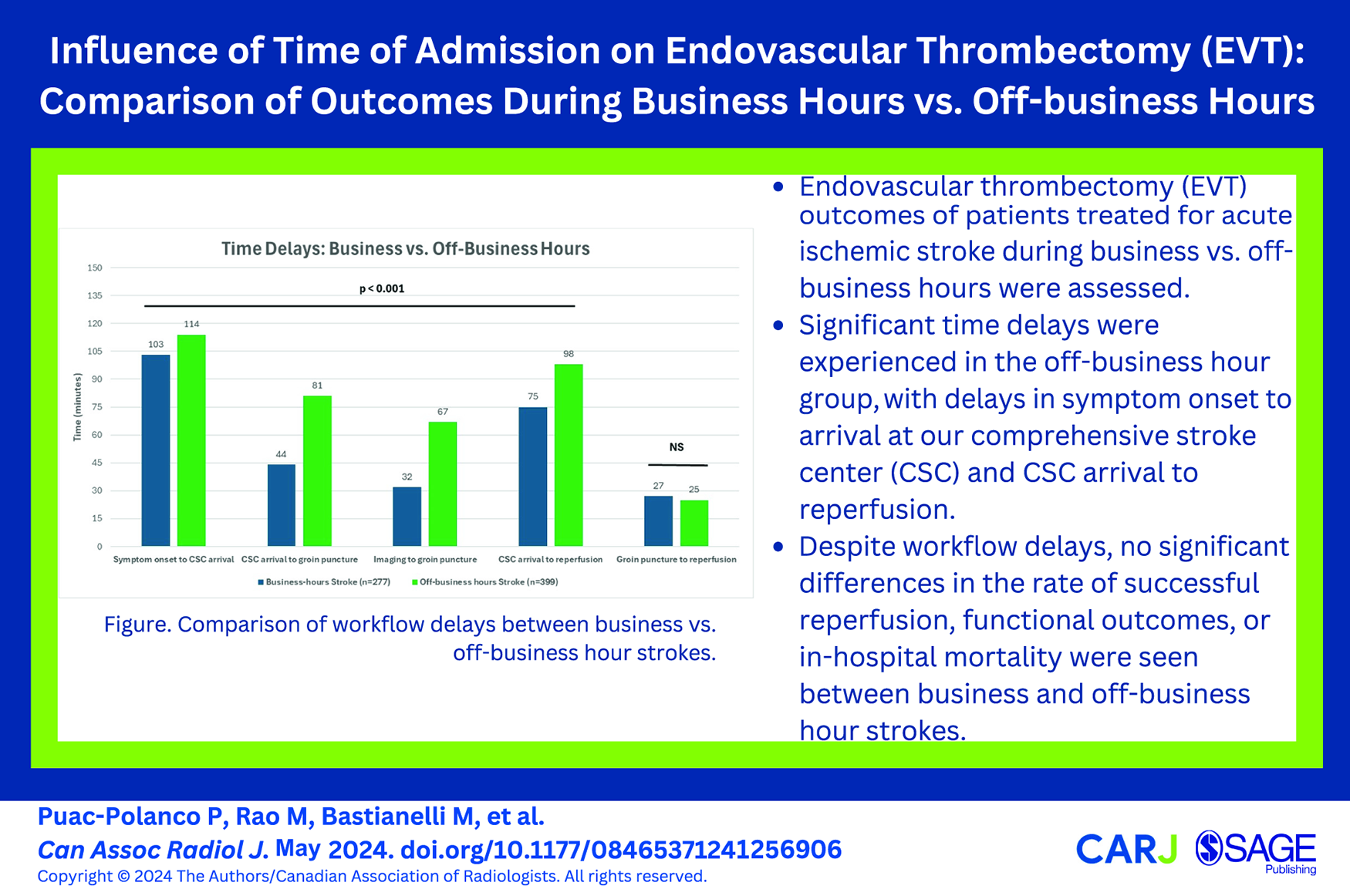
Introduction
The safety and outcome of endovascular thrombectomy (EVT) for acute ischaemic stroke (AIS) performed during off-business hours could be hampered by the intrinsic variables associated with working after-hours. Reduced alertness and impaired performance due to sleep deprivation are well-known effects on workers during night shifts, 1 resulting in a higher rate of accidents and injuries than during daytime hours. 2 In the case of stroke neurologists and neuroradiologists, business and off-business working hours have increased since EVT was approved as one of the first-line treatments for AIS. 3 Increased working hours could pose a risk for both patient and treating physician since a positive correlation has been demonstrated between the number of accidents and working hours.2,4 Increased burnout, fatigue, and staffing shortages during off-business hours could also negatively affect patient outcomes.5,6
Current data on the functional outcome of patients with EVT during different times of day are inconsistent, with some studies reporting no difference in outcomes,7,8 while others demonstrating better outcomes during business hours9-11 or even during off-hours. 12 The impact of time of day on EVT is still variable and controversial, and further studies are needed to elucidate its influence on patient outcomes. This study aimed to investigate the differences in outcomes of patients treated with EVT for AIS during business versus off-business hours in a large academic tertiary care hospital. We hypothesized that the outcome of patients with EVT during off-business hours is worse than in patients admitted during business hours, reflecting the impact of time of day on procedure workflow.
Methods
Data Source, Population, and Hospital Setting
We conducted a single-centre retrospective cohort study of patients with AIS treated with EVT from February 1, 2015, to May 31, 2021. The institutional ethics board approved this study, and the requirement for informed consent was waived. The Ottawa Hospital Civic Campus is a comprehensive stroke centre (CSC) and the sole provider of EVT to the region, servicing the Eastern Ontario region, including remote rural and indigenous communities with a population of approximately 1.3 million. EVT at our institution is performed by our neurointerventional group which consists of 1 neurologist, 1 neuroradiologist, and 2 neurosurgeons who rotate in a 1:4 call schedule to provide coverage for 24 hours at a time. During afterhours, the on-call neurointerventionalist is not in-house and is notified by the in-house neurologist only once a stroke is confirmed and EVT is indicated.
Participants and Study Groups
We retrospectively identified consecutive adult participants presenting with AIS symptoms who underwent EVT. Patients were divided into business and off-business hours based on their arrival time at our CSC. Business hours were defined as Monday to Friday between 8 AM and 4:59 PM, and off-business hours were defined as weekends holidays, and from 5 PM to 7:59 AM, Monday to Friday. Patients were also subdivided into mothership and drip-and-ship groups. The mothership group consisted of patients with AIS onset outside a healthcare facility and transferred directly to our CSC. The drip-and-ship group consisted of patients transferred to our CSC through a primary stroke centre (emergency department (ED) to ED transfer), with or without IV recombinant tissue plasminogen activator (rtPA) treatment. At our institution, drip-and-ship patients do not receive a repeat CT scan unless the patient’s clinical status is changed.
Inclusion Criteria
Adult patients (>18 years old) with AIS due to a large vessel occlusion treated with EVT within 12 hours of symptoms onset.
Exclusion Criteria
Patients with extracranial arterial occlusion or symptomatic stenosis without intracranial occlusion.
Clinical, Parameters, and Outcomes Variables
Clinical and Imaging Evaluation
Stroke severity was assessed by the National Institutes of Health Stroke Scale (NIHSS) on CSC arrival by a stroke neurologist. Patient demographics, past medical history, therapeutic interventions, stroke etiology, and discharge destination were obtained through an electronic chart review from our hospital database. Premorbid functional independence was defined as a modified Rankin Scale (mRS) score of ≤2. The subtype of stroke was further classified according to the Trial of Org 10172 in Acute Stroke Treatment classification. 13
All patients underwent computed tomography-computed tomography angiography imaging at our CSC or primary stroke centre before treatment as per institutional protocol. The ASPECTS score and occlusion site were obtained from the diagnostic imaging or endovascular therapy reports. The site of occlusion was defined as a large vessel occlusion in the anterior circulation (intracranial internal carotid artery [ICA], proximal A1, M1, and proximal M2 segments) or posterior circulation (proximal intracranial vertebral arteries and basilar artery).
Thrombectomy Procedures
EVT was performed using any approved device, such as a stent retriever, aspiration device, or a combination of different techniques. The number of EVT passes was extracted from the procedural report. Successful reperfusion was defined as a score on the modified treatment in cerebral ischaemia (mTICI) score ≥2b. 14
Timing
The following process measures were studied: symptom onset to CSC arrival, stroke onset to initiation of alteplase, CSC arrival to groin puncture, imaging to groin puncture, CSC arrival to reperfusion, and groin puncture to reperfusion.
Outcomes
The primary endpoint was functional neurological disability scored on the mRS at 90 days after EVT. Secondary outcomes were the rate of successful reperfusion after EVT and procedural workflow time delays. Safety outcomes included intracranial hemorrhage, defined as a parenchymal haematoma occupying more than 30% of the infarcted territory (PH2 according to the Heidelberg Classification 15 ) within 5 days after EVT, and mortality within 90 days.
Statistical Analysis
Categorical or ordinal variables are reported as percentages. Differences in proportions between groups were assessed using Fisher’s exact or Chi-Square tests as appropriate. Continuous variables are presented as median (interquartile range [IQR]). Variables were analyzed individually, and missing data was excluded from the analysis for that specific variable. We did not perform any imputation or substitution of a mean. Differences in medians between groups were assessed using Mann-Whitney U tests. Two-sided P < .05 was considered statistically significant. A favourable clinical outcome was defined as a 90-day mRS score of 0 to 2.
Results
A total of 676 patients were included in the final analysis after 88 exclusions (Figure 1). The business-hour stroke group comprised 41% (277/676), and the off-hour stroke group 59% (399/676) of the study population. Compared to the business-hours stroke patients, patients admitted during off-business hours tended to be younger (median [IQR]: 70 [62-81] vs 73 [60-79], P = .06; Table 1), more likely to have high blood pressure (63% vs 55%, P = .05) and coronary atherosclerosis (18% vs 12%, P = .04). The median NIHSS score at arrival was 17 (IQR, 12-21; P = .47) in both groups. Cardioembolic strokes accounted for approximately half of the strokes in both groups (P = .64). Anterior circulation occlusions accounted for the vast majority of strokes (>90%), with the M1 segment of the MCA being the most common site of occlusion (35% vs 40%, P = .19). Intravenous thrombolysis was given to 60% of patients in both groups (P = .87), with a faster door-to-needle time for strokes occurring during business hours (minutes [IQR]: 32 [26-45] vs 35 [28-48], P = .02). No significant group differences were seen in sex, ASPECTS, or other risk factors.
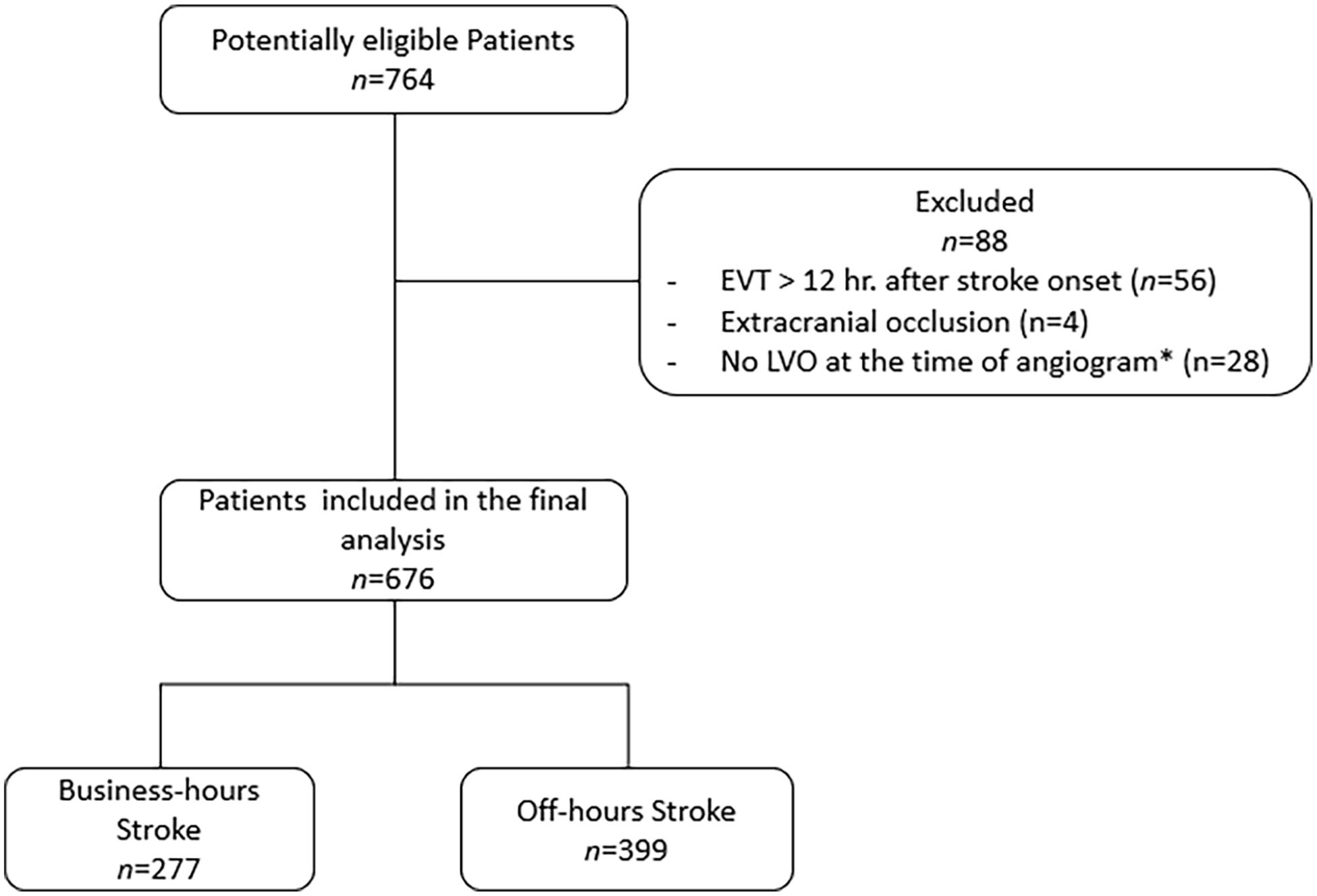
Patient flowchart.
Demographics and Baseline Characteristics of Business Hours Versus Off-Business Hours Strokes.
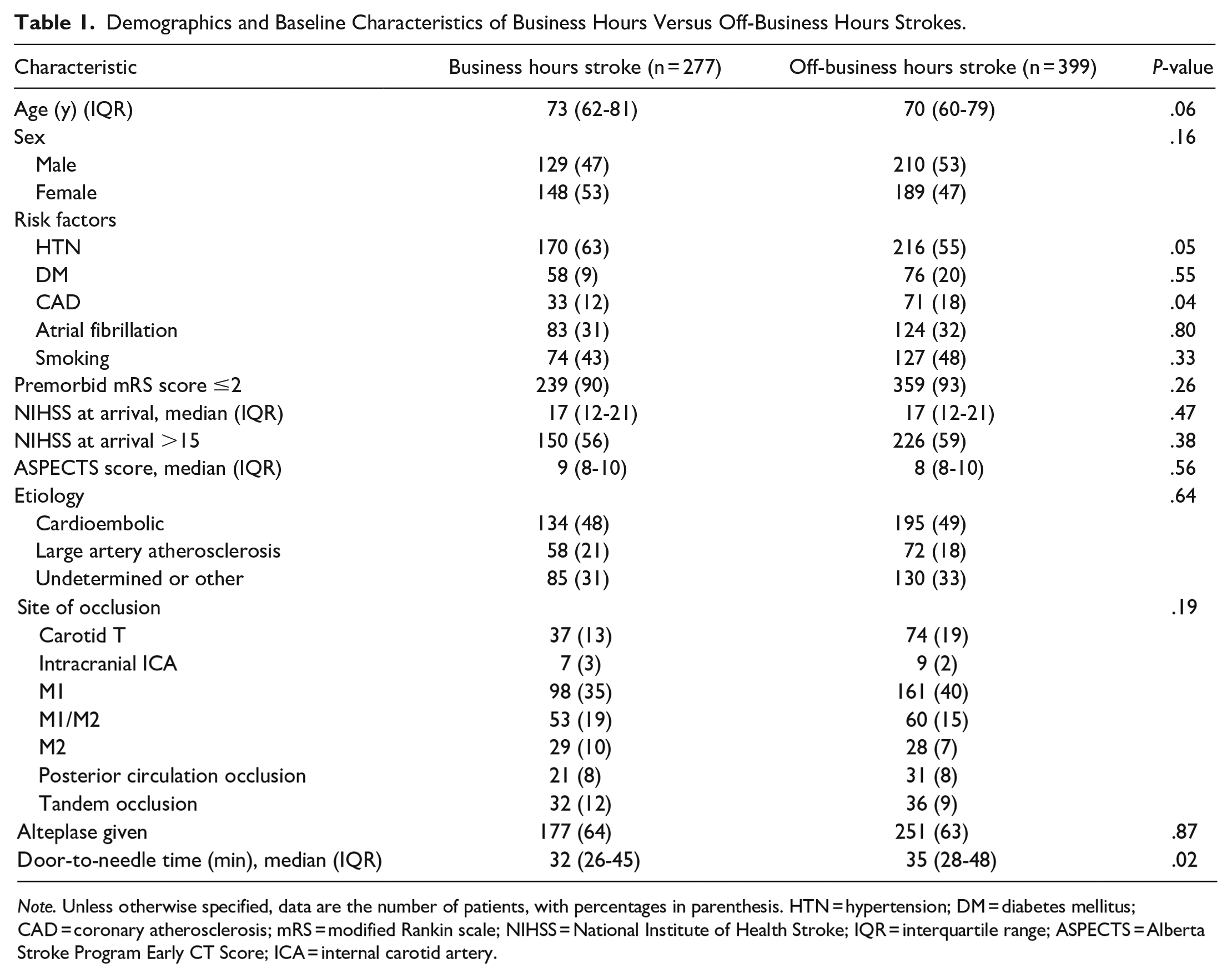
Note. Unless otherwise specified, data are the number of patients, with percentages in parenthesis. HTN = hypertension; DM = diabetes mellitus; CAD = coronary atherosclerosis; mRS = modified Rankin scale; NIHSS = National Institute of Health Stroke; IQR = interquartile range; ASPECTS = Alberta Stroke Program Early CT Score; ICA = internal carotid artery.
Overall, strokes during off-business hours were associated with longer workflow delays than business hours (Table 2). Time of arrival to the CSC from symptom onset was 11 minutes later in the off-business hours strokes (P < .001). Moreover, off-business hours strokes were associated with approximately twice the delay between CSC arrival to groin puncture (minutes [IQR]: 81 [61-99] vs 44 [37-54], P < .001) and imaging to groin puncture (minutes [IQR]: 67 [50-87] vs 32 [26-42], P < .001) compared to the business hour group. Regarding reperfusion, 4 out of 5 patients achieved successful recanalization in both groups. However, after CSC arrival, reperfusion took 23 minutes longer for off-business hours strokes (P < .001). No significant difference in the rate of in-hospital mortality (P = .47), parenchymal haematoma (P = .26), or NIHSS at discharge (P = .73) between the 2 groups (Table 2) was observed. At 90 days, the median mRS score was 1 (IQR, 0-4; P = .91), with 65% of patients having an mRS ≤2 at 90 days in both groups.
Time Delays and Outcomes Comparison Between Business and Off-Business Hours Strokes.
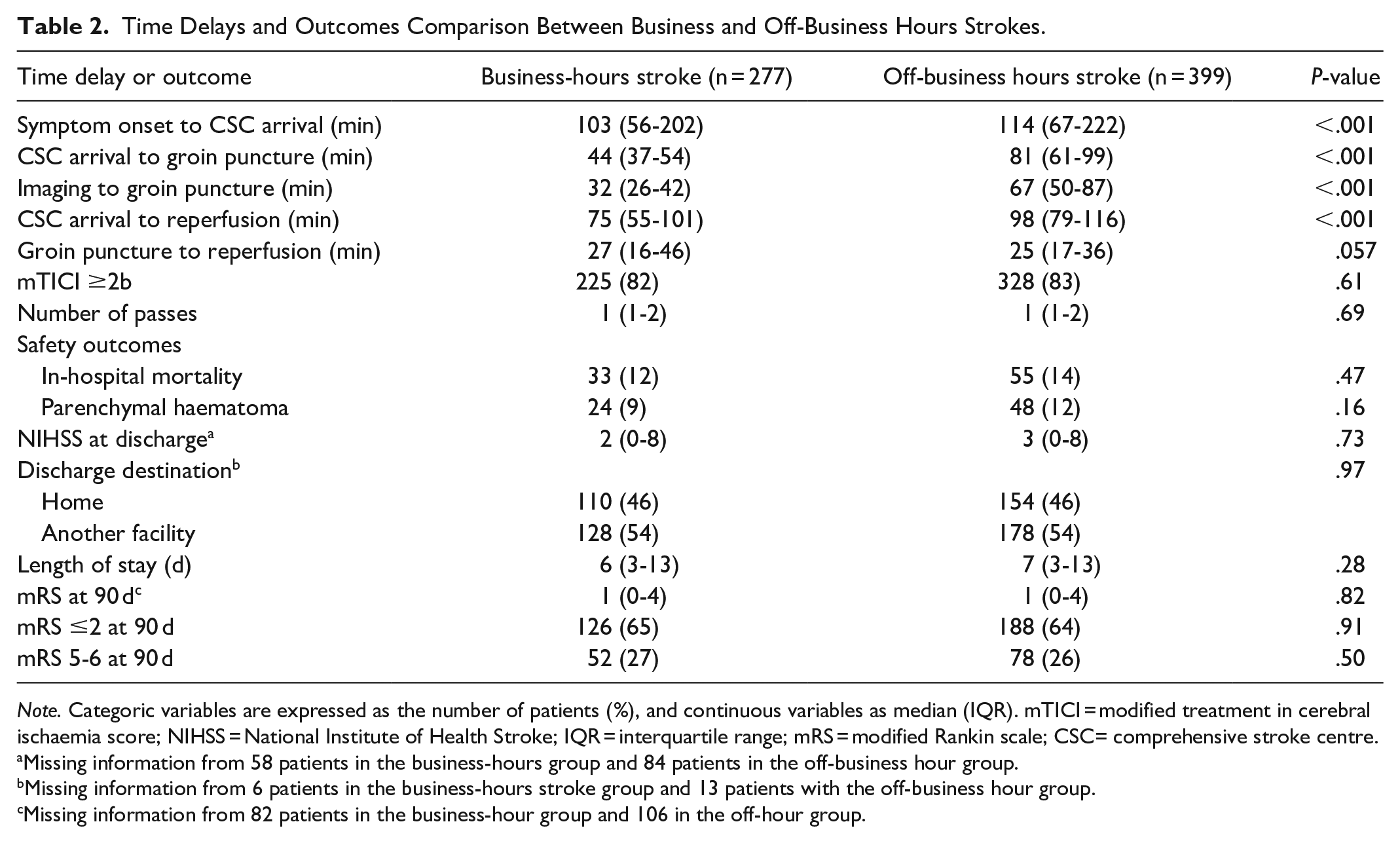
Note. Categoric variables are expressed as the number of patients (%), and continuous variables as median (IQR). mTICI = modified treatment in cerebral ischaemia score; NIHSS = National Institute of Health Stroke; IQR = interquartile range; mRS = modified Rankin scale; CSC= comprehensive stroke centre.
Missing information from 58 patients in the business-hours group and 84 patients in the off-business hour group.
Missing information from 6 patients in the business-hours stroke group and 13 patients with the off-business hour group.
Missing information from 82 patients in the business-hour group and 106 in the off-hour group.
Subgroup Analysis: Mothership Versus Drip and Ship
In the subgroup analysis, business and off-business hour strokes were subdivided further into those admitted directly to the CSC (mothership) and those transferred from a primary stroke centre to our CSC (drip and ship).
From the 277 patients in the business hour group, 69% (191) were mothership transfers, and 31% (86) were drip and ship transfers (Table 3). There was a significantly higher proportion of men in the mothership group (51% vs 37%, P = .04), and diabetes was more common in the drip and ship group (30% vs 18%, P = .04). Otherwise, there were no significant differences in other co-morbidities, NIHSS scores, and pre-morbid mRS scores. Significant delays were seen in the drip and ship group, with a median time of 3.4 hours from symptom onset to CSC arrival versus 1.2 hours in the mothership group (P < .001). However, drip and ship patients had a shorter time delay between CSC arrival to groin puncture (minutes [IQR]: 47 [39-58] vs 37 [31-45], P < .001) and CSC arrival to reperfusion (minutes [IQR]: 77 [63-108] vs 60 [51-88], P < .001). No significant difference was seen in groin puncture to reperfusion (minutes [IQR]: 29 [16-45] vs 26 [15-48], P = .4). A similar proportion of successful recanalization was seen between the 2 groups (84% vs 77%, P = .18). No significant differences were seen in favourable outcome rates at 3 months (67% vs 57%, P = .23).
Subgroup Analysis of Business-Hours Strokes.
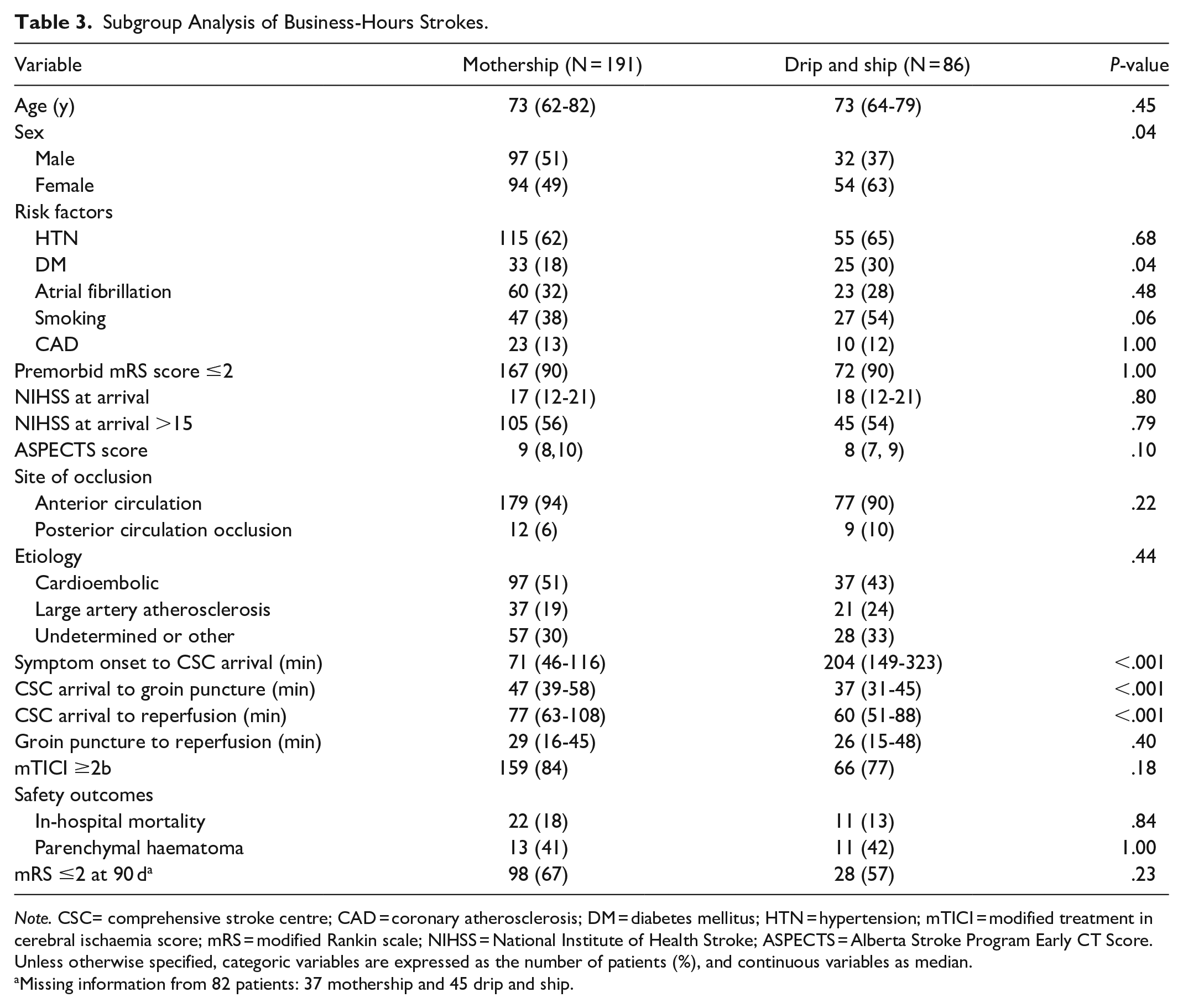
Note. CSC= comprehensive stroke centre; CAD = coronary atherosclerosis; DM = diabetes mellitus; HTN = hypertension; mTICI = modified treatment in cerebral ischaemia score; mRS = modified Rankin scale; NIHSS = National Institute of Health Stroke; ASPECTS = Alberta Stroke Program Early CT Score. Unless otherwise specified, categoric variables are expressed as the number of patients (%), and continuous variables as median.
Missing information from 82 patients: 37 mothership and 45 drip and ship.
From the 399 patients in the off-business hour group, 72% (287) were mothership transfers and 28% (112) were drip and ship transfers (Table 4). There was a significant proportion of men having a direct transfer to the CSC (56% vs 44%), and more women admitted through a drip and ship route than their counterparts (55% vs 45%; P = .04). Mothership patients were more likely to present an NIHSS score at arrival >15 (64% vs 41%, P ≤ .01) and have a higher ASPECTS score on initial imaging (9 [8-10] vs 8 [7-9], P = .001). It took a median time of 3.4 hours from symptom onset to CSC arrival for drip and ship patients versus 1.4 hours for mothership transfer strokes (P < .001). On the other hand, drip and ship patients had a shorter time delay between CSC arrival to groin puncture (minutes [IQR]: 58 [39-81] vs 86 [62-115], P < .001), CSC arrival to reperfusion (minutes [IQR]: 86 [62-115] vs 115 [94-149], P < .001), and groin puncture to reperfusion (minutes [IQR]: 25 [16-34] vs 28 [18-43], P = .01) than mothership patients. Mothership patients had a more significant proportion of successful recanalization (86% vs 77%, P = .04) and a higher favourable outcome rate (68% vs 52%, P = .02) at 3 months than drip and ship patients.
Subgroup Analysis of Off-Business Hours Strokes.
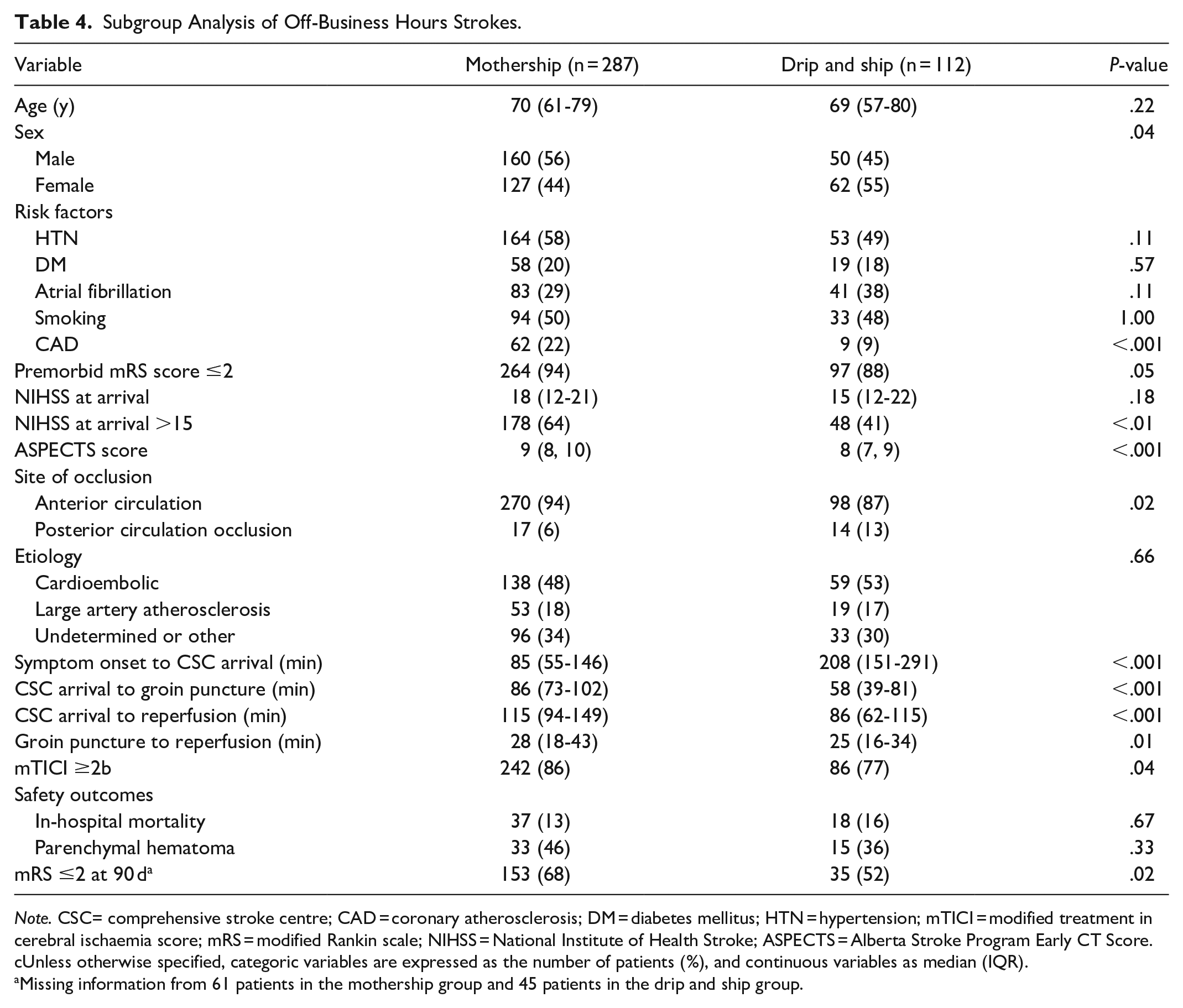
Note. CSC= comprehensive stroke centre; CAD = coronary atherosclerosis; DM = diabetes mellitus; HTN = hypertension; mTICI = modified treatment in cerebral ischaemia score; mRS = modified Rankin scale; NIHSS = National Institute of Health Stroke; ASPECTS = Alberta Stroke Program Early CT Score. cUnless otherwise specified, categoric variables are expressed as the number of patients (%), and continuous variables as median (IQR).
Missing information from 61 patients in the mothership group and 45 patients in the drip and ship group.
Discussion
The results of the study demonstrate significant time delays in the off-business hour group but no differences in the rate of successful reperfusion, functional outcomes, or in-hospital mortality. Significant delays between symptom onset and CSC arrival were noted at our institution in the off-business hours group, highlighting the need for better prehospital coordination during off-hours.
Off-hours effects regarding time delays have been well documented in the literature in patients with AIS receiving EVT.8,9,12,16-19 Following CSC arrival of patients with off-business hours strokes, significant delays were noted in CSC arrival to groin puncture, imaging to groin puncture, and CSC arrival to reperfusion in our study. A meta-analysis from Zha et al reported a delay in CSC arrival to groin puncture of 11 minutes in the off-business hour group compared to business hours strokes. 16 Our study noted a longer delay of 37 minutes. Imaging to groin puncture and CSC arrival to reperfusion were also longer in the off-business hour strokes, which aligns with previous publications. 10 Peri-procedural workflow components during off-business hours in our study could have contributed to delays particularly involving interventional suite setup and staff commute to the CSC. Our institution’s interventional neuroradiologists and EVT-related staff (nurses, technologists) are not onsite outside regular hours; therefore, delays in the commute of the treatment team might be a factor after a stroke requiring EVT is confirmed by the in-house neurologist.
In the subgroup analysis, the drip and ship patients in both business and off-business hour strokes showed significant delays in CSC arrival time from symptom onset, with a median time of nearly 2 hours longer than the mothership group. Delays in patient care at the primary stroke centre (ie, patient assessment, imaging interpretation, thrombolysis administration, telestroke communication with CSC) and patient transport between hospitals, may account for this. Conversely, time delays after CSC arrival were shorter in drip and ship in both business and off-business hour groups. The commute of the treatment team to the CSC would be less of a factor in drip-and-ship patients during off-hours, as the treatment team would likely be on-site once the patient has arrived. Additionally, drip-and-ship stroke patients are not re-scanned at our CSC unless the patient’s clinical status has changed. These factors may explain why the peri-procedural times for drip-and-ship patients after arrival to the CSC were shorter than the mothership group in the subgroup analysis.
Despite significant peri-procedural delays in the off-business hours strokes, our study found no significant difference in procedural times and reperfusion rates in the off-business hour group. Although some studies described similar results, 7 this was inconsistent with the findings reported in the meta-analysis by Zha et al, who noted significantly lower reperfusion scores in the off-business hour group despite similar procedural times. 16 These differences may be explained by institutional differences in stroke case volume, call schedules, or the definition of “off-hours.”
Intriguingly, the procedural delays observed in our study did not appear to translate into significantly worse in-hospital mortality or prognosis in the off-business hour group. These findings were comparable to the literature,8,17 including a study by Tschoe et al which featured data from nearly 2000 patients across 6 high-volume US centres. 18 In the subgroup analysis, functional outcomes differed only in the off-business hour group, with mothership patients having more favourable outcomes despite a higher proportion of NIHSS >15 at arrival. These results are discordant with the literature where Mourand et al reported no differences in mRS at 90 days 19 and Benali et al reported more favourable outcomes with drip-and-ship patients. 12 Lower pre-stroke disability and higher ASPECTS and reperfusion scores in our off-business hour mothership group may, in part, explain our results. Moreover, our results show that significant time delays experienced by the drip-and-ship group before CSC arrival may contribute to less favourable outcomes during off-business hours. Further studies should investigate time delays in drip-and-ship patients and explore possible underlying variables to explain these differences.
There are limitations to our study. Our results were retrospectively analyzed, and any missing data may lead to bias. As our study involved only a single comprehensive stroke centre, generalization to other centres is limited. Other centres may have different call schedules or definitions of off-business hours. Other factors such as population density, hospital workflow, and healthcare infrastructure may influence peri-procedural time metrics that were studied. Finally, our study excluded patients with EVT >12 hours window and may limit generalization as more thrombectomies are being performed outside this established window.
Conclusion
Despite workflow delays before EVT initiation for AIS during off-business hours, there were no differences in the rate of successful reperfusion, functional outcomes, or in-hospital mortality. Worse functional outcomes for drip-and-ship patients with delays in CSC arrival were noted, highlighting the need for faster transportation of stroke patients between healthcare facilities during off-business hours. Establishing a more streamlined process for drip-and-ship patients and improving pre-EVT workflow at the CSC during off-hours is needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.