
Abstract
Imaging of pregnant patients who sustained trauma often causes fear and confusion among patients, their families, and health care professionals regarding the potential for detrimental effects from radiation exposure to the fetus. Unnecessary delays or potentially harmful avoidance of the justified imaging studies may result from this understandable anxiety. This guideline was developed by the Canadian Emergency, Trauma and Acute Care Radiology Society (CETARS) and the Canadian Association of Radiologists (CAR) Working Group on Imaging the Pregnant Trauma Patient, informed by a literature review as well as multidisciplinary expert panel opinions and discussions. The working group included academic subspecialty radiologists, a trauma team leader, an emergency physician, and an obstetriciangynaecologist/maternal fetal medicine specialist, who were brought together to provide updated, evidence-based recommendations for the imaging of pregnant trauma patients, including patient safety aspects (eg, radiation and contrast concerns) and counselling, initial imaging in maternal trauma, specific considerations for the use of fluoroscopy, angiography, and magnetic resonance imaging. The guideline strives to achieve clarity and prevent added anxiety in an already stressful situation of injury to a pregnant patient, who should not be imaged differently.
This Practice Guidelines has been reviewed and endorsed by Canadian Association of Radiologists, the Canadian Association of Emergency Physicians (CAEP)
Recommendations
After major trauma, the management and initial imaging priorities of a pregnant patient are equivalent to those of a non-pregnant trauma patient.
Trauma radiographs and extended Focused Assessment with Sonography in Trauma (e-FAST) play an important role in the initial assessment of pregnant trauma patients in the trauma bay.
When justified, CT (including whole-body CT) should be performed in pregnant trauma patients according to the same local protocol used for a non-pregnant patient.
MRI is rarely used for the initial workup of trauma patients and should be reserved for specific circumstances.
Intravenous iodinated contrast is recommended in initial CT of the pregnant trauma patient for accurate and timely diagnosis of the maternal injuries. There is no known adverse effect of use of low-osmolality iodinated contrast to the fetus. Cystic and enteric contrasts can be used as deemed appropriate.
Gadolinium-based contrast agents should be avoided for imaging the pregnant trauma patient.
The use of shielding is not recommended.
Introduction
Trauma is the leading non-obstetrical cause of maternal and fetal mortality and affects an estimated 5% to 7% of all pregnancies. Motor vehicle collisions as the most common cause of trauma in pregnancy, accounting for up to 58.1%, followed by falls (16.7%) and assaults (14.9%). 1 Trauma in pregnancy is underreported, especially in cases involving domestic violence,2,3 limiting recognition of its actual magnitude. As a measure of injury severity in trauma, the Injury Severity Score (ISS) is routinely used in trauma with scores ranging from 1 (near normal) to 75 (non-survivable). 4 The score cannot usually be assigned during resuscitation but does serve a purpose for description in trauma registries and for use in research. While in non-pregnant trauma patients, severe trauma is considered at a cut-off of 15, Tenami et al divided major and minor injuries in pregnant trauma patients at an ISS of <9, reflecting the compounding effect of fetal life. 5 Fetal loss happens in 50% of the major traumas and 1% to 5% of the minor ones.6,7 Due to the significantly higher number of patients presenting with minor trauma, this accounts for the majority of fetal losses. 5 However, the urgency of care provision and the multitude of care providers involved in major trauma resuscitation may lead to more anxiety than in minor trauma evaluation. For this reason, the multidisciplinary panel gathered for this guideline has decided to focus on major trauma as the scope for this guideline.
General Principles
Every injured person of reproductive age who can get pregnant, should be considered pregnant until proven not to be pregnant. The primary focus of initial management of the pregnant patient after major trauma is maternal stabilization, which will directly benefit fetal outcome. The pregnant trauma patient represents a unique cohort of patients, with distinctive physiological and anatomical changes that increase the risk of certain traumatic injuries, such as bladder and uterine injuries, and can have placental and fetal injuries.
Medical imaging plays a crucial role in the diagnosis and management of injured patients which cannot be obtained by physical examination alone. The foundations of the Advanced Trauma Life Support (ATLS) program, which is taught in over 80 countries, are the primary and secondary structured physical exams (surveys) aimed at identifying the greatest threats to life and limb. 8 Despite the success of ATLS, physical examination has its own limitations. Among clinicians with variable levels of experience, physical examination of life- and limb-threatening injuries demonstrate sensitivities that vary by body region from low (23.5%; pelvic injuries) to high (69.9%; long bone fracture). 9 In stable, examinable patients who experienced high-energy blunt trauma, up to 19% of patients without physical examination findings revealed imaging results that changed clinical management. 10 In light of these clear limitations of physical examination in trauma patients, ancillary tests including imaging are of paramount importance.
As with the management of non-pregnant trauma patients, trauma bay radiographs, extended Focused Assessment with Sonography in Trauma (e-FAST), and subsequent Computed Tomography (CT), where indicated and possible, remain the primary modalities of initial imaging. Modalities that do not use ionizing radiation, such as broader formal ultrasonography and Magnetic Resonance Imaging (MRI), have a very limited role in the initial imaging of a major trauma in a pregnant patient. Using appropriate diagnostic imaging is not only of paramount importance to timely diagnose the maternal injuries, it is equally pivotal to avoiding non-obstetrical laparotomies that are associated with an approximate 26% and 82% incidence of preterm labour in second and third trimesters, respectively.11,12
All imaging examinations in trauma must be justified and, in all patients, potentially harmful radiation should only be used if the benefits outweigh risks. Since maternal life remains the priority for both maternal and fetal outcome, the justification for the use of diagnostic imaging in the pregnant patient is the same as that for other patients who have sustained major trauma. A multidisciplinary collaborative management approach is crucial for standardized patient care, including an imaging approach for pregnant trauma patients that does not deviate from that of a non-pregnant trauma patients. 13
Initial Maternal Imaging After Trauma
In this section, we will describe topics that support this general statement. Evidence will be provided for questions that often arise, followed by specific descriptions of modalities that should or may be used.
Radiation Concerns
The concerns for the use of ionizing radiation during pregnancy originate from the risks associated with fetal exposure, as a developing fetus is more sensitive to the potential harms. It is estimated that a fetus is exposed to 1 mGy of background radiation during pregnancy. 14 For imaging examinations in which the fetus is not in the field of view, such as craniocervical, thoracic, or extremity imaging, radiation doses are well below the fetal dose from naturally occurring background radiation and should not elicit concerns about the radiation exposure to the fetus. However, interventional fluoroscopic procedures or CT that expose the fetus directly may result in higher radiation exposure, with risks to the fetus depending on the radiation dose received and the gestational age at time of exposure.
According to the American College of Radiology (ACR), American College of Obstetricians and Gynecologists (ACOG), and the National Council on Radiation Protection and Measurements (NCRPM), a fetal radiation dose of less than 50 mGy is not associated with increased fetal anomalies nor fetal loss. 13 In the first 2 weeks after conception, the main risk to the embryo is spontaneous abortion. The effect is all or none, and only observed at doses greater than 50 to 100 mGy. 15 Beyond 2 weeks, risk of anomalies, growth restriction, or abortion have not been reported with radiation exposure less than 50 mGy. 16 The ionizing radiation dose of diagnostic imaging examinations that are used in the initial trauma evaluation are well below this threshold (Table 1).
Estimated Fetal Radiation Dose From Conventional Radiographic and CT Examinations.
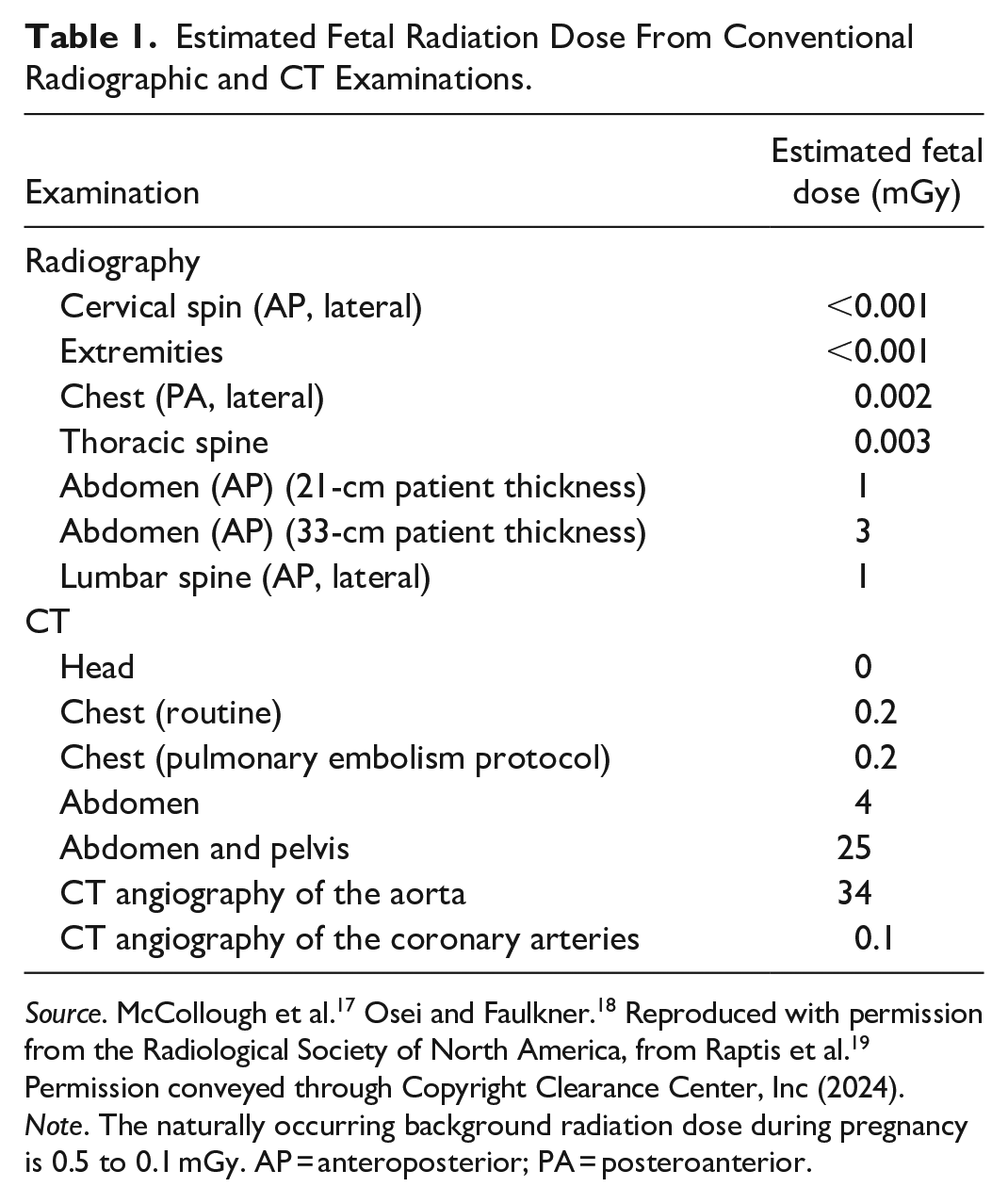
Source. McCollough et al. 17 Osei and Faulkner. 18 Reproduced with permission from the Radiological Society of North America, from Raptis et al. 19 Permission conveyed through Copyright Clearance Center, Inc (2024).
Note. The naturally occurring background radiation dose during pregnancy is 0.5 to 0.1 mGy. AP = anteroposterior; PA = posteroanterior.
All ionizing radiation procedures should adhere to the “as low as reasonably achievable” (ALARA) principle since the stochastic effects of the radiation have no known threshold dose. The most effective way to limit radiation exposure to the pregnant patient is to avoid unnecessary imaging or when appropriate, use alternative modalities without ionizing radiation.
Contrast Administration
Iodinated Contrast
Intravenous iodinated contrast agents are justified and recommended as part of standard trauma CT imaging for the detection and characterization of parenchymal and vascular injuries. Iodinated contrast can be instilled in the urinary bladder to evaluate for bladder injury. According to local protocols, oral and rectal iodinated contrast media can be administered, usually for specific clinical scenarios such as penetrating trauma. Angiography and interventional radiology procedures necessitate intra-arterial administration of iodinated contrast.
Iodinated contrast materials have been proven to cross the blood-placental barrier to the fetus in measurable quantities, and therefore administration of any of these agents warrants consideration of risk versus benefit.20,21 While no controlled studies have been performed in pregnant women, low-osmolality iodinated contrast agents have not been associated with any adverse mutagenic or teratogenic effects in studies using animal models, and are accordingly classified in the United States as category B (FDA) pharmaceuticals. Reports of the development of hypothyroidism in the newborn infant after the administration of an iodinated contrast agent during pregnancy are limited to amniofetography, using a fat-soluble contrast material, that is no longer in general use.
At this time, there are no documented cases of neonatal hypothyroidism from the maternal intravascular injection of water-soluble iodinated contrast agents.22-24 Given the lack of evidence of any significant harm to the fetus, iodinated contrast agents should not be withheld for CT examinations performed in the setting of major trauma.
Gadolinium-Based Contrast
Gadolinium-based contrast agents used in MRI performed for adjunct assessment have been shown to cross the blood-placental barrier to the fetus. Depending on the gestational age, the contrast agent can be taken up and then excreted by the fetal kidneys into the amniotic fluid for potential recirculation. 25 A retrospective review of Canadian cases of gadolinium-based contrast exposure in pregnancy found an association with the increased risk of stillbirth or neonatal death in late term exposure, and of rheumatological, inflammatory, or infiltrative conditions in early term exposure, though the findings are limited by potential confounders. 26
As in other scenarios where gadolinium-based contrast is considered in pregnancy, administration requires that the benefits outweigh the potential risks. Informed consent should be obtained when possible.
Shielding Consideration
While historically offered for patient reassurance, the use of shielding potentially increases internal scatter and therefore, likely increases the radiation dose to the fetus. The improper placement of the shielding may either obscure the imaged field of view or introduce artifact leading to repeat imaging. Furthermore, if shielding is used, the automatic exposure control may overcompensate by increasing mAs and increase the fetal dose.
The American Association of Physicists in Medicine issued a statement in 2019 indicating that shielding does not stop the internal scatter. The ACR, the NCRPM, the American Board of Radiologists, and the Society of Pediatric Radiology recommend against the use of shielding.27,28 In May 2021, the Canadian Association of Radiologists also provided a position statement on Gonadal and Fetal Shielding for X-rays, recommending the discontinuation of routine use of gonadal and fetal shielding.28,29
Patient Consent and Counselling
The consent process for imaging pregnant trauma patients follows the same process as with any medical procedure, intervention, or diagnostic test. As outlined by the Canadian Medical Protective Association, valid consent must be voluntary. The patient must have had the capacity to consent, and the patient must have been properly informed.30,31
In patients with major trauma, an important exception to the requirement of valid informed consent may apply. When the patient or substitute decision maker is unable to consent and there is an imminent threat to life, limb, or health, the physician has the duty to do what is immediately necessary without consent. 31 The need to continue with diagnostic imaging without valid consent will often apply in pregnant patients with major trauma. Once the patient regains capacity or a substitute decision maker is present, informed consent must then be obtained for additional diagnostic imaging or treatment.
Patient counselling is a crucial step to provide detailed information about the use of diagnostic modalities and an objective assessment of the potential risk to the developing fetus. Addressing patient and family concerns about the risks and benefits of CT imaging in pregnant patients is the role of the most responsible physician. For the initial imaging of the trauma patient, this responsibility typically falls to the trauma team leader. The physician caring for pregnant trauma patient should understand the benefits of appropriate imaging for maternal and fetal health and the risks of radiation and contrast exposure to the fetus, which should be discussed with the patient or substitute decision maker if possible and time permits. Where needed and if time permits, a radiologist can be consulted to discuss uncertainties.
In cases where repetitive CT of the abdomen and pelvis is considered for clinical needs, involvement of a radiologist and/or Radiation Safety Officer/Medical Physicist beforehand could be useful to provide adequate information about the risks involved. Consultation may also be useful in cases of concern after patients underwent imaging with radiation exposure. We recommend estimating the fetal radiation exposure dose especially in patients who have been exposed to a large radiation dose. In this setting, consultation with a Radiation Safety Officer/Medical Physicist is recommended to obtain the most accurate estimate of the fetal radiation dose and help guide appropriate patient counselling.
Imaging Modalities
Trauma Bay Modalities: Radiography and e-FAST/Ultrasound
To screen for immediate life-threatening findings and confirm positioning of lines and tubes, similar to any non-pregnant trauma patient, a routine series of radiographs after major trauma consists of at least a chest and a pelvic radiograph. Point of care ultrasonography via e-FAST is usually used as an adjunct to the initial assessment to assess at the bedside for intraperitoneal, pericardial, or pleural fluid and pneumothorax. The e-FAST has a wide range of reported sensitivities and accuracies and requires appropriate training and technical skill to be useful. Ultrasound may still be less sensitive for the detection of intraperitoneal free fluid in pregnancy.32-34 The primary role of bedside ultrasound is the early recognition of fluid and air and help identify select immediately life-threatening injuries. However, it is not a substitute for a clinically indicated diagnostic (whole-body) CT to detect visceral and vascular injuries.
Computed Tomography (CT)
Given the variability in equipment and local protocols, prescribing how to perform a CT in the setting of trauma is beyond the scope of this guideline. Guidelines on imaging patients after major trauma have been published by the American College of Surgeons (ACS), the ACR, the Royal College of Radiologists (RCR), and the European Society of Emergency Radiology (ESER), all whom provide a thorough review on this topic.35-38 While a comprehensive review of these guidelines is also outside the scope of this document, there is broad support for judicious liberal imaging protocols in major trauma. The ACS guidelines note that indications for whole-body CT include clinical suspicion of multi-system injury, altered level of consciousness, or significant mechanisms of injury. 37 While the ACR guidelines note that whole-body CT is categorized as either “may be appropriate” or “usually appropriate” in every category of injury pattern. 36 Both the RCR and ESER guidelines endorse the use of whole-body CT as routine, with RCR noting that “whole-body contrast-enhanced multi-detector CT is the default imaging procedure of choice in the severely injured patient.” 38
Pregnant patients warrant no different treatment from non-pregnant patients, and the best medical care for the mother is the also the best medical care for the fetus. The guidelines from ACS, ACR, and RCR explicitly describe the acceptability of CT imaging in pregnant patients.36-38 These positions are supported by colleagues in obstetrics and gynaecology. The ACOG guidelines on imaging during pregnancy note that “the use of CT and associated contrast material should not be withheld if clinically indicated” 1 while the Society of Obstetricians and Gynaecologists of Canada guidelines advise that maternal evaluation of the abdomen using CT should not be deferred or delayed due to concerns for fetal exposure to radiation. 30
Using triage methods, a distinction can be made between patients whose risk of occult injury is sufficiently high to warrant liberal CT imaging regardless of clinical findings and those with lesser risk for whom selective regional CT would be sufficient. Definitions of major trauma vary, but the ACS national guidelines for field triage in trauma serve as an accepted standard in North America and define major trauma by a combination of injury patterns, patient factors, mechanisms of injury, and associated high-risk clinical circumstances. 39 Patients who sustained major trauma should undergo liberal imaging, rather than selective imaging. Clinicians involved in trauma care should be assured that in the published literature and among invested stakeholders there is no deviation in guidance for imaging the pregnant patient after trauma. In circumstances where imaging using ionizing radiation is indicated, stakeholders in trauma services, emergency medicine, radiology, and obstetrics endorse its use without modification of usual care pathways.
Fluoroscopy/Angiography
Angiography and image guided procedures have a well-established role in the treatment of trauma patients. 40 This is particularly apparent in patients with contraindications for surgical management or in those with proven outcome when using image-guided treatment options. Angiographic interventions are usually the primary management technique for active or possible future bleeding from pelvic or solid abdominal vascular injuries, or injuries to the thoracic or abdominal aorta and proximal major branches. 41 In the setting of advanced blunt cerebrovascular injuries, angiography may provide a treatment option for patients that are at high-risk for surgical intervention or unsuitable for conservative management. Angiographic and interventional procedures may also be utilized in cases of drainage or urinary diversion where a combination of cross-sectional imaging (CT, US) may be combined with fluoroscopic techniques to achieve optimum treatment goals. 42
Radiation doses in interventional radiology procedures vary depending on the type of procedure and the area exposed 43 ; however, can quickly exceed radiation levels historically thought to be associated with radiation-induced anomalies.42,44 As such, strategies to reduce fetal radiation exposure should be employed. These include minimizing fluoroscopy time, using low pulse-rate fluoroscopy, avoiding magnification, reducing exposure by utilizing last image hold, minimizing the distance between the patient and receptor, maximizing the distance between the X-ray source and receptor, using appropriate collimation, using a reduced tube current, and avoiding digital subtraction angiography when possible.42,44 The use of a lead apron to reduce the dose to the fetus when not in the direct field of exposure is of limited value as the majority of the dose arises from internal scatter.
Other considerations during angiographic interventions include the medications used during these procedures. As described above, iodinated contrast media is generally considered safe to the fetus; however, other medications such as sedatives and embolic material should be carefully considered prior to use. 45 Additionally, the use of peripheral stents or intracerebral coils sometimes require the use of antiplatelet therapy which is not contraindicated during pregnancy.46,47 If needed systemic anti-coagulants may be challenging to use during pregnancy. This should be taken into consideration and compared with other possible treatment options.42,45
Magnetic Resonance Imaging (MRI)
MRI is not typically used in the initial evaluation of pregnant patients involved in trauma due to long examination times, the need to remove the patient from the acute care setting, and lack of availability. The ACR and the CAR recommend against the use of MRI in the initial assessment of the pregnant trauma patient. Following stabilization, MRI can be used as a problem-solving imaging modality in some specific situations, such as spinal, complex neurological, and soft-tissue injuries. MRI may also have a role in reducing radiation exposure in patients who require follow-up imaging or further evaluation of specific injuries diagnosed at initial presentation, or in stable patients who develop new pain or concerning symptoms after an initially negative evaluation. 13
Preponderance of research studies to date have demonstrated no reproducible harmful effects to either the mother or the developing fetus following exposure to 3 Tesla or weaker magnetic fields used in routine clinical MRI examinations. 25 The primary safety concerns are the heating effects of radiofrequency pulses and the effects of acoustic noise to the fetus. 48 To minimize these potential risks, it is recommended that MRI examinations of pregnant patients are performed at a field strength of 1.5 T or less.
As described above, there is widespread consensus to avoid gadolinium-based contrast agents (GBCAs) in pregnancy, therefore MRI contrast agents should not be routinely administered to pregnant patients. 49 The use of medication to reduce fetal motion is also not recommended. 50
Imaging of Fetus and Obstetrical Complications
A detailed account of fetal imaging in a major trauma setting is outside the scope of these guidelines. Accurate and detailed assessment of fetal injuries is difficult on the maternal abdominopelvic CT performed during initial trauma imaging. Injuries to the gravid uterus and placenta, however, can be broadly assessed.
The mainstay of fetal imaging assessment is obstetric ultrasound. Depending on the severity of trauma and other clinical findings, ultrasound examination can include screening for placental abruption, (presence of a sub-placental/sub-chorionic haematoma), feto-maternal haemorrhage-related anaemia (elevated middle cerebral artery Doppler peak systolic velocity), preterm premature rupture of the membranes (PPROM, presence of oligohydramnios), and preterm birth risk (cervical length assessment). Placental abruption is the most common and significant pregnancy complication of trauma and can be associated with fetal hypoxaemic-ischaemic neurological injury, feto-maternal haemorrhage, and fetal death. 30 However, ultrasound evaluation has low sensitivity for placental abruption, and clinical assessment of features such as uterine contractions, vaginal bleeding, and abnormalities in the fetal heart rate pattern are more reliable. Also, a normal amniotic fluid volume does not rule out PPROM and oligohydramnios does not confirm PPROM, necessitating correlation with clinical findings. A follow-up obstetric ultrasound (or MRI) assessment 2 to 3 weeks after the trauma incident needs to be considered to evaluate for consequences of placental abruption or maternal haemodynamic instability, as well as the possibility of fetal intracranial injury or fetal growth restriction. Overall, fetal injury and uterine rupture occur quite infrequently.
Follow-Up Imaging
The follow up imaging in a pregnant trauma patient is generally a tailor based individualized approach. Diagnostic imaging modalities that do not use ionizing radiation, such as ultrasound and MRI are frequently used for follow-up imaging to effectively reduce the cumulative radiation dose to the fetus after the initial trauma CT. Formal ultrasound can be used to assess fetal status as required and MRI can be used after the initial trauma imaging to follow-up on any known maternal abdominopelvic traumatic injuries, including uterine and placental injuries, as well as superior visualization of the maternal soft tissue injuries. However, after appropriate consideration, certain injuries may still require repeat evaluation with CT.
Footnotes
Acknowledgements
The authors would like to thank Dr. Gilles Soulez, Montréal, Québec for his comments on the interventional radiology section of the practice guideline. The authors would also like to thank the members of the Canadian Emergency, Trauma and Acute Care Radiology Society, and the further members of Canadian Association of Radiologists and the Canadian Association of Emergency Physicians, who took the time to provide their feedback and peer review during the drafting of these guidelines.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Venu Jain reported receiving honoraria for speaker or moderator engagements from Ferring Pharmaceuticals and Bayer. Dr. Jain has previously been a member of the advisory board at Ferring Pharmaceuticals. No other authors declared potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.