
Abstract
Introduction
Breast imaging is a critical component of diagnostic radiology, encompassing a range of techniques essential for the early detection, diagnosis, and treatment of breast diseases, particularly breast cancer. With the rising incidence of breast cancer globally, there is an increasing emphasis on the quality and comprehensiveness of breast imaging training for radiologists. 1 Despite the growing demand for radiologists comfortable interpreting breast imaging, the workforce supply remains insufficient. A 2009 study in the United States projected that the limited number of graduating radiologists specializing in breast imaging would lead to a diminished workforce over the next 20 years, with similar issues projected in Canada.2,3 Although interest in breast imaging fellowship training among Canadian residents has increased over the past decade, this field still attracts fewer trainees compared to other subspecialties, with between 1% and 7% of trainees pursuing fellowship training in breast imaging.4,5 Considering this shortage, breast imaging is an important part of residency training and encompasses a large component of any radiology practice.
In Canada, the structure and content of diagnostic radiology residency programs vary across provinces, influencing the extent and quality of breast imaging exposure that residents receive. The Royal College of Physicians and Surgeons of Canada (RCPSC) outlines the competencies required for radiology residents, but there is variability in the implementation of these standards across different residency programs, accentuated by the implementation of the Competence By Design (CBD) program in 2022. 6 Studies have shown that structured breast imaging training, including hands-on procedural experience and multidisciplinary collaboration, enhances residents’ diagnostic accuracy and procedural skills. 7 However, disparities in training opportunities can lead to inconsistencies in the readiness of radiologists to independently perform breast imaging procedures.
This survey aims to capture detailed information about the structure and content of breast imaging training in Canadian diagnostic radiology residency programs. By identifying gaps and areas of variability, the survey aims to provide insights that can inform future curriculum development and policy recommendations to standardize breast imaging education, ultimately improving the quality of care for patients with breast disease.
Methods
Following ethics approval, a 45-question survey was created and distributed to all 16 diagnostic radiology residency program directors at Canadian residency programs via email using the secure online survey software platform SurveyMonkey.
A consent form preceded the survey where respondents provided consent for data collection of their responses which would subsequently be presented in aggregate. The survey (Supplemental Appendix) consisted of 3 parts. The first part collected demographic information about the respondents’ residency program and breast imaging curriculum. The second part assessed the incorporation of other learners (fellows and medical students) in breast imaging at the respondents’ institution. The third part collected information on the broader curriculum and the subspecialties of program and departmental leadership to evaluate if the subspecialty of leadership correlated with the program’s breast imaging curriculum or resident experience.
The survey was distributed via email by the coordinator for national diagnostic radiology residency program directors in Canada. Survey responses were collected over a 2-month period from March 4th, 2024 through May 4th, 2024. Reminder emails were sent at 2-week intervals. Descriptive analysis was used to analyze survey responses. Fisher Exact tests were performed to compare survey responses to the subspecialty of practice of the survey respondent and program size.
Results
Twelve of the 16 (75%) diagnostic radiology residency program directors across 7 provinces responded.
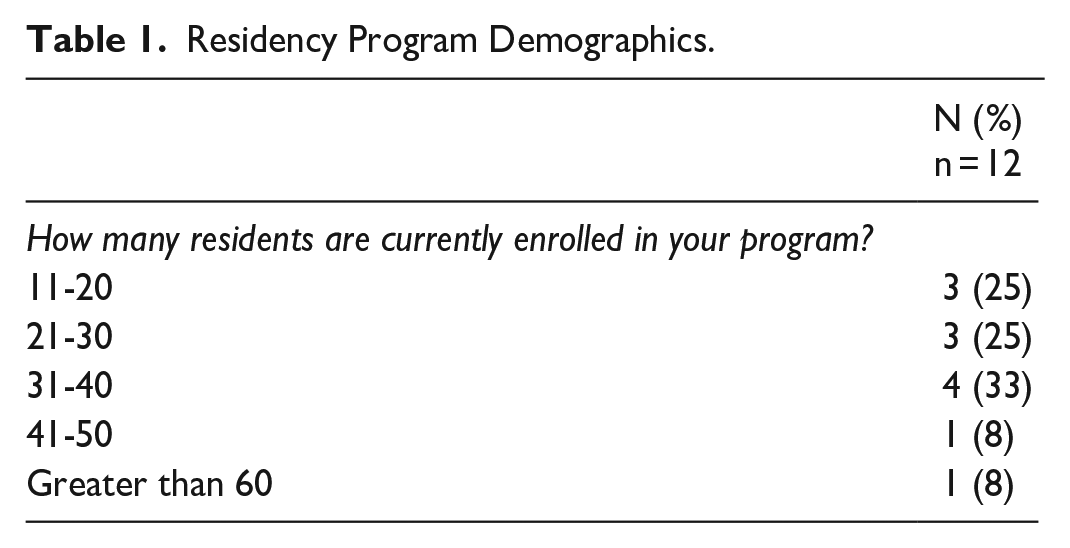
Survey responses reveal significant variability in program structures and resources. Most programs have between 11 and 40 residents enrolled in their program (Table 1). All programs provide 4 months of mandatory breast imaging training as per the RCPSC requirements. However, available elective time varies between programs; 8/12 (67%) programs offer 3 or fewer elective months, while 3/12 programs (25%) offer more than 5 months of elective time. One program stated elective time was variable. Residents are typically scheduled for their first breast imaging month in postgraduate year (PGY)-2 (5/12, 42%) or PGY-3 (7/12, 58%) and most complete their final breast imaging rotation in PGY-5 (11/12, 92%).
Residency Program Demographics.
Most programs (75%, 9/12) provide residents with experience interpreting screening mammography, often beginning in PGY-2 or PGY-3; however, 25% of programs (3/12) do not (Figure 1). Exposure to diagnostic breast imaging is provided across all 12 programs, with experience often beginning in PGY-2 or PGY-3 (10/12, 83%; Figure 1).
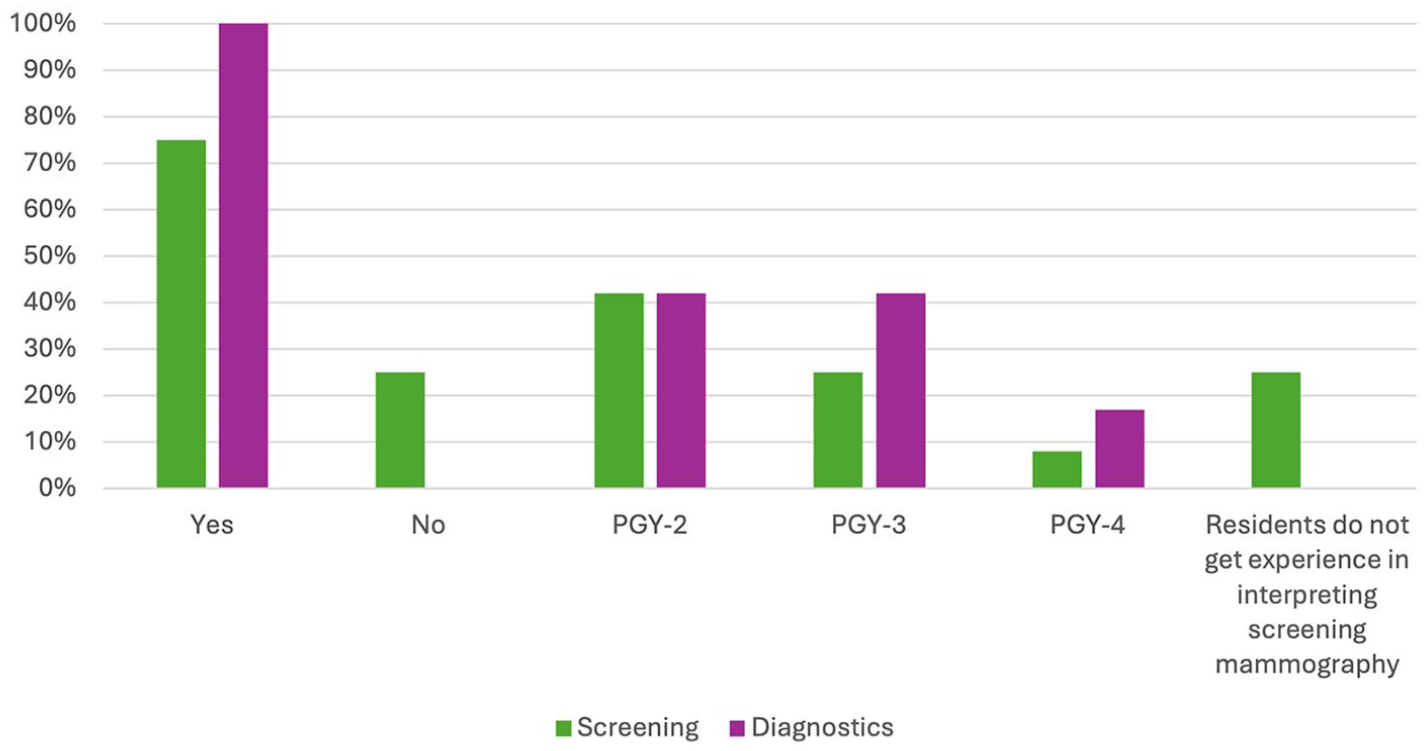
Resident exposure to screening mammography and diagnostic breast imaging.
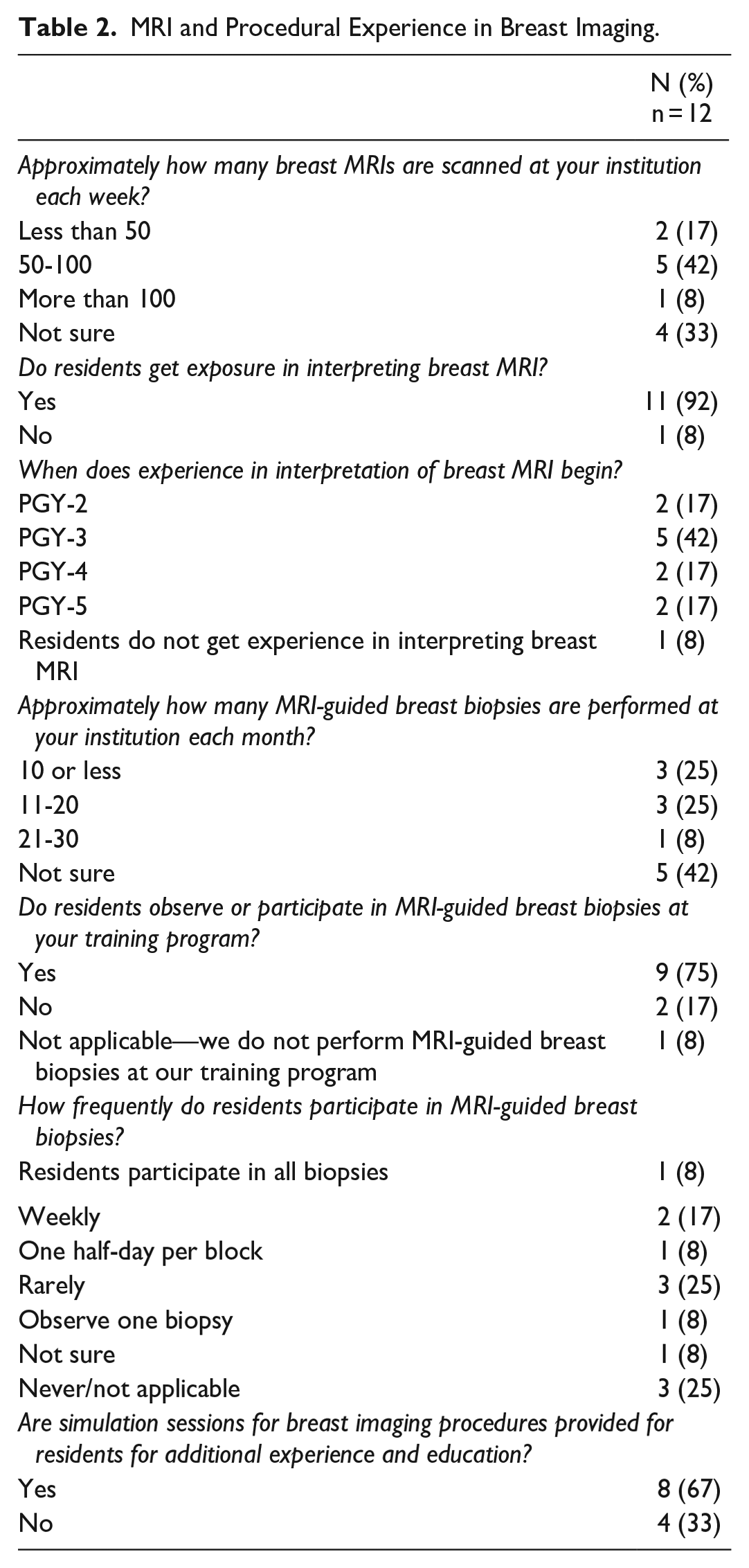
Experience with ultrasound-guided and stereotactic-guided procedures varies, beginning between PGY-2 and PGY-4; however, 67% (8/12) of programs state that residents rarely or never participate in MRI-guided breast biopsies (Table 2, Figure 2). Qualitative comments left by survey respondents indicate that residents usually observe one MRI-guided biopsy, however, conflicts with didactic teaching schedules and the presence of fellows can limit opportunities for exposure. While some program directors indicate that breast imaging fellows enhance the learning experience of residents through hands-on teaching and provided lectures, procedural opportunities for residents are negatively impacted by the presence of fellows in 25% (3/12) of programs. Simulation sessions may bridge this gap but are only offered by 33% (4/12) of responding programs. One respondent indicated that a simulation course was currently under development.
MRI and Procedural Experience in Breast Imaging.
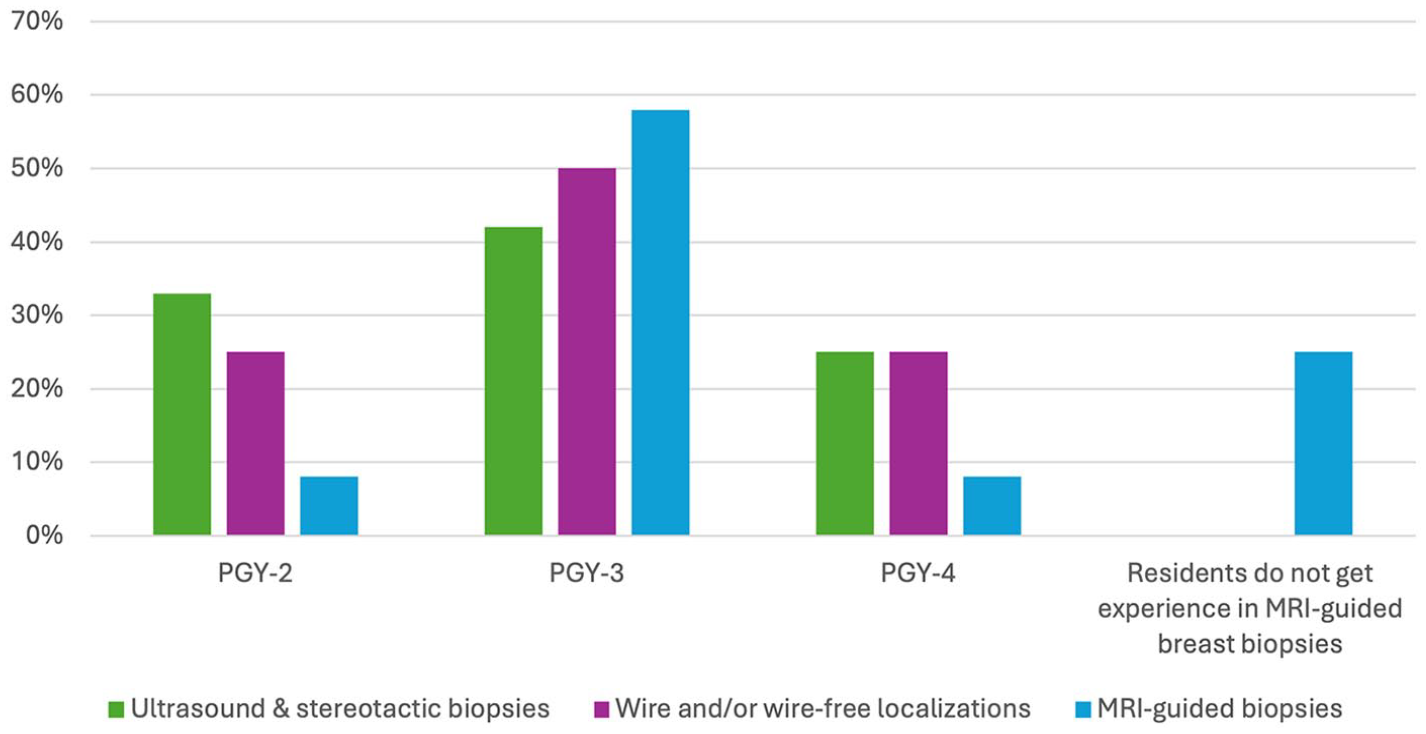
Resident experience to breast imaging procedures.
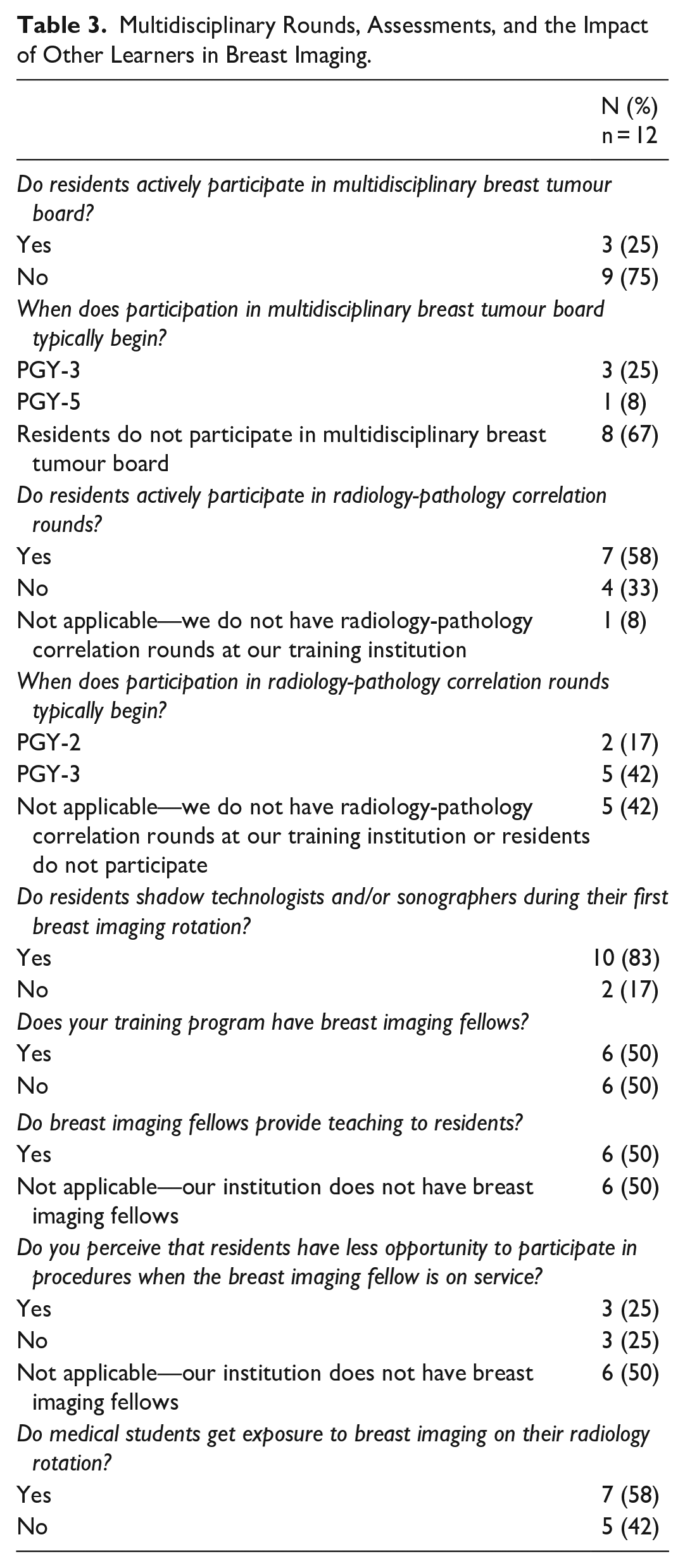
Integration of residents into the multidisciplinary facets of breast imaging also varies between programs. Most programs do not involve their residents in multidisciplinary breast tumour boards (75%, 9/12), although more than half of respondents indicate that residents at their program participate in radiology-pathology rounds, if offered at their institution (58%, 7/12; Table 3).
Multidisciplinary Rounds, Assessments, and the Impact of Other Learners in Breast Imaging.
The didactic teaching program for breast imaging varies across residency programs, although nearly all programs offer regular breast imaging didactics throughout the year for all residents in the program (Figure 3). Half of participating programs (50%, 6/12) host a breast imaging journal club (Figure 3). Free-text answers were provided by some participants, highlighting variations in teaching program structure. For example, one program offers a visiting professor lecture in breast imaging every 2 to 3 years, while other breast imaging didactics are offered as part of the university division rounds or academic half-day cycle. Another program integrates a breast imaging station in their yearly in-training oral examination and their objective structured clinical examinations (OSCEs) held twice yearly.
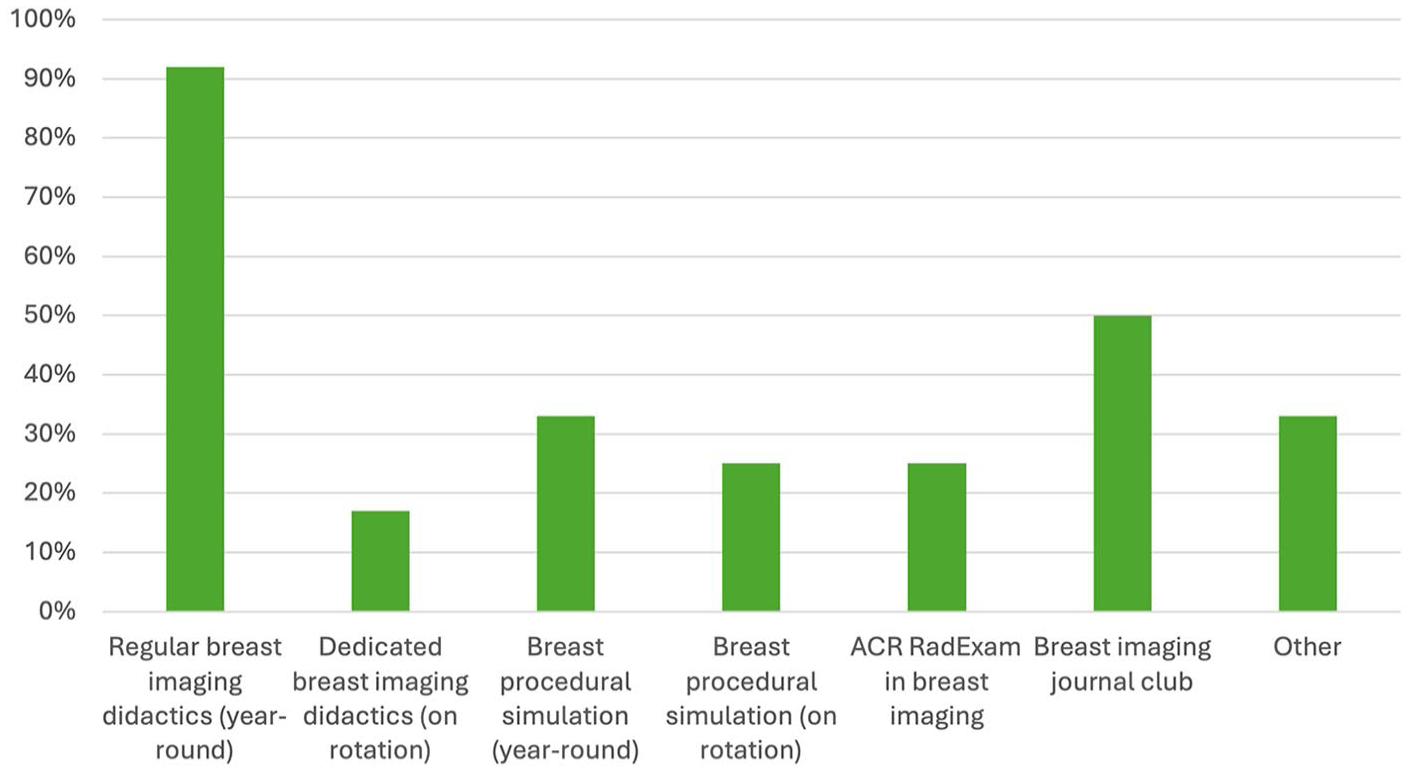
Breast imaging didactics and learning opportunities.
Assessment methods across programs also vary, although all use subjective evaluations from fellows and staff radiologists at minimum (Figure 4). Only 17% (2/12) of programs require a post-rotation test and 33% (4/12) have a required case log for residents to complete.
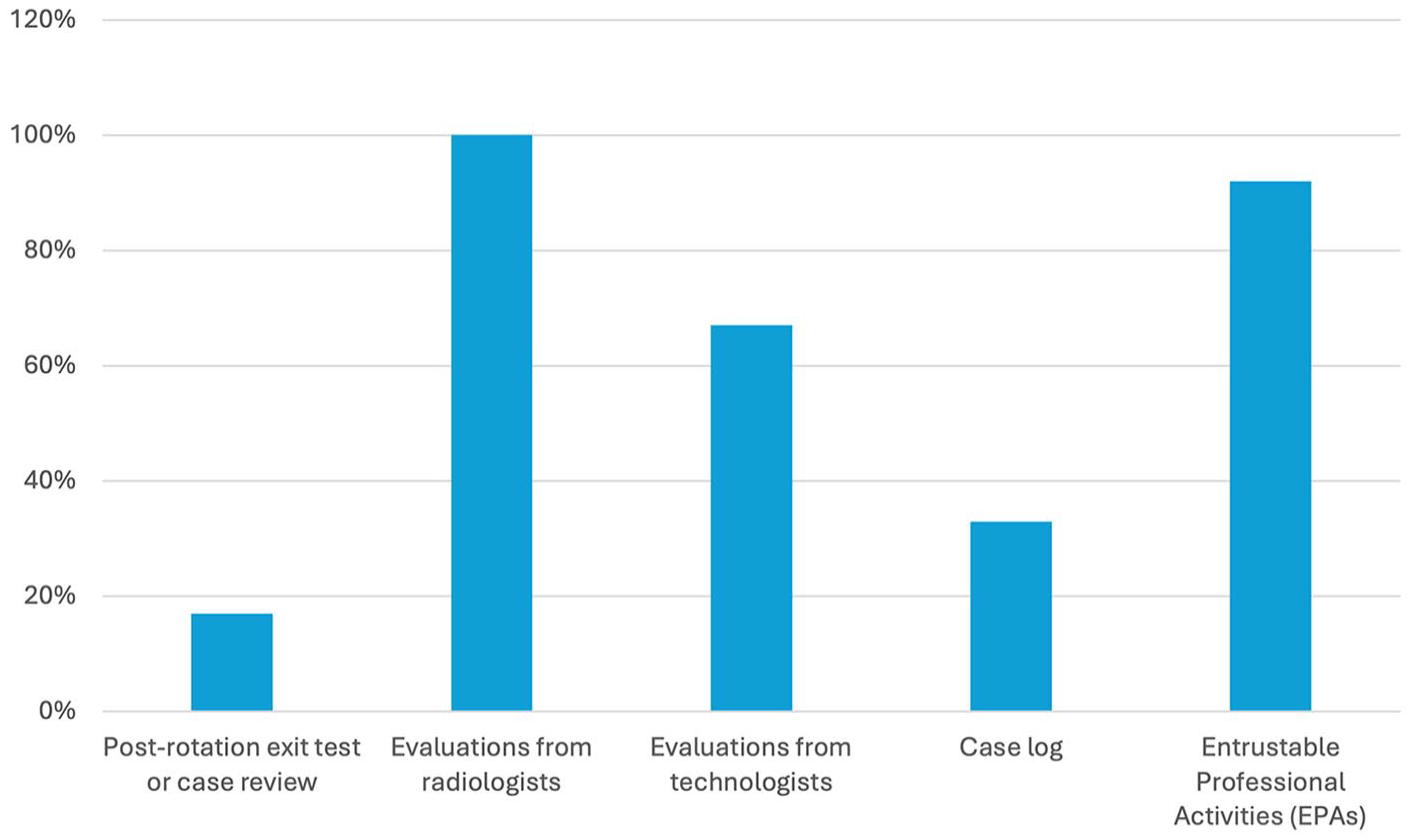
Method of resident evaluation in breast imaging.
The presence of breast imaging fellows within a training program is perceived in most programs to hinder residents’ ability to gain procedural experience (75%, 3/12; Table 3). One of the 3 programs which do not perceive this issue outline a detailed daily schedule for each learner to avoid overlap and conflict, while another program finds that the presence of fellows enhances the residents’ learning experience.
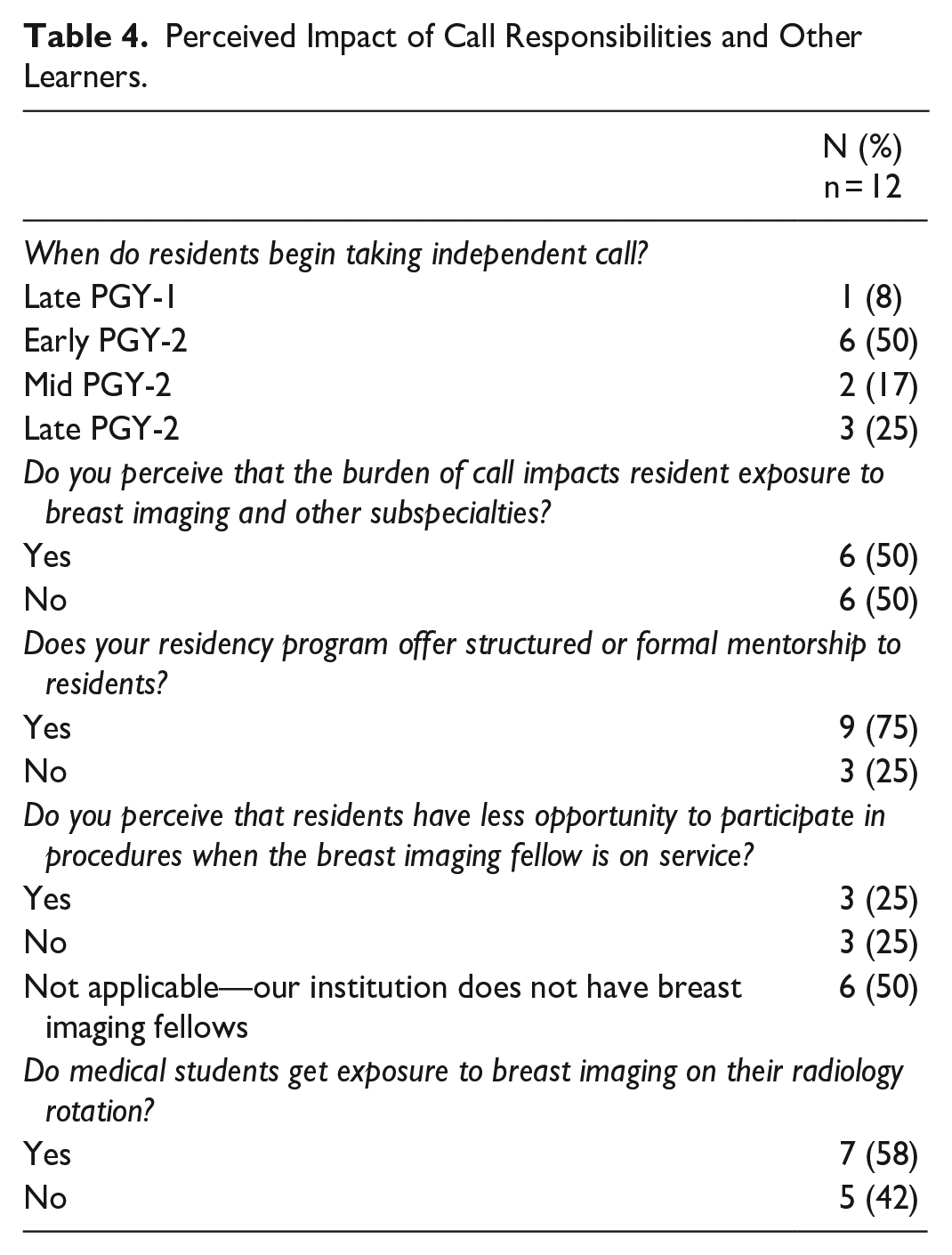
The timing of the first breast imaging rotation is comparable to other subspecialties including nuclear medicine, cardiac imaging, interventional radiology, and pediatric radiology (Figure 5). Half of participating program directors (50%, 6/12) indicate that the call schedule may impact a resident’s exposure to and experience during their breast imaging rotation and other subspecialty rotations, particularly the impact of post-call days (Table 4).
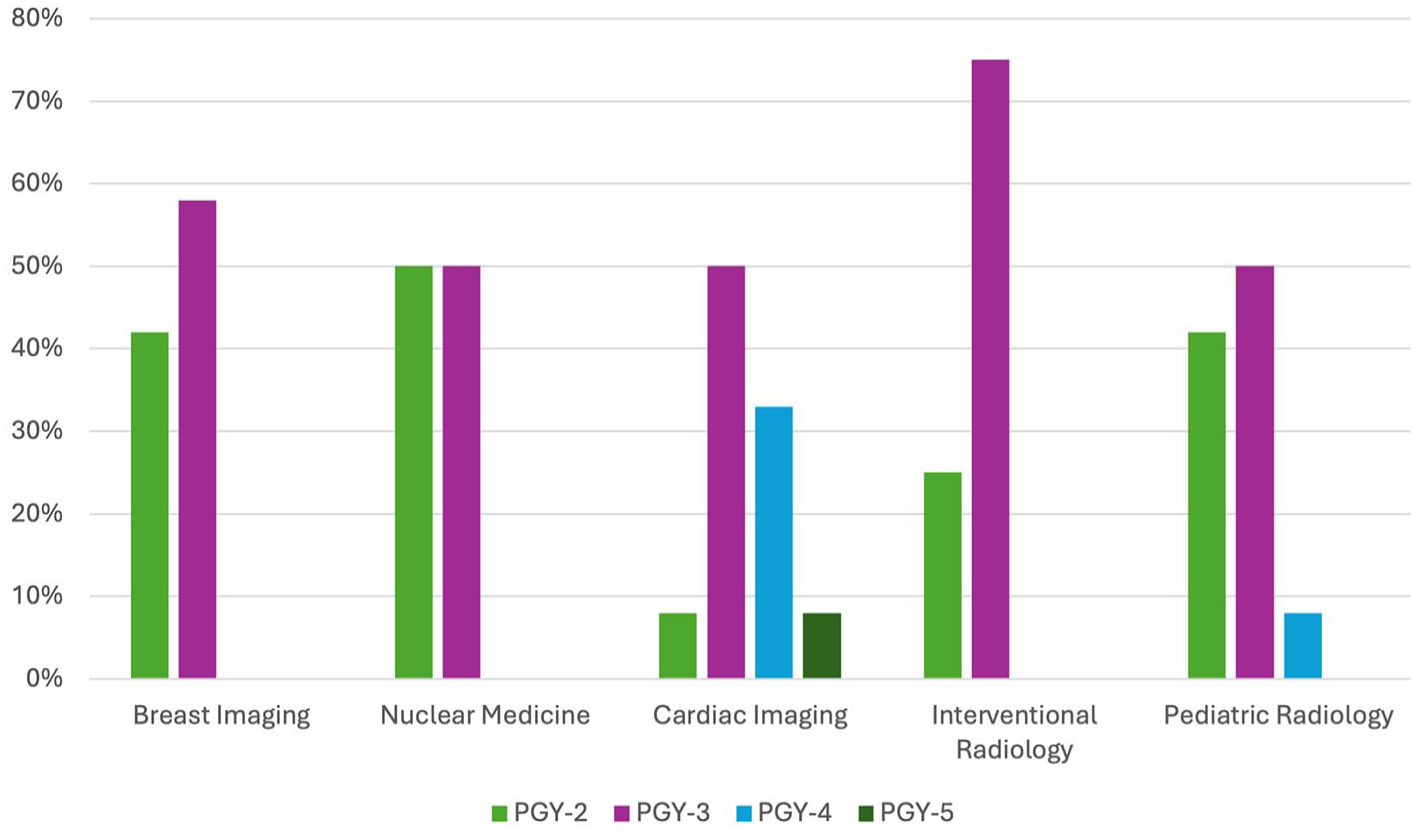
Timing of resident exposure to various radiological subspecialties.
Perceived Impact of Call Responsibilities and Other Learners.
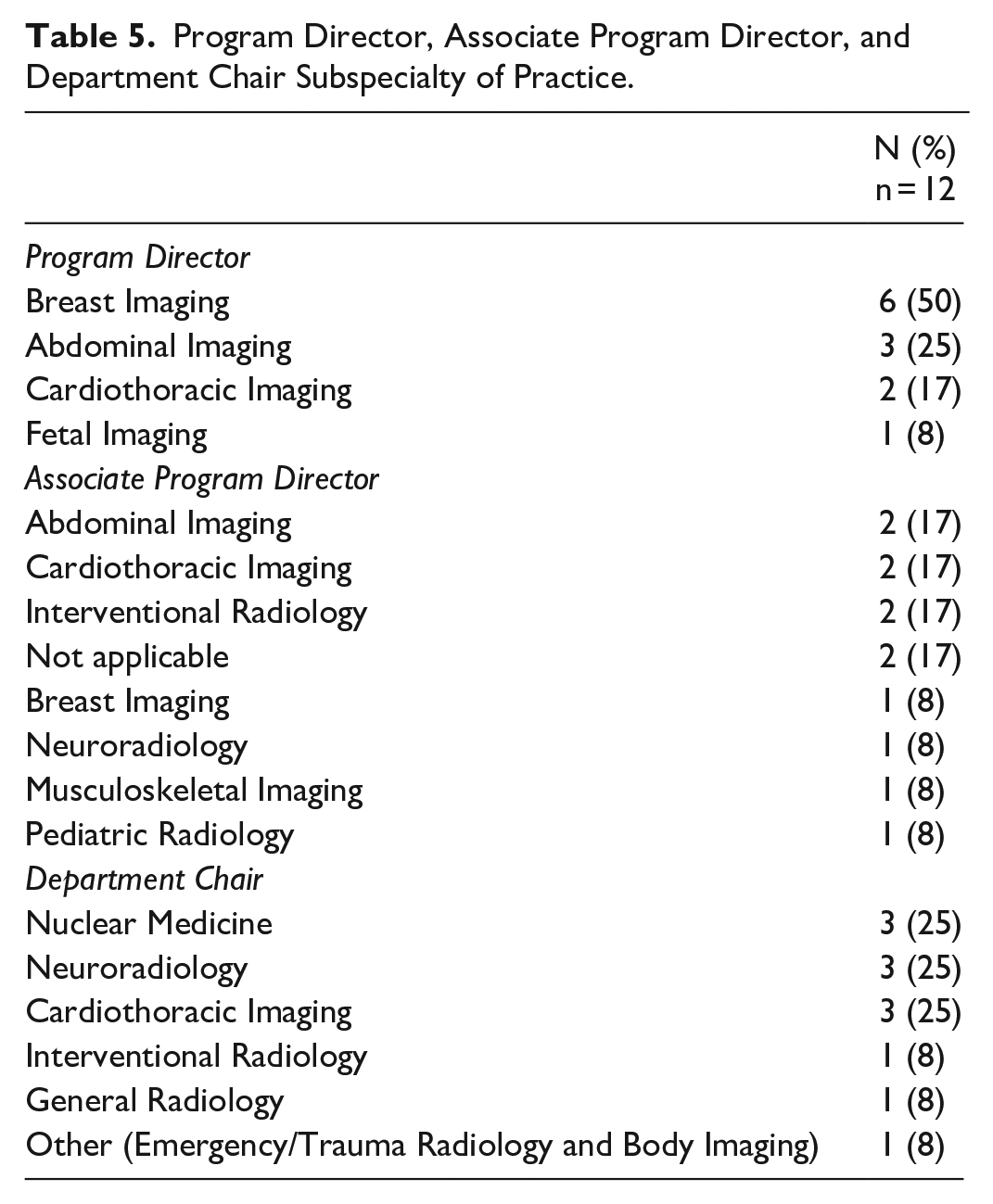
The subspecialty of practice of the program director, associate program director, or department chair were not significantly associated with any particular training difference (P > .05; Table 5).
Program Director, Associate Program Director, and Department Chair Subspecialty of Practice.
Discussion
The results of this survey demonstrate the variability in structure and exposure to breast imaging between residency programs across Canada, which can significantly impact residents’ preparedness and interest in the field. 8 Ensuring a comprehensive standardized training curriculum is essential to maintain high standards of care and attract more trainees. Furthermore, emphasizing and incorporating the model of multidisciplinary care of breast imaging into the residency curriculum may highlight the dynamic and collaborative nature of the field.
Breast imaging remains a vital component of diagnostic radiology for detecting and managing breast diseases which includes breast cancer. Despite its critical role, breast imaging faces challenges, including workforce shortages and variability in radiology training. 8 The current and projected decline in breast imagers across North America highlights the urgency to address the aforementioned issues. 2
Several factors contribute to the variability in breast imaging exposure among radiology residents, including the number of dedicated breast imaging rotations, availability of elective opportunities, and access to advanced imaging modalities. Additionally, the presence of breast imaging fellows, the extent of multidisciplinary involvement, and the availability of simulation sessions further influence the training experience. Previous research highlights the need for a standardized approach to ensure comprehensive breast imaging education across all residency programs. 9 Early clinical exposure, a comprehensive curriculum, and mentorship are essential for recruiting trainees to any subspecialty in radiology. A 2021 Canadian survey highlighted the key factors impacting interest in breast imaging including perceptions of repetitiveness (which was associated with decreased interest) and the appeal of procedures (which was associated with increased interest). 2 Lower relative remuneration under some provincial models, the perceived increased medicolegal risk, and the perception of less flexibility to work remotely may also deter trainees from fully pursuing breast imaging as a career option. 8 Mandatory requirements for minimum annual mammography reads and increased scrutiny from peer review under the current national accreditation program may also deter residents from pursuing breast imaging.
Early exposure to breast imaging, and addressing training inadequacies, were suggested solutions to enhance interest in the field. Furthermore, ensuring a diverse workforce in breast imaging departments through engaging both male and female radiologists, can encourage trainees to seek focused mentorship.
Standardizing and promoting breast imaging education in residency, rather than deferring it to a fellowship curriculum, is vital given that all aspects of breast imaging (including screening, diagnostic breast imaging, and intervention) are a significant component of any radiology practice. Many radiologists interpreting breast imaging do not have formal fellowship training in breast imaging and thus rely on their breast imaging exposure and education from their residency training. This is of particular importance in rural or remote locations and in community practices. Furthermore, fostering an interest in breast imaging amongst those trainees who go onto pursue subspecialty training in breast imaging is paramount to ensure appropriate training for future generations of radiologists and to promote ongoing excellence in research, innovation, and leadership in the field. 2
The shortage of radiologists comfortable interpreting breast imaging across the country can be in part due to suboptimal exposure and training during residency, which has downstream effects on the field as a whole. Inconsistent training may lead to increased recall rates, limited adoption of newer technologies such as digital breast tomosynthesis and contrast-enhanced mammography, and scarcity of professionals advocating for systemic change including supplemental screening and updated billing codes. Furthermore, a shortage of radiologists comfortable practicing breast imaging can result in increased referrals to tertiary breast imaging centres, potentially contributing to prolonged wait times and increased burnout amongst academic breast imaging radiologists, which may in turn exacerbate the workforce shortage.
Comprehensive breast imaging education in residency may also support improved clinical outcomes. Previous studies have found a steep learning curve and decline of false positive callbacks from screening mammography in the first 3 years of practice amongst radiologists without fellowship training in breast imaging. 10 This sharp decline could in part be mitigated by a more comprehensive and standardized curriculum in breast imaging during residency training. Focused but separate education on screening mammography versus diagnostic breast imaging is necessary given the distinct skillsets and competencies required. 11
The implementation of CBD may further expand disparities in radiology residency programs across the country as more flexibility is permitted with individual programs deciding how to integrate various subspecialties. Prior to the implementation of CBD, residents were required to complete 4 mandatory breast imaging rotations 12 ; after CBD was implemented in 2022, programs are permitted greater flexibility, with the RCPSC suggesting 4 blocks during core training. 13 There may also be less emphasis on breast imaging teaching for residents both at the workstation and during didactics given the relatively low yield of breast imaging questions on the RCPSC examination compared to other subspecialties. Programs should emphasize the importance of being fully engaged in all rotations, regardless of personal subspecialty interests, as many residents may be expected to interpret breast imaging in a community practice setting. Additionally, consideration should be given to the time of breast rotations throughout residency. Some residents may not have sufficient exposure to breast imaging prior to applying to fellowship programs, which may impact their choice of subspecialty. Programs should ensure adequate exposure to all subspecialties, including breast imaging, prior to submission of fellowship applications, particularly in subspecialties with workforce shortages. 14
Addressing these challenges requires a focus on the root of the issue: lack of standardized breast imaging training during residency. Through enhancing training standards, focusing on early exposure to breast imaging, and providing mentorship, residency programs can produce trainees who are both skilled clinically and who are motivated to drive policy change. 2 Discussing these topics during curriculum reform can help ensure that future radiologists are better equipped to meet the demands of breast imaging and elevate patient care. Providing this multifaceted experience in breast imaging is vital, not only for trainees seeking to subspecialize in breast imaging, but also for those who may go on to general community or rural practices, where access to resources can be limited.
We acknowledge several limitations. The small sample size due to the inherent low number of diagnostic radiology residency programs in Canada limits the study’s power and assessment of statistical significance of survey responses. Furthermore, the response rate of less than 100% does not entirely represent the experiences in training programs across Canada as some provinces with a single residency program were not represented. As with all survey studies, selection and response bias plays a role, half of the participating program directors self-identified as breast imaging radiologists. We also acknowledge the subjective nature of some of the survey questions and answers which reflect the perceptions of the participating program directors. We also did not address any perceived gender bias in breast imaging. Finally, as program structure varies across the country, there is the potential for limited or inconsistent involvement of program directors in the specifics of the day-to-day experiences of residents in breast imaging, particularly at institutions with multiple training sites.
Future work should include resident surveys to further understand career planning and subspecialty choices in the evolving radiology landscape as well as perceived readiness for general practice based on current breast imaging training. The effect of perceived differential remuneration across specialty choices can also be considered. These findings may help inform future curricular development to promote the field of breast imaging earlier in training and to better prepare graduating residents for general practice in breast imaging.
In conclusion, the results of our survey demonstrate marked variability in breast imaging training and evaluation across Canadian diagnostic radiology residency programs. These inconsistencies in training and evaluation may have implications on the ongoing shortage of breast imaging radiologists, increased screening recall rates, and low uptake of newer technologies such as digital breast tomosynthesis. Furthermore, limited exposure to breast imaging in training may also result in a smaller pool of advocates for more widespread access to advanced breast imaging technologies and updated provincial fee codes. Improving standardization of breast imaging training for Canadian diagnostic radiology residents in line with the requirements set out by the RCPSC may help tackle these issues and forge a path forward for breast imaging across Canada.
Supplemental Material
sj-docx-1-caj-10.1177_08465371251344246 – Supplemental material for Insights From a National Survey on Gaps and Opportunities for Curriculum Improvement in Breast Imaging Education in Canadian Radiology Residency Programs
Supplemental material, sj-docx-1-caj-10.1177_08465371251344246 for Insights From a National Survey on Gaps and Opportunities for Curriculum Improvement in Breast Imaging Education in Canadian Radiology Residency Programs by Kaitlin M. Zaki-Metias, Sri Sannihita Vatturi, Aleena Malik, Hayley McKee, Silma Solorzano, Jean M. Seely, Supriya Kulkarni, Zina Kellow and Raman Verma in Canadian Association of Radiologists Journal
Footnotes
Acknowledgements
The authors would like to thank and acknowledge Dr. Mona El-Khoury, Dr. Carolyn Flegg, Dr. Charlotte Yong-Hing, and Christie Barbesin for their contributions to development of the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.