
Abstract
Introduction
Endometriosis is a gynecological condition impacting premenopausal women, 1 causing a range of chronic intermittent symptoms requiring multiple clinical and imaging evaluations. It affects 10% of women and individuals assigned female at birth and up to 50% of those individuals who are sub-fertile. Symptoms include severe pain, dysmenorrhea, dyspareunia, dysuria, subfertility, and fatigue, resulting in significant patient morbidity. 1-3 The challenge in managing endometriosis is due to its wide range of vague clinical symptoms and a lack of uniform knowledge of imaging options and interpretative expertise. 4 Nevertheless, this health problem is being increasingly recognized over time.
While laparoscopic exploration used to be the diagnostic gold standard for endometriosis, surgery is not devoid of risks 1,5 and may be of limited availability. Furthermore, it cannot be used as a follow-up modality. Therefore, a combination of clinical and imaging evaluation for monitoring treatment response is the current recommendation for these patients. 5 Diagnostic imaging plays an essential role in diagnosing and managing patients, especially in cases of deep endometriosis. Advanced pelvic ultrasound and magnetic resonance imaging (MRI) are often used to confirm the diagnosis, to follow up for known disease, and for pre-surgical planning. As a complex disease involving many pelvic organs, the imaging evaluation, either by advanced pelvic ultrasound or MRI, has to be performed and/or interpreted by a trained radiologist or gynecologist/sonologist (particularly in the case of ultrasound) to provide the information required to facilitate patient management.
The CAR Endometriosis working group developed a national cross-sectional survey to inform forthcoming practice guidelines for endometriosis MRI and advanced pelvic ultrasound. 9 This survey aimed to collect information about current practice patterns across Canada regarding endometriosis imaging.
Subjects and Methods
The working group developed the survey based on the best available information consisting primarily of comments and expert opinions, as there was no validated radiology questionnaire on the subject. All radiologists currently in practice in Canada and members of CAR were eligible to participate. The consent to participate was based on the completion of the survey.
The survey was available in English and French-language and comprised 36 questions, most of which were multiple-choice. In addition, many questions had the option to select “other” with an open box to allow open-ended answers. The questionnaire was distributed electronically through communication channels of the CAR, and the survey was available for 37 days through SurveyMonkey (SVMK Inc.) Platform. As per the standard CAR process for surveys of members related to practice patterns and quality assurance, Institutional review board approval was waived.
The questionnaire was anonymous, and no financial incentives were given to participants. The target population was radiologists who report or plan to report pelvic MRI and advanced pelvic ultrasound for evaluation of endometriosis. The participants were allowed to leave questions unanswered, or they would be led to specific parts of the survey based on their interest/expertise in pelvic MRI and or advanced pelvic ultrasound. The participants had 37 days to answer the survey. Follow-up email reminders to complete the survey were sent on June 1st, 7th and 14th. The survey was closed on June 28th, 2022. Descriptive statistics were summarized, and the data was managed with Excel for Windows software (Microsoft).
Results
The full report of all survey results is available in the supplementary appendix to this article.
Demographics
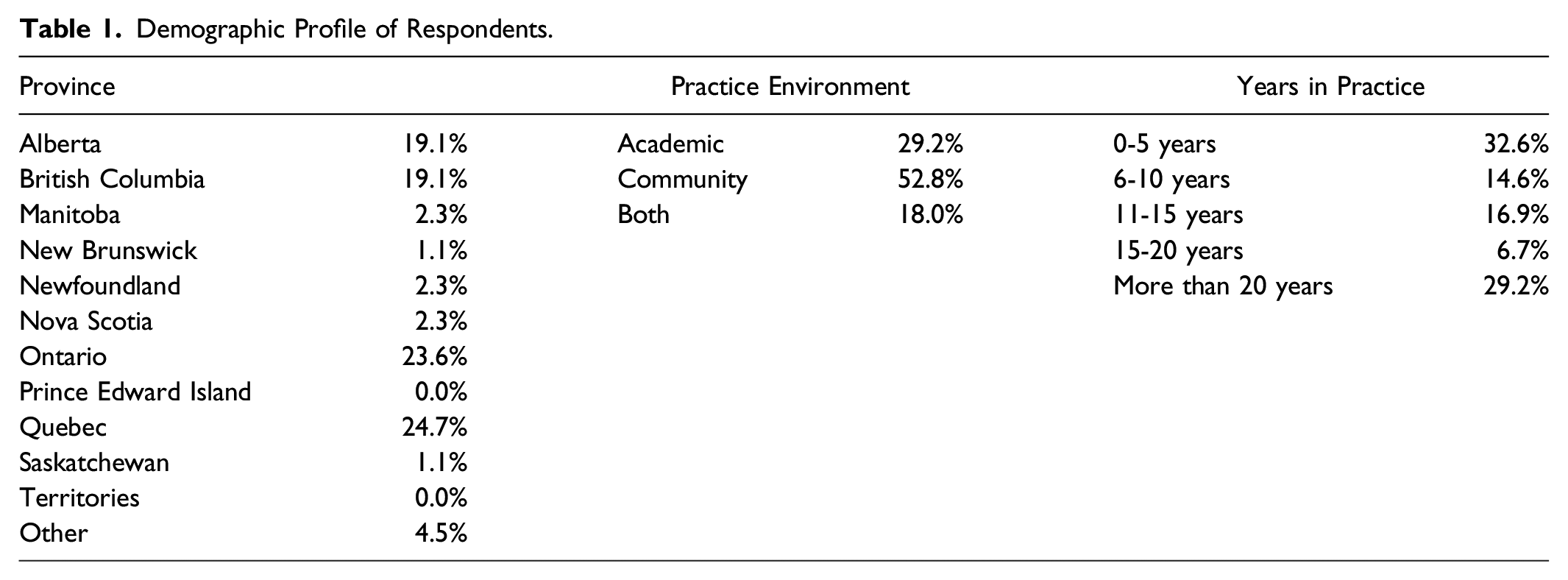
Demographic Profile of Respondents.
Advanced Pelvic Ultrasound for Endometriosis Results
When asked if the radiologist or their institution performed advanced pelvic ultrasound for diagnosis, staging, and follow-up of pelvic endometriosis, only 33 of the 89 participants answered affirmatively (38%). Of those, 12 (36%) received their training during residency, 11 (33%) during the fellowship, 9 (27%) had hands-on training from an expert at their institution, 5 (15%) had CME training, 8 (24%) did not receive any training, and 2 (6%) answered “other” type of training as non-CME training, personal reading, or their own learning technique.
Regarding what format of training in advanced pelvic ultrasound for endometriosis the participants would like, 27/89 participants replied (30%). 41% (11/27) preferred a workshop format, 74% (20/27) web-based learning, and 15% (4/11) chose “other,” with open-ended answers stating they would like both or none. 39% of respondents indicated that they would be interested in being trained within the next 12 months, 8/31 (26%) within 12-24 months, 2/31 (6%) within 24-36 months, and 9/31 (29%) were not interested in seeking additional training related to advanced pelvic ultrasound for endometriosis.
Of those who already performed advanced pelvic ultrasound for endometriosis (33/89), most have been performing the procedure for less than 5 years (63%; 17/27), and only 5 of 27 respondents (18.5%) over 6 years (Figure 1). Number of years performing advanced pelvic ultrasound for endometriosis.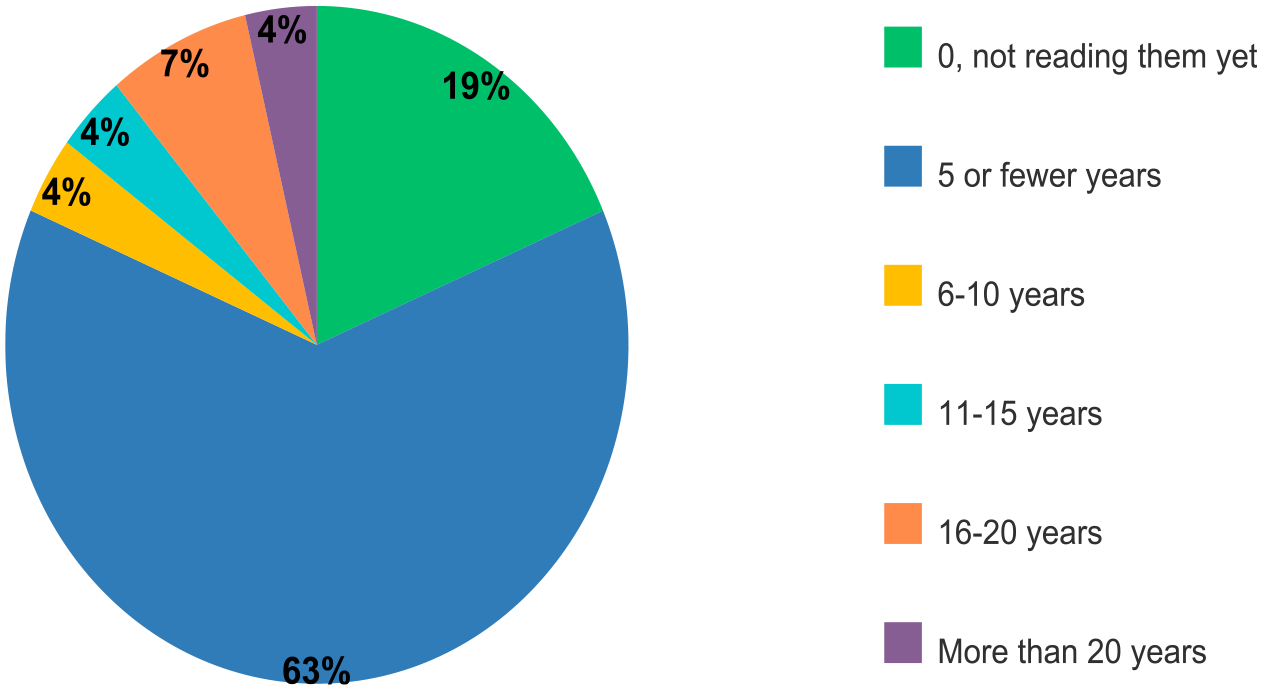
Advanced Pelvic Ultrasound Practice Structure
Of the respondents who answered that their institutions currently perform advanced pelvic ultrasound for endometriosis, roughly half 14/27 (52%) were performed by radiologists, 10/27 (37%) each by gynecologists and sonographers and 9/27 (33%) were performed by both sonographer and radiologists.
In terms of case volumes, 67% (18/27) of respondents who perform advanced pelvic ultrasound for endometriosis interpret/perform 0-5 studies per week. Only one respondent reported interpreting/performing more than 50 cases per week.
In most institutions where advanced pelvic ultrasound for endometriosis is performed, the requisitions come from gynecologists, either from the same institution (70%) or outside the institution (59%). Only 8 of the 27 answers stated the request would come from primary care physician (29%). No specific answers were given when “other” was chosen (Figure 2A). (A) Source of referrals for advanced pelvic ultrasound for endometriosis. (B) Percentage of referrals for advanced pelvic endometriosis meeting particular criteria.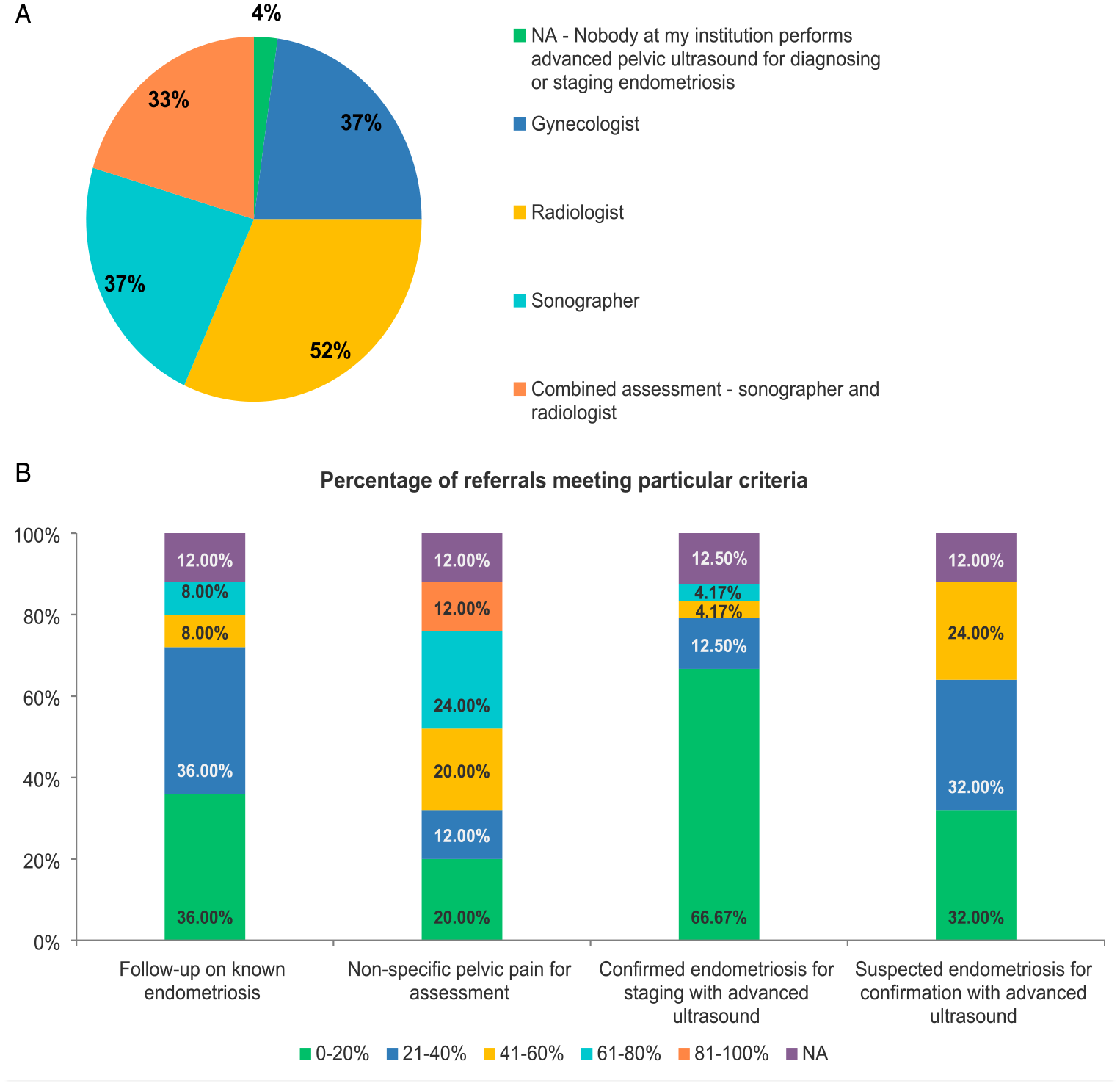
The indications for the participants’ requests for advanced pelvic ultrasound for endometriosis were usually multifactorial and are illustrated in Figure 2B.
At most of the participants’ institutions, advanced pelvic ultrasound for endometriosis is scheduled for a time slot of 30-45 minutes (17/26; 65%).
Pelvic Endometriosis MRI Results
Fifty-five of seventy-seven respondents (70%) stated they currently interpret pelvic endometriosis MRI, while 24/77 (30%) did not. Regarding interest in undergoing additional training in pelvic endometriosis MRI, most participants would prefer a web-based self-directed course (36/77; 47%) or a live-web course (30/77; 40%). In addition, most participants would be interested in training within the next 12 months (34/77; 43%), while 37% (29/77) were not interested in additional training.
Regarding experience (in years) reading pelvic MRI for endometriosis, 30% (24/79) had 1-5 years experience, 16% (13/79) had 6-10 years, 32% (25/79) did not interpret these MRIs and approximately 22% (17/79) had more than 10 years of experience. (Figure 3). Time (in years) respondents have been reading pelvic endometriosis MRI.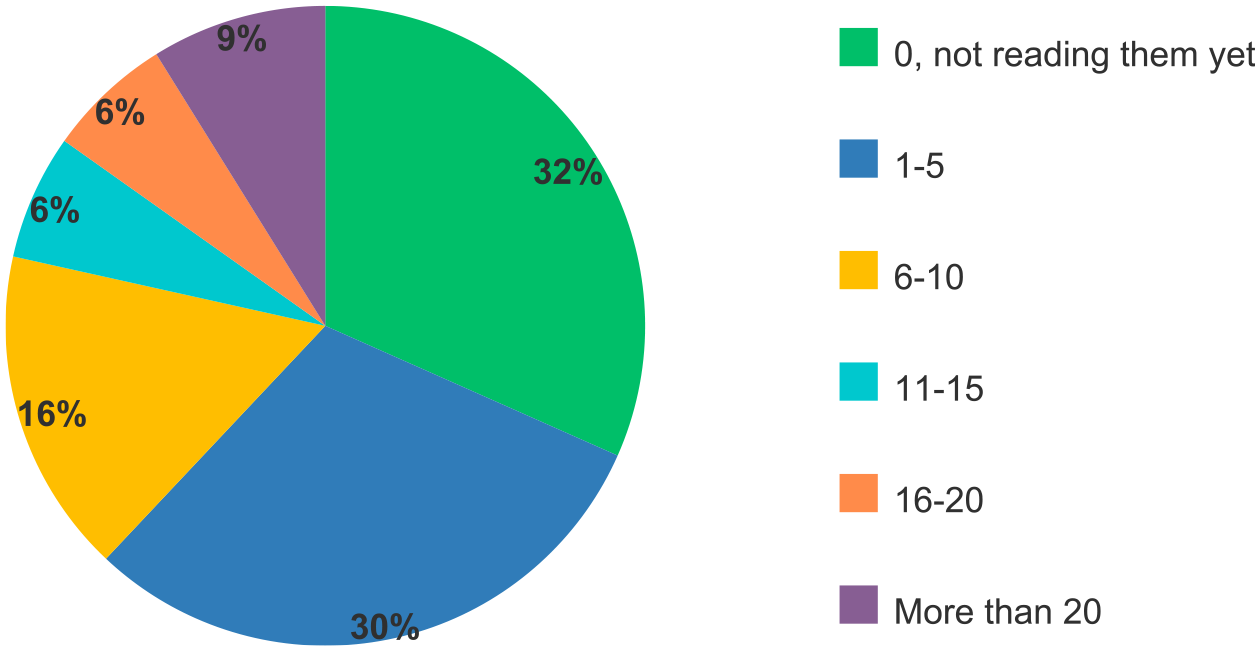
Pelvic Endometriosis MRI Practice Structure
53 responses were obtained regarding number of pelvic MRIs for endometriosis performed per week at the participants’ institutions, with the most common answer being 0-5 cases per week (47%; 25/53), followed by between 6 and 10 cases (17%; 9/53).
In the majority of the cases, requests to perform MRI for endometriosis originated from a variety of sources in most institutions. One respondent (1.89%; 1/53) wrote that almost zero imaging dedicated to endometriosis is done at their imaging facility, and for most of the cases, the patients undergo laparoscopic surgery (without prior imaging) to evaluate the extent of the disease (Figure 4A). (A) Sources of referrals for endometriosis MRI. (B) Percentage of referrals for endometriosis MRI meeting particular criteria.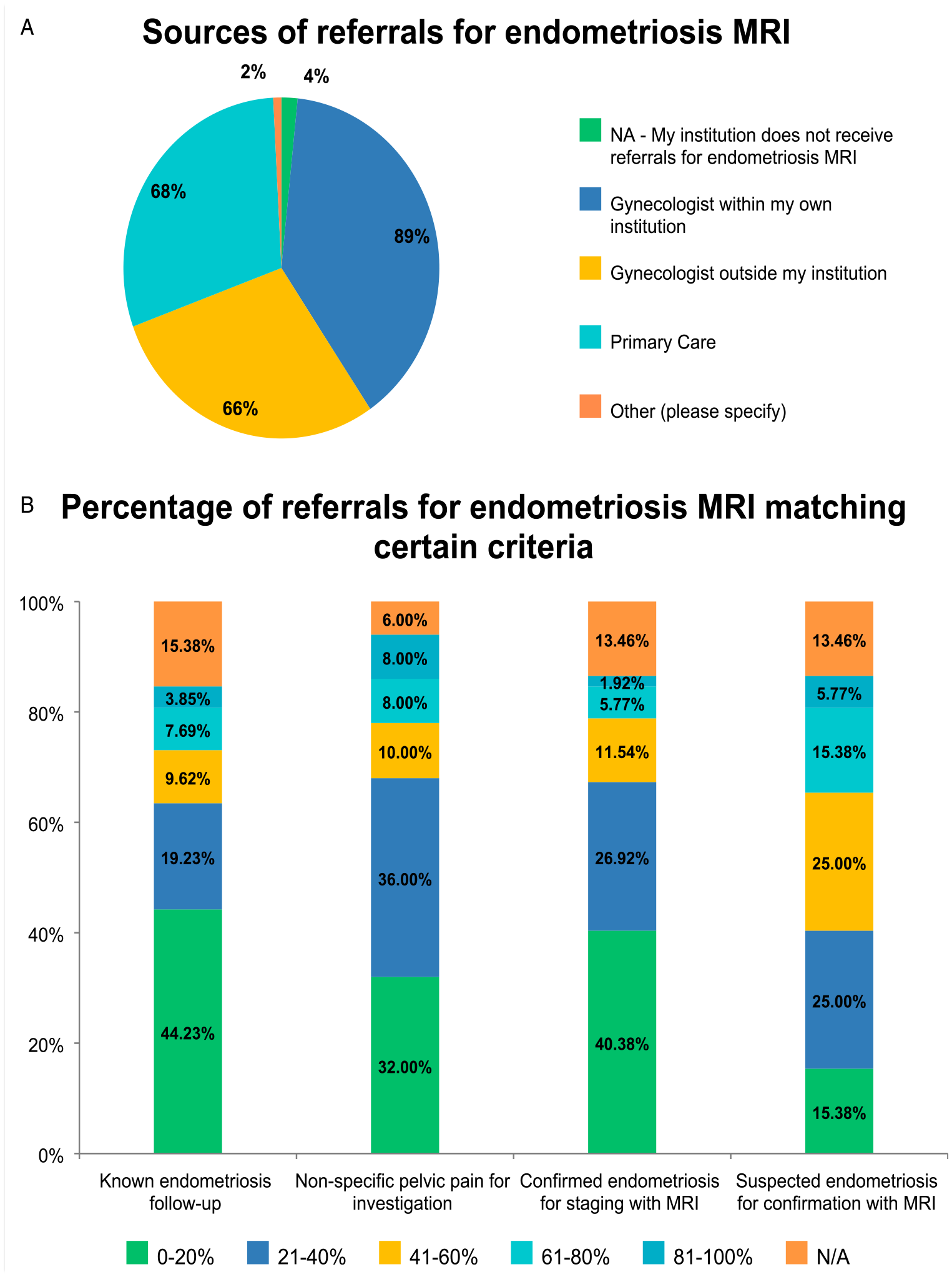
The most frequent reason for an MRI request was suspected endometriosis, followed by non-specific pelvic pain for investigation. (Figure 4B).
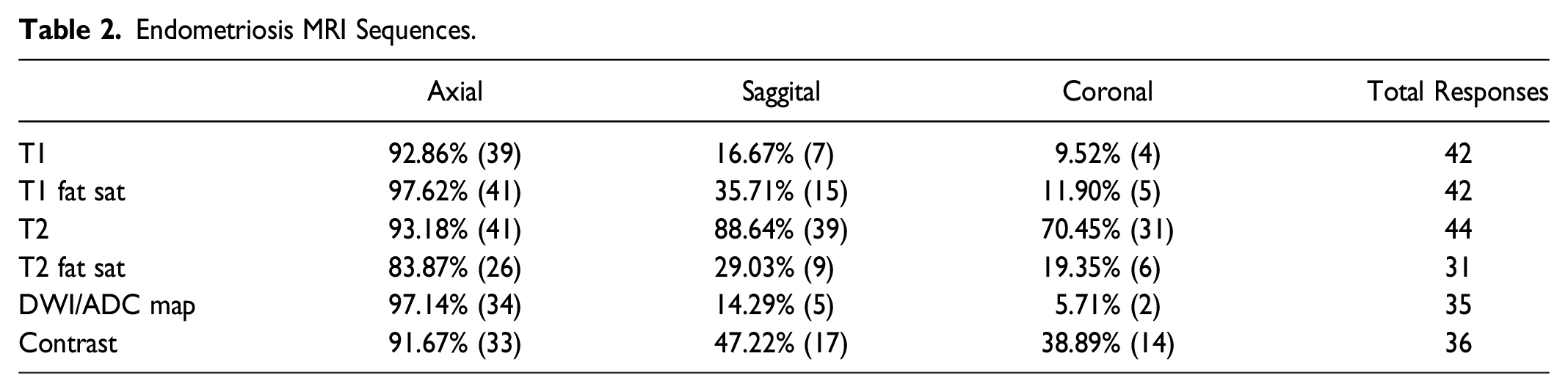
Endometriosis MRI Sequences.
A spasmolytic agent is administered at approximately 55% (23/46) of the institutions, and the technologist administers it in almost half of the sites. Bladder voiding instructions were used in 56% of the sites (23/46). Endorectal and endovaginal contrast, previously a common technique when studying endometriosis, is still implemented at only one site (2.33%) (Figure 5). When inquired about the specific dose of spasmolytic agent, the most frequent drug and dose administered was Buscopan® 20 mg, either IV or IM. Finally, at most sites, there is no radiologist/physician actively supervising the pelvic endometriosis MR (91.3%; 42/46). Patient preparation steps prior to endometriosis MRI.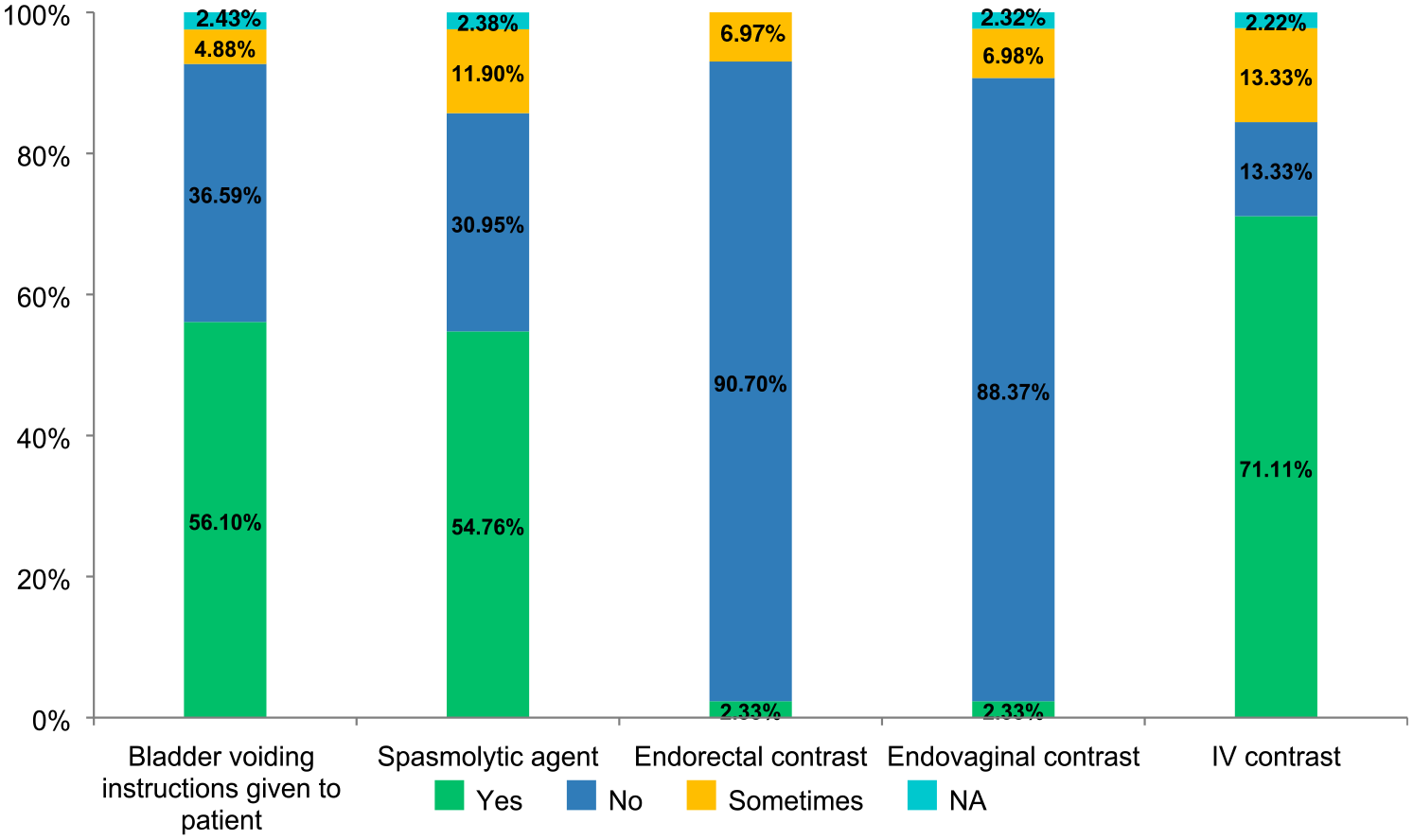
Extra-Pelvic Endometriosis
When asked about extra-pelvic endometriosis, the most frequent studies were MRI for soft-tissue endometriosis (eg abdominal wall) in 81% (36/44) of responses and CT for thoracic/diaphragmatic in 45% (20/44) of responses. In these cases, the request would come from the gynecologist in more than 77% (34/44) of the cases. See data from Questions 25-30 in the Supplementary Appendix for more details.
Quality Assurance and Challenges
Multidisciplinary endometriosis rounds are performed in only seven of sixty-five respondents’ institutions (10.7%); audits are conducted in 15 institutions (23%), and template reporting is used in only eight institutions (12.3%) (Figure 6). Of those who use template reporting, 17% (10/58) developed their own. Regional and provincial health authority templates represented 0% (0/58) of the respondents’ choices, reflecting the paucity of current guidelines and recommendations from the radiology societies. Methods for institutional quality assurance.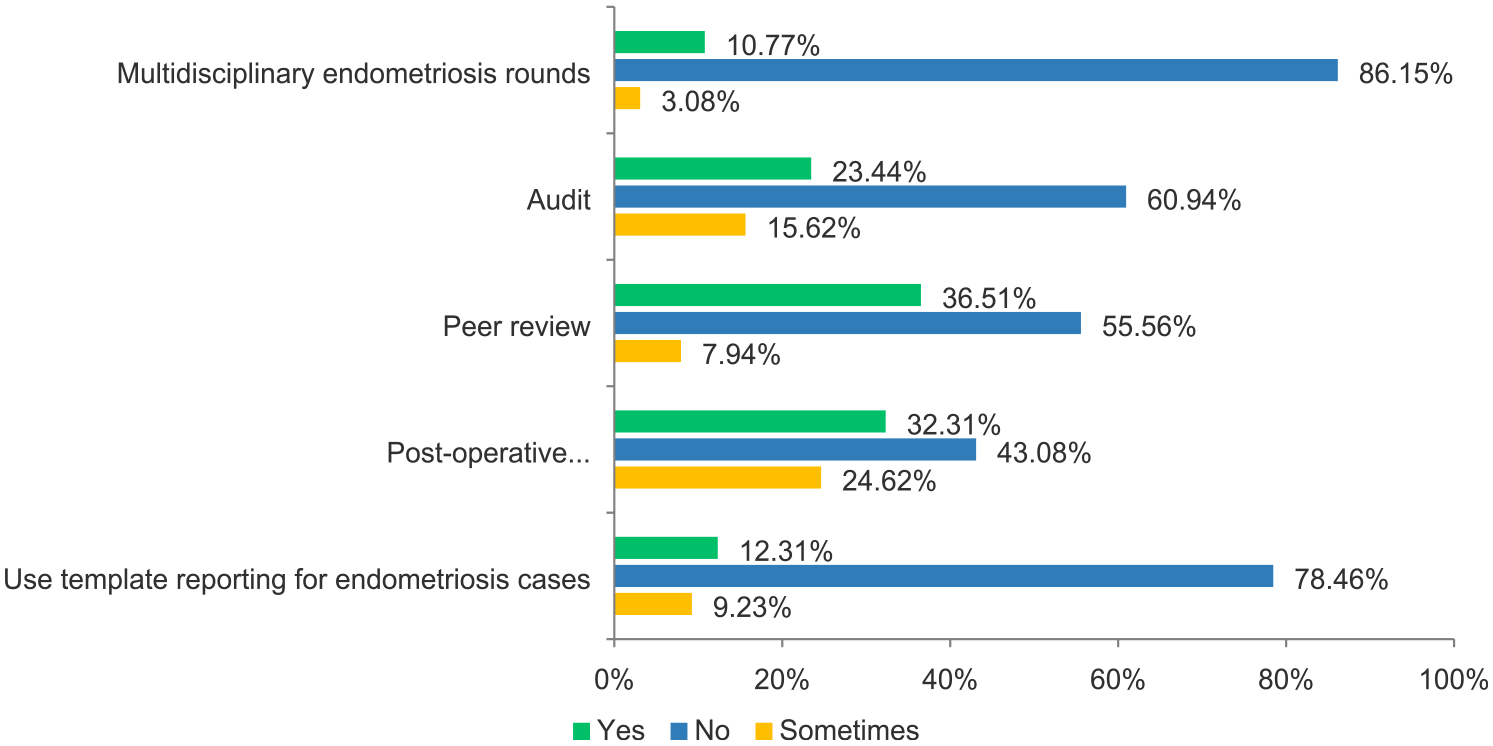
Barriers to Endometriosis Imaging.
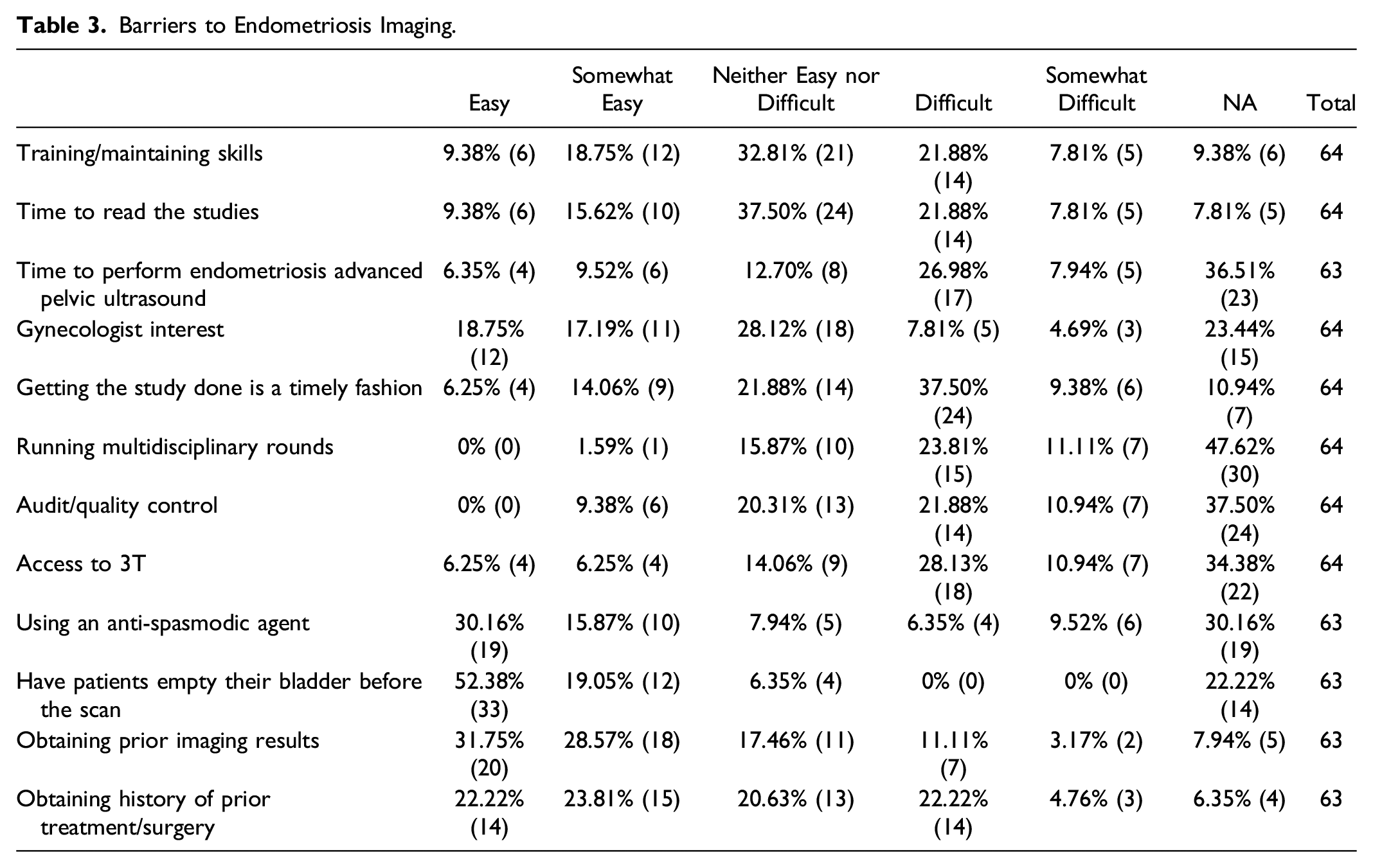
We finalized our survey by asking if there were any challenges the participants encountered that were not listed in the questions and about topics that the respondents would like to see covered in forthcoming CAR/CSAR clinical practice guidelines on endometriosis. The main challenges listed in the first question were scheduling and study time when performing dedicated ultrasound for endometriosis. For the later enquiry, the respondents wrote they would be interested in teaching activities, official guidelines and templates, with a specific request for indications for dedicated ultrasound vs MRI in the different clinical contexts (academic, community, etc.).
Discussion
This survey aimed to understand the overall knowledge and practice of advanced pelvic ultrasound and MRI for endometriosis among radiologists in Canada. Unfortunately, the response rate for the survey was approximately 5%, which is lower than other radiology questionnaires. 6 We believe this reflects the fact that despite endometriosis being a frequent complaint at clinicians’ offices and an important disease affecting the quality of life of many patients, there is a lack of understanding of how much these dedicated studies can benefit the patient. The results also demonstrated that most respondents were not currently performing dedicated studies evaluating endometriosis. Not having many professionals performing the studies also limits the transfer of knowledge to new trainees, perpetuating deficiencies in the area.
Another issue that emerged from our results is that there are still places where patients undergo surgery without prior imaging. Laparoscopic surgery has risks and may also underestimate the extent of the disease, with possible procedures resulting in incomplete treatment. 1 Being aware of the magnitude of the findings (such as hydroureter or bowel invasion) helps to achieve better postsurgical outcomes as it allows the gynecologist to have other specialties (i.e., urology and general surgery) involved in the surgery beforehand.
Moreover, there is an ongoing paradigm shift to a more multidisciplinary approach, with the combination of symptoms, imaging findings and response to treatment to help clinical management, even before any surgical confirmation, given the poor correlation between the symptoms and severity of lesions. This accentuates the need to make dedicated studies more accessible for those interested in learning and performing them at their imaging facilities.
The survey also highlighted the fact that despite many being interested in some training to start practicing, there was a higher interest in MRI than in advanced pelvic ultrasound. However, studies have shown high accuracy when the dedicated exams for endometriosis are performed and interpreted by training specialists, 4 resulting in better surgical outcomes and decreasing the chance of incomplete treatment or the need for re-intervention. 7 In this scenario, advanced pelvic ultrasound offers the prospect of being more available and less expensive technology, which may benefit remote and less assisted areas, making the results from this survey even more critical.
The other challenge emphasized by the respondents is related to scheduling. A dedicated advanced pelvic ultrasound for endometriosis usually takes longer to be performed and interpreted, impacting the workload and staffing in an environment that usually already works with limited resources. As jurisdictions struggle to meet MRI demand due to resource shortages, timely access to MRI remains an issue. 8 The lack of national guidelines or training from the specialist societies was also a limiting factor for many respondents, resulting in reduced confidence, possibly increased time, as well as practice variability. Some also highlighted the importance of a suggested template to optimize their workflow, which would help standardize reporting and facilitate quality improvement nationwide.
In conclusion, the difficulties and limitations demonstrated by the survey are factual, and, as radiologists, we face them daily. However, the benefits of developing the skillset and the technology to perform these dedicated studies overcome the cons, given how much it will impact patient outcomes and health resources, decreasing the number of repeat surgeries in cases of incomplete evaluation. Furthermore, the results highlight the importance of official guidelines and recommendations, which would facilitate their implementation in the radiology departments. The results will inform the development of Canadian-specific guidelines on how to perform and interpret dedicated endometriosis advanced pelvic ultrasound and MRI, as well as guides to help the sites to adjust their schedules and protocols considering resource challenges that exist in jurisdictions across the country. The survey results will also help to inform future endometriosis-specific CAR educational endeavours, promote a multidisciplinary approach to endometriosis imaging, and develop standardized templates and guidelines.
Supplemental Material
Supplemental Material - Current Practice Patterns, Challenges, and Need for Education in Performing and Reporting Advanced Pelvic US and MRI to Investigate Endometriosis: A Survey by the Canadian Association of Radiologists Endometriosis Working Group
Supplemental Material for Current Practice Patterns, Challenges, and Need for Education in Performing and Reporting Advanced Pelvic US and MRI to Investigate Endometriosis: A Survey by the Canadian Association of Radiologists Endometriosis Working Group by Priscila Sacilotto Crivellaro, Iffat Rehman, Silvia Chang, Shauna Duigenan, Signy Holmes, Casey Hurrell, Ania Z. Kielar, Mathew Leonardi, Emily Pang, Arvind Shergill, and Basma Al-Arnawoot in Canadian Association of Radiologists Journal
Footnotes
Acknowledgments
The authors would like to thank the members of the Canadian Association of Radiologists who took the time to provide their responses to the survey that informed this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.