
Abstract
The Canadian Association of Radiologists (CAR) Endometriosis Working Group was tasked with providing guidance and benchmarks to ensure the quality of technique and interpretation for advanced imaging modalities associated with diagnosing endometriosis. This practice statement provides an overview of the state of the art of advanced pelvic ultrasound in the diagnosis and mapping of pelvic endometriosis. While acknowledging that advanced pelvic ultrasound in some practices falls within the scope of clinical colleagues rather than imaging departments, the statement seeks to guide radiologists interested in implementing these techniques into their practice for patients referred for evaluation and diagnosis of endometriosis. The statement covers indications, some components of the ultrasound assessment and technique, reporting, and recommendations for starting an ultrasound endometriosis evaluation program.
Overview of Major Endometriosis Guidelines of International Societies
Given the complexity of endometriosis, various national and international working groups have published guidelines in the past few years to help standardize imaging techniques and reporting of findings identified with ultrasound.
This includes the landmark 2016 consensus opinion from the International Deep Endometriosis Analysis (IDEA) group, supported by the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG). This statement described standardized terminology and nomenclature to use when describing endometriosis as well as a systematic approach to imaging with a dedicated transvaginal ultrasound (TVUS) endometriosis protocol.1,2
Whilst an updated Society of Obstetricians and Gynaecologists of Canada (SOGC) Endometriosis Guideline is in development, we can look to guidance developed by other large, recognized organizing bodies. The 2022 Endometriosis Guidelines of the European Society of Human Reproduction and Embryology (ESHRE) strongly recommend clinicians to use imaging (either ultrasound or magnetic resonance imaging (MRI)) in the diagnostic work-up for endometriosis, noting that a negative result does not exclude endometriosis, particularly non-invasive superficial disease. 3 The National Institute for Health and Care Excellence (NICE) guideline in the United Kingdom recommends consideration of a dedicated ultrasound to investigate suspected endometriosis, even in patients with “normal” pelvic/abdominal physical examination. 4 This guideline also recommends considering a pelvic ultrasound or MRI before an operative laparoscopy for women with suspected deep endometriosis. 4 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) 2021 clinical practice guidelines amplify the utility of ultrasound as a diagnostic tool while also recognizing its drawbacks. 5 The American College of Radiology (ACR) Appropriateness Criteria ® for Female Infertility recommends TVUS as a primary modality for the imaging of patients with suspected endometriosis, along with MRI, and notes that it may be superior to MRI in the detection of rectosigmoid and retrocervical endometriosis. 6
TVUS for the detection of endometriosis may not yet be widely adopted by North American imaging centres, 7 partly due to the practice of having sonographers to perform ultrasound examinations that are subsequently interpreted by radiologists or gynecologists rather than live scanning by the interpreting physician.8,9 Expert-guided TVUS and dedicated ultrasound protocols performed by experienced sonographers/imagers in collaboration with interpreting physicians are instrumental for broad implementation in North American imaging practices.9,10
Indications
The nomenclature, advanced pelvic ultrasound, describes an ultrasound which provides detailed information on the presence and extent of endometriosis. This comprehensive assessment goes beyond the relatively basic “standard of care” pelvic ultrasound evaluation involving the uterus, ovaries, and cul-de-sac for fluid or mass. 11 Endometriosis is a disease that primarily affects the extra-uterine and extra-ovarian structures, 12 making the basic pelvic ultrasound inadequate for patients with appropriate indications. In many centres around the world, advanced pelvic ultrasound is performed by a physician with expertise in performing and interpreting ultrasound—a sonologist.
Understanding the differences between basic and advanced pelvic ultrasound is important as it impacts scheduling. Other relevant factors for access to advanced pelvic ultrasound include training of sonographers, radiologists, and sonologists. This statement is written with current realities in mind. However, future approaches to comprehensive endometriosis assessment will evolve based on the principles of advanced pelvic ultrasound.
There are 3 broad categories, which may overlap in an individual patient, that are indications for advanced pelvic ultrasound: 1. Dysmenorrhea (i.e. pain with menstruation) 2. Chronic pelvic pain 3. Infertility
In each of these populations, the prevalence of endometriosis is high, warranting intentional and directed assessment of the disease. The path of a patient with these concerns may differ, but one should consider an advanced pelvic ultrasound a valuable tool in their diagnostic journey.
Practical Considerations
Ultrasound Technique and Components of Assessment
The approach to an endometriosis-focused advanced pelvic ultrasound should follow the International Deep Endometriosis Analysis (IDEA) in their landmark consensus article, “Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions, and measurements: a consensus opinion from the International Deep Endometriosis Analysis (IDEA) group.” 1 This has been utilized in many studies and has been validated in a large international, prospective diagnostic test accuracy study. 13 A practical, stepwise approach of the IDEA consensus can also be used as a roadmap for the components and order of performance, and to inform the development of local TVUS protocols.2,14
Most advanced pelvic ultrasound for endometriosis is performed via transvaginal ultrasound (TVUS). Transabdominal ultrasound (TAUS) can be added to exclude general/other pelvic pathology. Moreover, TAUS of the kidneys and proximal ureters is recommended to rule out asymptomatic hydronephrosis from ureteral endometriosis. 1 If patients do not consent to TVUS, transrectal ultrasound can be an alternative, as there is evidence of similar diagnostic test performance for identifying deep endometriosis. 15
The IDEA consensus statement focus was on deep endometriosis, ovarian endometriomas, and endometriosis-associated adhesions. There has been development regarding the identification of superficial endometriosis16,17 though this has not yet been validated.
Preparation
Most centres performing gynecologic ultrasound assessments have a process of performing a TAUS with a full bladder first, followed by emptying of the bladder, and then an intracavitary ultrasound (usually TVUS). As noted above, most information pertinent to an endometriosis-focused advanced pelvic ultrasound is attained via the intracavitary assessment (TVUS or transrectal). This calls into question the utility of requiring a full bladder for patients with endometriosis ultrasound indications, which can be painful. If an intracavitary ultrasound is to be performed, it would be more comfortable for patients not to require a full bladder, except for in situations where bladder endometriosis is suspected. The TAUS component can still be performed to exclude large pelvic pathology that could potentially be missed on an intracavitary assessment (e.g., large pedunculated fibroids, dermoid ovarian cysts), which would not generally be enhanced dramatically with a full bladder. The TAUS component can be combined with a focused assessment of the kidneys if deemed appropriate.
Patient preparation for endometriosis-focused advanced pelvic ultrasound sometimes includes bowel preparation. The reasoning is that an empty bowel may be easier to assess for deep bowel endometriosis. This concept has been studied repeatedly, and in the past few years, within the same journal—Ultrasound in Obstetrics and Gynecology—contradictory results have been published.18,19
Equipment for advanced pelvic ultrasound should consist of a 2D or 3D wideband endocavity transducer with a 4–9 MHz frequency range for transvaginal or transrectal use. 3D ultrasound for endometriosis has not yet been universally adopted; however, it is valuable for characterizing uterine pathologies such as congenital anomalies and adenomyosis, which are commonly co-existent with endometriosis.20-22 One advantage of a 3D probe beyond rendering 3D images is the ability to steer the scan plane via crystal movement rather than probe manipulation, enhancing patient comfort. This is an important feature as patients being assessed for endometriosis often experience pelvic discomfort with TVUS compared to those without endometriosis.
Transducers with a frequency range of 5–13 MHz can also be used with the advantage of improved visualization of more subtle and superficial structures, such as superficial endometriosis lining the peritoneum.
Ultrasound Operators
Ultrasound for endometriosis has been predominantly under the domain of the sonologist due to its advanced nature and often complex anatomy. In Canada, sonographers are equipped to perform basic pelvic ultrasound but have not yet had formal training in advanced pelvic ultrasound techniques. However, around the world, sonographers are developing enhanced skills permitting them to perform advanced pelvic ultrasound.9,23,24 The USA and Australia have been leaders in enhancing the skills of sonographers. The Sonography Canada SonoCon 2022 featured its first focused talk on endometriosis to raise awareness and education among sonographers.
Reporting
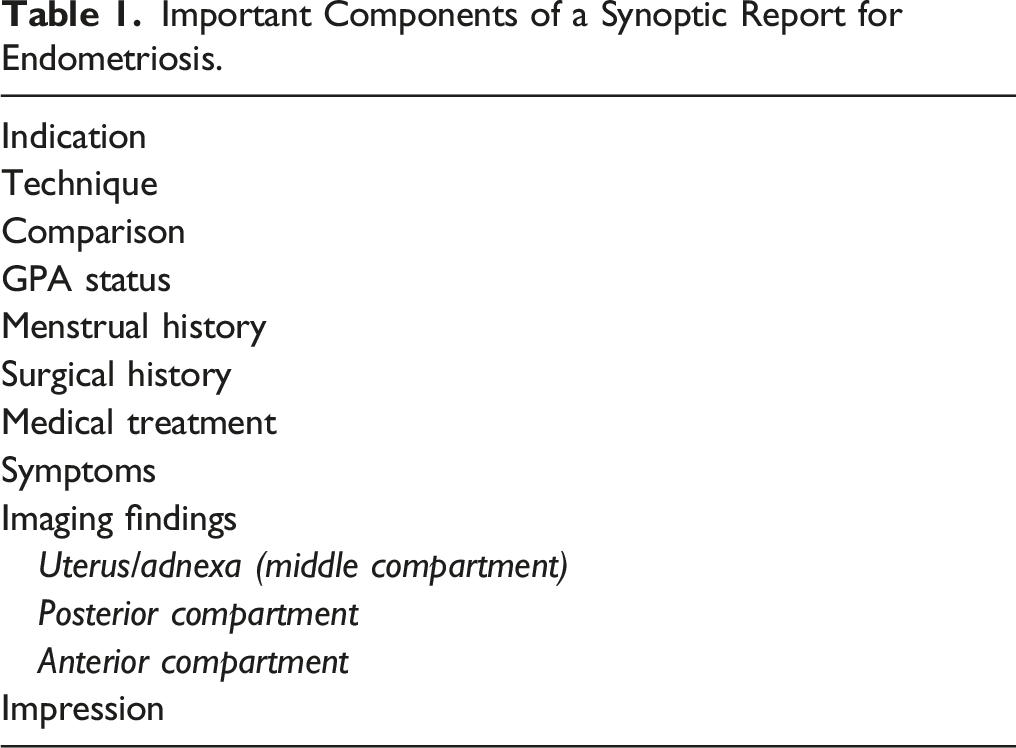
Structured or synoptic reports allow information to be presented in a tabular, consistent, and summarized form ensuring consistency and completeness in imaging reporting.1,2,8 The structured report for advanced pelvic ultrasound aims to standardize the format, descriptive terms, anatomical compartments, and organ assessment for consistent and accurate communication facilitating diagnosis and treatment planning. Structured template reports for endometriosis divide the pelvis in compartmental anatomy allowing a structured analysis and encouraging consistent identification of disease. Similar to how scanning of patients with dynamic ultrasound should follow the IDEA-suggested methodology, a standardized structured report for endometriosis-focused advanced pelvic ultrasound should adopt IDEA-suggested anatomic terms, methods and measurements. 25 There are several endometriosis staging systems that are applied surgically and may be applicable to imaging findings. As they are still in development, more research is needed to determine their diagnostic utility and value for imaging.26,27
Important Components of a Synoptic Report for Endometriosis.
Pelvic Compartment Model.
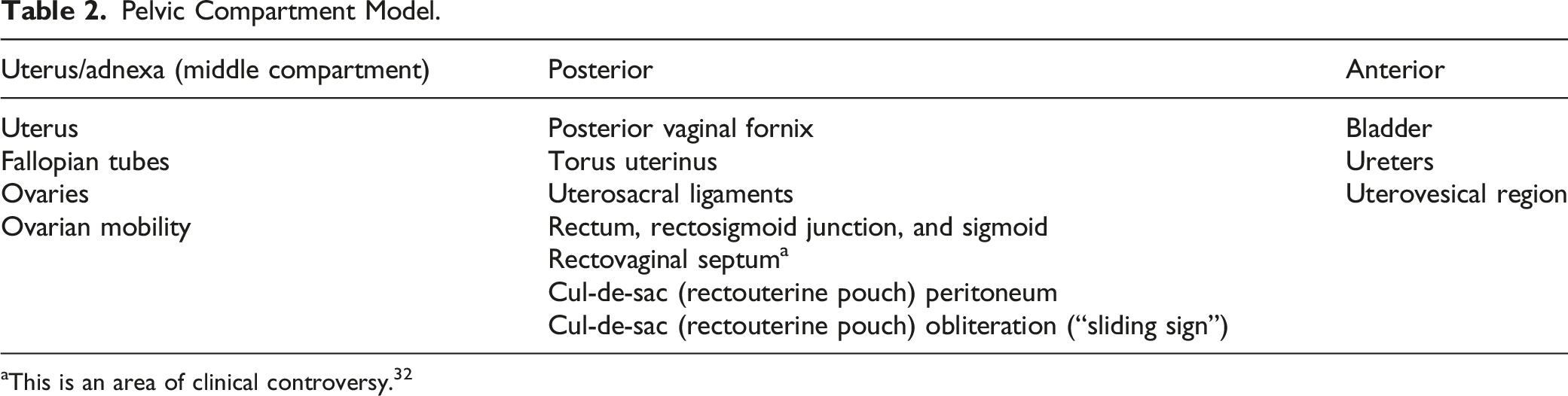
aThis is an area of clinical controversy. 32
When identifying features and describing findings in the uterus and adnexa, it is recommended to adhere to existing lexicons, mapping, and classification systems. For adenomyosis, refer to the MUSA statement; 28 for fibroids, refer to the FIGO classification system; 29 and for ovarian masses, refer to ACR O-RADS™.30,31
With respect to the bowel, it is essential for potential surgical planning to include information on the number and size of lesions(s) (measurements in 3 orthogonal places), the distance between lesions if there are multiple, and the distance between the lowest aspect of the most caudal bowel lesion and the anal verge.33,34 The location of the bowel can be described using sections that are measured from the anal verge.
In addition to the compartmental model, additional sections of the standardized report may provide further information on areas outside the pelvis, such as the cecum or appendix, which could be affected by endometriosis. Moreover, anterior abdominal wall nodules should be considered when clinically relevant.
Incorporating the IDEA terminology and site-specific nomenclature into a standardized reporting template can allow accurate mapping of pelvic endometriosis on ultrasound facilitating treatment planning and assessment by multidisciplinary team members. According to IDEA, dynamic ultrasound techniques can be used to assess areas of site-specific tenderness and abnormal ovarian motility (“soft markers”).
If findings are normal, it is recommended to include a statement at the conclusion of the report to inform the referring physician of the limitations of the imaging findings in making a diagnosis. In instances where anatomy was not assessed or visualized, we recommend including the note “Not Assessed” or “Not Visualized” to ensure that the report is complete.
The sliding sign to assess the rectouterine pouch obliteration state is performed during real-time transvaginal imaging and stored using Cine clips. Directed transvaginal probe pressure is applied gently to the cervix and/or the uterus is balloted gently, in order to identify if the uterus and rectum/rectosigmoid glide freely next to each other. Positive sliding (i.e. organs glide relative to each other) indicates a normal rectouterine pouch state and negative sliding (i.e. organs do not glide and are adherent to each other) indicates an abnormal rectouterine pouch obliteration state. A negative sliding sign is also an indirect way to identify deep endometriosis (DE).35,36
For a more in-depth explanation of the technique, and to visualize the normal (positive) and abnormal (negative) sliding sign, the working group recommends consulting a video resource. 37
Sample Statement for Normal Findings
“It is important to remember that a normal ultrasound does not mean the patient is normal. It simply means that we have not identified endometriosis or other pelvic pain-generating pathology on today’s ultrasound. At this point, we cannot entirely rule out endometriosis on imaging tests. If there is a high clinical suspicion of endometriosis in the setting of normal imaging, then referral to gynecology or additional diagnostic strategies can be considered.”
Starting an Endometriosis Ultrasound Evaluation Program
As with any other endeavour, introducing a new program requires forethought and planning. There are several change management models which can help ensure a smooth process, including Kotter’s change management. 38
Relevant stakeholders for an ultrasound endometriosis program include gynecologists, radiologists, technologists, imaging administrators, and pathologists. Administrators are tasked with ensuring adequate resources and scheduling/imaging timeslots to accommodate the required longer examination times. 39 The feasibility of running the program must also be assessed. This must consider the scheduling demands to ensure an adequate workload-to-imaging expert ratio and ensure the availability of staff to be scheduled for such a service.
It is worthwhile to identify imaging and sonographer “champions”; these are individuals who will serve as the mentors for others in their peer group to learn imaging techniques related to the sonographic evaluation of endometriosis, and these individuals will endeavour to continue to focus their continuing medical education on cutting edge information related to endometriosis imaging. Radiologist champions in academic centres, as well as community hospitals, may also consider participating in endometriosis research, including various quality initiatives.
Gynecologists who will refer patients for imaging are of particular interest as stakeholders, given that these specialist physicians will subsequently treat patients diagnosed with endometriosis with medical or surgical intervention. In some cases, they themselves have specialized training in performing and interpreting advanced pelvic ultrasound for endometriosis. A collaborative relationship is paramount, and communication is integral for feedback purposes, determining necessary additions to the standardized template report, and obtaining feedback on successes and misses. 40
Technical considerations for the program include ensuring that the ultrasound machines and probes are up-to-date and adequate for obtaining high-quality images. The room must be set up to accommodate a longer exam time. Examinations should be performed on an adjustable examination table; tables with stirrups are preferred and adequate padding is necessary given that examinations can last up to 45 minutes 39 (though most are significantly shorter in duration than the maximum). Preparing patients in advance by ensuring that the schedulers can consistently and fully communicate what patients should expect at the time of their study and confirming they are scheduled to arrive with a full bladder, when indicated, for the transabdominal component of the scan. Consideration about timing the scan to be at a different time from the patient’s menstrual cycle can reduce discomfort, though it is not required for adequate imaging.
When a program is started, keeping everyone informed of the progress and celebrating the successes will keep all those involved in a new program engaged and up to date.
Key Points
1. Endometriosis is common in the population; diagnosis and mapping of endometriosis on ultrasound are possible. We cannot currently rule out endometriosis on imaging; therefore, symptomatic patients should not be dismissed based on normal imaging findings. 2. There are criteria to differentiate basic from advanced ultrasound. Advanced comprehensive ultrasound is required for the assessment of endometriosis. 3. Adopting a standardized reporting template enables systematic and reproducible communication between healthcare providers. 4. The posterior compartment is the most common site of endometriosis and therefore the area in which reporting physicians can add the most value to patient management. 5. There is a lot of research activity in advanced ultrasound for endometriosis that will continue to evolve over the coming years.
Supplemental Material
Supplemental Material - CAR Practice Statement on Advanced Pelvic Ultrasound for Endometriosis
Supplemental Material for CAR Practice Statement on Advanced Pelvic Ultrasound for Endometriosis by Basma Al-Arnawoot, Silvia Chang, Shauna Duigenan, Ania Z. Kielar, and Mathew Leonardi in Canadian Association of Radiologists Journal
Footnotes
Acknowledgments
The authors acknowledge the assistance and contributions of the other members of the CAR Endometriosis Working Group: Dr. Signy Holmes, Dr. Emily Pang, Dr. Iffat Rehman, Dr. Priscila Sacilotto Crivellaro, Dr. Arvind Shergill. The authors would also like to thank the members of the Canadian Association of Radiologists who took the time to provide their feedback and peer review during the drafting of these guidelines.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Unrelated to the recommendations contained herein, Dr. Leonardi is a member of the AbbVie advisory board; has delivered lectures for AbbVie, Hologic, and TerSera; has received research grants from Hyivy, AIMA, and AbbVie; and has participated in clinical trials within the past 36 months funded by Hyivy, and AIMA.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.