
Abstract
Objective
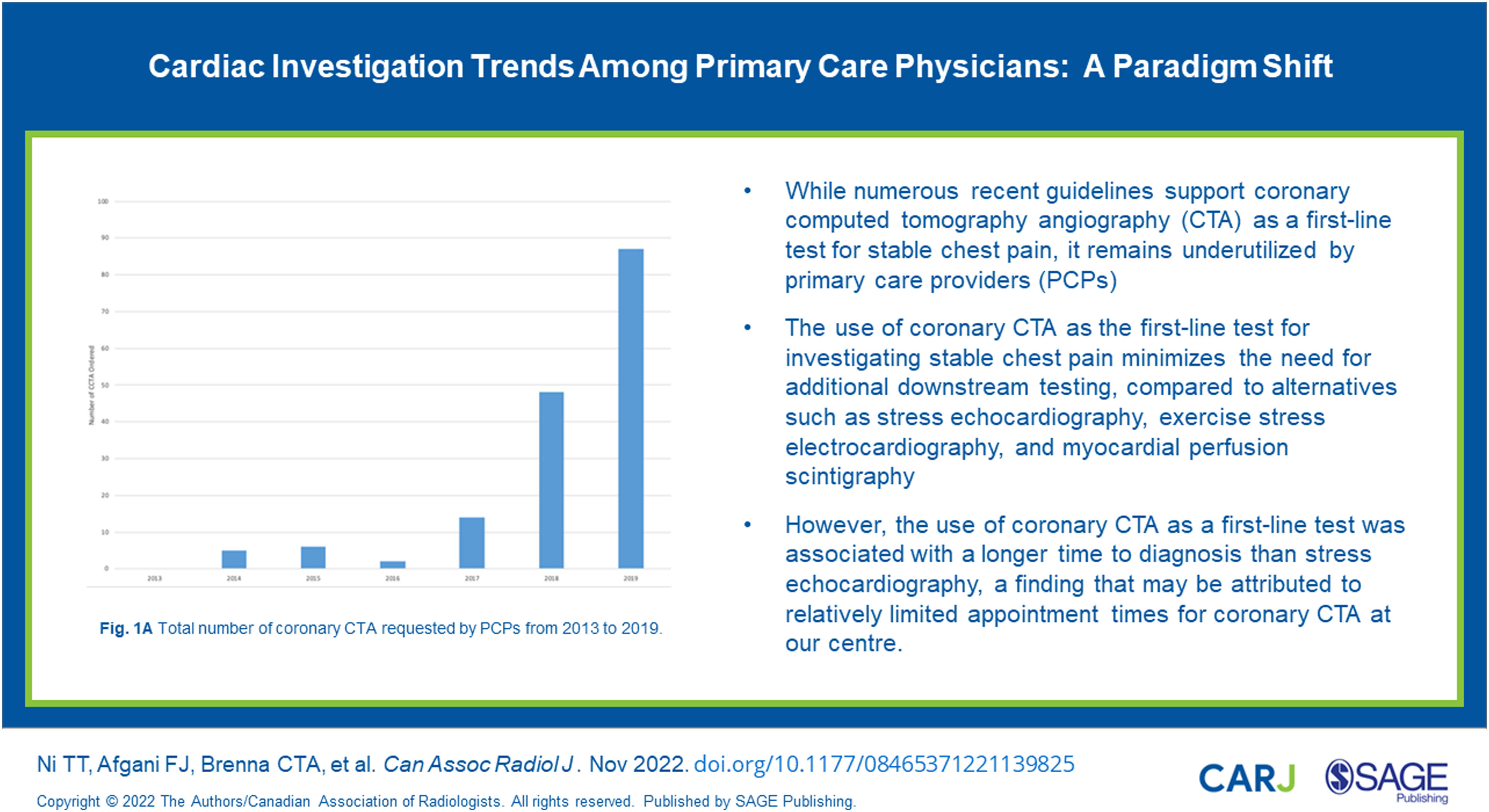
While numerous recent guidelines support coronary computed tomography angiography (CTA) as a first-line test for stable chest pain, it remains underutilized by primary care physicians (PCPs). We aimed to evaluate cardiac investigation ordering practices following education sessions, as well as the total number of downstream tests and time to diagnosis for patients presenting with stable chest pain.
Methods
A retrospective chart review was completed for eligible patients assessed at the Women's College Hospital Family Practice Health Centre between 2017 and 2019 following the education sessions. The outcome measures were first-choice cardiac investigation, additional downstream testing, time from presentation to first investigation, and time to final diagnosis.
Results
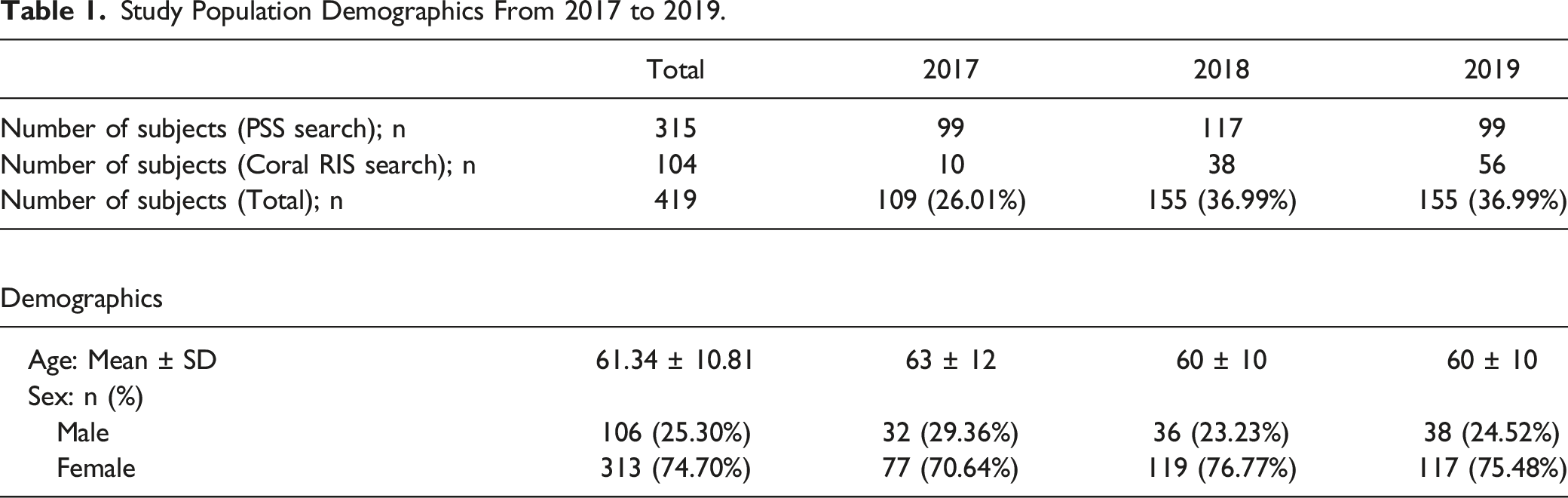
419 patients were included in the final analysis (74.70% female; mean age 61 ± 11 years). Coronary CTA requests by PCPs increased between 2017 and 2019 (18 vs 72 tests; P < .0001). When coronary CTA was the first-line test, patients were less likely to receive additional downstream testing when compared to those receiving other first-line investigations (P < .0001). Coronary CTA was associated with longer time to diagnosis than stress echocardiography (47 ± 45 vs 27 ± 36 days; P = .0068) due to limited availability of coronary CTA appointment times. There was no significant difference in time to final diagnosis among the cardiac imaging modalities observed in the cohort (P = .0623).
Conclusion
Utilization of coronary CTA as the first-line test for stable chest pain increased following our education sessions targeting PCPs. Coronary CTA was associated with less downstream testing compared to other non-invasive cardiac investigations.
Introduction
Chest pain is a common symptom among patients presenting to primary care physicians (PCPs) in Canada. 1 Classically, “typical” chest pain associated with coronary artery disease (CAD), also known as “angina,” consists of (1) substernal chest pain that is (2) triggered by physical exertion or emotional stress and is (3) relieved by rest or nitroglycerin. 2 Stable CAD is common among aging patients who develop cardiac risk factors, when a gradual build-up of cholesterol, inflammatory cells, and calcium leads to narrowing in the lumen of coronary arteries and periods of demand ischemia. 3 In contrast, unstable CAD or “acute coronary syndrome” occurs due to abrupt rupture in the cap of an atherosclerotic plaque, leading to secondary blood clot formation, myocardial ischemia, and tissue injury or death. 3
A variety of non-invasive testing modalities are available to investigate chest pain associated with CAD and assess the degree of coronary artery obstruction that leads to ischemia and chest pain or equivalent symptoms, including stress electrocardiography (GXT), stress echocardiography (SE), and myocardial perfusion scintigraphy (myocardial perfusion imaging/MPI).4-7 When used in conjunction with clinical assessment, these tests aid in evaluating patients’ risk of CAD and help to direct appropriate management. Unfortunately, they also frequently yield equivocal or inconclusive results, necessitating additional downstream testing and resulting in delayed diagnosis. Additionally, for a variety of reasons, these tests have suboptimal performance in women with a high incidence of false positives compared to men.6,8-13
Coronary computed tomography angiography (CTA) has emerged as a robust imaging tool with an extremely high negative predictive value for the exclusion of CAD.14,15 Because coronary CTA directly visualizes the coronary vessels, it can also characterize the extent and severity of both non-obstructive and obstructive CAD, delineate atherosclerotic plaque composition, and identify higher risk imaging features for plaque rupture (e.g., positive remodeling or low attenuation plaque). 16
Accordingly, guidelines on the investigation of CAD have evolved significantly over the past 2 decades to reflect the advantages of coronary CTA. In 2016, the United Kingdom’s National Institute for Health and Care Excellences (NICE) and, in 2019, the European Society of Cardiology updated their guidelines to recommend coronary CTA as the first-line test for all patients with typical or atypical stable chest pain to either rule out or establish a diagnosis of CAD.17,18 Most recently in 2021, the American Heart Association and the American College of Cardiology published updated guidelines for evaluating and diagnosing chest pain. 19 For intermediate- or high risk patients with stable chest pain and no known CAD, anatomic imaging with coronary CTA and functional testing are appropriate first-line tests to exclude atherosclerotic plaque and obstructive CAD. 19 According to these guidelines, coronary CTA is favored when the clinical question is focused on ruling out obstructive CAD or detecting non-obstructive CAD, whereas functional testing is favored for ischemia-guided management. Coronary CTA is also favored for intermediate-high risk patients who are <65 years of age with lower pre-test likelihood of obstructive CAD. 19
While numerous emerging studies and guidelines support the use of coronary CTA as an early triage tool to investigate stable chest pain, it remains underutilized by PCPs. Coronary CTA is primarily requested by cardiologists in Canada.20-22 Without targeted educational efforts on relatively newer cardiac imaging modalities and their appropriate use in clinical practice, many PCPs bear the burden of trying to interpret and understand the strengths and limitations of these complex tests, which may inadvertently expose patients to unnecessary testing and delayed diagnoses. 22
This study aimed to characterize trends in the first-line cardiac investigations requested by PCPs at Women's College Hospital (WCH) between 2017 and 2019, following a series of educational sessions (targeting PCPs and presented by cardiothoracic radiologists) regarding the merits of using coronary CTA as the first-line test to investigate stable chest pain in intermediate- or high-risk patients. We also aimed to assess the number of downstream tests and the length of time each investigative pathway required to reach a final diagnosis.
Methods
This study was formally reviewed and approved through the WCH Ethics Assessment Process for Quality Improvement Projects (APQIP) as a quality improvement project (#2019-0117-E).
Educational Intervention and Study Participants
As part of the WCH family medicine grand rounds program and annual group retreat, we developed an educational workshop on the novel merits of coronary CTA as a first-line test in the investigation of stable chest pain in intermediate- or high-risk patients. Educational sessions were presented to PCPs in the Family Practice Health Centre (FPHC) at WCH (Toronto, Ontario) in November 2013, May 2014, and November 2016. Content and delivery methods were based on a review of the contemporaneous literature and further refined by the Joint Department of Medical Imaging cardiothoracic radiology team. The educational sessions provided an overview of the available investigations for the workup of stable chest pain and each test’s strengths and limitations, the consequences of over-testing, the unique risks for female patients, and the emerging evidence in support of coronary CTA as the first-line test for the investigation of stable chest pain.
Participant eligibility included all patients seen by PCPs involved in ordering cardiac testing modalities between January 2013 and December 2019.
Data Collection
A retrospective chart review was completed for all eligible patients seen at the WCH-FPHC between January 1, 2017 to December 21, 2019. The time period was selected to evaluate how ordering practices evolved over the 3 years after the completion of the educational sessions.
Eligible patients were identified using a customized search feature within PS Suite (PSS; formerly Practice Solutions), the electronic medical record software used at WCH-FPHC. The search terms and criteria included age equal to or above 40 years, “chest pain,” “chest discomfort,” “chest tightness,” “angina”, “r/o CAD,” “CP,” and “C/P.” Charts with the term “no chest pain” were excluded. Patients were also excluded if there was a prior history of CAD and acute coronary syndrome, including acute myocardial infarction or unstable angina, at presentation. Charts identified by the search subsequently underwent manual review in detail to exclude patients who were explicitly investigated for conditions unrelated to CAD, such as upper respiratory tract infections, or who were undergoing follow-up imaging for other cardiac conditions. A second search for eligible patients who received coronary CTA imaging between 2017 and 2019 was performed through the Coral Radiology Information System (RIS) to manually identify eligible patients whose charts did not bear the search terms as described above, but who were referred for the investigation of stable chest pain. Patients identified in this search similarly underwent individual chart review according to the abovementioned eligibility criteria, and duplicate cases were excluded.
Outcome Measures
Outcome measures included the type of first-line cardiac imaging ordered (defined as the first cardiac imaging test obtained after an initial presentation of chest pain), the total number of cardiac tests conducted before reaching a diagnosis, and the total length of time elapsing between presentation and final diagnosis. The length of time to reach the final diagnosis was defined as the time interval between the date of a patient’s presentation at WCH-FPHC with chest pain and the date of diagnosis. The date of diagnosis was defined as the date of follow-up appointment with the PCP or cardiologist during which CAD was officially diagnosed or excluded as a cause for symptoms. In the absence of a follow-up visit or phone call with either physician, the date of the last cardiac investigation was used.
As Holter monitor testing was frequently requested in conjunction with other forms of cardiac imaging (especially stress echocardiography), the frequency of Holter monitoring as a first-line test was also recorded. 23
Statistical Analysis
Statistical analysis was completed using SAS Studio (SAS Institute, North Carolina, USA). All continuous data were tested for normal distribution using the Shapiro–Wilk test. Continuous data were described using mean and standard deviation or median and interquartile range (IQR), and categorical data were described using numbers and percentages. Comparisons between groups were made using Chi-square test for categorical variables. Continuous variables were assessed using the ANOVA test and Cox proportional hazards model for continuous variables with non-normal distribution. A two-tailed P-value of <.05 was used to define statistical significance.
Results
Patient Characteristics
In total, 3428 patients presenting between January 1, 2017 and December 31, 2019 were identified from PSS based on initial keyword searches (Figure 1). Six charts were flagged as private by patient request and therefore excluded before the screening. Following individual chart screening the remaining 3422 charts, 3082 patients were manually excluded. A detailed secondary screening process further excluded 31 patients due to missing appointments (n = 16), individual patient test preferences (n = 3), inconclusive tests due to limited diagnostic quality (n = 5), incorrect tests ordered in error by PCPs (n = 1), tests rejected by the radiologist (n = 1), test orders which were not submitted (n = 1), tests which were performed outside of the study timeline (n = 2), or test results which were missing in our electronic medical record system (EPIC, n = 2). In the case of the PCP ordering an incorrect test, the initial test ordered was an echocardiogram, which was amended at a later date to GXT. Additionally, in the case of the test request rejection, the radiologist deemed the request for coronary CTA to be inappropriate due to a lack of documented patient history. Method of identification of eligible patients from PS Suite (PSS) and Coral RIS.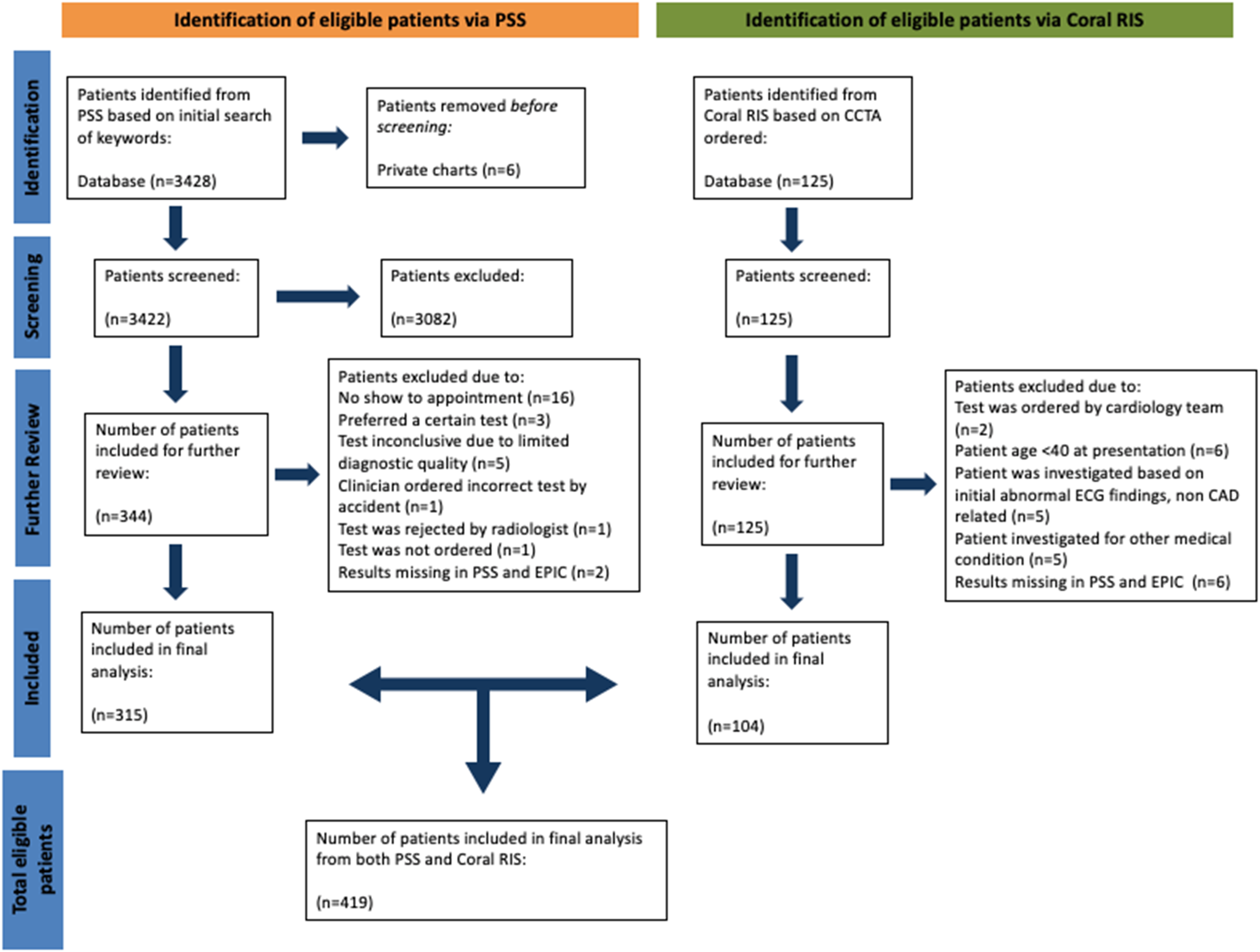
In addition, 125 eligible patients were identified from Coral RIS after receiving coronary CTA imaging and were reviewed in detail, and 104 patients were included in the final analysis (Figure 1). Following chart review, 21 patients were excluded due to a test order placed by the cardiology team (n = 2), age below 40 years at presentation (n = 6), imaging ordered based on non-CAD–related ECG abnormalities (n = 5), investigated for another medical condition (n = 5), and/or test results which were unavailable in our electronic medical record system (n = 6).
Study Population Demographics From 2017 to 2019.
First-Line Cardiac Investigations
Trends in First-Line Cardiac Investigations Among PCPs.
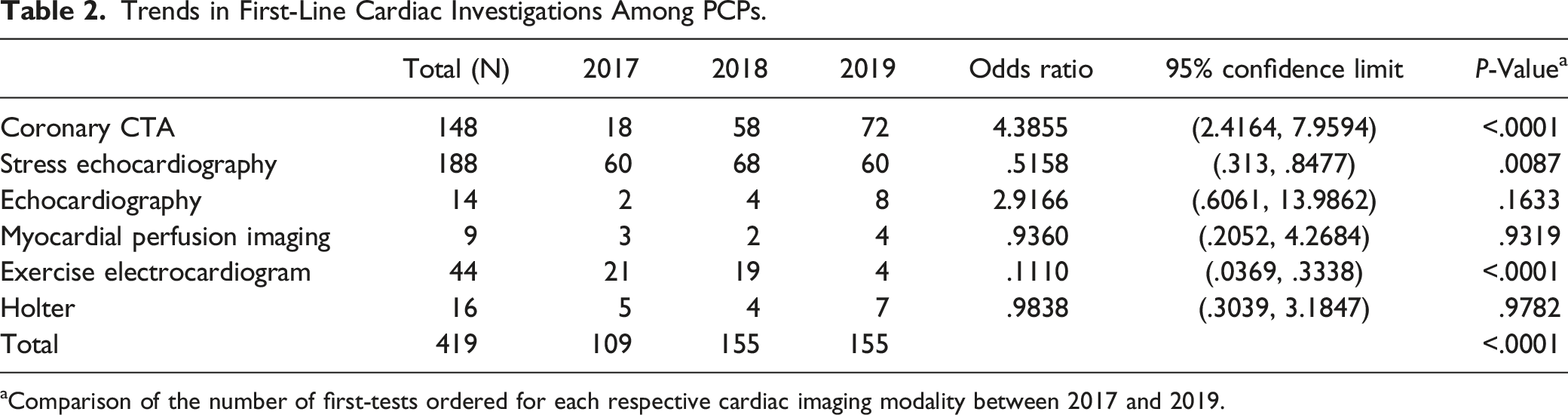
aComparison of the number of first-tests ordered for each respective cardiac imaging modality between 2017 and 2019.
There was a statistically significant increase in the number of coronary CTAs requested by PCPs between 2017 and 2019 (18 tests vs 72 tests; P < .0001), with an odds ratio of 4.39 and 95% CI [2.42, 7.96]. In contrast, the number of stress echocardiograms requested between 2017 and 2019 significantly decreased (P = .0087), with an odds ratio of .5158 and 95% CI [.31, .85]. There was also a significant reduction in the use of GXT as the first-line test between 2017 and 2019 (P < .0001). For both MPI and echocardiography, there was no significant change in ordering between 2017 and 2019 (P = .9319 and P = .1633, respectively). From 2017 to 2019, there was no significant difference between the number of Holter monitoring tests ordered (5 vs 7; P = .9782).
Total Number of Cardiac Tests Conducted to Reach a Diagnosis
Downstream Testing Following Each First-Line Cardiac Investigation Modality.
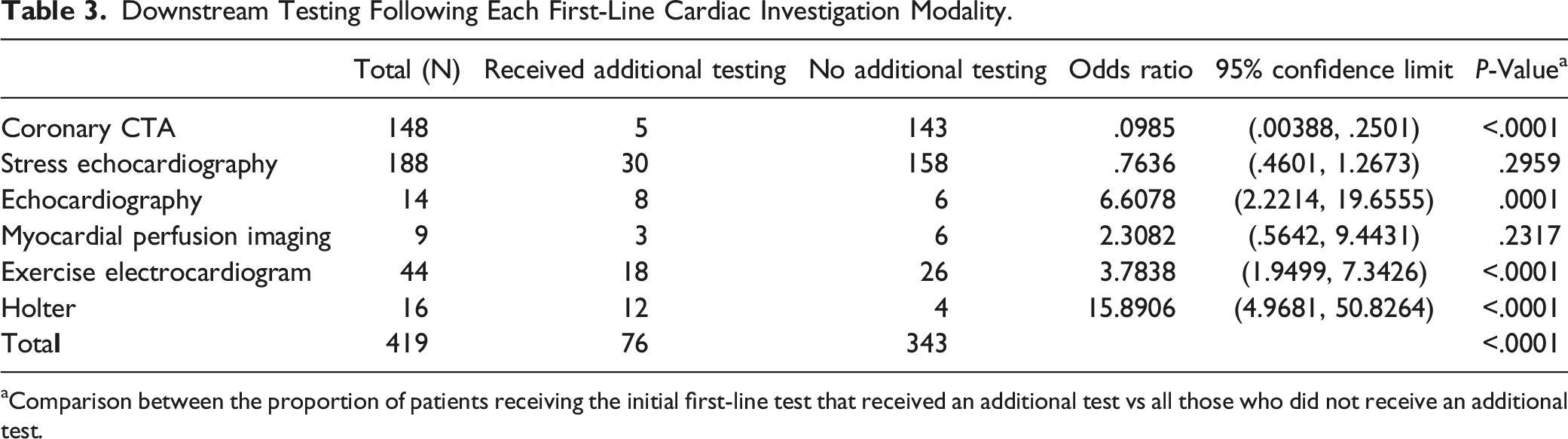
aComparison between the proportion of patients receiving the initial first-line test that received an additional test vs all those who did not receive an additional test.
Time to First Test
(A) Booking Time for Each Cardiac Investigation Modality. (B) Time to a Final Diagnosis for Each Cardiac Investigation Modality.
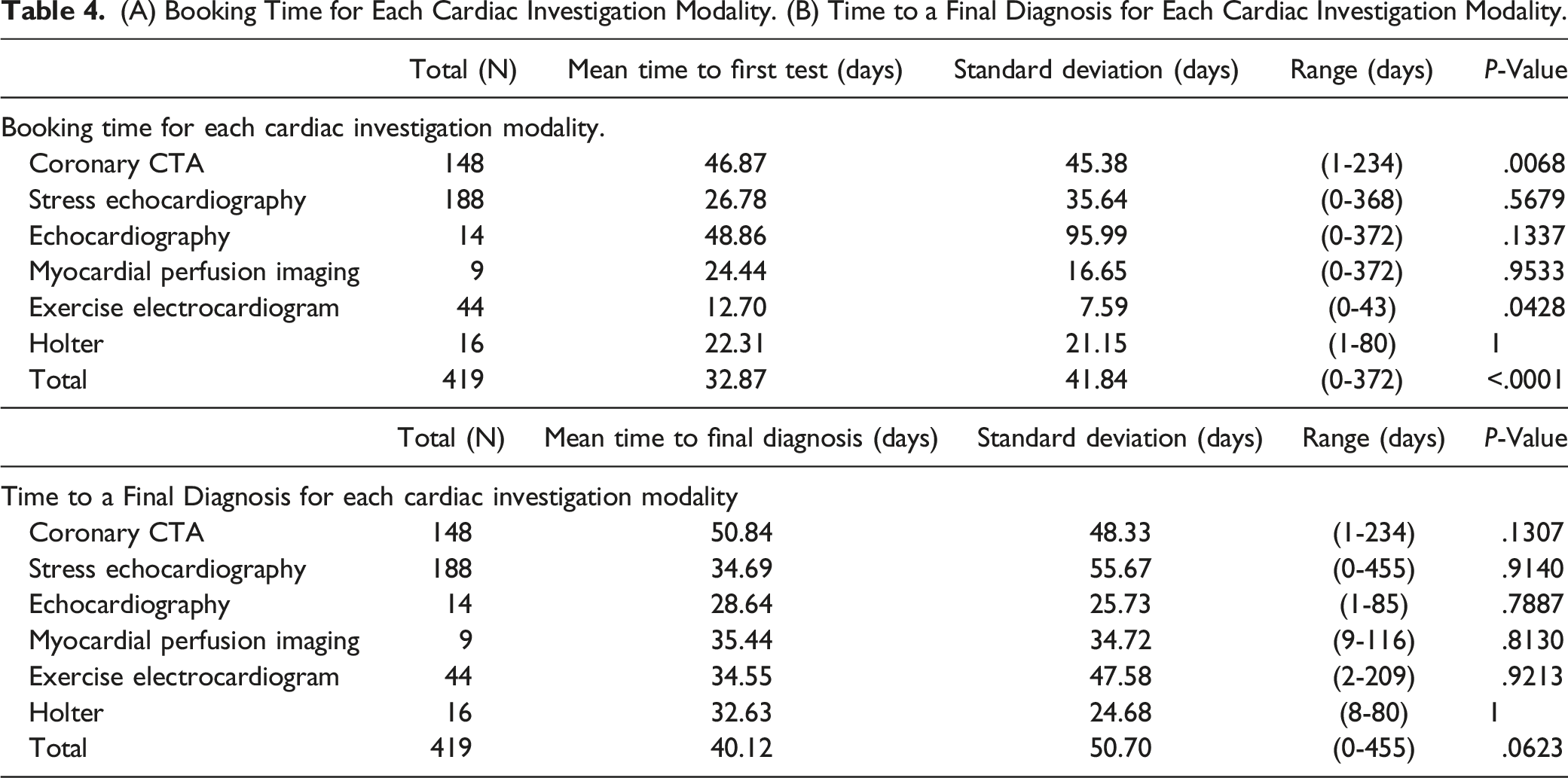
Time to Final Diagnosis
The length of time required to receive the final diagnosis was also examined for all 6 cardiac investigations (Table 4). Overall, the average time to achieve a final diagnosis among patients in our cohort was 40 ± 50 days, with a range of 0–455 days. Across the 6 cardiac imaging modalities, there was no significant difference in the time to diagnosis when analyzing variance between the groups (P = .0623).
Discussion
Coronary CTA has emerged in recent years as a robust first-line test for investigating CAD, especially in intermediate-risk patients without a known history of CAD.14,15 The current study demonstrates the expanding usage of coronary CTA as the first-line cardiac test for patients presenting with stable chest pain over a 3-year period, following targeted educational sessions for PCPs at our center. Our study demonstrates value in educating PCPs regarding relatively newer imaging modalities and the potential to influence requesting practices that mirror trends in specialist care. 24 Furthermore, we also demonstrate that, compared to other cardiac investigations, coronary CTA as a first-line test was associated with less downstream testing which could provide potential cost-savings from a health care system perspective.
Despite the support for coronary CTA as an early triage tool in investigating stable chest pain, it remains underutilized by PCPs21,22,25 (Appendix Figure A1). Our study highlights changing practice trends and the importance of targeted educational sessions by cardiac imagers to liaise with PCPs and share knowledge about the strengths and limitations of the various cardiac imaging modalities. In addition, these education sessions allow radiologists to directly address potential concerns from PCPs surrounding coronary CTA use, including ionizing radiation exposure or unique risks posed to patients with severe renal dysfunction. This empowers PCPs to effectively rule out important CAD with coronary CTA, and to streamline appropriate specialist referral.
Our study also found that coronary CTA is associated with a longer time to first-test compared to stress echocardiography. This may reflect the limited number of appointments for coronary CTA scanning at our center, emphasizing a need for capacity-building to match the growing need for coronary CTA imaging. Similar concerns regarding the availability of CT scanners and the number of trained healthcare professionals have been reported in Europe. 26 Following the 2016 NICE guidelines, an estimate published by the British Society of Cardiovascular Imaging/British Society of Cardiovascular CT suggested that a 700% increase in cardiac CT will be required across the UK to comply with the guideline recommendations. 26 The present study corroborates these reports and recommends a greater allocation of resources and investment in CT technology and training to meet the growing demand for coronary CTA imaging. Currently in Ontario, Canada, the majority of referring physicians for coronary CTA imaging are cardiologists. 27 One commonly held concern is that broadening the scope of referrals for coronary CTA imaging to PCPs may potentially increase the number of both inappropriate and appropriate referrals, thus further increasing wait times. We observed that with increasing coronary CTA requests from PCPs, booking wait times also increased (mean 36 days, SD 25 days during 2013–2016 prior to the education sessions and 61 days, SD 21 days during 2017–2019, following the education sessions). This highlights the importance of capacity building and the development of streamlined referral pathways 28 in order to meet the clinical demands for an emerging cardiac investigation that has demonstrated significant diagnostic and prognostic value.
Limitations
As this is a retrospective observational study, we cannot determine with certainty that the educational sessions caused PCPs to request more coronary CTAs. However, it is known that the number of coronary CTAs requested by PCPs was very low during 2013–2016 (Appendix Figure A1), simply due to lack of awareness of the value of coronary CTA. The retrospective, observational nature of the study did not permit exploration of why women were disproportionately represented among study participants. PCPs were more likely to request cardiac investigations in women, possibly due to higher prevalence of atypical symptoms, but our study did not explore the underlying reasons for this. Moreover, eligible patients in this current investigation were referred for coronary CTA by PCPs based on clinical suspicion for CAD causing symptoms, most often chest pain. We cannot conclude from the current investigation methods whether there was also a corresponding increase in the number of inappropriate referrals for coronary CTA during the study period as this data is not tracked using our current radiology information system.
Conclusion
Coronary CTA is a robust cardiac imaging tool and is now a recommended first-line cardiac investigation, particularly for both intermediate- and high-risk patients according to multiple international guidelines.17-19 Following targeted educational sessions for PCPs, we observed an increase in coronary CTA utilization as a first-line test for stable chest pain in our tertiary referral center, and this is associated with reduced downstream testing.
Supplemental Material
Supplemental Material - Cardiac Investigation Trends Among Primary Care Physicians: A Paradigm Shift
Supplemental Material for Cardiac Investigation Trends Among Primary Care Physicians: A Paradigm Shift by Tiffany T. Ni, MSc, Fahmeen J. Afgani, MBBS, Connor T. A. Brenna, MD, Nikita Patel, MD, CCFP, and Elsie T. Nguyen, MD, FRCPC in the Canadian Association of Radiologists Journal.
Footnotes
Acknowledgments
The authors acknowledge Corwin Burton from WCH for his assistance in the data retrieval process. We would also like to acknowledge Drs. Kate Hanneman, Tristal Li, and Pascal Tyrrell for their assistance and guidance in the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix 1
Total number of coronary CTA requested by PCPs from 2013 to 2019.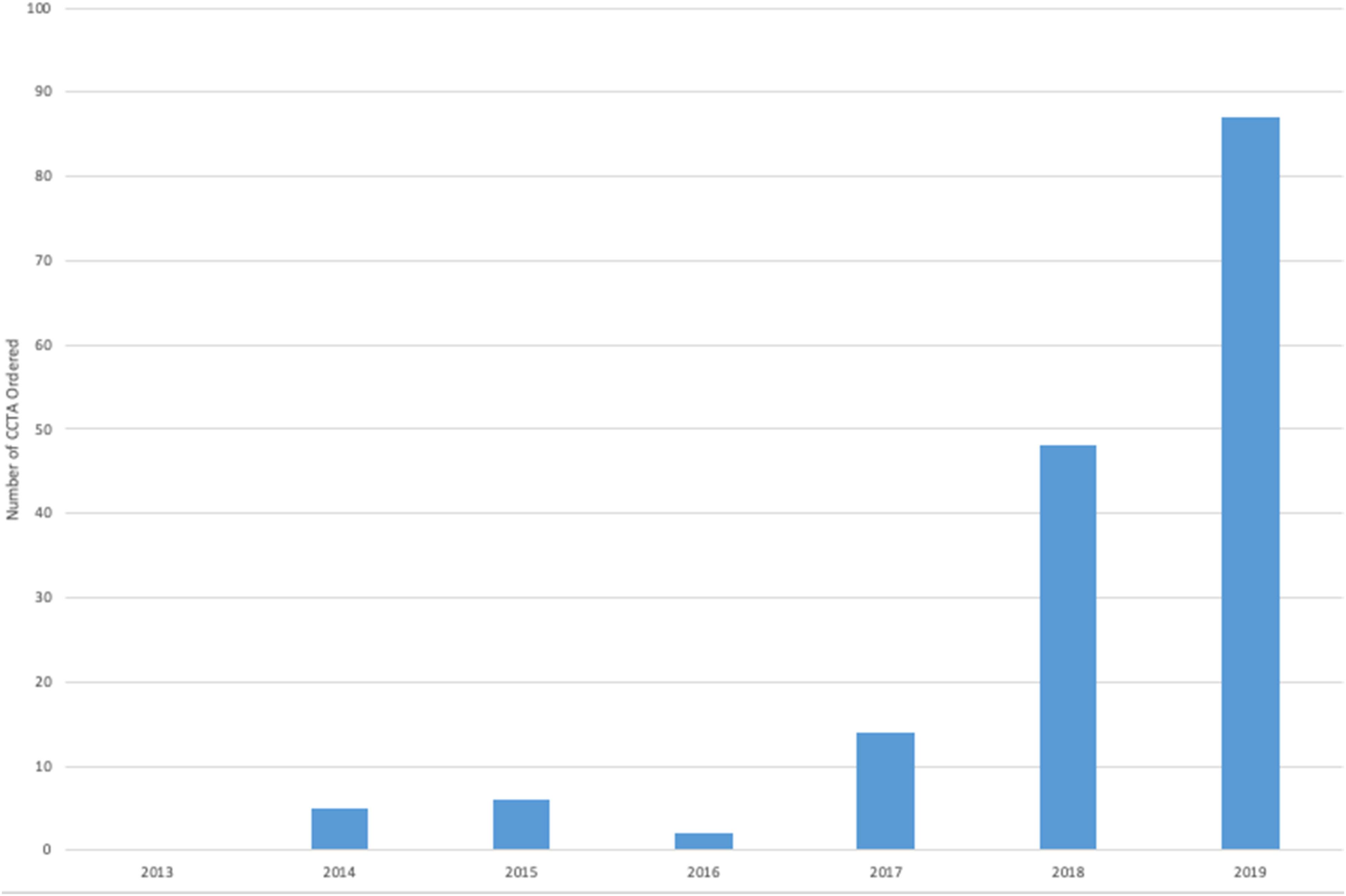
Appendix 2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.