
Abstract
Purpose:
To identify patient and procedural factors associated with extrusion of the Dacron cuff from the subcutaneous tunnel of tunneled hemodialysis catheters (THDCs).
Materials and methods:
Single center 5-year retrospective analysis of 625 catheters in 293 adult patients. Patient data included age, gender, body mass index (BMI), and common comorbidities. Procedural details included type of procedure (new insertion vs. exchange), operator seniority, side of insertion, catheter model and presence of catheter wings skin-sutures. Complications were reported as cumulative risk over time and Cox proportional hazards model was used to evaluate risk factors for cuff extrusion (CE).
Results:
Median patient follow-up was 503 days (188,913 catheter-days) and median catheter survival 163 days. CE occurred in 23.8% of catheters, at a rate of 0.79 per 1,000 catheter-days and a median time of 64 days. It was more common than infection (14.6%) and inadequate flow (15.5%). The 1-month and 12-month risk of CE was 5.9% and 21.3% respectively. A first episode of CE was a strong predictor of future CE episodes. The only patient factor that affected the risk of CE was BMI (Hazard Ratio 2.36 for obese patients). Procedural factors that affected the risk of CE, adjusted for BMI, were catheter model, type of procedure (lower risk for new insertions) and catheter wings skin-sutures; the latter reduced the 30-day CE risk by 76% without increasing catheter-related infections.
Conclusion:
Cuff extrusion is common in long-term THDCs. The risk increases with obesity, history of previous cuff extrusion, certain catheter models and absence of wing-sutures.
Introduction
Tunnelled hemodialysis catheters (THDCs) are the most common type of vascular access for patients commencing hemodialysis in North America, and are used long-term by up to one third of patients. 1 Complications associated with THDCs are generally divided into infectious and non-infectious. This study focuses on inadvertent catheter displacement, presenting as distal extrusion of the Dacron cuff outside the subcutaneous tunnel. The term cuff extrusion (CE) encompasses all cases where the Dacron cuff is visible outside the tunnel, either completely or partially, and includes those cases where the entire catheter is outside the body (catheter fall-out). This non-infectious complication is well documented for peritoneal dialysis catheters2,3 and its incidence has been reported for hemodialysis catheters in pediatric populations with incidence of up to 25% 4 and a rate of 2.4 episodes/1,000 catheter-days. 5 For adult patients, although it has been previously mentioned in the literature,6-9 it has never been the focus of attention and some publications do not discuss it as a possible complication.10,11 The purpose of this study was to examine CE cases in the adult population and to identify patient and procedure-related factors that may be associated with CE of THDCs.
Materials and Methods
Patient Population
This was a retrospective analysis of all THDC insertion and THDC exchange procedures performed in one Interventional Radiology (IR) department during a 5-year period (October 2013 through September 2018). Search of the local PACS (Picture Archiving and Communications System) identified 1103 procedures, performed on 596 patients (Figure 1). These results were cross-referenced with the DMARTM database (Dialysis Measurement Analysis and Reporting), in order to identify only those patients who received their first THDC during the 5-year period (n = 447). Exclusion criteria were patients with less than 90 days of follow-up available, those who died within 90 days of first THDC insertion, those who required a THDC for less than 90 days, those who had their first THDC inserted at a different institution, those with absent procedural details, and those with THDC placed outside the internal jugular vein (IJV). A total of 293 patients were enlisted and their characteristics are presented in Table 1.
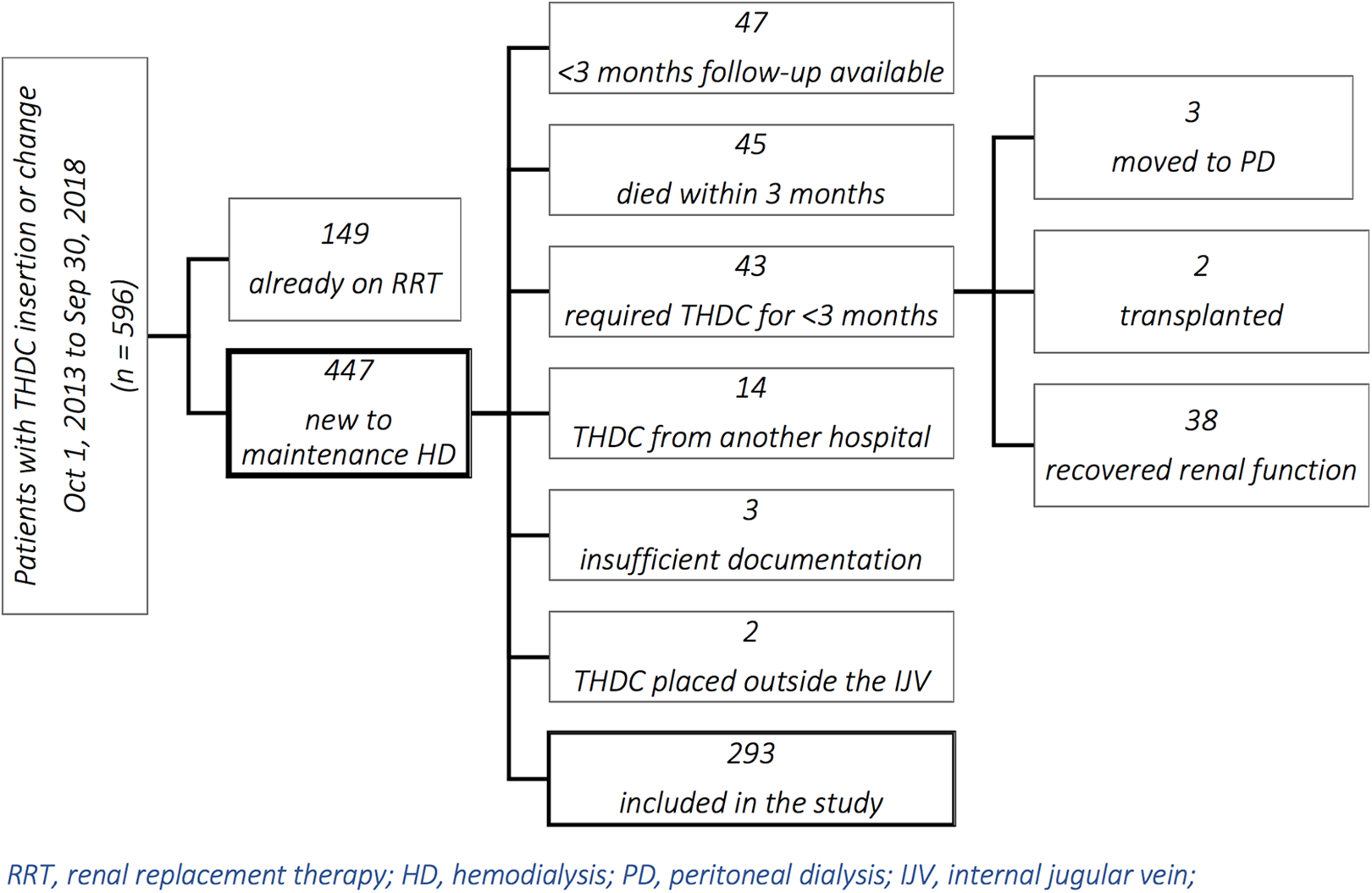
Cohort creation flowchart.
Demographics by Subset of Subjects With and Without at Least One Cuff Extrusion During Follow-Up Period.
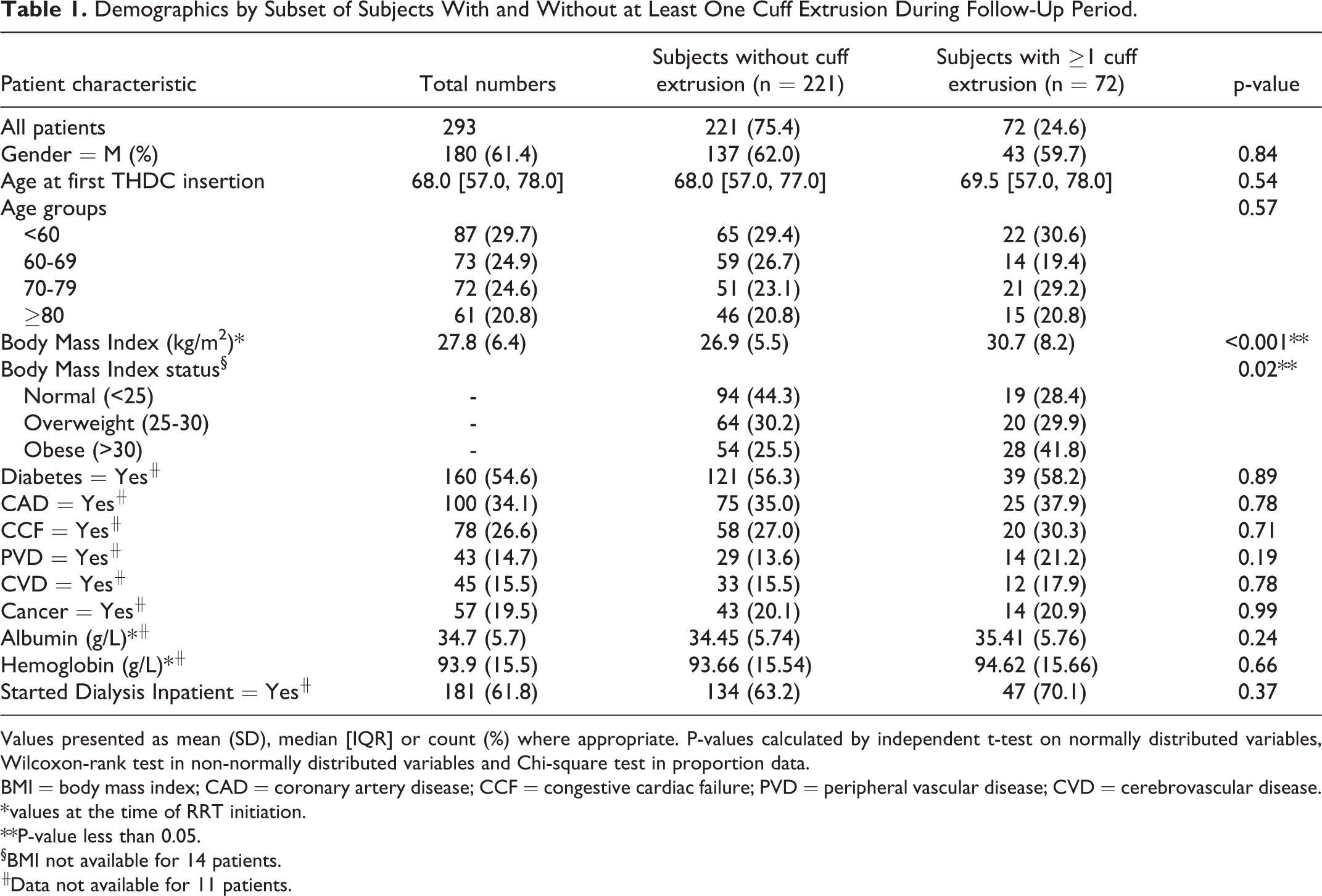
Values presented as mean (SD), median [IQR] or count (%) where appropriate. P-values calculated by independent t-test on normally distributed variables, Wilcoxon-rank test in non-normally distributed variables and Chi-square test in proportion data.
BMI = body mass index; CAD = coronary artery disease; CCF = congestive cardiac failure; PVD = peripheral vascular disease; CVD = cerebrovascular disease.
* values at the time of RRT initiation.
**P-value less than 0.05.
§BMI not available for 14 patients.
╫Data not available for 11 patients.
Patients were followed-up from the date of their first THDC insertion through September 2019, or when the first of the following occurred: patient death, patient moved out of program, elective catheter removal (no longer needed because of recovery of renal function, renal transplant, transition to peritoneal dialysis or to a different vascular access, progression to palliative care).
Data Sources
The local PACS provided the procedural details and the indication for each procedure. The DMARTM system is a prospective database that provided the information about patients’ baseline demographics, comorbidities and laboratory investigations; DMARTM also documents any vascular access related procedure or any change in a patient’s status (e.g., transferred to peritoneal dialysis, moved out of program, received renal transplant etc.), and these are updated every 90 days by dialysis nurses and reviewed by a medical expert (Author MO).
The research protocol was approved by the institution’s Research Ethics Board.
THDC Insertion Procedure
All THDCs were inserted in the IR department, either by staff interventional radiologists (n = 314) or IR fellows (n = 311). Operator experience varied from less than 3 years of IR practice for the fellows and 1 staff radiologist, to more than 10 years for the other 3 staff radiologists. Insertion technique varied only slightly between operators and followed the conventional interventional radiological method, as described in several publications,12,13 using ultrasound guidance for the venous puncture and fluoroscopic guidance for the remainder of the procedure. The length of the tunnel and the location of the skin exit site were measured using a calibrated 0.038” wire. A transverse incision was made at the skin exit site, approximately 10 mm long. The intent was to position the Dacron cuff between 1 cm and 2 cm above the skin exit site, and this was documented in the procedural report; however, cuff position and the width of the skin incision could not be verified for the purposes of this review, and it is possible that some operators and/or procedures resulted in a deeper or shallower cuff implantation. Catheters were secured with a monofilament absorbable suture (3-0 Biosyn, Covidien, Dublin, Ireland) using an intradermal purse-string suture at the tunnel exit site, similar to that described by Bond & Bond. 14 Only in selected cases, at the operator’s discretion, the wings of the catheter were sutured to the chest wall using a non-absorbable monofilament suture (2-0 Surgipro, Covidien, Dublin, Ireland); in such cases, only one suture was used, anchored to the skin very close to the exit site of the tunnel, as opposed to suturing each wing individually to the chest wall underneath it (Figure 2). This allowed the catheter to be lifted and easily cleaned underneath. These non-absorbable wing-suture were removed by HD nurses at the interval specified in the radiology report, which varied between 2 and 8 weeks, at the operator’s discretion. The data regarding these procedural details was collected from the radiological report.
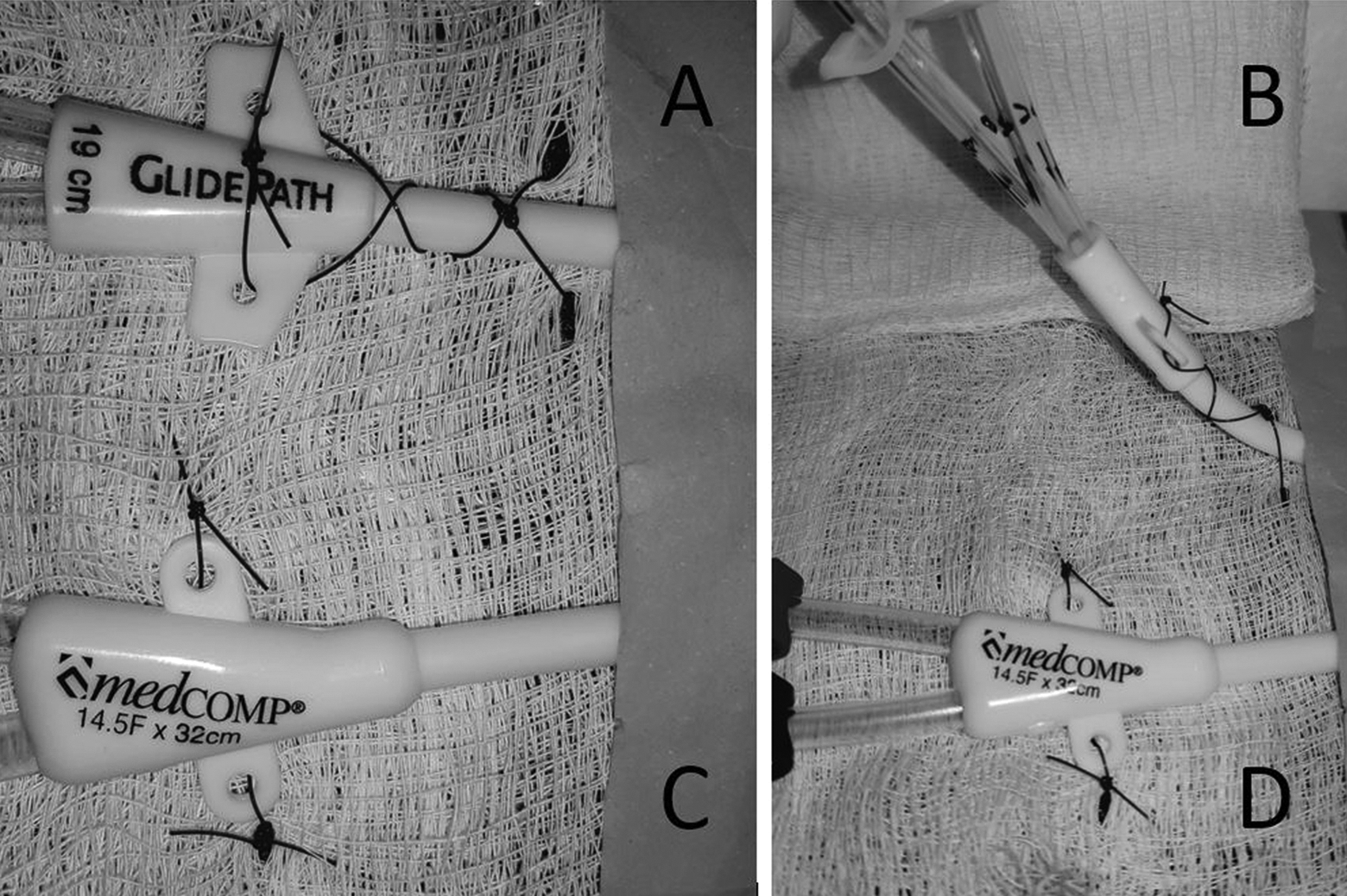
Example of wing-suture used to anchor catheters to the skin. The single suture next to the tunnel exit site (A) allows the catheter to be lifted and cleaned underneath (B), as opposed to suturing the wings individually (C and D).
Baseline Data
Patient data collected at baseline included age at time of first THDC insertion, gender, body mass index (BMI), comorbidities (diabetes, coronary artery disease, congestive cardiac failure, peripheral vascular disease, cardiovascular disease, cancer) and laboratory values (hemoglobin, albumin) at the time of commencing renal replacement therapy (RRT), and whether RRT commenced during a hospital admission.
Procedural details collected included type of procedure (new insertion via new tunnel and new venipuncture (irrespective of the patient’s history of previous catheters), or exchange over the wire (eOTW) via existing tract and existing venipuncture), operator seniority (fellow or staff), side of insertion (right or left IJV), model of THDC used and whether the catheter wings were sutured to the skin.
Outcomes
The primary outcome was catheter exchange or removal due to CE. Secondary outcomes were catheter exchange or removal due to catheter related infection (both blood stream infections and skin/exit site infection) or due to inadequate flow.
Statistical Analysis
Descriptive statistics were presented as mean (Standard deviation (SD)) and median (Interquartile Range [IQR]) for continuous variables and frequency (%) for categorical variables. All descriptive statistics were compared by T-test and Wilcoxon Rank-sum tests for continuous variables, and Chi-square test for categorical variables.
A cumulative incidence function was used to estimate the risk of requiring a second THDC exchange due to CE after an initial episode of CE. Competing risks (events that may occur before the primary event of interest, i.e. a second THDC exchange), were defined as death, catheter change due to other reasons, catheter no longer required and other causes. Censoring events were defined as lost to follow-up or end of follow-up period. Failure to account correctly for competing risks by using Kaplan-Meier estimates generally results in overestimation of the probability of occurrence of the event of interest. 15 Hazard ratios (HR) and 95% confidence intervals (95% CI) for the risk of having a CE due to baseline characteristics were modeled by unadjusted and adjusted Cox proportional hazard models with the outcome (CE) as recurrent event. Adjusted models included presence of wing-sutures, BMI, and intervention type. All predictors included in the model were time invariant. In this analysis patients were censored due to death, transplant, and recovery of kidney function, or transition to peritoneal dialysis, transfer, lost to follow-up or for reaching the end of the study without developing the outcome.
Patients with at least one CE were used to estimate the effect of wing-sutures and of operator seniority on the risk of presenting with early CE (less than 30 days from insertion). Odds ratios and 95% CI were estimated by logistic regression model with presence of wing-sutures (yes vs. no) and operator seniority as predictors and CE before 30 days (yes vs. no) as outcome. Both models were adjusted for BMI and intervention type (new THDC insertion or eOTW).
Missing data on baseline characteristics was assumed to be missing at random and was not imputed.
All statistical analyses were performed in R software, version 3.6.3.
Results
A total of 625 procedures, in 293 patients, were included in the analysis and consisted of 374 new catheter insertions (59.9%) and 251 eOTW (40.1%).
Population characteristics are included in Table 1. Median patient follow-up time was 503 days (IQR 243, 948) with a mean of 645 days (SD = 499) resulting in a total of 188,913 catheter-days. Fifty-one patients were lost to follow-up before the end of the study period. Median catheter survival was 163 days, (range 1-1963, IQR 58, 406).
CE was the most common complication, encountered in 149 catheters out of 625 (23.8%), in 72 of the 293 patients (24.6%), at a rate of 0.79 per 1,000 catheter-days. In comparison, infection and inadequate flows were seen in 91 catheters (14.6%), 63 patients (22%), 0.48/1,000 catheter-days and 97 catheters (15.5%), 51 patients (17%), 0.51/1,000 catheter-days respectively. The mean number of CE per patient was 0.51 (±1.12), with a maximum of 7 per individual. A total of 221 patients (75.4%) reached the end of follow-up without reporting cuff extrusions, 34 patients experienced only one, 17 experienced 2 and 21 reported more than 3.
Median time to CE was 64 days (IQR 28, 181). Early CE was seen in 39 catheters (27 patients). The probability of CE gradually increased with time, from 5.95% at 1 month, to 17.8% at 6 months and 21.3% at 1 year, followed by a slow, continued rise to 26.7% at 5 years (Figure 3).
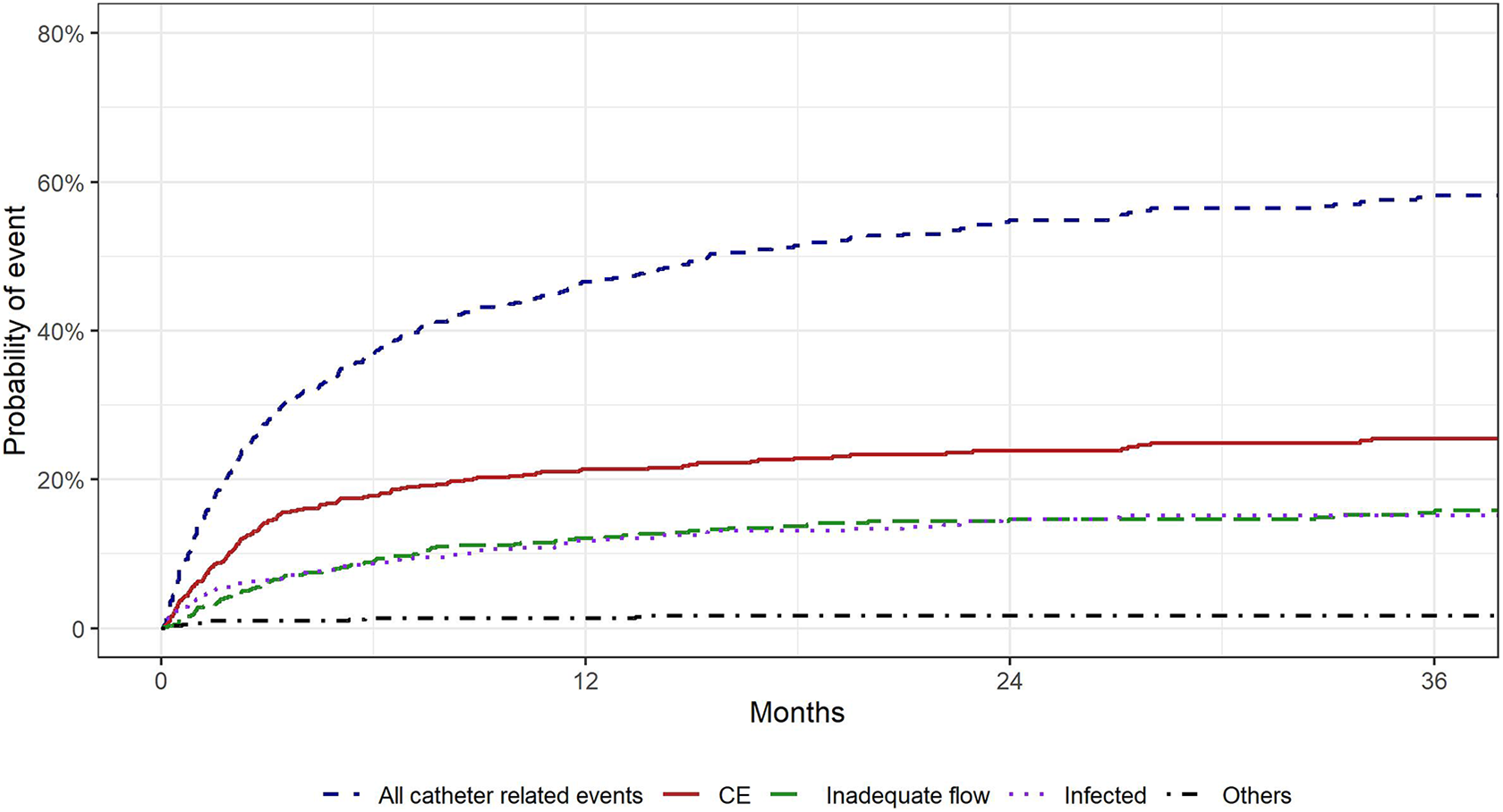
Probability of catheter related complications over time.
Patient Factors
A direct correlation was observed between BMI and incidence of CE; compared to patients with normal BMI (18.5-24.9), those overweight (BMI ≥25) had a HR of 1.93 (95% CI, 1.02-3.66), while obese patients (BMI >30) had a HR of 2.36 (95% CI, 1.36-4.10). The HR and statistical significance were unchanged when adjusting for presence of wing-sutures and type of intervention.
All other patient factors analyzed were found to be non-significant (Table 1).
The cumulative incidence functions showed that an initial episode of CE was associated with an increased risk of further episodes of CE (Figure 4), with a probability of a second catheter exchange being caused by CE at 1 year of 0.29, compared to 0.02 for patients that had their first catheter exchange because of other reasons (Gray’s test p < 0.001).
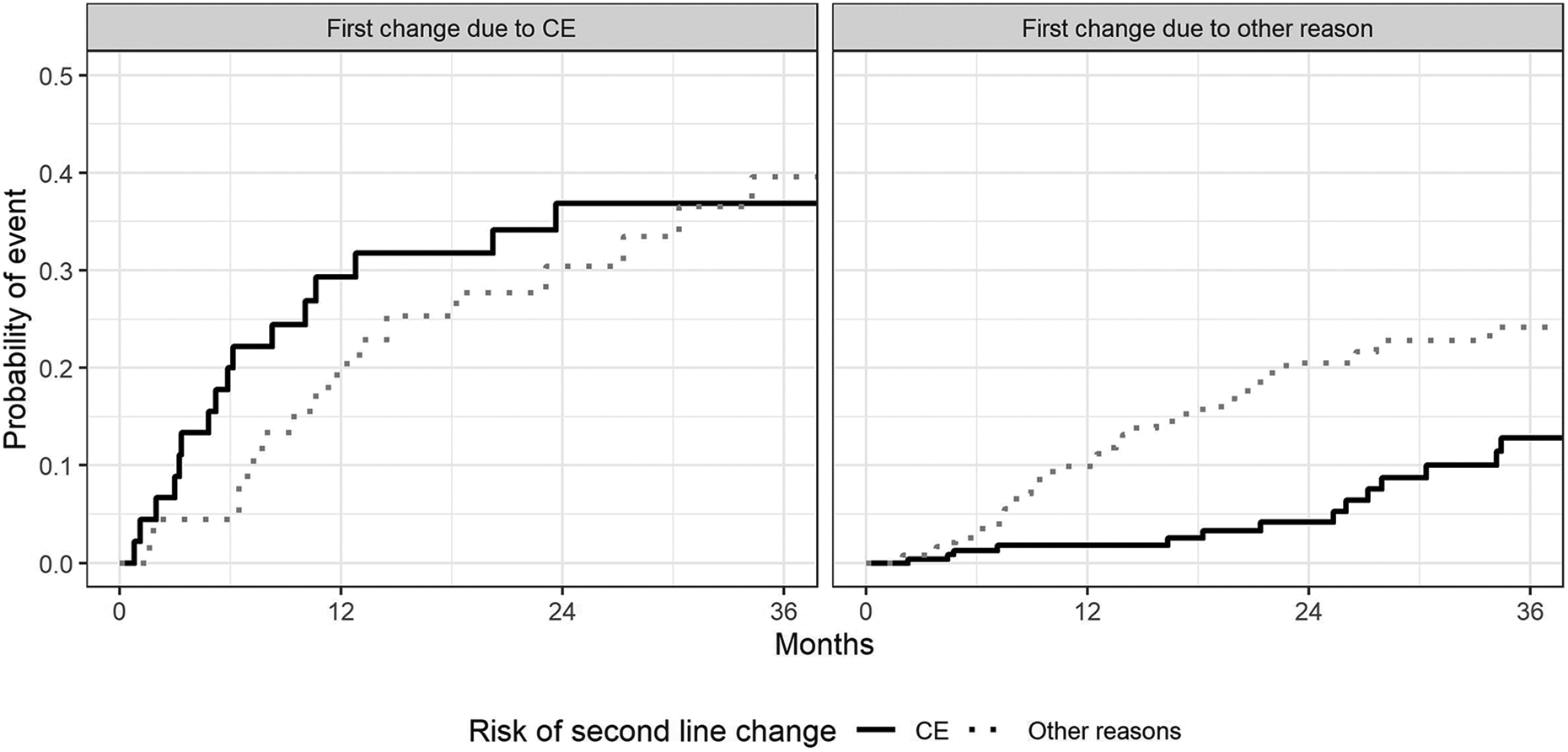
Cumulative incidence functions for risk of a second THDC change due to cuff extrusion. The black solid line represents the risk of requiring a catheter exchange due to CE; this is much greater in patients who have already had an initial catheter exchange due to CE (left graph) compared to patients who had a prior catheter exchanged due to other complications (right graph). The gray dotted line represents the risk of requiring a catheter exchange due to other complications.
Procedural Factors
The influence of procedural factors on the rate of CE is summarized in Table 2.
Catheter Outcome by Procedural Variable.
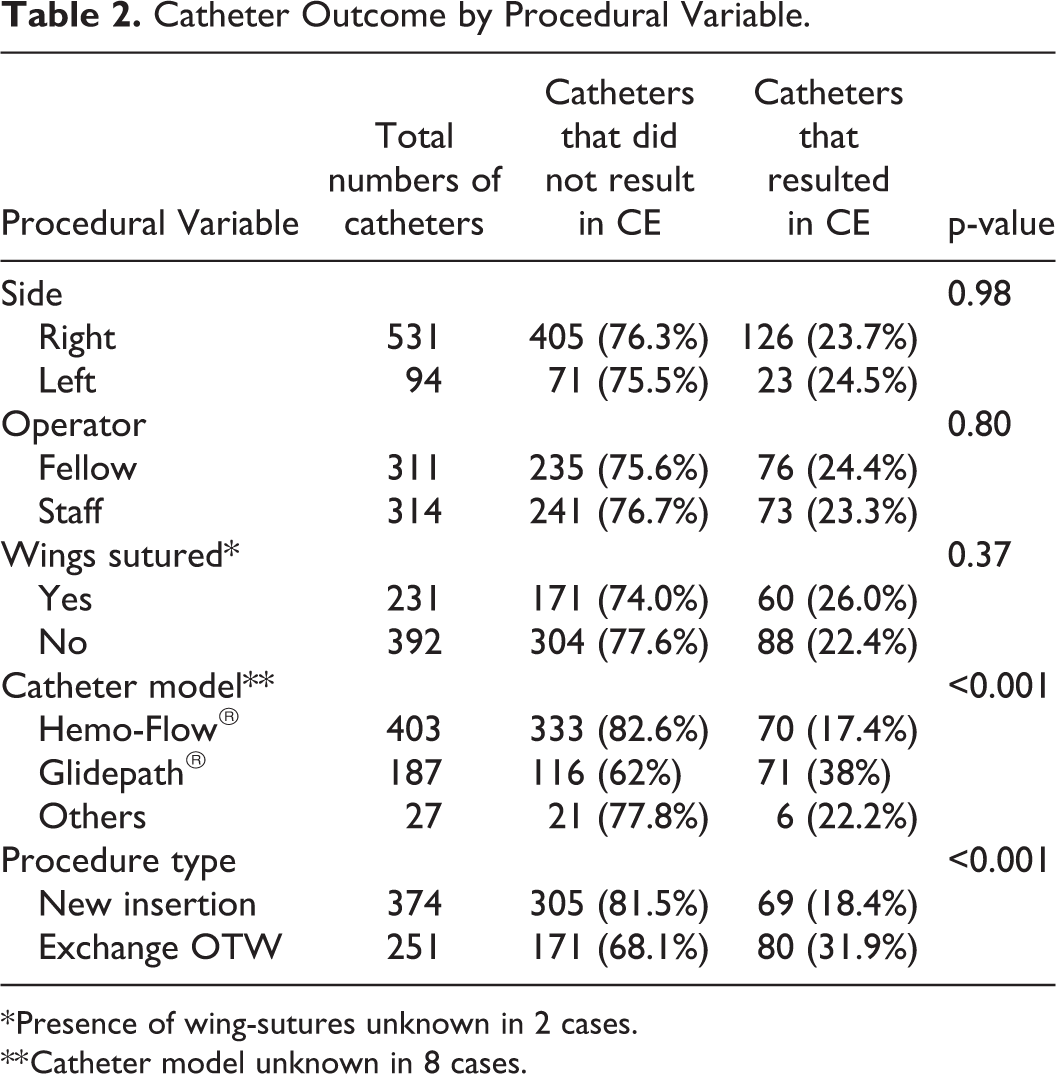
* Presence of wing-sutures unknown in 2 cases.
** Catheter model unknown in 8 cases.
Catheter wing-sutures
Suturing the catheter wings to the skin reduced the risk of early CE by 76% (Odds Ratio 0.24, 95% CI, 0.1-0.6; p = 0.002). Of the 231 THDCs that had the wings sutured, only 7 (3.0%) resulted in CE within 30 days, compared to 7.9% of those THDCs without wing-sutures (31 out of 392; note that in 2 cases, presence of sutures was unknown). Wing-sutures were not associated with an increase in THDC-related infection (Adj OR 0.81, 95% CI, 0.29-2.13, p = 0.31).
Procedure type
The risk of CE was significantly lower for new THDC insertions compared to eOTW (HR 0.38, 95% CI, 0.26-0.56, p < 0.001), even after adjusting for BMI and presence of wing-sutures. A statistically significant benefit of new insertions over eOTW was also seen in the subset of patients with repeated episodes of CE (n = 38, events = 115).
Catheter type
Four different catheter models were used during the 5-year period covered by this study and CE occurred with all of them. Hemo-Flow® (Medical Components, Inc., Harleysville, USA) and Glidepath® (Bard Peripheral Vascular Inc, Tempe, USA) accounted for almost 95% of the total THDCs in the study and were used during the same period; the choice of catheter model was dictated by the department’s stock at the time of the procedure. CE occurred with 18% of Hemo-Flow® catheters and 39% of Glidepaths®. The risk of CE with Hemo-Flow® was 74% lower compared to the Glidepath® (HR 0.26, 95% CI, 0.18-0.39; p < 0.05); the estimated HR remained similar after adjusting for BMI, presence of wing-sutures and type of procedure (HR 0.30, 95% CI, 0.21-0.44).
Side of insertion (Adj HR 0.69, 95% CI, 0.41-1.13, p = 0.14) and operator seniority (fellow vs. staff Adj HR 0.88, 95% CI, 0.65-1.20) were non-significant. The latter also did not influence the risk of early CE (Adj OR 0.88, 95% CI, 0.4-1.94, p = 0.75).
Discussion
This study focused on identifying risk factors for CE of long-term THDCs, a complication rarely discussed in the literature. This was found to be a frequent complication, occurring in almost 25% of patients, especially those overweight or obese, but independent of age, gender, or comorbidities. Importantly, patients who experience 1 episode of CE were found to be more likely to suffer future episodes of CE—over 77% of dislodged catheters (115 of 149) occurred in just 38 patients. The study also identified procedural factors that increased the risk of CE, mainly the lack of wing-sutures, catheter eOTW, and certain models of catheter.
While CE has been quantified in numerous previous publications (Table 3), it is not always a complication mentioned in adults.10,11,16 The published literature also shows that incidence can vary greatly, ranging from 0.75% to 19.0% of catheters, or 0.08 to 3.73 per 1,000 catheter-days,8,9 with higher rates in the pediatric population (up to 24% of THDCs and 2.4 per 1,000 catheter-days). 5 In this study’s adult elderly cohort, CE incidence was 0.79 per 1,000 catheter-days; however, a large proportion of these THDCs suffered from this complication, 23.8% (149 of 625), which is similar to figures reported for pediatric populations4,5 and for femoral THDCs. 9 Of these, 39 catheters were displaced in the first 30 days after insertion, which was considered early CE. The 30-day cut-off was chosen based on the authors’ experience and previous publications, 9 as the time required for the Dacron cuff to be incorporated in the tunnel lies between 2 and 4 weeks. For these cases of early CE, we scrutinized the insertion technique. Size of the skin incision, position of the cuff in the tunnel and method of suturing, all could play a role in the risk of early CE. Suturing the wings was not routinely used in this cohort, in an effort to reduce the rate of catheter related infection. However, our results show that such sutures are highly effective in reducing the risk of early catheter dislodgement, by as much as 76%, without increasing the infection rate. The position of the cuff within the tunnel has been shown to influence the rate of dislodgement, with more frequent cases when the cuff is less than 2 cm from the skin exit site. 17 In this study, the operators’ intention was to position the cuff 1 to 2 cm from the skin exit site.
Summary of Previously Published Studies Documenting Cuff Extrusion or Catheters Falling-Out.‡‡
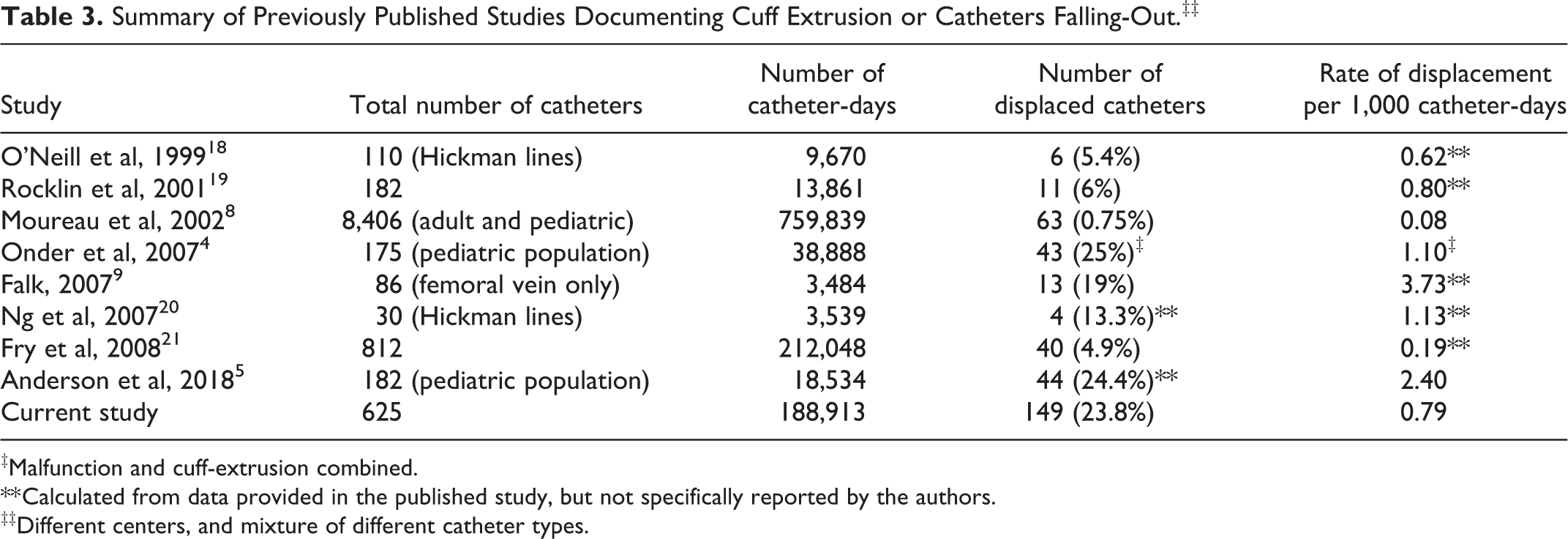
‡Malfunction and cuff-extrusion combined.
** Calculated from data provided in the published study, but not specifically reported by the authors.
‡‡Different centers, and mixture of different catheter types.
After the initial 30 days, one would expect incorporation of the cuff in the tunnel and, therefore, a reduced risk of CE with increasing time. However, this study found the probability of CE rose sharply and constantly throughout the first year, from 5.9% at 1 month to 21.4% at 1 year. In this cohort, 73.8% of cuff extrusions (110 of 149 catheters) occurred more than 1 month post-insertion (median 93 days), suggesting inadequate tissue growth around the Dacron cuff, which could be related to patient factors, or catheter related factors, or a combination of both.
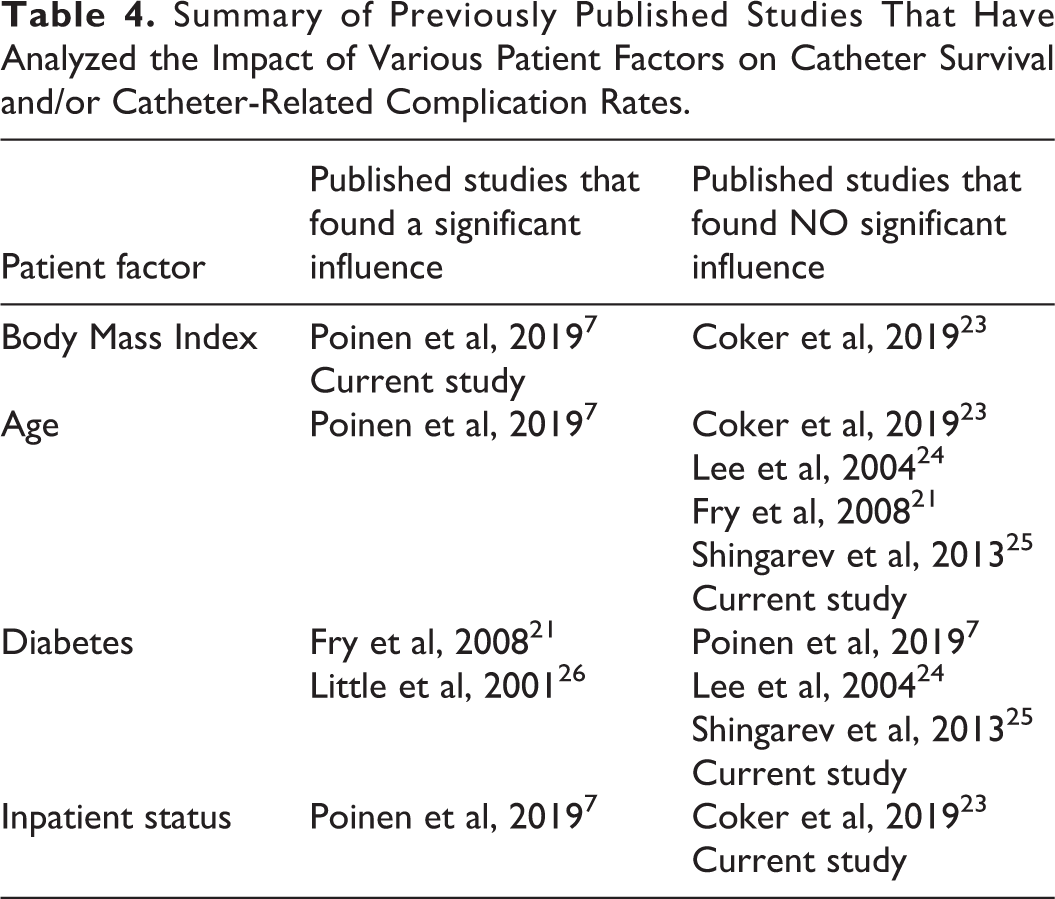
Several published studies have analyzed the impact of various patient factors on catheter survival and/or complication rates, but without reaching a consensus (Table 4), suggesting that other factors, not yet investigated, may play a significant role. Such a factor could be the catheter model, which was found to influence the risk of CE in this cohort. While this complication occurred with all the different models used, comparison of the 2 most used catheters showed a much higher risk of CE with Glidepath®, compared to Hemo-Flow®. Although not a randomized study, these findings were statistically significant after adjustment for various confounding factors. One hypothesis is that this finding is related to the design of the Glidepath® Dacron cuff, which has a lower-profile and smooth surface when compared to the Hemo-Flow® cuff, and this may hinder tissue adherence to the cuff. Other authors have reported issues with respect to Dacron cuff construction in certain types of catheters 22 and although the mechanism of this statistically significant result is unclear, our hypothesis is that it relates to cuff design.
Summary of Previously Published Studies That Have Analyzed the Impact of Various Patient Factors on Catheter Survival and/or Catheter-Related Complication Rates.
There are several limitations to the present study. It represents the experience from a single center, conducted in a Canadian population that tends to have higher THDC use; therefore, conclusions may not apply to other institutions or territories. It is also a retrospective study, not randomized, therefore results regarding performance of different catheters or different operator groups should be interpreted cautiously. The study focused on the chronic hemodialysis population, which is why patients that used the catheter for less than 90 days were excluded; however, this limits the ability to report early complications. Furthermore, only certain patient factors that seemed intuitively relevant were examined, but many others may play a significant role, such as patient medication (e.g., immunosuppressants), neurological or psychological conditions, socioeconomic status, etc. Studying the impact of these on catheter related complications may improve our body of evidence and ultimately, patient outcomes.
This manuscript highlights a complication that is likely underreported in the literature, but nonetheless important. CE often leads to loss of vascular access and/or catheter dysfunction that require more invasive procedures. One important finding from this study is that a patient who requires a catheter exchange because of CE is significantly more likely to require a second exchange for the same reason, compared to a patient that had the initial catheter exchanged for other reasons. In fact, over 77% of dislodged catheters (115 of 149) occurred in just 38 patients. This finding should prompt operators to adapt their technique and use preventative methods in certain patients, in order to minimize recurrent CE.
Conclusion
Cuff extrusion is an important complication of long-term THDCs. The risk is increased by obesity and history of previous CE, certain catheter models and absence of wing-sutures.
Footnotes
Declaration of Conflicting Interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.