
Abstract
Background
Transgender and non-binary (TGNB) individuals face significant discrimination and underrepresentation in healthcare, particularly within the nursing workforce. These challenges often lead to increased stress, limited career opportunities, and the concealment of identities.
Purpose
This study investigates the experiences and challenges faced by TGNB nursing students and nurses in Canada.
Methods
An online anonymous questionnaire, featuring both closed and open-ended questions, was used to gather data from participants recruited through social media and nursing networks across Canada.
Results
The survey was completed by 101 participants, with most being nursing students (54.5%) or registered nurses (20.8%), and predominantly practicing in Ontario (53.5%). While many participants were open about their TGNB identity, they reported insufficient TGNB representation and inadequate education on TGNB healthcare. Disclosing their gender identity remained difficult primarily due to fear of rejection, with 43.6% encountering barriers related to their gender identity when applying to nursing programs. Additionally, 67.3% experienced derogatory comments personally, and 66.3% witnessed similar remarks towards the TGNB community. Among 46 nurse participants, 84.7% have noticed discrimination towards TGNB patients during care and 80.4% towards a peer, colleague or superior. Only 29.7% reported to have received education on TGNB topics, which was often superficial.
Conclusions
The study reveals significant challenges for TGNB individuals in nursing education and the workforce, including discrimination, inadequate educational content, and barriers in professional settings. These findings highlight the need for more inclusive, supportive, and comprehensive education on TGNB healthcare to create a more equitable environment for TGNB nurses and patients.
Background and Purpose
Transgender individuals have a gender identity that differs from the sex they are assigned at birth (Bourns, 2019). Those with a gender identity that is not male or female may identify as having no gender, a gender other than male or female, or more than one gender, and may use the term non-binary (James et al., 2016). The recent Canadian census suggests one in 300 people in Canada over the age of 15 identify as transgender or non-binary (TGNB) (Statistics Canada, 2022); other estimates suggest that 0.6% of adults identify as transgender (Giblon & Bauer, 2017). Overall, there is significant lack of data on TGNB individuals in Canada with official estimates likely grossly underestimating the true number. This is especially likely among young people living with a family member who completed the census on behalf of the household e.g., in one survey half of self-identified TGNB young people lived with their parents (Taylor et al., 2020). It is important to note that the proportion of TGNB individuals captured in the census is significantly higher among those under 35 years (Statistics Canada, 2020). Similar findings have been reported based on US data: one US survey from 2017 showed that nearly 12% of millennials identified as TGNB (GLAAD, 2017), while another conducted in 2020 found that 1 in 4 LGBTQ youth use non-binary gender pronouns or pronoun combinations (The Trevor Project, 2020).
Access to competent healthcare allows TGNB individuals to maintain their health, and can reinforce a sense of belonging and support, both socially and institutionally. The Canadian Trans and Non-binary Youth Health Survey (TNBYHS) was completed by 1519 young people between 14 and 25 years of age, the majority of whom (70%) were 18 and above. The majority of youth surveyed planned to attend post-secondary education (Taylor et al., 2020). Therefore, for some of these youth, their experiences attempting to access healthcare will significantly impact on their own academic and professional trajectories.
TGNB youth continue to experience barriers accessing gender-affirming healthcare services (Chong et al., 2021; Clark et al., 2018; Inwards-Breland et al., 2021; Pampati et al., 2021). The Canadian TNBYHS found that 43% of participants did not receive the physical healthcare they needed, and 71% were not able to access mental healthcare (Taylor et al., 2020). A recent systematic review by Chong et al. (2021) found that TGNB youth experienced vulnerability, fear and multiple barriers when accessing healthcare services. These challenges led many youths to avoid care and engage in high-risk behaviors to initiate their transition (Chong et al., 2021). For some of these youth however, challenges acted as a catalyst to entering the healthcare field to make a difference and effect change (Eliason et al., 2018). For example, when asked about entering the field of health science, a researcher (molecular virologist) stated “I’m Black, queer, and trans non-binary. Having that personal experience, I want to bring that to the scientific space, and also go to the community and bring my scientific expertise there” (Santora, 2021, p. 2075). In a study by MacDonnell and Grigorovich (2012) one participant stated that being a transman “led me into the health sector…wanting to take care of my own health,” and another transgender participant who went into healthcare stated that “it can be helpful for trans clients. . . Having a trans-[identified. . .] worker. . . would make sense for them” (p. 5).
Overall, the voices of TGNB people are missing from the workforce. This has been attributed to their voluntary silence to protect themselves against discrimination and harassment (Beauregard et al., 2018). Most public organizations continue to operate under the gender binary with regards to organizational set-up such as restrooms and lockers room, or expectations about gender presentations (Elias et al., 2018). A national Human Rights Campaign study (United States) about workplace climates for LGBTQ individuals found that 46% of LGBTQ workers are not out at work and 59% of non-LGBTQ respondents believed it was unprofessional to discuss sexuality and gender identity in the workplace (Fidas & Cooper, 2018). Research has demonstrated that LGBTQ nurses make up a large portion of the nursing workforce, but remain invisible in practice settings, are unrepresented in nursing journals, and are pathologized or ignored in nursing curricula (Eliason, DeJoseph, et al., 2011; Goldberg et al., 2018; Kellett & Fitton, 2017; Lim et al., 2019; Merryfeather & Bruce, 2014). Hughes and Kentlyn found that the ‘don’t ask, don’t tell’ policy in healthcare settings is “so heteronormative that it is inconceivable that anyone could be non-heterosexual” (2015, p. 63).
Nurses who are out at work, meaning they are open about their gender identity, have experienced hostile and homophobic work environments causing dissatisfaction, burnout, and high turnover (Lim et al., 2019). Invisibility becomes a strategy for dealing with these stressors, but resulting tension between personal and professional identity is its own source of stress (Goldberg et al., 2018). Feeling unsafe being out at work is not only common in the healthcare sector: LGBTQ individuals working in science, technology, engineering and mathematics fields are also more likely to report not being out at work (Yoder & Mattheis, 2016). One study found that LGBT health professionals working in settings that facilitate LGBT inclusion and visibility have higher work satisfaction and retention, and engage in supportive role modeling (Sanchez et al., 2015).
Although researchers are increasingly focusing on LGBTQ health professionals, very few studies have explored the experiences of transgender nurses in the workplace. The last known study was published by Eliason, DeJoseph, et al. (2011). Though their sample focused broadly on the LGBT population, with only 1.2% of their sample identifying as transgender, this is likely a reflection of the lower level of public discourse around transgender issues at the time the study was done and as such, the study continues to have relevance today. These authors reported that their participants had witnessed discrimination and harassment in the workplace, and identified a concerning lack of workplace policies to protect LGBT staff (Eliason, DeJoseph, et al., 2011). The authors replicated their study to explore the experiences of LGBT physicians in the workplace, with a similar percentage (1%) of participants identifying as transgender (Eliason, Dibble, et al., 2011). That study revealed that LGBT physicians similarly encountered discrimination and harassment, in addition to exclusionary policies and lack of referrals from colleagues (Eliason, Dibble, et al., 2011). Meanwhile, similar work focusing on the TGNB nursing community has not been undertaken. Such work completed at present could provide valuable information about this group while also highlighting possible changes in societal attitudes. Increased visibility of transgender issues may affect the experiences of workers in general over time. LGBTQ + healthcare professionals experience additional levels of stress working in heteronormative settings with unsupportive co-workers and patients, and those who are ‘out’ in the healthcare setting are subjected to fewer promotions, negative comments, and gossip (Eliason et al., 2018). One participant who identified as a trans/genderqueer nurse commented, “I think being out is a slippery concept in my professional life” (Eliason et al., 2018, p. 566). TGNB individuals are often expected to conform to traditional gender binaries and tend to have poor support from supervisors and leaders (Elias et al., 2018).
LGBTQ students in healthcare and social service programs also experience barriers related to their sexual orientation and/or gender identity (Craig et al., 2017; Frost & Regehr, 2013). Clarke (2014) found that gay nursing students struggle to negotiate their sexuality, particularly in clinical placements. Dimant et al. (2019) found that TGNB medical students, residents, and physicians experience discrimination, lack of support, and stigma. Many have witnessed discriminatory care of a TGNB patient and feel the need to hide their identities. Mansh et al. (2015) found that only half of TGNB medical students disclose their gender identity during medical school. Kvach et al. (2021) found that TGNB individuals feel unsafe disclosing their gender identity during applications for medical residency programs and have experienced discrimination, misgendering, and misnaming. The discrimination faced by sexual and gender minority healthcare providers often starts in their educational program and continues throughout their career (O'Mahony et al., 2020). According to Levesque (2015) the nursing faculty needs to be responsible for creating an environment which is gender-inclusive and free from harm and prejudice. This approach would give TGNB students a safe place to learn and become nurses.
The voices of TGNB nurses and nursing students have recently been emerging in traditional and social media. For example, one Twitter user leverages the platform to highlight their struggles as a TGNB nurse: “being trans in nursing is the most exhausting thing I’ve ever done” (trans nursing student, 2021); and has now started a Podcast focusing on LGBTQIA + voices in nursing (trans nursing student, 2022). Another nurse was interviewed about her experiences as a trans nurse in the UK; she commented, “living as a trans person is not so easy and I felt I had to sacrifice who I was to do a job I loved” (Still, 2020).
Violence, harassment, discrimination and lack of support in education and workplace among TGNB individuals have been associated with suicidal thoughts and behaviors (Eustaquio, 2024; Haas et al., 2014; James et al., 2016). In Canada, gender and sexual minority adolescents are found to be at increased risk of suicidal ideation and suicide attempt compared with their cisgender and heterosexual peers (Kingsbury et al., 2022). The findings of a recent study in the U.S. indicate that transphobic laws and attitudes negatively impact the mental health of transgender individuals. These conditions can lead to higher psychological distress and increased suicidality (Price et al., 2024). The situation is exacerbated by the fact that TGNB people there have less access to supportive mental healthcare, making the impact of transphobic policies even more severe (Hollinsaid et al., 2024; Snow et al., 2019; TransPULSE Canada Team, 2020). While there is minimal literature about the experiences of TGNB nurses in a Canadian context, findings in the national and international literature highlight the urgent need to explore the experiences of TGNB nurses and to understand these experiences in light of personal and professional identity. Nurses are the largest group of regulated health professionals in Canada and make up half the healthcare workforce (Registered Nurses Association of Ontario, 2017). Clarifying the experiences of TGNB nursing students and nurses in the workforce will help advance nursing knowledge and support policy development to support and protect all Canadian nurses.
The purpose of this study is to understand the experiences and issues faced by TGNB individuals attempting to access professional nursing education as well as those working or who have worked in the nursing field in Canada.
Methods and Procedures
Research Design and Ethics Approval
This study used an online design and data was collected using an anonymous questionnaire. The study was approved by the ethics boards at all the authors’ institutions. Information about the study, including purpose, risk and benefits was provided to the participants in an information sheet and in the consent form and informed consent was obtained through an online consent. Each participant received a $25 honorarium for completion of the survey.
Setting and Sampling
This study took place in Canada and was administered using Google Forms. Participants were recruited using social media platforms and nursing networks such as Two-Spirit, Lesbian, Gay, Bisexual, Transgender and Queer (2SLGBTQ) Nursing Interest groups. Potential participants were invited if they met the inclusion criteria: self-identify as TGNB, a nursing student or nurse (RPN, LPN, RN, or NP) or former nurse in Canada. They also had to be able to communicate in English.
Data Collection and Analysis
The survey was developed by the research team and includes questions from the survey developed by Dimant et al. (2019) who provided permission for its use. The survey collected data using closed-ended questions about demographic variables such as gender identity, province/territory of work, age, type of nursing license, and workplace setting (hospital, primary care, community, public health). Open ended questions probed about experiences with discrimination, barriers and facilitators in the workplace, and disclosure of gender identity.
The data from the questionnaires were entered into and analyzed with the Statistical Package for the Social Sciences (SPSS). Descriptive statistics were employed to characterize categorical variables through the use of percentages. Inferential statistics were employed to discern associations between variables, utilizing crosstabs to reveal any significant relationships. A portion of the survey developed by Dimant et al. (2019) used questions from the validated tool the Nebraska Outness Scale, which was modified for TGNB individuals, under which NOS-D (Disclosure subscale) and NOS-C (Concealment subscale) tests were administered.
Results
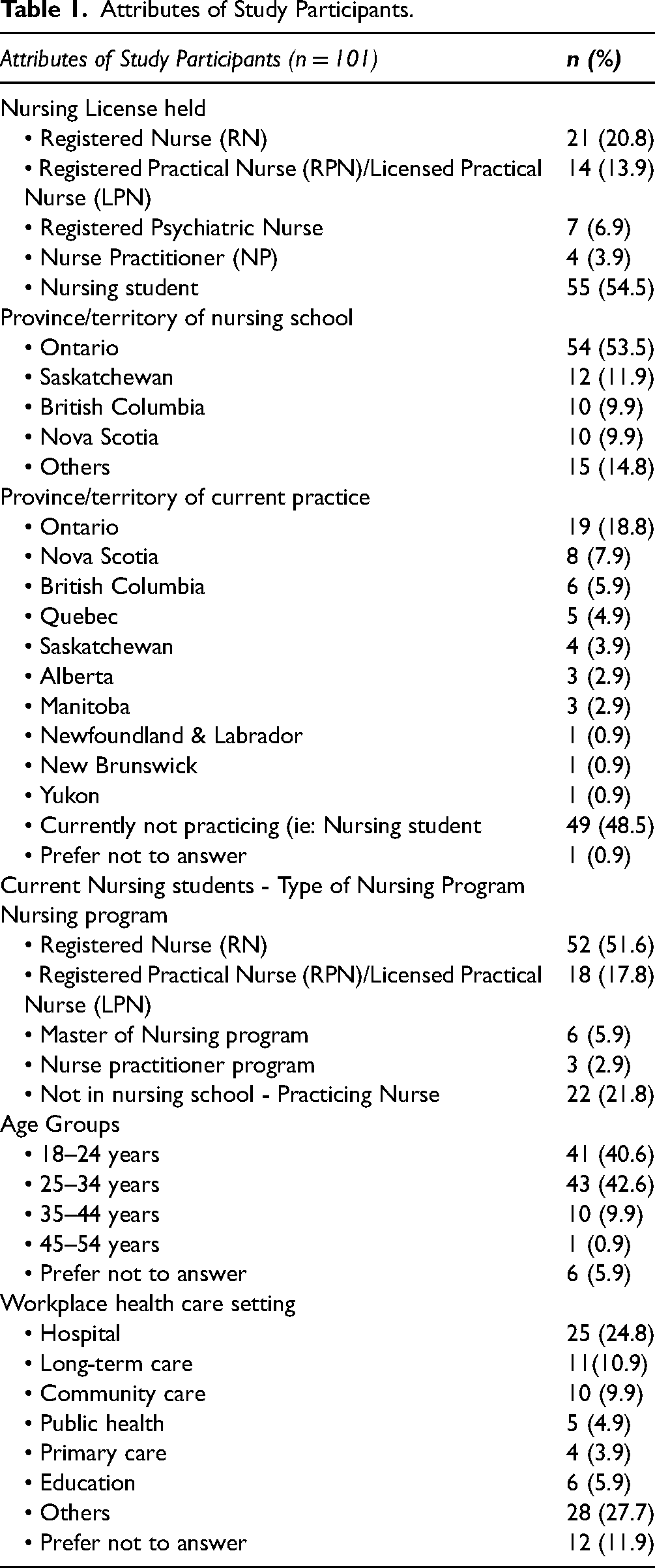
A total of 119 individuals initially accessed the survey, out of which 114 passed the eligibility question (identified as TGNB). A final response rate of 101 participants proceeded to share their experiences as TGNB persons. The basic attributes of the study participants are given in Table 1. A glossary of terms (Table 2) is provided.
Attributes of Study Participants.
Glossary of Terms.
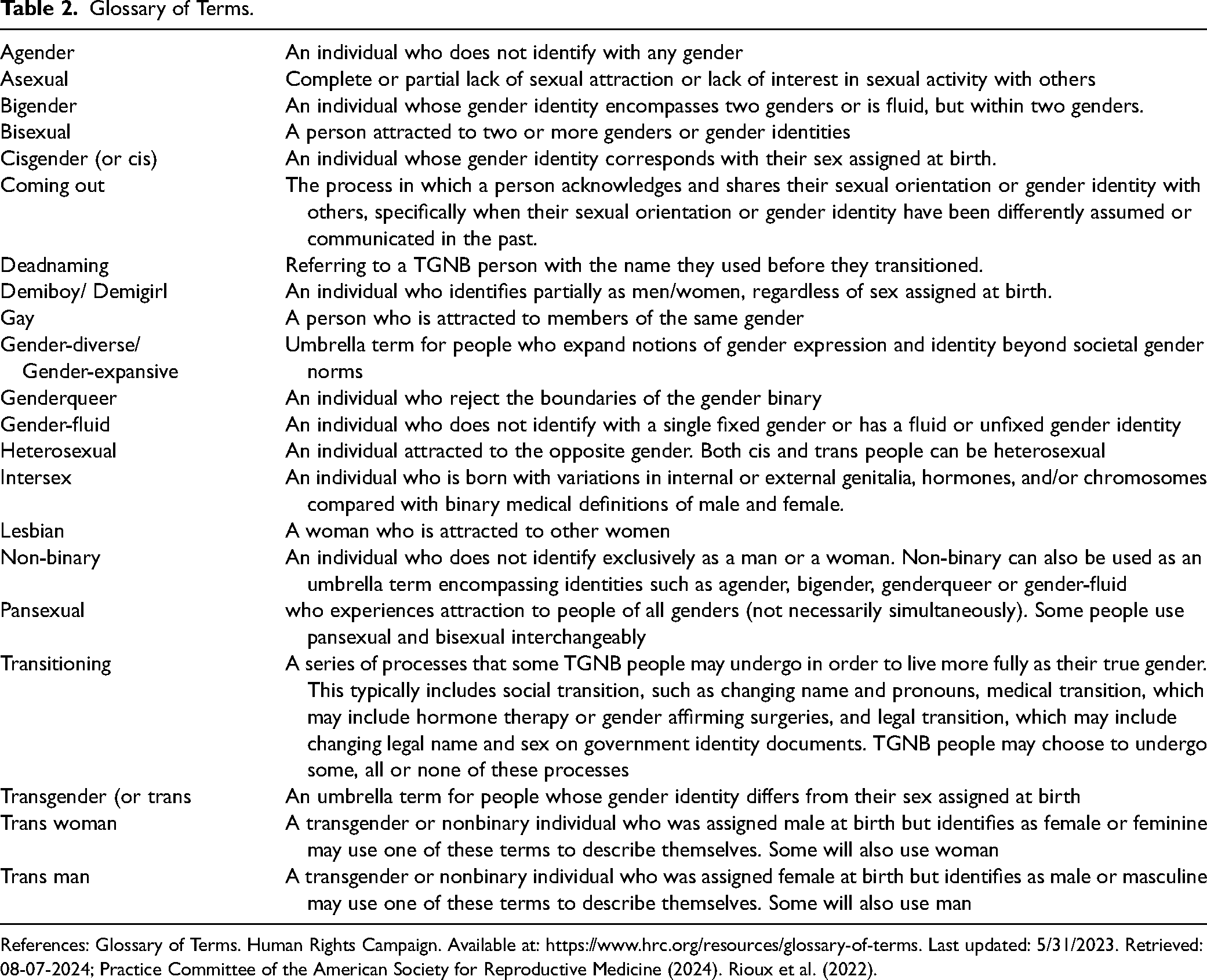
References: Glossary of Terms. Human Rights Campaign. Available at: https://www.hrc.org/resources/glossary-of-terms. Last updated: 5/31/2023. Retrieved: 08-07-2024; Practice Committee of the American Society for Reproductive Medicine (2024). Rioux et al. (2022).
Participants were asked to identify their sex assigned at birth and their current gender identity. Among the participants, a majority were assigned female at birth (n = 75, 74.3%), while 23 (22.8%) were assigned male at birth. One participant (0.9%) was designated as intersex at birth, and the rest (1.9%) chose not to disclose their sex assigned at birth. When asked about their current gender identity, the majority identified as non-binary (n = 28, 27.8%), followed by trans men (n = 23, 22.8%), trans women (n = 20, 19.9%), gender queer (n = 16, 15.9%), gender fluid (n = 10, 9.9%), women (n = 2, 1.9%), men (n = 1, 0.9%), and demi-boy (n = 1, 0.9%). The current sexual/ romantic orientation of the respondents was also recorded. Most of the respondents identify their sexual and/or romantic orientation as bisexual (n = 35, 34.9%), followed by pansexual (n = 19, 18.9%), queer (n = 16, 15.9%), lesbian (n = 14, 13.9%), asexual (n = 9, 8.9%), heterosexual (n = 4, 3.8%), gay (n = 3, 2.8%) and queer/bisexual (n = 1, 0.9%).
Experiences of TGNB Individuals in Nursing School
In the survey, participants were asked whether they were open about their TGNB identity when applying to nursing school. A total of 95 respondents answered this question, with 76 (80%) of them indicating that they were out as TGNB while in nursing school. Out of these 76 participants, the largest group (n = 35; 36.8%) fell within the age range of 25–34 years. For those participants who were not open about their TGNB identity during the application, they were asked to provide the reasons behind their decision. The majority of these individuals (n = 8, 8.4%) mentioned that they were either confused and still figuring out their gender identity or chose to conceal their identity due to discomfort and the fear of potential rejection.
Diversity and Inclusivity in Nursing Education and Practice: TGNB Representation and Its Impact
Participants were asked if they were aware of or knew any other TGNB nursing students in their nursing school. Out of 65 respondents, 11 (16.9%) were not aware of any, while 40 (61.6%) reported there being 1 to 5 other TGNB nursing students in the nursing school. Additionally, 13 (20%) respondents indicated the presence of 6 to 10 TGNB nursing students, and 1 (1.5%) respondent reported having more than 10 TGNB nursing students in their school.
Similarly, participants were asked about the number of TGNB faculty or staff members working in their nursing school. Among the 65 respondents, 37 (56.9%) did not have knowledge of this number, while 28 (43.1%) respondents mentioned having 1 to 5 TGNB faculty or staff members in their nursing school.
Participants were asked about the presence of TGNB nursing or other healthcare colleagues working alongside them in the workforce. Out of the 98 respondents to this question, 35 (35.7%) replied affirmatively. The effect of having TGNB nurses or nursing students at work or school, on their experience was shared by 17 of the respondents. Among these, 13 (76.5%) respondents described this effect as fostering a sense of family and unity, indicating a positive and supportive environment. Expressing themselves a respondent wrote, “In graduate school I became very close friends with the other gender expansive peer. We have got through a lot together. We talk about our issues and experiences with discrimination and encourage each other in our research”. Another respondent conveyed a similar sentiment, saying, “even if they didn’t know, I felt connected to them like I belonged”. However, four of the respondents reported that they did not experience any significant effect from the presence of other TGNB nursing or healthcare colleagues.
Educational Gaps in TGNB Healthcare Training for Nursing Students
Information regarding education related to TGNB healthcare topics was collected. All 101 participants responded to this question, with only 30 (29.7%) participants confirming that they had received education on these topics during their nursing school studies. Out of the 14 who responded regarding the duration of the education they received, 5 (35.7%) reported having received less than 5 h of education, 2 (14.3%) received between 5 to 10 h, and 7 (50%) respondents reported receiving more than 10 h of education on TGNB healthcare.
The TGNB healthcare content that was integrated into the nursing school curriculum consisted of concise education on mental health and counseling, HIV/STI prevention and care, as well as just surface-level introduction to the LGBTQ-related terminology. Meanwhile, respondents suggested essential topics necessary to be included in any healthcare professional curriculum. These would include learning about the lived experiences of TGNB individuals, open, live discussions outlining population-specific needs related to inclusivity and healthcare, specific needs, awareness activities to build understanding about the discrimination they face in healthcare, and clinical and social training targeted at building awareness about gender-affirming care, hormonal therapy and counseling processes. Commenting on the accuracy and comprehensiveness of TGNB care content provided in schools, one participant stated, “we need to move beyond definitions. It was inadequate and didn't prepare nurses for practice.” However, four participants out of 12 did find the TGNB care content in the nursing school to be comprehensive, appropriate and helpful. As per one of the respondents, “it's very good. No complaints. My institution has done an excellent job”.
Experiences of TGNB Individuals in the Nursing Workforce
Participants were asked if they disclosed their gender identity and outness as TGNB in the workplace, either as a student nurse in placement or working as a nurse. Here, participants replied as yes (n = 38); and a substantial number (n = 16; 42.1%) also belonged to the 25–34 years age group. The major reason for not disclosing their identity as TGNB was reported as fear of rejection. Participants used words such as “challenging”, “tough”, “isolating”, and “difficult” to describe their experience of identifying as TGNB in the nursing workforce. In the words of one of the respondents, “I came from a job in LTC [long-term care] where I was out and it wasn’t always positive. So, I started a new job and new identity as a man and didn’t want people to see me differently.” Another participant stated “I almost gave up”.
Another reason for not being out in the workplace, identified by participants, was that it was sometimes easier to say nothing. “I feel like I pass well; My identity is not obvious. I don’t think most people know, and so I am often treated as a cis woman”. Another participant stated, unless you work in certain niche areas that attract a lot of queer nurses or for progressive organizations, it's difficult to be ‘out’. I pass as cis so I have just always kept my work life and gender stuff separate. I think it's especially difficult given the gendered history of nursing my team uses the right pronouns (they/them). Those who are not on my direct team often misgender me. My work has been respectful and understanding. It is quite a small team (4 nurses). When I correct others, folks are responsive and don't dwell on it
Discrimination in Nursing Education and the Workforce
Out of the 101 respondents, 44 (43.6%) indicated that they encountered barriers related to their gender identity or expression when applying to nursing school. Forty-seven respondent (46.5%) reported that they did not face any barriers when applying to nursing school, where 10 (9.9%) reported “It's complicated”. Specifically, 7 (6.9%) respondents mentioned that they perceived a lack of diversity in the application process, while 6 (5.9%) respondents expressed fear of rejection related to their gender identity. As one nursing student commented, “I was rejected like four times before they finally agreed to take me in”; while another participant responded, “my application did not allow for diversity”. Among the nurse participants, 46 who responded to this question, a substantial number (n = 33) reported experiencing barriers based on their gender identity or expression when applying for nursing jobs. The barriers they faced included discrimination, harassment, delayed or no responses to their applications, as well as outright rejections. They shared experiences like, “I was denied chances in a few hospitals before getting a job”; and “many employees did not want to employ me due to my gender identity”.
Participants were asked about their experiences of hearing any type of demeaning language directed towards TGNB personnel. A majority (n = 68, 67.3%) have experienced derogatory comments directed towards them personally and 67 (66.3%) towards the TGNB community. Additionally, 18 (17.8%) and 15 (14.9%) replied positively when asked if they have heard defamatory remarks towards TGNB peers and supervisors respectively (Figure 1).
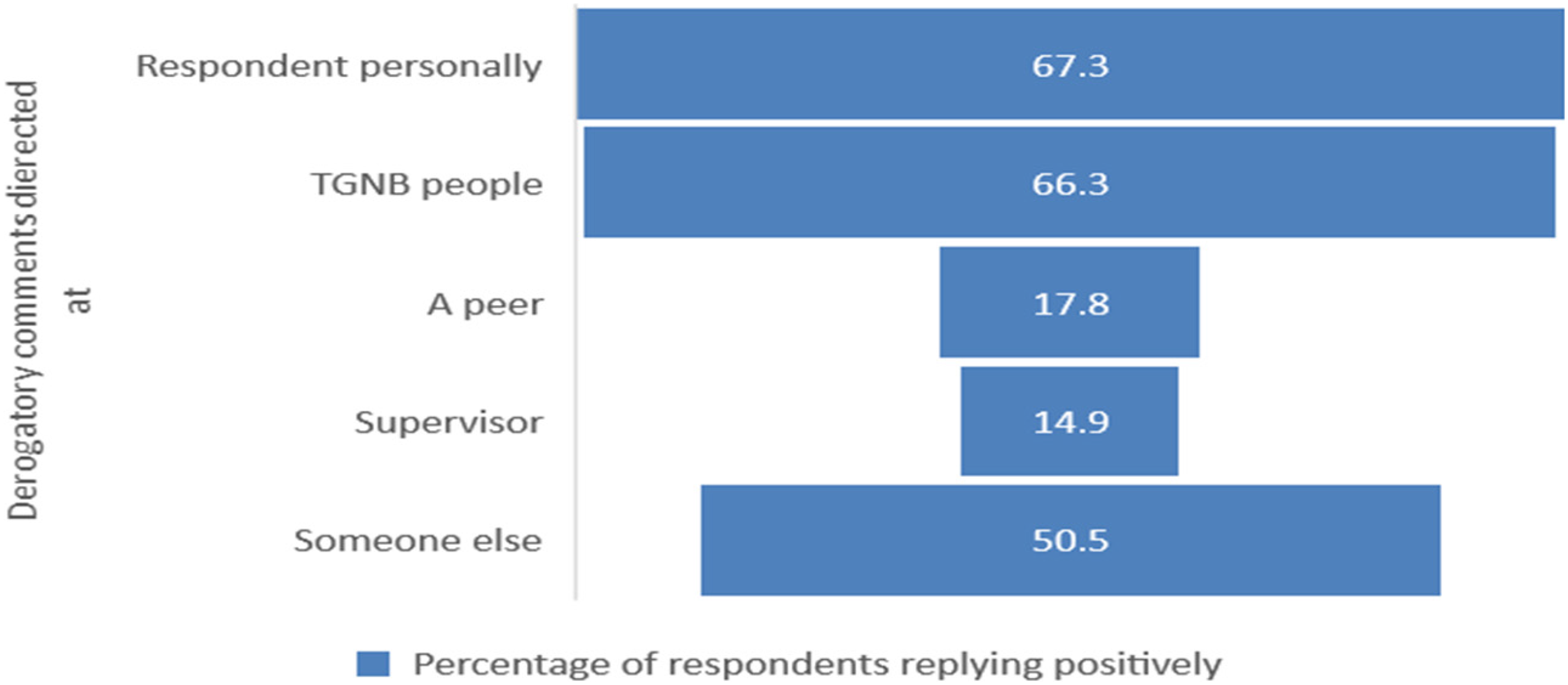
Experience of facing derogatory comments (N = 101).
The participants found the comments they received, both online and in person, to be disrespectful, hurtful, insulting and abusive. In the words of one of the respondents,
someone said you chose this path, what did you expect? Why should I have to remember your pronoun just because you changed it? Someone said I was a waste of skin…. When I returned back to work after transition, they put me in an office that had a window and then put a barrier on the window so you couldn’t look in on me
Impact of Discrimination on TGNB Nurses and Nursing Students
The impact of experiencing discrimination or harassment as a TGNB nurse or nursing student was also documented in the survey. Out of the 46 respondents, 36 expressed feeling a range of negative emotions, including “intimidation”, “heartbreak”, “disrespect”, “insult”, “demotivation”, “a sense of worthlessness”, and “feeling out of place”. One respondent shared their experience by saying, Hearing the words ‘when I looked under the hood, I was shocked to see it didn't match what was on top’ from a nurse it really shifted my perspective of people. I was horrified that a comment like that was even made, and that a person was being judged and spoken about like that
TGNB Identities and Social Circles
Figure 2 illustrates the percentage of individuals (out of an n of 95) who reported having disclosed their TGNB status to various groups of people. Only a small portion (n = 11, 1.1%) have not disclosed their TGNB status to even those closest people. A significant majority (n = 59, 62.1%) have shared their TGNB status with 81–100% of the people they are closest to. The largest group (n = 50, 52.6%) have disclosed their status to 61–80% of the individuals who are close to them, but seen less frequently. Additionally, 27 (28.4%) of the study participants noted that they are out to 41–60% of the people they socialize with. In terms of specific groups, 28 (29.4%) have disclosed their status to 41–60% of their peers, while 30 (31.6%) have done the same with their supervisors.
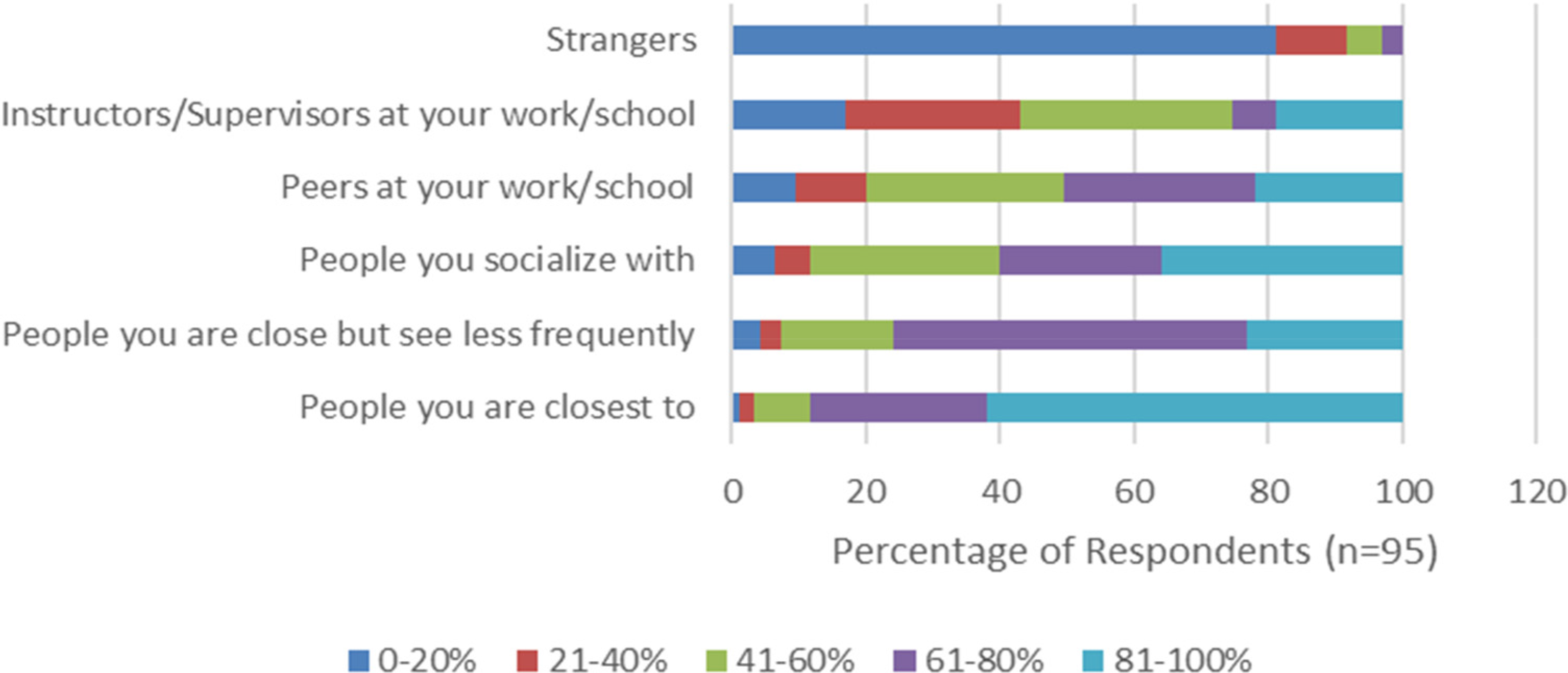
Outness as TGNB to various group of people.
Figure 3 represents how often the participants refrain from discussing topics related to or indicating their TGNB status with different groups of people. Out of the 93 participants who answered this question, surprisingly, a significant portion (n = 29, 31.2%) of respondents never avoids discussing TGNB topics or status with strangers. Only a small percentage (n = 20, 2.2%) avoids such discussions with people they are closest to. A majority (n = 42, 45.2%) of the participants sometimes avoid TGNB discussions when they are with individuals who are close to them but not seen as frequently. The highest percentage of participants (n = 53, 56.9%) avoid TGNB discussions approximately half of the time when socializing, and they do the same with their peers (n = 30, 32.3%) and supervisors (n = 23, 24.7%).
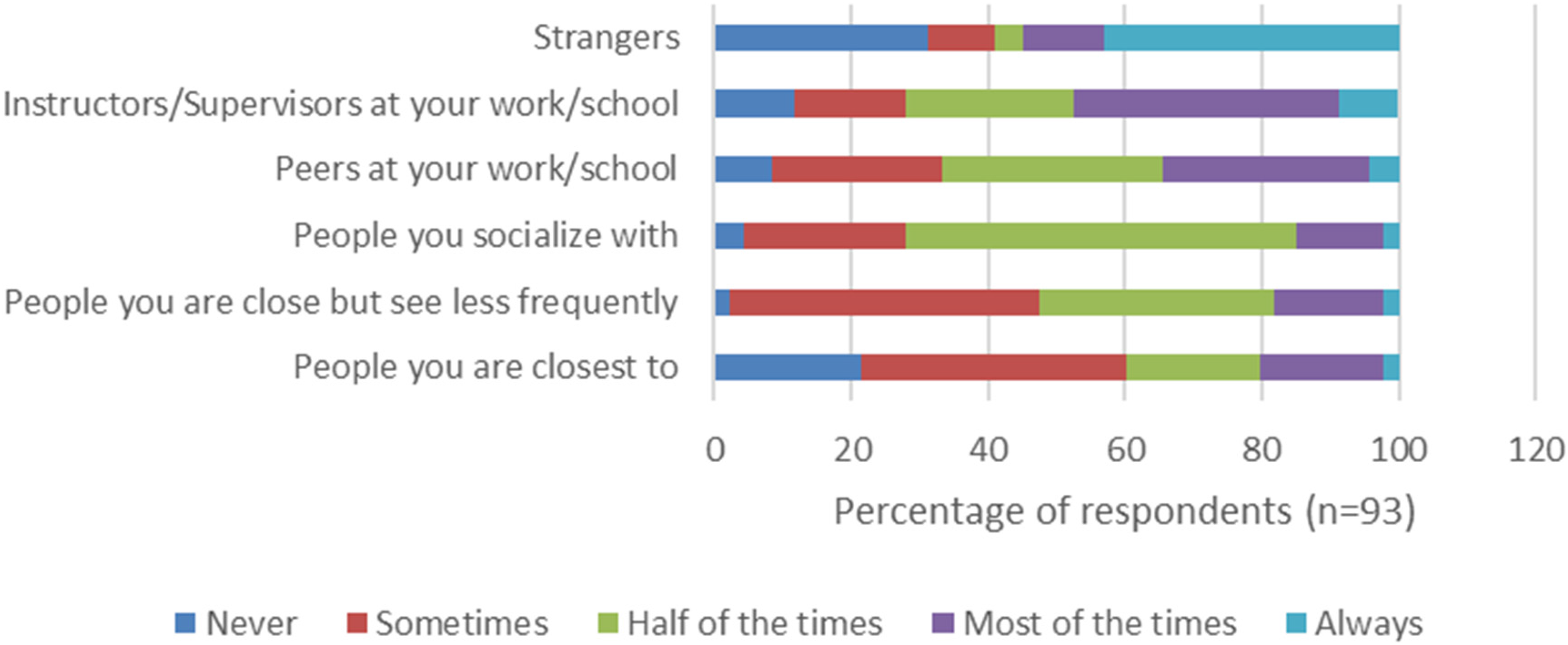
Avoiding TGNB talks with different set of people.
Discussion
The results of this study highlight a significant deficit in TGNB specific content within nursing education. Only 29.7% of participants reported receiving education on TGNB healthcare content during their nursing school studies. Despite the pressing need for inclusive curricula, our data suggests that nursing programs fail to adequately address TGNB healthcare issues. The limited coverage of LGBT health in nursing school curricula is a concern echoed in other studies (Bleasdale et al., 2024; Greene et al., 2018; Klotzbaugh et al., 2020; Manzer et al., 2018). For instance, Santiago et al. (2024) found that nursing students in Spain and Portugal had only a basic understanding of sexuality, sexual orientation, and gender diversity, indicating a lack of comprehensive knowledge. Respondents in our study emphasized that healthcare curricula could include the lived experiences of TGNB individuals, and discussions on their specific needs for inclusivity and healthcare, raise awareness about the discrimination they face, and provide training on gender-affirming care, hormonal therapy, and counseling.
Fear of rejection and the desire to avoid complications are major reasons TGNB individuals do not disclose their identity when applying to nursing school or in the workplace. Goldberg et al. (2019) noted that trans students frequently encounter cisgenderism and systemic ideology, which shapes their perception of campus climate differently from their LGB peers. Multiple studies have documented a discriminatory and exclusionary climate for the LGBTQ + community on college campuses (Broadhurst et al., 2018; Figueroa, 2024; Goldberg et al., 2019; Kortegast & van der Toorn, 2018). For example, trans students face institutional challenges such as inadequate restroom facilities, housing, health services, and documentation policies, resulting in a lower sense of belonging on campus (Goldberg et al., 2019).
Our findings indicate that the application processes for nursing and nurse practitioner (NP) programs may not support TGNB inclusivity, with 43.6% of respondents encountering barriers related to their gender identity or expression during the application process. These barriers included lack of gender-diverse options on the application beyond the traditional male or female, instances of heightened scrutiny, and sometimes requiring multiple follow-ups to ensure their applications were being adequately processed, adding to their burden and stress. This suggests a need for program accreditors to ensure that nursing programs have inclusive application procedures that support TGNB candidates. As more students openly identify as TGNB, it is increasingly imperative for nursing and NP programs to adapt their processes and environments to meet the needs of a more diverse student population. This demographic shift highlights the necessity of proactive measures to create truly inclusive and affirming spaces. Failing to address these issues risks alienating talented candidates and perpetuating inequities in the profession. According to Figueroa (2024), technical changes in university admission systems alone are insufficient, as entering a preferred name does not guarantee its use by everyone at the university.
Misgendering is a common issue identified in various studies (Figueroa, 2024; Markovic et al., 2021; Roach, 2024). Additionally, negative comments and harassment experienced by LGBTQ students have been reported in previous studies (Eliason et al., 2018; Figueroa, 2024). Eliason et al. (2018) found that LGBTQ nurses face harassment and discrimination from colleagues and educators, ranging from inappropriate comments to delays in promotions. Our study corroborates these findings, indicating that discrimination against TGNB nurses is widespread and deeply entrenched in the professional culture of nursing. The impact of discrimination or harassment on TGNB nurses or nursing students was described in our study as intimidating, heartbreaking, insulting, demotivating, and alienating. In contrast, having TGNB colleagues was associated with a sense of family and unity, indicating a positive and supportive environment.
The broader implications of our findings extend to patient care, particularly for TGNB individuals. The hostile and discriminatory environment within nursing affects not only TGNB nurses but also TGNB patients. Among the nurse participants, 84.4% observed discrimination towards TGNB patients during care. This highlights the necessity for trauma-informed care to address the unique challenges faced by TGNB patients, many of whom have experienced significant trauma related to their gender identity. Establishing best practices in trauma-informed care and primary healthcare screening for TGNB individuals is crucial to improving health outcomes and ensuring respectful and competent care. Pastor Bravo and Linander (2024) found barriers in all stages of healthcare access for TGNB youth in Spain and Sweden, with the most significant barriers arising in the appropriateness of services. Studies show that correctly referring to TGNB patients fosters an affirming environment, facilitating patient comfort and open communication essential for effective patient-provider relationships (Eisenberg et al., 2020; Reeves et al., 2024; Roach, 2024).
According to Bizzeth and Beagan (2023), the heteronormative culture in nursing is perpetuated through formal and informal curricula. LGBTQ individuals are often expected to assimilate and avoid presenting as overtly queer to maintain a professional image. TGNB nurses may be labeled as unprofessional due to their deviation from social norms (Beagan et al., 2023). Future healthcare professionals need to be educated to mitigate heteronormativity in healthcare and to provide equitable and high-quality care to gender-diverse populations. Higher education institutions must go beyond simply implementing technology that allows students to select their preferred names. These institutions have a responsibility to ensure that all university officials, including faculty, consistently use this information correctly. Universities should empower students to control how they are addressed, including the use of appropriate pronouns. While the preferred name system is a positive initial step in demonstrating institutional values, it must be complemented by comprehensive efforts.
Addressing the educational and professional barriers faced by TGNB individuals in nursing requires a comprehensive approach. Implementing standardized TGNB healthcare education, providing faculty training, and fostering an inclusive and supportive professional environment are essential steps towards achieving equity and improving the experiences and outcomes of TGNB nurses and patients alike.
Conclusion
This study highlights the experiences of TGNB nurses and nursing students in Canada. It was not uncommon for these participants to hide their gender identity for fears of discrimination or harassment. It is important to note that TGNB nursing students become TGNB nurses, so addressing these issues early is vital. Participants highlighted the lack of sufficient TGNB health topics in nursing curricula. Furthermore, the healthcare workforce continues to perpetuate an unsafe environment for TGNB nurses. This should no longer be accepted. Nursing schools and healthcare organizations need to do the necessary work to ensure that learning environments and workplaces are safe and inclusive for everyone.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by the Social Sciences and Humanities Research Council of Canada, (grant number 430-2022-00909).