
Abstract
Background
Early career nurses (ECNs) can be expected to assume shift charge nurse leadership roles quickly upon entering practice. Since the emergence of the COVID-19 pandemic, junior nurses may find their leadership capabilities tested further as the challenges of leadership are made increasingly complex in the context of an infectious disease outbreak.
Purpose
The purpose of this qualitative study was to explore early career registered nurses’ (RNs) experiences of engaging in shift charge nurse roles in hospital settings.
Methods
This study used an interpretive descriptive (ID) approach. Semi-structured, in-depth interviews were conducted with 14 RNs across Ontario, who had up to three years of experience and who had engaged in a shift charge nurse role in a hospital setting. Recruitment and data collection took place from January to May 2021 during the COVID-19 pandemic. Interviews were recorded, transcribed, and analyzed following the principles of content analysis.
Results
Content analysis of the 14 participant interviews revealed four main themes: nominated and necessitated into leadership, diverse and demanding responsibilities, factors that help and hinder, and leadership as an impactful experience.
Conclusions
Study findings provide insights into potential strategies to support ECNs in shift charge nurse roles, during the remaining course of the COVID-19 pandemic and beyond. Greater support for nurses who engage in these roles may be achieved by promoting collaborative unit and organizational cultures, prioritizing leadership training programs, and strengthening policies to provide greater clarity regarding charge nurse role responsibilities.
Keywords
Background and purpose
Leadership is integrated into national nursing entry-to-practice competencies (College of Nurses of Ontario [CNO], 2014), and as such, registered nurses (RNs) are expected to enact professional leadership roles upon licensure (Gore et al., 2015; Strickland & Welch, 2019). The roles of clinical staff nurse, shift charge nurse, and unit manager are each considered front line roles with varying degrees of leadership authority and responsibilities (Admi & Eilon-Moshe, 2016). As shift charge nurse roles are often rotated through staff RNs on a shift-by-shift basis (Bard, 2018), early career nurses (ECNs) employed as staff nurses may additionally engage in a leadership role with accountability for unit-level operations (Dyess & Sherman, 2010; Gore et al., 2015; Laut et al., 2018; Rush et al., 2014).
There is a lack of standardization and consistency with regards to the titles applied to the shift charge nurse role, with alternative terms including team leader and shift leader (Admi & Eilon-Moshe, 2016). Nurses engaged in the shift charge nurse role are accountable for care delivery and team functioning for a specified location and shift period (Admi & Eilon-Moshe, 2016). As such, shift charge nurses play a critical role in care delivery, human resource management, and clinical decision-making at the unit-level (Agnew & Flin, 2014; Eggenberger, 2012). Previous research indicates a positive impact of strong nursing leadership on patient and organizational outcomes, including safer unit environments and reduced adverse events such as falls, medication errors, pressure ulcers, nosocomial infections, and patient complaints (Agnew & Flin, 2014; Boamah, 2018). However, the literature indicates that nurses are often thrust into the shift charge nurse role with limited education or support (Delamater & Hall, 2018; Sherman et al., 2011; Wojciechowski et al., 2011), and that ECNs are particularly challenged to meet employers’ leadership expectations (Källestedt et al., 2020; Theisen & Sandau, 2013). Failure to provide ECNs with adequate support in shift charge nurse roles can result in excessive stress, errors leading to a breakdown in care, and the attrition of promising nursing leadership talent (Patrician et al., 2012).
The Coronavirus Disease of 2019 (COVID-19) pandemic has further driven unique challenges for frontline nurse leaders (Aquilia et al., 2020). Experienced RNs who acted as charge nurses during COVID-19 highlighted challenging responsibilities that were of heightened significance in the context of the pandemic, including transparent communication, maintaining patient safety, and assisting less experienced nurses (Holmgren et al., 2022). Compared to their more senior counterparts, ECNs in shift charge nurse roles may find their leadership capabilities tested further as the demands of leadership are compounded by the need to support staff and patients during periods of increased instability, and to advocate for critical frontline needs under resource-challenged conditions (Aquilia et al., 2020; Juan et al., 2021).
The purpose of this qualitative study, which took place during the COVID-19 pandemic, was to explore ECNs’ experiences of engaging in shift charge nurse roles in hospital settings. For the purpose of this study, shift charge nurse roles were defined as roles assigned responsibility for the care delivery and team functioning of a patient care area over a designated shift period.
Extant literature
Previous research indicates that ECNs feel confident in their teamwork and collaboration skills, while highlighting a need for greater preparedness for team leadership roles and responsibilities (Bayliss-Pratt et al., 2013; Mbewe & Jones, 2015). Much of the available quantitative evidence explores the impacts of programs aimed to foster ECNs’ informal leadership behaviors and skills (Al-Dossary et al., 2016; Greer-Day et al., 2015; Jeffries & Acuna, 2016; Laut et al., 2018). Despite wide variation in content, length, and method of delivery, results of previous studies indicate that such interventions can play a valuable role in helping ECNs incorporate leadership skills into their daily practice (Al-Dossary et al., 2016; Greer-Day et al., 2015; Jeffries & Acuna, 2016; Laut et al., 2018). ECNs described improved ability to think from a systems perspective, enhanced confidence in interprofessional communication, and improved perception of their ability to drive positive change (Dyess & Sherman, 2010; Jeffries & Acuna, 2016). Providing support for ECNs’ leadership competencies can contribute to improved job satisfaction, greater engagement of new nurses in quality improvement projects, and ultimately improved patient care services (Al-Dossary et al., 2016; Dyess & Sherman, 2011; Jeffries & Acuna, 2016).
Extant qualitative literature exploring ECNs’ leadership experiences largely focus on the leadership role of the RN in relation to teams comprising of healthcare aides or other non-registered staff in international settings. Team leadership was described as a challenge by ECNs in Sweden and Brazil, particularly in acute care settings where participants had not yet developed a solid foundation of clinical skills to effectively manage high-complexity care (Ekström & Idvall, 2015; Da Silva et al., 2010; Sundberg et al., 2021; Vilela & De Souza, 2010). Findings of these studies collectively highlight a need for greater support for ECNs as they enact team leadership responsibilities in both acute and long-term care settings, which may be achieved through protected orientation time and clearer delineation of team role expectations (Da Silva et al., 2010; Ekström & Idvall, 2015; Whitmore et al., 2019).
Supporting ECNs as charge nurse leaders requires greater awareness and understanding within healthcare organizations regarding their experiences of leadership (Sundberg et al., 2021). However, there is a dearth of research exploring ECNs’ engagement in shift charge nurse roles, particularly within Canadian contexts and during infectious disease outbreaks or other crises. As leadership demands vary across nations and healthcare sectors, there is a need for Canadian-based research exploring ECNs’ leadership of teams comprised of other nurses and interprofessional team members. The present study sought to address these gaps in the literature.
Methods and procedures
This study used an interpretive descriptive (ID) approach, an “inductive analytic approach designed to create ways of understanding clinical phenomena that yield applications implications” (Thorne et al., 2004, p. 1). ID acknowledges that researchers’ applied disciplinary orientation fundamentally influences and informs the research process, driving the co-construction of understanding and meaning between participants and researchers (Thorne, 2016). By focusing on ECNs’ subjective and contextual experiences, this study aimed to develop practice implications that were grounded in the complex realities of the clinical environment.
Sampling and recruitment
The study setting included hospital settings across Ontario. Criteria for inclusion were: RNs within the first three years of practice; working in a hospital; with experience in a shift charge nurse role since March 2020; fluent in speaking and reading English; and consent to audio-recording for an interview. Recruitment took place through the CNO database of members who consented to the release of their contact information for research. Study authors obtained a list of members working in hospital settings who possessed up to three years of RN experience. As the CNO does not collect information regarding the remaining inclusion criteria, a random sample of 300 potential participants were mailed a study letter of information inviting recipients who had experience in a charge nurse role to contact the study authors. Purposive sampling was used to recruit 14 ECNs willing to speak to their experiences in a shift charge nurse role for this study. One respondent to the mail-out did not meet the inclusion criteria and was excluded from the study.
While ID studies typically include five to 30 participants, there is no prescribed sample size for an ID approach; rather, sample size should be justified with rationale consistent with the research aim (Thorne, 2016). An adequate sample size for this study was considered to have been reached when a variety of perspectives had been collected to inform a rich understanding of ECNs’ experiences, such that the findings could help inform strategies to support ECNs as charge nurse leaders.
Data collection and analysis
Informed written consent was obtained from all participants included in the study. Data was collected through in-depth, semi-structured, 60- to 90-min interviews conducted by the primary author through videoconferencing or telephone. Interviews took place between January and May 2021. Participants were offered compensation in the form of an electronic Amazon gift card ($20.00 CAD). Interviews were audio-recorded and transcribed verbatim with the redaction of identifying information. De-identified transcripts were re-read to confirm accuracy while listening to their corresponding digital audio-recording, after which the recording was then deleted.
Content analysis as described by Erlingsson and Brysiewicz (2017) was used to analyze interview data. This approach to analysis is described as a “systematic classification process of coding and identifying themes or patterns” (Hsieh & Shannon, 2005, p. 1,278), and involves a recursive process of moving between increasing levels of abstraction and returning to the raw transcript data to reflect on initial interpretations and analyses (Erlingsson & Brysiewicz, 2017). This approach allowed themes to flow inductively from the data, facilitating the development of disciplinary insights that were grounded in the clinical realities of the research participants (Hsieh & Shannon, 2005). NVivo 12 Qualitative Data Analysis Software (QSR International Pty Ltd., 2020) was used to aid in the sorting and organization of data.
Reflexive field notes were used to note the researchers’ disciplinary orientations, knowledge, and pre-understandings as practicing nurses within clinical and academic settings. The aim of this exercise was to maintain an awareness of their potential influence on the co-construction of findings, and to avoid settling into familiar and potentially anticipated codes and categories (Erlingsson & Brysiewicz, 2017). The study authors met regularly during the data collection and analysis processes to discuss, challenge, and refine emerging findings. Follow-up sessions with participants were also performed for member-checking purposes to enhance data analysis (Farren, 2015; Thorne et al., 1997). An audit trail and reflexive journal were used to document analytic decisions and record the study authors’ rationale as they moved between the data, identification of recurrent patterns and emerging codes, and development of themes (Nowell et al., 2017).
Results
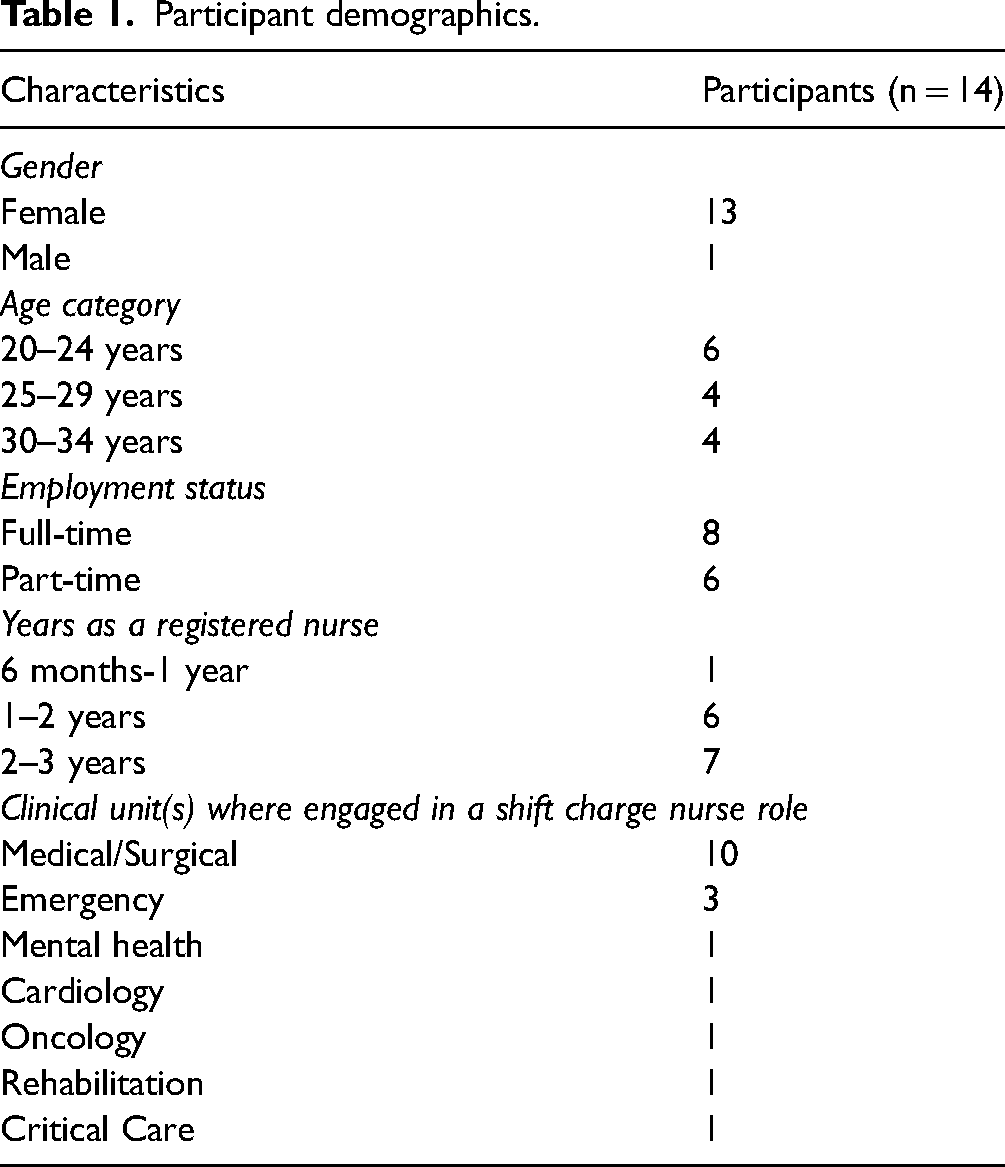
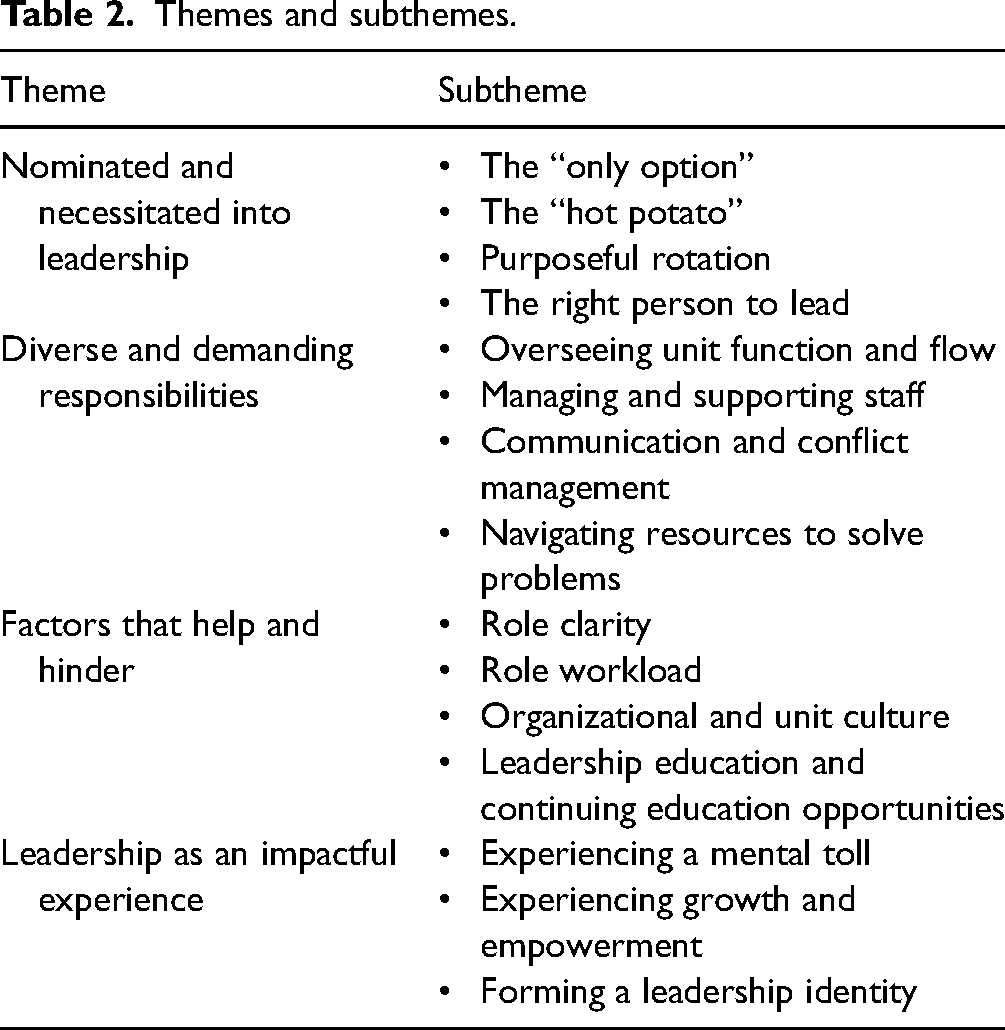
The final sample consisted of 14 participants (Table 1). All participants were clinical staff nurses who had engaged in a shift charge nurse role by rotating into the role or providing sick coverage for permanent charge nurses. Four themes were identified to elucidate ECNs’ experiences of engaging in shift charge nurse roles in hospital settings: (1) Nominated and necessitated into leadership, (2) Diverse and demanding responsibilities, (3) Factors that help and hinder, and (4) Leadership as an impactful experience. These themes and their subthemes are displayed in Table 2.
Participant demographics.
Themes and subthemes.
Theme 1: Nominated and necessitated into leadership
The circumstances surrounding ECN participants’ leadership experiences were emphasized as a catalyst for their engagement into roles they might not otherwise have taken on. Participants reported four types of situations in which they had been nominated or necessitated to take on a shift charge nurse role: the “only option”, the “hot-potato”, purposeful rotation, and the right person to lead.
The “only option”
Participants recounted situations in which they were defaulted into the shift charge nurse role by virtue of being the most senior or only RN in their clinical area. A participant noted in such situations, “Neither one of us knows what's right, we’re just kind of bumbling along” (P14). Many participants expressed a belief that they would not have been assigned to the role under ideal conditions; yet staffing shortages, high turnover rates and attrition of experienced RNs exacerbated by the pandemic, often made this necessary. For example, one participant recalled how their engagement in a shift charge nurse role was instigated by a shortage of senior staff: There were a lot of holes and not enough coverage during certain shifts. A lot of the senior staff had to be redeployed … A lot of the more senior staff volunteered to go to the ICU, so we were being spread thin in a lot of different directions. (P7)
The “hot-potato”
Another recurring pattern in participants’ accounts was the offloading of the shift charge nurse role to participants by senior RNs. One participant quipped, “I call it the hot potato. Nobody wants to do it, right? They don’t mind seeing us in charge, because that means they don’t have to do it” (P14). Participants noted that their more senior peers would, at times, resist frontline leadership roles, despite being more qualified than their junior counterparts. One participant shared: A coworker of mine has tons of experience. She's a fantastic nurse, she's my go-to for anything. But she says that whenever she's in charge, everything goes wrong, so she would prefer not to do it. She's always like, “You do it, and I’ll help you.” … Some people just prefer to not have that responsibility. (P4)
Purposeful rotation
One-third of participants described leadership as a shared responsibility in their clinical areas, such that all RN staff were rotated into the charge nurse role on a shift-by-shift basis. Purposeful rotation was pursued to increase leadership capacity amongst staff and to reduce the burden of leadership on senior nurses. These cases were characterized by an intent to ease the ECN into the role, with the planned presence of senior staff to support them. One participant explained: The idea was, ‘We’re making you charge on this night shift. It looks like it's going to be a quiet night. Eventually you’re going to have to be charge on a less quiet night, so we’ll get you used to this, and you can ask any questions you want to Co-worker Z who has 20-plus years of experience. (P6) Most people expressed that they would love to take on that opportunity, but they didn’t want to always be in that position. So, we tried different people taking on the responsibility here and there, and it just seems to be working. It gives people opportunity to have a break from charge, because sometimes it's a lot. (P4)
The right person to lead
A subset of participants described their engagement into leadership as stemming from traits or skills that prompted others to view them as suitable candidates for the shift charge nurse role. For example, a participant described their technological competency as a key reason they were nominated: I think it's mainly because of the way I can deal with the system that we have now … I was a super user so I guess they pushed me to be in charge because I can get things done faster. (P1)
Theme 2: Diverse and demanding responsibilities
Participants largely eschewed their shift charge nurse leadership role as one of authority, instead framing the role as one of diverse and demanding responsibilities to ensure effective unit and team functioning. Four subthemes were identified: overseeing unit function and flow, managing and supporting staff, communication and conflict management, and navigating resources to solve problems.
Overseeing unit function and flow
Participants described being responsible for oversight of their clinical areas, ranging from the minutiae of ensuring equipment was maintained, to procuring essential supplies required for care, addressing safety issues, and making strategic decisions to facilitate patient flow. Participants often characterized their accountability as all-encompassing, with one participant commenting: I feel like automatically when you come on and you’re told that you’re charge, your stress level just jumps. You’re like, okay, I have to pay a lot more attention to everything. Whereas, when you’re not in charge, you’re very much more focused on the patients you’ve been assigned. (P11) You’re responsible for placing COVID-positive people in specific rooms, discharging other patients, and accepting admissions from any other part of the hospital that needs room for a critical patient. And I feel like the hardest part with that is, you’re constantly looking at what patient has to stay where. (P2)
Managing and supporting staff
Strategic and compassionate management of staff was highlighted by participants as a significant shift charge nurse responsibility. Participants described closely monitoring staffing levels and attempting to contend with frequent shortages. The creation of nurse-patient assignments was described as a laborious process, with one participant noting the need to “strategically make [the assignments] to help people succeed in their role” (P5). Participants described attempting to create fair workloads by balancing a number of factors relating to the nurse, the acuity and social complexity of patients, and the geography of the unit. For example, participants avoided placing too many isolated patients in one nurse's roster, ensured critically ill patients were paired with nurses of appropriate skill, and refrained from assigning pregnant staff to patients with COVID-19. Redeployment of staff to other areas in need was also described as a complex decision-making process in which they balanced multiple factors: scope of practice; degree of experience and training; individual preference and comfort level; seniority; and time since last redeployment.
Throughout these decision-making processes and in their daily functions as shift charge nurses, all participants emphasized their role in being present to support their team members. One participant shared their approach: “I like to be a charge nurse that gets their hands dirty. Even though I’m a new charge nurse, I’ll be quick to jump in and help when help is needed. I think that's being a strong leader” (P5). Many participants shared the sentiment that the leaders they aspired to emulate were those who had been highly visible and present to aid them when needed. As a result, several reported foregoing their own work and breaks to assist team members with patient care.
Communication and conflict management
Participants emphasized the importance of maintaining open channels of communication to facilitate patient care, foster positive relationships, and mitigate and manage conflict. Participants perceived the shift charge nurse role as a centralized hub for communication between frontline staff, patients/families, interdisciplinary team members, leadership, and other clinical areas within the hospital. Participants were also often expected to field complaints from frustrated staff, patients, and families. One participant explained, “Management is not always there to hear their problems, and that's why they always go to the charge nurse with the issue” (P1). Nurse-patient assignments and restrictive visitor policies were points of frustration for staff and patients/families, respectively.
To prevent and address conflict, participants favored empathetic, transparent, and democratic approaches to communication. One participant described their gentle communication style when attempting to reach a mutually agreeable solution: “As the charge nurse, I did a lot of that – of just trying to talk to people, reassuring them and calming them and trying to find creative ways for them to be able to see their family members” (P12). Similarly, another participant shared their relational approach to difficult conversations with nurses who breached heightened infection control standards: I try to be more light-hearted, and not in a punitive way, like you’re trying to scold the person. Because I also understand where everyone's coming from, because I am a staff nurse, too … It may be a bit easier if I can tap into that ‘friendship’ aspect of it, but then also deliver the message I need to deliver. (P7)
Navigating resources to solve problems
Participants acknowledged the limitations of their knowledge and experiences as junior nurses, while emphasizing their resourcefulness in knowing where and how to access the information they needed to respond to the diverse issues that emerged in their clinical areas. Participants described a need to establish a strong familiarity with a multitude of specialized staff and interdisciplinary resources to aid them in addressing a broad range of unique issues—such as troubleshooting a medical device, assisting with a deteriorating patient, and facilitating a challenging discharge. One participant shared the importance of both knowing who to communicate with and how to communicate with them: I understood what phone calls I had to make, who can do the specific things for me that I need to get done before this patient can leave …. If I knew who I needed to call, I felt like getting the answer was a lot easier than asking who to call and then not knowing how to articulate what I need properly. (P2)
Theme 3: Factors that help and hinder
Factors that positively or negatively influenced ECNs’ experiences as shift charge nurses included four subthemes: role clarity, role workload, organizational and unit culture, and leadership education and continuing education opportunities.
Role clarity
Most participants identified that their organizations did not provide professional development activities specific for learning the shift charge nurse role. As a result, participants were often assigned a shift charge nurse role without a full understanding of its responsibilities. A participant recalled: “I started my shift and then I realized I’m the charge nurse. What do I do as a charge nurse? I don’t know! “I guess you guys don’t have a charge nurse tonight!”—that's what I told them” (P8). Participants who had been thrust into shift charge nurse roles without preparation expressed surprise, with one participant commenting, “A lot of it is learning on the job, which is just mind-boggling. How are you in charge of a floor when you don’t even know what the specs are?” (P11). Participants shared that much of their understanding was formed by consulting with experienced nurses or by modeling after other shift charge nurses.
For a subset of participants whose workplaces provided dedicated professional development opportunities to learn the shift charge nurse role, this most often constituted shadowing an experienced charge nurse. The length of this orientation ranged from one shift to two weeks. Participants viewed shadowing as a helpful exercise, yet opportunities were at times precluded by staffing shortages which had worsened in the pandemic environment. For many, however, professional development opportunities specific to the charge nurse role were not routine organizational practice. One participant shared, “I was told, “In your collective agreement, it doesn’t state anywhere that training is to be provided.” As an RN, [the shift charge nurse role is] a role that you’re expected to take sometimes – that's part of your role” (P14).
Role workload
Participants described a “juggling act” between working alongside their team members at the bedside and performing important administrative tasks behind-the-scenes. Accordingly, they highlighted the need for realistic workloads that allowed them to fulfill their many responsibilities. One participant shared, “I feel like I’m constantly in meetings and constantly on the phone, constantly defusing situations, constantly in crisis. So in the end, patients come secondary, when they should always be the center of care, right?” (P5). Notably, most participants additionally managed a patient assignment while assigned as the shift charge nurse. In some cases, this was a routine expectation; other participants were required to take on patient assignments due to a shortage of staff nurses. One participant articulated the compounded challenge of simultaneously learning to manage patient care and charge nurse leadership: When you’re a new nurse, you’re just struggling to keep up with your patients. So then when you have people coming and asking you questions, or coming to you to get help with their patients as well, suddenly you’re way behind. (P11)
Organizational and unit culture
Participants highlighted the significance of supportive workplace cultures, expressing a need for understanding from others as they learned from their mistakes. For example, one participant shared the constructive approach taken by their workplace: “There were things that I maybe didn’t make the best decision, but they were like, “Okay, so next time …” It's never being punished or told off, but just encouraged in a direction to go next time” (P4). Many participants expressed gratitude towards their teams, who viewed effective unit functioning as a shared goal and who aided them in their leadership responsibilities. For example, one participant shared: “They’re never like, “Oh, you’re charge, it's your problem to deal with.” Everyone's happy to jump in” (P4). Participants also expressed a desire for positive reinforcement: “It's definitely nice when peers or leadership recognizes that effort and reassures that it's not easy, but it is a good job that you’re doing … because that little bit would go a long way” (P7). Participants whose efforts had been recognized reported feeling pride, relief, and affirmation in their role as nurse leaders. Interdisciplinary staff and experienced nurses from other clinical areas were also identified as key supportive resources. One participant described a culture of reciprocity between units, stating, “I was told to give other units a call, so that was always ingrained in me … They’ve always been really receptive, always willing to come over to give a hand or to have a second look at a patient” (P9).
However, some participants acknowledged that workplace cultures were not consistently understanding or collaborative, leading to feelings of increased pressure in the shift charge nurse role. One participant shared: The way that I perceive [the charge nurse role] and take it on is, it's all on me. And some days you feel that more than others, depending on the staff you work with … When you’re working with newer staff or different staff that you don’t fully agree with the way they do things, then I really feel it so much more. (P12)
Leadership education and continuing education opportunities
While some participants recalled attending leadership courses as students, most felt that they had not obtained a strong grasp of the realities of charge nurse leadership. One participant stated: “It was very broad-spectrum, like if you’re introducing a brand-new policy to a unit … But it's not common for you to implement a brand-new policy as often as dealing with colleague disputes” (P2). Recurrent suggestions across interviews included a need for realistic scenario-based content, as well as opportunities to engage with charge nurse leaders as speakers or preceptors to help bridge the gap between education and practice. Many participants also described the need to correct an assumption that shift charge nurse roles were reserved for senior RNs, with one participant recalling: Most things I read about or learned about either didn’t discuss the timeframe that would take place before you could possibly be in a charge role – either stated or kind of implied it would be once you have a ton of experience. (P11)
Theme 4: Leadership as an impactful experience
Participants reflected on the professional and personal impacts of their charge nurse leadership experiences. These impacts comprised three subthemes: experiencing a mental toll, experiencing growth and empowerment, and forming a leadership identity.
Experiencing a mental toll
Participants described experiencing heightened stress and feelings of inadequacy and guilt due to their engagement into the shift charge nurse role. For example, one participant shared: “It feels like you’re not good enough. Like, why am I in this position? Definitely, someone is out there that can do it better than me … it did take a toll on [my] mental health” (P2). As shift charge nurses, participants often felt pressured to appease everyone on their teams, while acknowledging that doing so was rarely possible. Furthermore, as the most proximal leader to the point of care, participants perceived that they were targets for frustration stemming from issues that were intractable and systemic—such as nursing shortages and staff burnout. One participant recalled, “The [COVID-19] numbers were just through the roof … you could see that people were burning out. And it was hard, being in that position as a leader, and you don’t really have a solution to that” (P7). In some cases, participants questioned their commitment to the role. One participant stated: It's a lot of responsibility, and it's not glamorous at all. You have to fight with people and no one's happy ever, and you have to deal with all this BS … what am I struggling with this for? What am I putting all this effort in for? (P14)
Experiencing growth and empowerment
The challenging nature of charge nurse leadership was also perceived as a catalyst for growth. One participant reflected on their overall experiences as a shift charge nurse: “Despite it being stressful, I felt like I grew and I learned a lot” (P7). Participants perceived that their experiences accelerated the development of their professional competencies, including communication, critical thinking, decision-making, problem-solving, conflict management, and systems-level thinking. Participants also noted increased incentive to pursue professional development opportunities. For example, a participant shared: I was more willing to take on different assignments, different patients, and to go to more education events. I was interested in increasing my knowledge and learning about things I wasn’t comfortable with. It made me feel like, if I’m going to be in [the shift charge nurse] position, I should know what I’m doing. (P2)
Forming a leadership identity
Participants expressed that they had a greater sense of themselves as leaders due to their experiences in a shift charge nurse role. For some, these experiences prompted a re-evaluation of their self-doubt. A participant who had provided short-notice coverage for a sick charge nurse, shared: I probably wouldn’t have become charge if that moment hadn’t arisen … I feel like I would always just be in this circular mind, thinking I don’t have that much experience, and I would always feel that way. But … when I kept doing it, I was like, okay, you know what? It's not that bad. (P1)
Discussion
The findings of this ID study elucidate ECNs’ experiences in shift charge nurse roles in the context of the COVID-19 pandemic, and shed light on potential strategies to engage and support junior nurses as frontline leaders.
In many cases, participants expressed that their engagement into a leadership role felt premature, and that they had been nominated by others or necessitated to take on the shift charge nurse role. Previous research has indicated that ECNs lack competence and confidence in leadership, including in areas such as delegation, prioritization, and conflict resolution (Bagnardi, 2014; Theisen & Sandau, 2013). While previous research suggests that nurses are selected for charge nurse roles because of their experience and expertise (Homer & Ryan, 2013), participants in this study shared situations in which they were the most experienced or only RN available on their unit. These situations may become increasingly common as COVID-19 has precipitated staff redeployments and an exodus of experienced RNs from the profession (Lopez et al., 2022). Participants also described being unexpectedly assigned as shift charge nurse when the role was declined by more experienced RNs. These findings align with previous research that highlights the difficulties in recruiting nurses into hospital leadership roles (Dillard-Henderson, 2018). In contrast, participants who worked in areas that rotated the shift charge nurse role amongst staff RNs were comparatively eased into the role by a work culture that promoted frontline leadership as a responsibility to be developed and shared by all RNs. Deliberate efforts to build leadership capacity amongst ECNs can mitigate scenarios in which they feel thrust into a leadership role, and ultimately contribute to a pool of future leaders for much-needed leadership succession planning efforts (Bard, 2018; Patrician et al., 2012; RNAO, 2013).
The diverse and demanding responsibilities subthemes identified in this study echo challenges identified by charge nurses in previous research (Cathro, 2016; Eggenberger, 2012). However, this study is unique in its exclusive recruitment of ECNs, as well as its positioning within the COVID-19 pandemic. In contrast to previous works, the participants in this study did not identify supervision of staff as a key responsibility. Rather, as shift charge nurses, participants expressed a strong sense of obligation to support their team by being highly available at the point of care. Study findings also revealed a multitude of ways through which ECNs as shift charge nurses contributed to the experiences of patients, families, and staff. Participants made strategic decisions to optimize patient flow; compassionately managed staffing to optimize patient care in the context of human resource shortages; and maintained transparent communication channels to positively engage patients and staff in the context of heightened infection control measures and visitor restrictions. While studies predating COVID-19 have identified overall unit oversight, managing patient flow, and acting as an advocate for patients and staff as key charge nurse responsibilities (Cathro, 2016; Dillard-Henderson, 2018; Eggenberger, 2012), participants in this study highlighted these as continued priorities which were made more challenging in the context of the pandemic.
Despite acknowledgement of the challenges of the charge nurse role in the literature, most participants highlighted that they were not provided professional development opportunities to prepare them for the role, either in accordance with organizational practices or due to significant resource constraints created by COVID-19. This concurs with findings from extant literature, which indicates that nurses are often assigned shift charge nurse roles without training (Patrician et al., 2012; Sherman et al., 2011; Wojciechowski et al., 2011). Inadequate role preparation undermines nurses’ effectiveness as leaders and raises concerns for staff and patient safety (McCallin & Frankson, 2010), particularly in the context of COVID-19. With a scarcity of resources and increased demands upon nursing leadership, shift charge nurses may be contending with greater responsibilities in ensuring effective unit functioning and the reliable delivery of care than ever before (Shin et al., 2022). As such, an organizational focus on nurse leader development is made even more paramount in times of crisis (Fowler & Robbins, 2022).
In the absence of dedicated education or training, participants highlighted the significance of appropriate workplace resources and supportive intra- and inter-departmental cultures to facilitate their on-the-job learning. However, participants noted barriers which have been previously highlighted in pre-pandemic research, including heavy workloads, inadequate staffing, and unsupportive unit cultures (Regan et al., 2017). Leaders can help position ECNs for success in shift charge nurse roles by facilitating shadowing and mentorship opportunities with supportive frontline leaders, and by fostering positive unit cultures in which ECNs are encouraged to seek feedback and support (Ekström & Idvall, 2015; Regan et al., 2017; Spiva et al., 2020). Study findings also highlighted further supportive conditions, including adequate staffing to support achievable workloads; an appropriate balance of skill mix and experience levels across shift schedules; and a collaborative interprofessional and interdepartmental work environment in which ECNs may seek support from a rich variety of resources.
Many participants felt that their leadership experiences had a substantial impact on their perceived leadership capabilities, career aspirations, and the development of a professional leadership identity. These findings align with previous research describing charge nurse roles as a “starting point in a leadership career move” (Wojciechowski et al., 2011, p. E15). However, negative experiences can contribute to turnover and low job satisfaction, and can deter nurses from a leadership career path (Schwarzkopf et al., 2012). Accordingly, some participants expressed ambivalence about pursuing further leadership roles. Proactive support strategies are needed to mitigate adverse impacts of challenging leadership experiences, particularly in the context of the COVID-19 pandemic (Lopez et al., 2022). Evidence from the literature supports that professional leadership development opportunities can improve nurses’ leadership competencies, job performance, and job satisfaction (Delamater & Hall, 2018; Homer & Ryan, 2013). With dedicated education and conscious leadership support, the shift charge nurse role can provide ECNs with a rich opportunity for professional growth and valuable exposure to other leadership opportunities. ECNs who are well-supported as shift charge nurses can be applied in a greater capacity to support organizational outcomes, including during periods of crisis, and may be more motivated to pursue advanced leadership roles in the future (Eggenberger, 2012; Greer-Day et al., 2015; Jeffries & Acuna, 2016).
Limitations
This study contributes to several under-studied areas of research, including charge nurse leadership by ECNs during infectious disease outbreaks. However, as participants were recruited exclusively from Ontario hospitals using a sample who self-reported meeting the inclusion criteria, the study findings may have limited applicability to other regions and clinical contexts. The heterogeneity in participants’ clinical settings may influence the relation of study findings to specific clinical workspaces. Furthermore, although the demographics of the study sample were comparable to provincial figures for gender and age (Canadian Institute for Health Information, 2019), the transferability of the study findings should be considered in the context of the sample's demographic profile which was mostly female and under 35 years of age. Qualitative studies that further focus on specific demographic characteristics or clinical areas may provide greater insights unique to those groups and settings.
Conclusion
This ID study has elucidated ECNs’ experiences in shift charge nurse roles in hospital settings in the context of the COVID-19 pandemic. Study findings reveal opportunities to enhance supports for ECNs who engage in shift charge nurse leadership roles during periods of increased practice setting pressures. Facilitating early mentorship opportunities with nurses in shift charge nurse roles can help ECNs build a robust understanding of frontline leadership in action, promote the conceptualization of leadership development as a meaningful goal, and enhance readiness to enact charge nurse leadership role responsibilities. Greater support for ECNs who engage in shift charge nurse roles may be achieved through the promotion of collaborative and supportive unit cultures, the prioritization of dedicated professional leadership development opportunities, and the strengthening of organizational policies to provide greater clarity regarding shift charge nurse role responsibilities.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Research ethics
Ethics approval for this study was obtained from a university ethics review board in Ontario.