
Abstract
Background
Individuals with inflammatory bowel disease (IBD) require life-long interactions with the healthcare system. Virtual care (VC) technologies are becoming increasingly utilized for accessing healthcare services. Research related to the use of VC technology for the management of IBD in Canada is limited. This study aimed to examine the VC experiences from the perspectives of individuals with IBD and gastroenterology care providers (GCPs).
Methods
A patient-oriented, qualitative descriptive approach was used. Semi-structured interviews were completed with individuals with IBD and GCPs. Data were analyzed using an inductive content analysis approach.
Results
A total of 25 individuals with IBD and five GCPs were interviewed. Three categories were identified: benefits of virtual IBD care delivery, challenges of virtual IBD care delivery, and optimizing IBD care delivery. Individuals with IBD and GCPs were satisfied with the use of VC technology for appointments. Participants believed VC was convenient and allowed enhanced access to care. However, VC was not considered ideal in some instances, such as during disease flares or first appointments. Thus, a blended use of virtual and in-person appointments was suggested for individualized care.
Conclusions
The virtual method of connecting patients and providers is deemed useful for routine appointments and for persons living in rural areas. VC is becoming more common in the IBD care environment. Nurses are in a key position to facilitate and enhance virtual IBD care delivery for the benefit of both individuals living with IBD and providers.
Background and purpose
Canada has one of the highest rates of inflammatory bowel disease (IBD), with over 320,000 individuals living with this lifelong chronic condition in 2023 (Coward et al., 2023). In 2016, 6468 individuals had IBD in Saskatchewan (SK); this is in the context of a prevalence that has tripled in the past 20 years (Osei et al., 2020). IBD is characterized by an immune-mediated response that results in inflammation and ulceration within the digestive system. Management of IBD requires repeated interactions with the healthcare system, including physician follow-up, diagnostic procedures, long-term medications, and in some cases hospitalizations and surgeries, resulting in direct healthcare costs that exceeded $7,100/patient/year in SK in 2016 (Osei et al., 2020). Exacerbation of symptoms is unpredictable and can occur between scheduled in-person appointments with gastroenterology care providers (GCPs). Individuals with IBD may be too unwell to sit in a clinic waiting room or to travel to an in-person appointment and may require frequent washroom access. Furthermore, persons with IBD often take immunosuppressive medications, may have other disease comorbidities, and may be over the age of 65, placing them at greater risk for contracting and having more negative outcomes due to community-acquired illnesses. Virtual care (VC) is one solution to provide access to a GCP from the comfort and safety of one's home. VC is defined as “any interaction between patients and/or members of their circle of care, occurring remotely, using any forms of communication or information technologies, with the aim of facilitating or maximizing the quality and effectiveness of patient care” (Jamieson et al., 2015, p. 4). Examples of VC options include electronic messaging, Telehealth, video consultations, remote telemonitoring, and telephone care appointments. VC technologies are becoming increasingly utilized, particularly since the onset of the COVID-19 pandemic. VC is a strategy to allow GCPs to intervene early, promote good patient outcomes, and prevent direct costs to the healthcare system (Avery, 2020).
Worldwide, a variety of VC technologies are used for IBD-related care, including electronic communication via computer or through mobile applications; web-based remote patient monitoring portals through which persons with IBD can enter personal data, such as weight or symptoms, and GCPs can then review the data entered; telephone advice lines; and Telehealth or other video technology for virtual consultations (Bhattacharya et al., 2020; Chang et al., 2020; Correal et al., 2019; George & Cross, 2020). Underutilization of VC technologies for IBD care is common and similar barriers are noted globally (Lees et al., 2020). Since the COVID-19 pandemic was declared, telephone appointments for virtual IBD care have seen the biggest increase in utilization worldwide (Lees et al., 2020) compared to other VC technologies, but experiences and satisfaction with using this technology have had limited evaluation in Canada.
Individuals with IBD whose health is managed via VC report an improved quality of life, improved disease outcomes, increased disease-related knowledge and understanding of the plan of care, and decreased in-person clinic visits (Davis et al., 2021; Pang et al., 2022). Internationally, high satisfaction accompanies the use of VC initiatives for IBD-related care (Storan et al., 2023; Taxonera et al., 2021). VC technologies can bridge barriers to specialist health care access in communities without such providers (e.g., rural areas) (Rohatinsky et al., 2021). Notably, individuals with IBD residing in rural areas have limited access to GCPs and report more hospitalizations and emergency department visits than those in urban areas (Benchimol et al., 2018; Pena-Sanchez et al., 2023). When individuals with IBD are monitored by a GCP and have access to appropriate, efficient care, the potential health system cost savings are significant and include reduced disease-related complications, hospital admissions, and surgeries.
Using VC for IBD-related care is not without its challenges, and barriers depend on the type of VC technology used. Decreased satisfaction with VC occurs due to technological difficulties, variable audio or video connections, lack of in-person contact, and lack of confidence or training with the technology (Gilbert et al., 2020; LeBlanc et al., 2020). Barriers to using VC for IBD-related concerns includes lack of provision for physician remuneration, technology implementation/infrastructure challenges, lack of provider and patient acceptance, inability to obtain informed consent, and inability to ensure security and privacy (George et al., 2020). Not all communities or individuals have access to Telehealth technologies or high-speed internet, limiting access to care via some VC means. However, VC technologies, such as telephone or non-Telehealth video calls, can bridge gaps in access.
Most research related to the use of VC technology for IBD care management discusses the use of Telehealth or novel VC interventions (e.g., remote monitoring, mobile applications), and is primarily occurring in Europe and the United States (Chang et al., 2020; George & Cross, 2020). Minimal literature has examined the use of IBD-specific VC within Canada (Jones et al., 2021) and none in the SK context. Telehealth has been used in SK to manage some conditions (Jong et al., 2019), but its regular use for IBD care is limited. Globally, the literature related to the integration and assessment of IBD telephone care is limited to nurse-led telephone advice lines (Harris et al., 2020), a practice not formally established in Canada (Chauhan et al., 2022). To our knowledge, there is no literature on satisfaction with VC or perceived quality of IBD-related care by persons with IBD or GCPs in the SK context, and there is limited literature concerning VC use in Canada for IBD care. By assessing and understanding the experiences of VC from the perspectives of persons with IBD and providers, results can inform decision makers to make system improvements related to VC, facilitate greater use and integration of these technologies, and enhance patient and provider satisfaction with VC. Using VC can facilitate early interventions to prevent complications and decrease costs to the healthcare system and to persons accessing health services.
We aimed to examine the VC experiences of individuals with IBD and GCPs in SK. Study findings can facilitate an understanding of the VC experiences so strategies can be developed to enhance the health and well-being of persons with IBD while decreasing direct costs to the healthcare system and individuals living with IBD.
Methods and procedures
Study design
This study is part of a larger patient-oriented mixed-methods study that utilized a convergent design approach (QUAN + QUAL) (Creswell & Plano Clark, 2018). This manuscript reports on the qualitative findings. A qualitative descriptive design was used (Sandelowski, 2000, 2010). As a patient-oriented research project, our research team engaged patient and family partners who were active and equal members in decision-making throughout the entire research project, from proposal development to project completion and manuscript writing.
Setting and sample
The setting for this study was the province of SK. Purposive sampling was used and included individuals with IBD and GCPs. Eligibility criteria for individuals with IBD included a diagnosis of IBD, age of 18 years or over, current status as a resident of SK, and having had at least one in-person and one virtual appointment with a GCP for IBD care. Eligibility criteria for GCPs included employment as a gastroenterologist or nurse practitioner who provided VC to individuals with IBD in SK.
Protection of human subjects
Ethical approval was obtained from the University of Saskatchewan (BEH # 2704) prior to recruitment and data collection.
Data collection procedures
Study information (i.e., recruitment poster, an invitation letter with a link to the online survey/quantitative phase) was distributed to all SK GCPs via mail, followed by a follow-up email. Individuals with IBD were recruited out of four GCP offices; administrative personnel at these offices distributed the study information to potential participants via mail or email (as per clinic routine) during the scheduling of appointments. Recruitment and data collection occurred between December 2021 and June 2022. Interested individuals with IBD could contact the study's principal investigator for more information and could request to only participate in the qualitative phase, although none did.
Once individuals completed the online survey (quantitative phase), they were directed to an independent section of the survey where they could voluntarily provide their name and contact information to participate in the qualitative phase. Potential participants were next contacted by the research assistant (BR) to voluntarily opt-in to the qualitative phase. Prior to data collection, participants were provided with the rationale for the study and completed a consent form and demographic questionnaire. Participants self-selected a private location for the digitally recorded 1:1 telephone interview (∼60 min) with BR. Using a semi-structured interview guide, questions focused on gaining an understanding of participant experiences and perspectives of virtual IBD care along with their suggestions for ways to enhance VC services and supports for individuals with IBD (see supplemental materials for the interview guide). While all participants were asked the same base interview questions, depending on the data provided by the participants during the interview, additional interview questions were sometimes asked to seek out clarification, alternative associations, possible relationships, or exceptional circumstances. Field notes were taken by BR during the interview to capture participant responses, interviewer insights and questions, and topics to clarify or explore with the participant later in the interview. Each participant was interviewed once, and the transcripts were not returned to participants for review. Data on individuals who decided not to participate was not collected and there was no attrition during the qualitative phase.
Data analysis procedures
Interviews were transcribed verbatim, with transcripts reviewed for errors or omissions by comparing them against the digital recordings. Data were stored and managed using NVivo® software. Data were analyzed by BR using an inductive conventional content analysis approach (Elo & Kyngas, 2008; Hsieh & Shannon, 2005). Data were collected and analyzed concurrently to allow for the development of a fulsome and rich description of the categories to allow for category saturation. The principal investigator (NR) supervised and oversaw the data analysis process. All research team members, including patient and family partners, reviewed and approved the categories.
Results
A total of 25 individuals living with IBD and five GCPs participated in interviews. Descriptive characteristics and health care utilization and VC preferences and satisfaction among individuals living with IBD are given in Tables 1 and 2, respectively. Descriptive data and VC preferences among GCPs are in Table 3. As this was a mixed methods study, persons who participated in the qualitative phase were similar in their demographic characteristics as compared with the larger quantitative sample (n = 87). See Tables 1 and 3 for comparisons. Inductive content analysis of the interviews with both persons living with IBD and providers resulted in three overarching key categories: benefits of virtual IBD care delivery, challenges of virtual IBD care delivery, and optimizing IBD care delivery.
Descriptive characteristics and health care utilization of individuals living with inflammatory bowel disease.
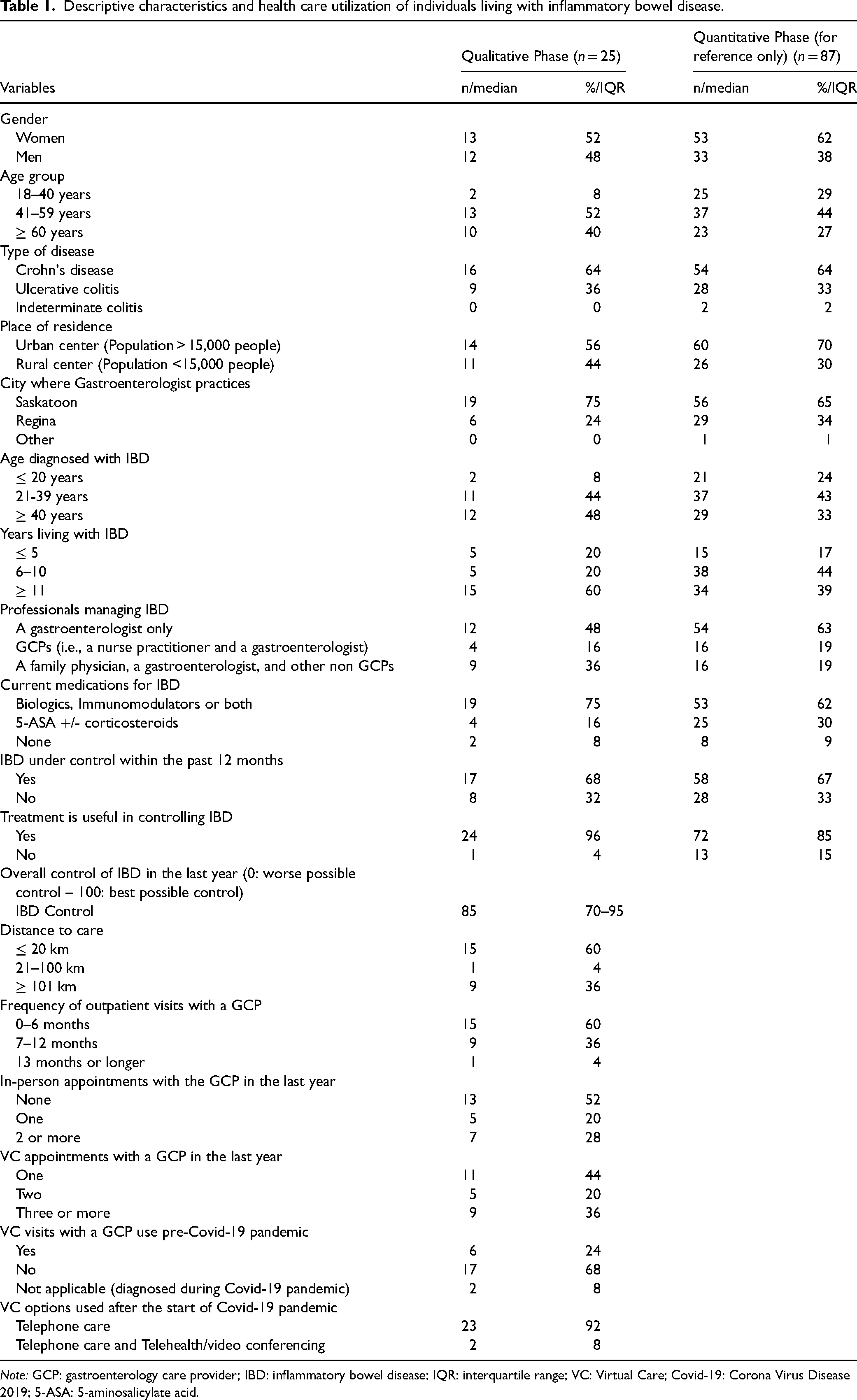
Note: GCP: gastroenterology care provider; IBD: inflammatory bowel disease; IQR: interquartile range; VC: Virtual Care; Covid-19: Corona Virus Disease 2019; 5-ASA: 5-aminosalicylate acid.
Preferences, perceptions, and satisfaction of individuals living with inflammatory bowel disease (n = 25).
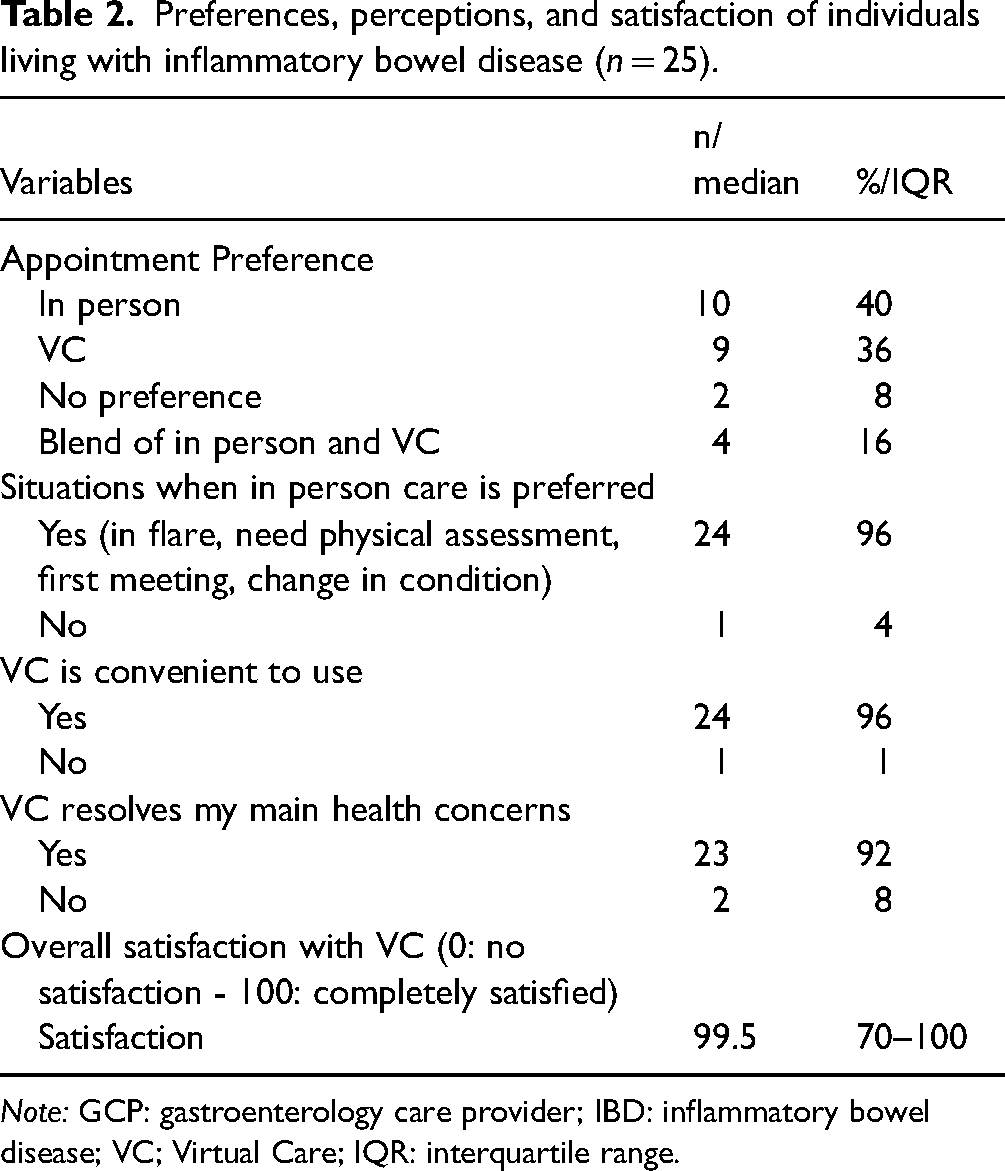
Note: GCP: gastroenterology care provider; IBD: inflammatory bowel disease; VC; Virtual Care; IQR: interquartile range.
Descriptive characteristics of the gastroenterology care provider participants.
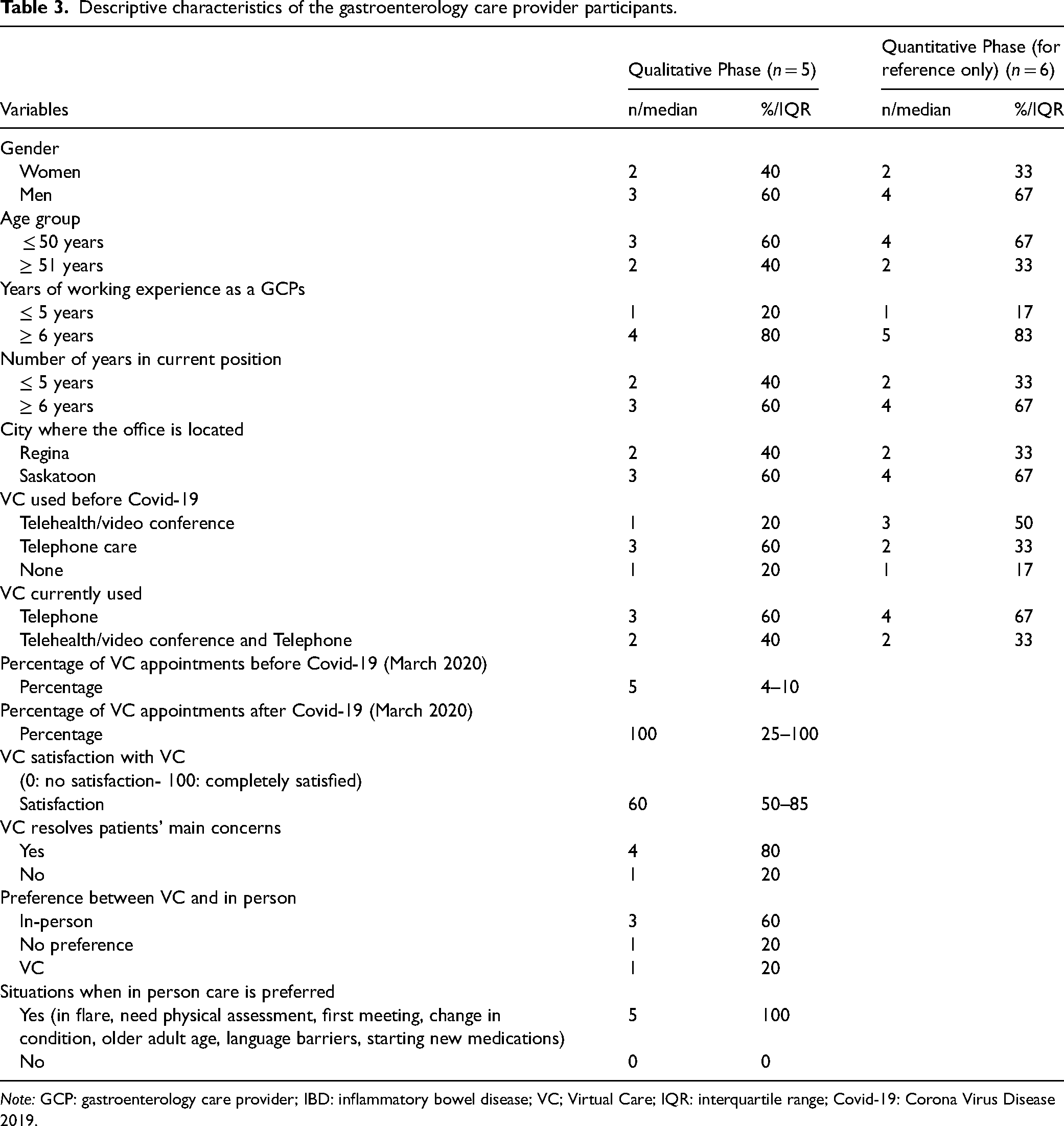
Note: GCP: gastroenterology care provider; IBD: inflammatory bowel disease; VC; Virtual Care; IQR: interquartile range; Covid-19: Corona Virus Disease 2019.
Benefits of virtual IBD care delivery
Virtual IBD care delivery had several advantages for both patients and providers. These benefits are embodied by four subcategories: improving patient access to specialized care; flexibility in care delivery; cost savings for patients; and minimizing risks.
Improving patient access to specialized care
For patients interviewed, quality IBD care often meant timely access to specialized GCPs and IBD-related services (i.e., laboratory services, diagnostics, pharmaceuticals, infusions, emergency services). Many patients noted VC significantly decreased the wait times they experienced pre-pandemic to obtain an appointment with a GCP: …it's easier and faster to get appointments – I don’t have to wait two months to get something – they’ll usually call me in a week – it means that we can resolve acute issues quicker, versus having them blow up to something more chronic. (PT01)
Some GCPs noted they could fit more patient visits into a work day through VC delivery, as VC allowed for impromptu phone calls for patient check-ins and follow-ups when lulls in schedules arose. GCP01 stated: “I’m able to get to more people now. I can cold call somebody and say ‘I was just reviewing your labs, do you have time to chat about this?’ and just do a visit right there on the fly”. Flexibility in scheduling, improved patient-provider contact, and accelerated timelines for patient care delivery were listed as benefits of VC for some GCPs. “I think our communication is still good. I think our work/life balance is much better, and I think access to patients and timeliness of their care is better. So I don’t think we have lost very much at all” (GCP01).
Flexibility in care delivery
VC was seen as convenient for patients, and having the option of meeting with a provider within the comfort of one's personal residence or community was seen as valuable. You can take the call anywhere. You don't have to be sick. You don't have to be in an emergency place…I've taken calls when I'm on a tractor…you're not tied to any place for the call. (PT07)
Patients residing in rural environments often valued the convenience and efficiency that virtual consultations provided: “For me it's six hours out of my day to go into the hospital to see somebody in-person for 15 min” (PT17). GCPs noted that rural and remote patients often benefited most from VC delivery formats: Some people I don't see because they don't have the means to get out of their office and go to your office and they live two, three hours away. And for [these] people [virtual care] might be the only option, the only way to get access to you and in those cases I think it's pertinent. (GCP04)
Cost savings for patients
Telephone appointments eliminated most of the out-of-pocket expenses that patients incurred when attending in-person consultations. For patients, costs such as parking, travel, meals, accommodations, missed work hours, and obtaining childcare were notable. “We used to live in the north and I wish that we had video conferencing when I lived in the north because to drive six hours to see somebody or 12 [hours] there and back, it's hard” (PT11).
Minimizing risks
VC minimized the potential risks and stresses associated with winter travel, during which time road conditions were considered especially hazardous. GCP05 noted that one of the benefits of VC for patients was: …not having to travel. So especially out-of-towners love it. In the wintertime, roads are terrible, dealing with winter ice, so I think they love the idea that they don't have to get in a car and come down. And I think that's reasonable. And that's what I really think phones should be for.
Challenges of virtual IBD care delivery
For participants, VC delivery was not without challenges. Providers reported more issues with VC delivery than patients, but experiences within both patient and provider groups were variable. The challenges of virtual IBD care were articulated by four subcategories: patient fit for the type of service; communication; relationship building; and coordination of care.
Patient fit for the type of service
VC often satisfied the IBD care needs of medically stable patients, where one's IBD was considered well managed with a stable and effective treatment regimen. If a patient was due for a routine check-up, receiving unremarkable test results, or in need of prescription refills, patients often reported no difference between the quality of IBD care received virtually or in-person. However, most patients preferred in-person appointments with a trusted GCP if one needed a physical assessment, was experiencing a health crisis, was managing a flare, or had current pain levels that were considered unmanageable. PT04 explains that VC is: …very, very convenient when you’re in maintenance mode, it's very convenient for everybody. It's cost effective for the medical health system, I'm a senior citizen so I don’t like getting in my car [to] try to find parking, it's very convenient for me too. But when people are in crisis, convenient isn’t what you need, you need care. And so I feel like we’re sacrificing care for convenience. …when you're reading a [test] result with a simple result, those are easy and that's efficient. Those people don't have to take a day off work, those people don't have to drive, it's a little quick phone call, it takes five minutes of their day, provides me with all the information I need to give them good care. That's who virtual care should be for. It shouldn't be for full assessments and complex follow-ups. (GCP05)
COVID-19 restrictions necessitated the rapid transition to VC for most patient-provider interactions, regardless of patient preference or patient fit for service. The majority of GCPs expressed concerns that certain patients were not necessarily served best through virtual means: “in the beginning we didn't have a filter to say who is a good IBD patient for [VC] or not because everybody had to be done by [VC]; there was no choice” (GCP05). Patients who were unwell, new intakes, starting new treatment regimens, of advanced age, with limited English proficiency, and with hearing deficits were listed by GCPs as poor candidates for VC.
Communication
Telephone consultations often proved problematic for unwell patients as they did not allow for comprehensive visual and physical assessments. For example, in-person appointments allowed patients to easily point to areas of pain and facilitated ease and clarity in communicating specific IBD care needs: “when you’re trying to explain approximately where you’re having sensitivity in your bowels, it's hard to do that virtual versus in person. You can’t quite easily explain it or point it out as to exactly where that's bothering you” (PT02).
In-person appointments also allowed for careful observations of a patient's current mobility level, mood, and general demeanour. Such observational health indicators lend additional information to the holistic assessment of patient overall well-being: …even just seeing them you get so much information, just the how they walk into the office. What are limitations for mobility or are they having pain? Do they look tired? Do they look weak? You get all those cues into one 10-s view of the patient walking into your office that you cannot get by other means. (GCP04)
Similarly, some participants mentioned that significant health indicators may be easier to overlook through virtual communication methods: I think sometimes you can get a feel of a person better in-person…my mother's 90-years-old and I know when she goes to see the doctor, the doctor can read more about what's going on than when she talks to her on the phone, and I feel that's the same with me. (PT11)
In VC, GCPs were often left with less assessment data on which to base clinical decisions. The increased onus was placed on the patient to be forthcoming with changes in health status and for the provider to ask the right questions to ensure optimal VC: …when a patient's talking to me about how bad the arthritis is in her hand; I don’t get to see that. And so I have to question them thoroughly about it and try and guess what it looks like. And those details sometimes make a difference – sometimes they don’t. So I actually don’t know how much I don’t know, and that makes me uncomfortable. (GCP01)
Thus, transparency and honesty in the communication between patients and GCPs were considered important factors in the quality of VC: I am honest with them when they call about my situation. What I’m eating and what I’m – else I’m doing. And so, as long as [they] think you’re being honest, then they can make the right calls about whether you should come [in], they need to see you or whether they can continue on the phone. (PT03)
GCPs reported devoting extra effort and time to probe for more health data. Providers often reported they checked in frequently with certain patients, including those with active disease, with complex case histories, or managing multiple comorbidities. Some participants noted that patients may not be completely forthcoming with changes in personal IBD-related health needs during VC consultations: “Somebody could be feeling terrible and not want to talk about it or not really come forth with all their issues. But then if you’re looking at them, you know that there's more going on than what they’re saying” (PT06). GCP03 explained the quality of assessment virtually: …depends how good you are at squeezing out their problem and how open they are to discussing it with you versus generally on the phone you’re only using verbal communication – whereas if you’re in clinic, you’re using different modes of communication. So I can read a cue better from a patient if they’re not disclosing everything or they’re minimizing their symptoms. I can read that better in-person.
Telephone appointments made it difficult to visually assess patient reactions to the information provided. In-person consultations allowed for more opportunities to offer additional support if patients appeared confused or overwhelmed by the topic at hand. GCP05 stated that with VC: …sometimes patients don't get a chance to ask that second time, ‘can you go over that again? I don't understand this?’ Whereas in person [I can say], ‘Do you have anything else that doesn't make sense?’ …[I] don't have that body language piece of communication, when you can see their eyes that they don't know what you're talking about. …on a phone it's so difficult.
Relationship building
Most participants noted that the development and maintenance of a solid patient-provider relationship was an important factor in the overall quality of IBD care delivery. GCPs noted in-person appointments were more appropriate than VC consultations for relationship building and developing baseline rapport between patients and providers. In-person appointments were important for: …relatively new patients as well. [We] don't have any rapport, it could be somebody you just scoped, you diagnosed, you're following up, you're talking about drugs, you have to counsel them on different medications, how they work. That's so hard to do over the phone. (GCP05) …sometimes it's better in that when you need some emotional support to be with a real physical person versus on the phone. So I think it's, less isolating. I think there's still some elements of person to person contact that makes someone feel more supported emotionally. I think that is missing from the virtual. (PT05)
Likewise, GCPs noted some patients truly benefited from the connection that in-person consultations offered. Some felt VC delivery may not meet these needs, especially if patients were unwell, experiencing a health crisis, or receiving upsetting test results.
A few patients worried that VC delivery could potentially result in GCPs minimizing or dismissing patient health concerns: …I feel like when you see the person, you get a better sense of what's really going on. I think they listen better when you have a physical person sitting in front of you, it's hard not to be empathetic. (PT23)
Knowing that a GCP was engaged and taking personal health concerns seriously was considered important for some patients: I think that one of the biggest things about seeing someone in person is body language. I think of my provider in some days when [the provider is] not listening to me or some days when [the provider is] fully invested right. And there's a difference there when you’re looking at the person and you’re not actually listening to me right now. (PT09)
Coordination of care
While most patients and a few GCPs found VC consultations convenient and efficient, some GCPs reported significant sustained interruptions to normal work day flow. Some GCPs reported ongoing administrative challenges associated with patient scheduling, patient preparedness, and coordination of IBD care virtually. For example, in-person appointments were organized and structured with a familiar administrative booking system. With the switch to VC, booking and successfully connecting with patients for virtual IBD consultations often became complex: …you schedule a call, have to hope everything works out, that you're one, calling them on time, but two, that they're answering, you never know what comes up in their lives, or something. There's a lot of missed appointments as a result of virtual care too. And so how do you chase down these patients? It's tough. (GCP05) … don’t walk into your clinic, they don’t make the process of preparing themselves for the appointment when they line up their complaints, bring their medications, bring their results, or to take the family member who has questions with them. So they lose all that process in preparation.
Traditionally, in-person consultations allowed for accessible and immediate transfer of medical forms, such as lab requisitions and prescriptions. GCP03 explained with VC: I have to either mail it [requisitions] to them or I email and they have to print it, so then they have to have a computer, they have to have a printer, they have to have a home address that way they can pick up a piece of paper.
Additionally, a few patients missed the organizational process and flow of in-person appointments: …usually there is a requisition to get bloodwork, so what that means if I do it virtually, she has to email it to me, then I have to go print it off. And so getting that from the office at the time, I like the fact that I know I'm leaving with these things in my hand. (PT25)
It was common for GCPs to report paying out-of-pocket for some aspects involved with the coordination and delivery of adequate VC during the pandemic. Home office supplies, telephones for communicating with patients, personal computers for office work, internet and phone bills, and extra administrative support services were just some of the extra costs associated with optimal VC delivery: …it needs to be organized to make it not cause any distress to our financial structure at this point, which it is, but we understand that it's COVID times so we just say ‘whatever we have to do’. But eventually if it gets normalized, they should recognize all the limiting factors and all the extra expenses and all the extra resources that are needed to run a proper practice. (GCP04)
Optimizing virtual IBD care delivery
Patients and GCPs provided several recommendations to enhance and streamline future virtual IBD care delivery. A blend of virtual and in-person options was suggested for optimal IBD care delivery. …in a perfect world, it would be virtual care. But basically, it's part and parcel of the whole picture. And really, you can't say yes, that's the only way to go [virtual care] or no, get rid of it and get only in person visits. Because they work fine together. (PT07)
Likewise, GCPs acknowledged that VC should be an additional patient appointment option if it truly meets a patient's IBD healthcare needs: I think it's 100% what are the patient needs… that their needs have to be taken into account. So, I think even for someone that needs a face to face, but they don't want to travel, that doesn't cut it either, we need to see you face to face. So, sometimes they're not going to be happy about having to make a trip, but I think it's their medical needs and also meeting them in the middle. (GCP02)
GCPs noted providers should have the option of VC delivery formats in the future, especially if services become sustainable and delivery equalizes patient access to care: For me I think it's great that we have the option of virtual care, if we can improve it that’d be even better. Meaning if we set it up in a more formal way that might help the people, especially the people that are far away so we don’t have to necessarily bring them down for one appointment. (GCP03)
However, participants noted that virtual IBD care should be optimized to adequately meet the needs of both patients and GCPs. Comfort levels and familiarity with virtual technology were noted as potential challenges for optimal VC delivery for some: “But there's also going to be a downfall there because you’re going to have people that aren’t tech savvy. For instance, my husband doesn’t even have a cell phone. I mean he could never navigate something like that” (PT04). Participants noted additional supports were needed to normalize VC delivery. Extra assistance was needed to effectively organize, educate, orient, and ensure equitable access to VC services for all patients and providers who wanted to utilize these services.
Most patients and GCPs felt the addition of video conferencing services could mitigate some of the concerns raised over the quality of IBD care received and delivered through telephone consultations. However, potential issues such as technology failure, internet availability and reliability, and patient/provider access to technology left some respondents hesitant to use this form of virtual technology in the future: Would I prefer to actually be visiting with my patient with an image and Zoom? Yes, I would. I think we would have so many issues on the other end of that for the patients that we would probably lose time and focus in dealing with tech issues to be honest. (GCP01)
Development and provision of standardized, reliable VC infrastructure and corresponding technical support were suggested by GCPs to prevent, mitigate, and resolve potential technical challenges.
Ensuring equitable patient and provider access to VC requirements such as privacy, phone lines, stable internet, and up-to-date software and technology were important for patients and GCPs. Reliable and stable internet access was also seen as a particular potential challenge for rural and remote patients: Some marginalized patients don't have access to technology or phones as readily or live in a shared living environment or [experience lack of] privacy. There's a lot of factors that go into not knowing how good virtual care is on the other end of the phone. (GCP05)
Patients and GCPs called for the expansion of existing videoconferencing services such as Telehealth. GCP03 stated optimal VC should include: …having better times or better hours for the Telehealth. My Telehealth right now is restricted by the amount of rooms that are available by the amount of time that people are willing to provide support in the hospitals. Having extended hours might facilitate my practice to some patients who are working and don't have time to come and see me but could go at 6 pm to their hospital to get a Telehealth encounter. It's not everybody but that would facilitate my job. And having Telehealth in my office so I don't have to go to the hospital.
Discussion
The COVID-19 pandemic forced healthcare systems and services to be nimble and pivot to virtual service delivery. The goal of this project was to examine the VC experiences of individuals with IBD and GCPs. The study results are not dissimilar to other projects examining the use of VC delivery for IBD-related care. However, what is novel is the greater reliance on telephone care in SK and the contribution this project makes to the Canadian VC landscape for individuals with IBD.
Generally, most participants in this study and in the extant literature are satisfied with VC delivery and felt that patient care needs are met using this type of technology, especially when an individual's disease activity is stable (i.e., in remission) and appointments are used for routine care and follow-up (Guillo et al., 2022; Kumar et al., 2022; Lahat & Shatz, 2021; Shah et al., 2021). From the perspectives of both patients and providers, the quality of care provided using VC technologies is believed to be equivalent to in-person care, especially for routine, non-emergent appointments (Guillo et al., 2022). However, many individuals with IBD and GCPs believe in-person appointments are important when patients are experiencing a flare or new symptoms have developed. These findings also align with the extant literature (Guillo et al., 2022; Storan et al., 2023).
Individuals with IBD and GCPs in the current study and the greater literature identify benefits of VC options, including reduced out-of-pocket expenses such as parking fees and fuel costs (Guillo et al., 2022; Kumar et al., 2022). Both patients and providers also note other non-financial and time-savings benefits, including reduced waiting room times, having to take less time off work to attend appointments, and not having to arrange childcare (Kumar et al., 2022; Shah et al., 2021). Having options for VC appointments also allows for greater flexibility when inclement weather and driving conditions are treacherous as well as greater accessibility for individuals living in rural areas (Rohatinsky et al., 2021).
Limitations with VC delivery are noted in the current study and others, including the inability to perform a hands-on physical examination (Kumar et al., 2022; Lahat & Shatz, 2021). GCPs believe it is difficult to assess patient bodily or verbal cues in a virtual appointment and, as a result, they believe such appointments lead to less optimal management of a patient's condition (Guillo et al., 2022). Some individuals with IBD believe it is more difficult to ask questions of the provider using a VC format (Guillo et al., 2022). Thus, inherent limitations when using VC are noted and VC is not considered the appropriate option for all patients and situations. Some providers in the study mentioned that VC appointments were sometimes missed by patients. Other researchers have noted that patients can be unreachable when using VC for appointments resulting in inefficient use of provider time (Guillo et al., 2022).
Strategies for integrating and improving vc into IBD health service delivery
Individuals with IBD and GCPs both acknowledge that a blended model of in-person and VC health service delivery should be offered. This finding is consistent with the literature (Kumar et al., 2022). Strategies for integrating VC into health service delivery not only for individuals with IBD, but other chronic health conditions, should be considered. Flexible health service delivery options, whereby the preferences of both individuals with IBD and GCPs are considered, are essential. Individualization of care is a longstanding expectation of health service delivery and individual preferences for using VC should be taken into account. Individuals may prefer in-person appointment options if they do not have access to reliable telephone or internet services, are less comfortable using technology, have hearing impairments, or prefer to see a provider or patient in person (Kumar et al., 2022; Lahat & Shatz, 2021).
Appropriate technology infrastructure is critical for ensuring streamlined service delivery. Greater accessibility to Telehealth or other secure mobile video services with options for those outside hospital settings would assist with the limitations regarding the lack of a visual assessment and connection. The extra time, costs, and administrative resources needed to support VC services need to be acknowledged, especially for those GCPs who are in independent practices. Appropriate and standardized remuneration for GCPs using VC services should be instituted to ensure cost recovery.
Registered nurses and nurse practitioners who specialize in IBD have offered informal telephone care services for years; however, these services are not formally organized within Canada (Chauhan et al., 2022). Such nurse-led VC services should become more formalized, as these providers can address most patient disease-related concerns (Chauhan et al., 2022). Nurse-led VC services can decrease ever-growing wait lists, reduce health care resource utilization, and enhance access to care (Gleeson et al., 2023; Karimi et al., 2021). For instance, nurse-led VC services can facilitate timely access to an in-person appointment or diagnostic testing if a person with IBD is experiencing flare symptoms. Greater numbers of nurses who specialize in IBD are required to make this formalization a reality. Input from IBD nurses who do utilize VC services can be used to help plan or improve VC services overall.
If VC services are being integrated into service delivery, building rapport and trust between individuals with IBD and GCPs is important. Starting with an in-person meeting may be best to establish a therapeutic, patient-centered relationship before integrating VC services. GCPs believe the depth and breadth of conversations are better facilitated during in-person appointments (Kumar et al., 2022).
Education for individuals with IBD in preparation for an upcoming VC appointment is important (Guillo et al., 2022). If using more complicated technology or applications for VC appointments, training to allow individuals with IBD to familiarize themselves and become comfortable with the technology prior to appointments would be appropriate. GCPs could create or adapt/adopt training or preparatory resources that would meet the provider or clinic expectations.
A VC appointment checklist for persons with IBD and GCPs may be helpful to assist with preparation for meeting (Lewin et al., 2020). For example, individuals with IBD should be encouraged to ensure they are prepared and dedicating focused time during the VC appointment that is free of distractions. Other suggestions include encouraging individuals with IBD to have a list of questions ready for the GCP, or having the GCPs provide a list of key questions in advance that they will ask during the appointment so that individuals with IBD can be best prepared to respond to them. Having administrative support or nurses collect pre-appointment data and be able to troubleshoot technological challenges in advance could also be helpful. Protocols can also be established if the telephone or video connection is dropped with regards to the process for reconnection. Also, if phone calls are being made, providing information on what phone number the GCP will be calling from (i.e., a blocked number) is recommended so calls do not go missed. Additionally, if GCPs are running ahead or behind on their appointment schedule, establishing a mechanism to let individuals with IBD know, so that they can be aware and prepared, is a good practice.
Study limitations and future research
This study explored experiences from one Western Canadian province. Experiences from other provinces may be different, especially if they use VC or Telehealth more frequently or extensively than SK. The participants in the study primarily used telephone care as the VC modality for IBD-related care. While our findings are similar to other studies using a variety of other VC modalities, some findings may not be applicable to all VC contexts. Due to the limited use of VC for IBD-related care prior to data collection, this context could have influenced participant responses. A future longitudinal or cross-sectional study may be helpful to explore changes in individuals’ perceptions with more frequent use of VC over time. Future research is recommended to compare the VC experiences of individuals with IBD and GCPs across and between provinces. As with all qualitative research, generalizability is limited. This study featured limited input from GCPs (n = 5) and further research is suggested to gather perspectives from this important group of individuals. Future research could also include the integration and evaluation of a VC appointment checklist to enhance IBD care delivery.
Conclusion
Individuals with IBD and GCPs are both satisfied with the use of VC technology for appointments; however, it is not ideal in some instances, such as during disease flares or first appointments. This virtual method of connecting patients and providers is deemed especially useful for routine appointments and for persons living in rural areas. A combination of options (virtual and in-person) is recognized as the best strategy to individualize care. VC is becoming more common in the IBD care environment, but use of this technology can still be enhanced for the benefit of both patients and providers.
Supplemental Material
sj-docx-1-cjn-10.1177_08445621231219299 - Supplemental material for Exploring the Experiences of Virtual Inflammatory Bowel Disease Care in Saskatchewan
Supplemental material, sj-docx-1-cjn-10.1177_08445621231219299 for Exploring the Experiences of Virtual Inflammatory Bowel Disease Care in Saskatchewan by Noelle Rohatinsky, Brooke Russell, Juan Nicolás Peña-Sánchez, Shannon Boklaschuk, Sanchit Bhasin, Sharyle Fowler, Tomasz Guzowski, Kendall Wicks and Mike Wicks in Canadian Journal of Nursing Research
Supplemental Material
sj-doc-2-cjn-10.1177_08445621231219299 - Supplemental material for Exploring the Experiences of Virtual Inflammatory Bowel Disease Care in Saskatchewan
Supplemental material, sj-doc-2-cjn-10.1177_08445621231219299 for Exploring the Experiences of Virtual Inflammatory Bowel Disease Care in Saskatchewan by Noelle Rohatinsky, Brooke Russell, Juan Nicolás Peña-Sánchez, Shannon Boklaschuk, Sanchit Bhasin, Sharyle Fowler, Tomasz Guzowski, Kendall Wicks and Mike Wicks in Canadian Journal of Nursing Research
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided through a Saskatchewan Health Research Foundation, Solutions: Innovation Grant (#6036).
Supplemental material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.